Department of Anesthesiology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Contributor Roles: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing
Department of Anesthesiology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Contributor Roles: Data curation, Formal Analysis, Investigation, Writing – original draft, Writing – review & editing
Department of Anesthesiology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Department of Anesthesiology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Department of Anesthesiology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Department of Anesthesiology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Department of Anesthesiology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Department of Anesthesiology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Background: The insertion depth of the bronchial blocker demands precise positioning and bronchoscopic confirmation. This study aims to investigate the parameters that influence the insertion depth of bronchial blockers in thoracic surgery. Methods: 110 adult patients receiving thoracic surgery at Yichang Central People's Hospital were recruited as study participants. Age (A), gender (G), weight (W), and height (H) of patients were recorded. Following general anesthesia, a single-lumen tube was intubated. The bronchial blocker was placed using a video flexible scope at the optimal position in the left or right main bronchus, noting the depth (D) of tube insertion. Pearson correlation analysis and linear regression analysis were conducted on the data. Results: There was a significant gender difference in the insertion depth of the bronchial blocker (P < 0.01); There was no statistically significant difference in insertion depth between the left and right sides (P > 0.05). Height was significantly correlated with the insertion depth of the bronchial blocker (P < 0.01). Weight showed a weak correlation with insertion depth (P < 0.05), and age showed no correlation with insertion depth (P > 0.05). The single-factor linear regression equation for height and the insertion depth was D = 5.841 + 0.138H (coefficient of determination R² = 0.42). The multivariate linear regression equation with height, weight, and age as independent variables was D = 2.638 + 0.158H - 0.017W + 0.016A (coefficient of determination R² = 0.51), indicating a better linear fit than the former. Conclusion: The multivariate linear regression equation D = 2.638 + 0.158H - 0.017W + 0.016A can be used to quickly predict the insertion depth of bronchial blocker, which can then be confirmed visually with flexible scope techniques.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
The double lumen tube (DLT) intubation and Bronchial Blocker (BB) insertion are two commonly used methods for implementing one-lung ventilation in clinical settings
[1]
Shum S, Moreno Garijo J, Tomlinson G, et al. A Clinical Comparison of 2 Bronchial Blockers Versus Double-Lumen Tubes for One-Lung Ventilation. J Cardiothorac Vasc Anesth [J]. 2023, 37(12): 2577-2583.
Yang L, Wei X, Wang B, et al. A comparison between bronchial blockers and double-lumen tubes for patients undergoing lung resection: A propensity score-matched cohort study. Int J Med Sci. 2022, 19(11): 1706-1714.
. DLT intubation is characterized by higher operational difficulty, longer positioning time, and a higher risk of airway injury. In contrast, BB offers advantages such as easier insertion, less injury, shorter insertion time, and fewer complications
[3]
Nakanishi T, Sento Y, Kamimura Y, et al. Combined use of the ProSeal laryngeal mask airway and a bronchial blocker vs. a double-lumen endobronchial tube in thoracoscopic surgery: A randomized controlled trial [J]. J Clin Anesth. 2023, 88: 111136.
Guoqin Zhao. Comparison of the application effect of double-lumen tracheal catheter and bronchial occluder in thoracic surgery [J]. China Prac Med, 2024, 03: 45-48.
. Although many different types of BB have been widely used in thoracic surgery, imprecise insertion of BB can lead to prolonged insertion times, poor lung collapse quality, and adverse outcomes such as hypoxemia after one-lung ventilation
[5]
Palaczynski P, Misiolek H, Szarpak L, et al. Systematic Review and Meta-Analysis of Efficiency and Safety of Double-Lumen Tube and Bronchial Blocker for One-Lung Ventilation [J]. J Clin Med. 2023; 12(5): 1877.
Kumar N, Mitchell J, Siemens A, et al. Left-Sided Double-Lumen Tube vs EZ-Blocker for One-Lung Ventilation in Thoracic Surgery: A Systematic Review and Meta-Analysis. Semin Cardiothorac Vasc Anesth. 2023; 27(3): 171-180.
. Thus, quickly predicting BB insertion depth and accurate positioning are crucial for airway management during thoracic surgeries. Traditional localization methods after BB insertion include auscultation, monitoring of partial pressure of carbon dioxide at the end of expiration and peak pressure of airway, and ultrasonic localization. These methods are time-consuming, complicated to operate, and inaccurate
[7]
Zetlaoui PJ. Ultrasonography for airway management [J]. Anaesth Crit Care Pain Med. 2021, 40(2): 100821.
Congedi S, Savio F, Auciello M, et al. Sonographic Evaluation of the Endotracheal Tube Position in the Neonatal Population: A Comprehensive Review and Meta-Analysis. Front Pediatr. 2022; 10: 886450. Published 2022 Jun 2.
Mitra A, Gave A, Coolahan K, et al. Confirmation of endotracheal tube placement using disposable fiberoptic bronchoscopy in the emergent setting. World J Emerg Med. 2019; 10(4): 210-214.
