3. Discussion
Lemierre’s syndrome or necrobacillosis or “forgotten disease”
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
[2, 3, 6]
. Its incidence is 2.8 cases/million/year in the general population, and 9.4 cases/million/year in the population of young people aged 15 to 24 in Europe
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
[6]
. The African incidence is poorly known
| [5] | Kewe I., Djomou F., Ze Minkande J., Kenna E., Mbélé P., Meva'a R., Fokouo V., Njdolo A., Bengono G. Lemierre Syndrome Revealed by Otomastoiditis in a Girl 12 years old in Yaoundé. Health Science and Disease 2016; 17 (2): 84-87. |
[5]
. It is a pathology of young, immunocompetent male adults in 75% of cases
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
| [5] | Kewe I., Djomou F., Ze Minkande J., Kenna E., Mbélé P., Meva'a R., Fokouo V., Njdolo A., Bengono G. Lemierre Syndrome Revealed by Otomastoiditis in a Girl 12 years old in Yaoundé. Health Science and Disease 2016; 17 (2): 84-87. |
| [11] | Ben Abdallah Chabchoub R., Riquet A., Ramdane A., Vallée L., Raccoussot S. Lemierre syndrome revealed by torticollis. Archives of Pediatrics 2015; 22: 540-543. |
[3, 5, 11]
. However, the incidence of infants and children is not exceptional
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
[3]
. They represent 20% of cases. LS progresses in three stages
| [11] | Ben Abdallah Chabchoub R., Riquet A., Ramdane A., Vallée L., Raccoussot S. Lemierre syndrome revealed by torticollis. Archives of Pediatrics 2015; 22: 540-543. |
[11]
. It most often begins with pharyngitis or tonsillitis
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
[2]
. Isolated cases in which sinusitis, otitis media or mastoiditis and dental abscess were the primary focus of LS have been reported
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
| [5] | Kewe I., Djomou F., Ze Minkande J., Kenna E., Mbélé P., Meva'a R., Fokouo V., Njdolo A., Bengono G. Lemierre Syndrome Revealed by Otomastoiditis in a Girl 12 years old in Yaoundé. Health Science and Disease 2016; 17 (2): 84-87. |
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
| [7] | Perreault M. A case of Lemierre syndrome. Pharmacactual 2006; 39(4): 213-217. |
[2, 5-7]
. After a few days, flu-like and anginal-like symptoms appear such as fever, chills, nausea, vomiting, neck pain and cervical lymphadenopathy
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
| [10] | Panchavati P K., Kar B, Hassoun A., Centor R M. Fusobacterium necrophorum tonsillitis with mild cases of Lemierre's syndrome. Anaerobe 2017; 43: 102-104. |
[2, 10]
. In a second phase, the infection continues to progress to the neurovascular system via the parapharyngeal space, which gives rise to thrombophlebitis of the internal jugular vein. In front of the sternocleidomastoid muscle, in the angle of the jaw, a unilateral swelling develops, painful on pressure, and more rarely trismus
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
| [5] | Kewe I., Djomou F., Ze Minkande J., Kenna E., Mbélé P., Meva'a R., Fokouo V., Njdolo A., Bengono G. Lemierre Syndrome Revealed by Otomastoiditis in a Girl 12 years old in Yaoundé. Health Science and Disease 2016; 17 (2): 84-87. |
[2, 5]
. Thrombosis of the internal jugular vein can only very rarely be palpated, in the form of a palpable cord in front of the sternocleidomastoid muscle
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
| [5] | Kewe I., Djomou F., Ze Minkande J., Kenna E., Mbélé P., Meva'a R., Fokouo V., Njdolo A., Bengono G. Lemierre Syndrome Revealed by Otomastoiditis in a Girl 12 years old in Yaoundé. Health Science and Disease 2016; 17 (2): 84-87. |
| [12] | Benhammou A., Mimouni H., Nazih N., Boulaadas M., Benbouzid M A., Boulaich M., Essakali L., Kzadri M. Lemierre syndrome secondary to chronic cholesteatomatous otitis media. The ENT and head and neck surgery letter 2009; 318: 29-31. |
[2, 5, 12]
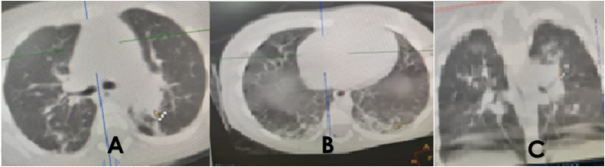
. Damage to cerebral nerves X–XII and Horner syndrome are very rare. During the third phase, from jugular vein thrombophlebitis, dissemination and septic embolism occur, preferably in the lungs (80%), with bilateral nodular infiltrates, lung abscesses and pleural effusions. In 16.5% of cases, joint damage occurs, with arthralgia or septic arthritis. The patient then finds himself increasingly in a state of septic shock, with beginning multi-organ dysfunction and respiratory failure
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
| [5] | Kewe I., Djomou F., Ze Minkande J., Kenna E., Mbélé P., Meva'a R., Fokouo V., Njdolo A., Bengono G. Lemierre Syndrome Revealed by Otomastoiditis in a Girl 12 years old in Yaoundé. Health Science and Disease 2016; 17 (2): 84-87. |
[2, 5]
. Clinical manifestations and symptoms vary depending on the location of the septic emboli. It could be an isolated infectious syndrome, pulmonary, neurological, digestive or even joint symptoms...
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
[2]
. It occurs on average a few days to 3 weeks after an ENT infection
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
[2, 3]
. Cases of infectious endocarditis have also been reported
| [12] | Benhammou A., Mimouni H., Nazih N., Boulaadas M., Benbouzid M A., Boulaich M., Essakali L., Kzadri M. Lemierre syndrome secondary to chronic cholesteatomatous otitis media. The ENT and head and neck surgery letter 2009; 318: 29-31. |
[12]
. LS must systematically be part of the differential diagnosis in a child, adolescent or young adult presenting with an oropharyngeal infection which progresses unfavorably, with the appearance of local complications (painful swelling of the cervical region) or a serious septic state not present. controlled
| [7] | Perreault M. A case of Lemierre syndrome. Pharmacactual 2006; 39(4): 213-217. |
| [13] | Assouan C., Salami A., Anzouan-Kacou E., Nguessan N., Konan E. Cervical necrotizing cellulitis revealing Lemierre syndrome. Rev Stomatol Chir Maxillofac Oral Chir 2016; 117: 158-160. |
[7, 13]
. The pathogen most commonly responsible is a Gram-negative anaerobic bacterium,
Fusobacterium necrophorum (FN)
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
| [5] | Kewe I., Djomou F., Ze Minkande J., Kenna E., Mbélé P., Meva'a R., Fokouo V., Njdolo A., Bengono G. Lemierre Syndrome Revealed by Otomastoiditis in a Girl 12 years old in Yaoundé. Health Science and Disease 2016; 17 (2): 84-87. |
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
[2, 3, 5, 6]
. It is a commensal bacterium of the oropharynx, digestive tract and female genital tract
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
| [7] | Perreault M. A case of Lemierre syndrome. Pharmacactual 2006; 39(4): 213-217. |
[6, 7]
. It can be detected by blood culture which remains the reference examination, or from biological fluids, or by sampling abscessed collections
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
[3, 6]
. The negativity of the cultures can be explained by the significant fragility of the germ, particularly during its transport to the laboratory
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
| [4] | Salami A., N'guessan N D., Kadre A., Assouan C., Anzouan-Kacou E., Konan E. Lemierre syndrome: know it to better recognize it. Rev Col Odonto-Stomatol Afr Chir Maxillo-fac 2018; Special: 41-44. |
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
[3, 4, 6]
. Infections decapitated by prior administration of antibiotics are also a source of sterile cultures
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
[6]
. In blood cultures, FN bacteria are detected after 48 hours in approximately 70% of patients. Direct detection by PCR of FN is favored because of the rapid obtaining of results and the greater specificity and sensitivity
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
[2]
. In 5% of cases, other pathogens such as
Klebsiella pneumoniae are isolated
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
| [4] | Salami A., N'guessan N D., Kadre A., Assouan C., Anzouan-Kacou E., Konan E. Lemierre syndrome: know it to better recognize it. Rev Col Odonto-Stomatol Afr Chir Maxillo-fac 2018; Special: 41-44. |
| [5] | Kewe I., Djomou F., Ze Minkande J., Kenna E., Mbélé P., Meva'a R., Fokouo V., Njdolo A., Bengono G. Lemierre Syndrome Revealed by Otomastoiditis in a Girl 12 years old in Yaoundé. Health Science and Disease 2016; 17 (2): 84-87. |
| [9] | Kharoubi S. Lemierre syndrome due to Klebsiella Pneumoniae: Clinical and therapeutic considerations. J TUN ENT 2020; 43: 73-76. |
[2, 4, 5, 9]
. Mixed cultures are found in 10 to 30% of cases. A synergistic effect between different pathogens is discussed. Furthermore, scientists also discuss the possibility that LS caused by FN may be favored by a pre-existing infection with the Epstein-Barr virus (EBV), cytomegalovirus (CMV), influenza A virus, or even
Mycoplasma pneumoniae | [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
[2, 6]
. Different endotoxins, hemolysins and hemagglutinins cause a weakening of the local immune response, an intense inflammatory reaction and the formation of thrombi
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
[2]
. Biologically, the condition is characterized by an inflammatory syndrome. CRP often exceeds 150 mg/dl
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
| [9] | Kharoubi S. Lemierre syndrome due to Klebsiella Pneumoniae: Clinical and therapeutic considerations. J TUN ENT 2020; 43: 73-76. |
[2, 9]
. There may also be hyperbilirubinemia, elevated liver parameters, increased renal values, electrolyte abnormalities, thrombocytopenia (consumption coagulopathy, disseminated intravascular coagulation) and neutrophilia
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
[2]
. The imaging modality of choice is contrast-enhanced computed tomography (CT) of the neck and thorax
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
[2, 3]
. It makes it possible to visualize and characterize an endoluminal defect in favor of thrombosis of the jugular vein or one of its collaterals. Locoregional complications as well as distant septic localization, particularly pulmonary, are also objectified
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
[3]
. Depending on the clinical picture, it is also possible to perform an abdominal CT if there is suspicion of intra-abdominal organ involvement or a cranioencephalic CT if there is suspicion of intracranial involvement (meningitis, sigmoid sinus thrombosis or of the cavernous sinus)
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
[2]
. Cervical venous Doppler ultrasound is a non-irradiating, operator-dependent examination
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
[3]
. As an alternative or complement to CT, it has excellent sensitivity
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
[6]
. It can contribute to the diagnosis by objectifying a vein increased in diameter, incompressibility of the vein, and/or the absence of flow
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
| [12] | Benhammou A., Mimouni H., Nazih N., Boulaadas M., Benbouzid M A., Boulaich M., Essakali L., Kzadri M. Lemierre syndrome secondary to chronic cholesteatomatous otitis media. The ENT and head and neck surgery letter 2009; 318: 29-31. |
[3, 6, 12]
. As a result, it constitutes an excellent element for monitoring patients
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
[3, 6]
. However, it does not allow the identification of subclavicular, retro-mandibular and early thrombi
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
| [12] | Benhammou A., Mimouni H., Nazih N., Boulaadas M., Benbouzid M A., Boulaich M., Essakali L., Kzadri M. Lemierre syndrome secondary to chronic cholesteatomatous otitis media. The ENT and head and neck surgery letter 2009; 318: 29-31. |
| [13] | Assouan C., Salami A., Anzouan-Kacou E., Nguessan N., Konan E. Cervical necrotizing cellulitis revealing Lemierre syndrome. Rev Stomatol Chir Maxillofac Oral Chir 2016; 117: 158-160. |
[6, 12, 13].
Cervical MRI allows a precise study of the extension of the thrombus and a mapping of possible loco-regional complications
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
| [11] | Ben Abdallah Chabchoub R., Riquet A., Ramdane A., Vallée L., Raccoussot S. Lemierre syndrome revealed by torticollis. Archives of Pediatrics 2015; 22: 540-543. |
[3, 11]
. The 18-fluorodeoxyglucose PET scan allows early diagnosis, especially peripheral septic emboli. It contributes to early treatment as a complement or alternative to conventional imaging. The high costs and availability of these last two examinations constitute limitations in our context
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
[3]
. LS is a pathology that can be fatal with mortality estimated at 90% in the absence of early and adequate treatment. Optimal management makes it possible to lower this rate to a percentage between 2 and 10%
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
[2, 3, 6]
. The majority progresses towards complete recovery under treatment but can also lead to the death of the patient
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
[6]
. Treatment is based on first-line double antibiotic therapy combining a beta-lactam with a beta-lactamase inhibitor or a third-generation cephalosporin, with metronidazole intravenously then monotherapy with imipenem or moxifloxacin orally for a total duration of 3 to 6 weeks
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
[3]
. Some authors recommend intravenous monotherapy with clindamycin. For
Fusobacterium necrophorum, there is resistance to macrolides, quinolones, trimethoprim/sulfamethoxazole, amino-glycosides and partly also to penicillin
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
[2]
. Anticoagulation remains highly debated between the risk of thrombus dissemination and retrograde septic extension, so its use must be the subject of multidisciplinary discussion on a case-by-case basis
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
[2, 3, 6]
. Indications for anticoagulation are reserved for high-risk situations linked to thrombosis (retrograde septic extension from the internal jugular vein, sigmoid sinus thrombosis, thrombophilia, lack of response to antibiotic treatment, or even cerebral infarction)
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
[6]
. Surgical drainage of abscessed collections with abundant washing is of great benefit
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
| [9] | Kharoubi S. Lemierre syndrome due to Klebsiella Pneumoniae: Clinical and therapeutic considerations. J TUN ENT 2020; 43: 73-76. |
[2, 3, 6, 9]
. It represents an essential part of the care. It makes it possible to eliminate all local sources favoring anaerobic conditions
| [13] | Assouan C., Salami A., Anzouan-Kacou E., Nguessan N., Konan E. Cervical necrotizing cellulitis revealing Lemierre syndrome. Rev Stomatol Chir Maxillofac Oral Chir 2016; 117: 158-160. |
[13]
. This treatment allows for a favorable evolution, which was the case for our patient. Ligation-excision of the internal jugular vein remains exceptional and limited to certain cases of progression (persistence of septic emboli under optimal antibiotic treatment, extensive septic thrombosis, or even severe uncontrolled sepsis)
| [2] | Schahab C. Lemierre syndrome, A partly “forgotten” condition, but which has not disappeared. Swiss Medical Forum 2012; 12(19): 386–388. |
| [3] | Imane A., Sayad Z., Laassikri O., Nitassi S., Bencheikh R., Benbouzid M A., Oujilal A., Boulaadas M., Essakalli Hossyni L. An unexpected cause of forgotten illness: about 'a case. PAMJ Clinical Medicine. 2020; 4(21): 1-9. |
| [4] | Salami A., N'guessan N D., Kadre A., Assouan C., Anzouan-Kacou E., Konan E. Lemierre syndrome: know it to better recognize it. Rev Col Odonto-Stomatol Afr Chir Maxillo-fac 2018; Special: 41-44. |
| [6] | Mesrar H., Mesrar J., Maillier B., Kraoua S., Chapoutot L., Delclaux B. Lemierre syndrome: diagnosis, exploration, treatment. The Journal of Internal Medicine 2018; 39: 339–345. |
[2-4, 6]
.