. The purpose of this study is to investigate a quick method for BB insertion depth prediction and to explore the factors that affect BB insertion depth.
2. Materials and Methods
The study was approved by the Ethics Committee of the Yichang Central People's Hospital (No.2025-061-01). 110 adult patients (age > 18 years old) who underwent elective thoracic surgery in Yichang Central People's Hospital from March 2024 to March 2025 were selected, ASA I ~ III, regardless of gender. The types of surgery included thoracotomy or thoracoscopic lobectomy, esophageal surgery, and mediastinal surgery. All the selected patients had no history of serious heart, lung, liver, and kidney diseases, gastroesophageal reflux, respiratory tract infection, and abnormal airway anatomy.
All patients were fasting and drinking before the operation. After entering the operation room, peripheral venous and left radial arteries were established. ECG, HR, SpO2, and MAP were monitored. After preoxygenation, anesthesia induction was performed by intravenous midazolam 0.05mg/kg, sufentanil 0.6μg/kg, propofol 2mg/kg, and rocuronium 0.5mg/kg. After mandibular relaxation, a 7.5 mm single-lumen endotracheal tube and BB (Yichang Humanwell Bronchial Blocker; Yichang Humanwell Pharmaceutical CO., LTD, Yichang, China) were inserted sequentially. Then using a video flexible scope to locate the optimal placement position of BB: (1) The carina and the openings of the left and right main bronchi were observed through the tracheal catheter, and the blue cuff edge of BB was just below 2cm below the carina level; (2) The opening of the distal left upper lobe and lower lobe bronchus can be seen through the left bronchus. The opening of the distal right upper lobe, middle lobe, and lower lobe bronchus was not blocked by the BB in the right bronchus. In case of poor alignment, the proper position of BB was adjusted by a video flexible scope, and the actual insertion depth of BB was recorded again.
3. Statistical Analysis
Statistical analysis was performed using Stata 15.0 statistical software. The data was presented as mean ± standard deviation for continuous variables. The independent samples t-test was used to compare parametric data intergroup. Pearson correlation analysis was utilized to examine the correlation of the data. Linear regression explored the influencing factors of BB insertion depth and a regression equation was established. A p-value of < 0.05 was considered statistically significant.
4. Results
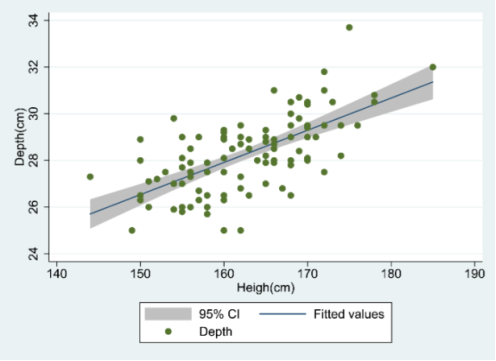
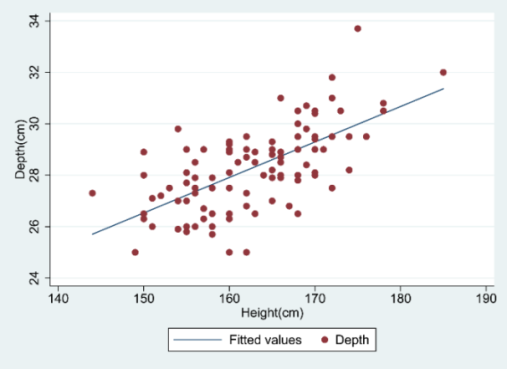
A total of 110 patients were included, including 57 males and 53 females. Compared with men and women, there are significant differences in height and weight (P < 0.01), but there is no significant difference in age (P > 0.05) (Table 1). The average insertion depth of BB was 28.27±1.58cm. The results of the stratified analysis showed that there was a significant difference in the insertion depth between the genders (P <0.01), but there was no significant difference in the insertion depth between the left and right sides (P > 0.05) (Table 2). Pearson correlation analysis showed that the height (r = 0.642, P < 0.01) was significantly correlated with the insertion depth of BB (Figure 1) and body weight (r = 0.211, P < 0.05) was weakly correlated with it. There was no correlation between age and the insertion depth of BB (P > 0.05). The linear regression equation between height and BB insertion depth was D=5.841+0.138H (the determination coefficient R2=0.42) (Figure 2). The multivariate linear regression equation between height, weight, age, and the insertion depth of BB was D=2.638+0.158H-0.017W+0.016A (the determination coefficient R2=0.51), which was better than the former.
Table 1. Patient Demographics.
Male (n=57)
Female (n=53)
Average
P
Height (cm)
167.09±6.59*
157.83±4.63
162.63±7.36
0.000
Weight (kg)
65.48±10.83*
55.81±8.95
60.82±11.05
0.000
Age (years)
61.86±10.08
62.66±10.68
62.25±10.33
0.687
NOTE. Data are presented as mean ± standard deviation.
Figure 2. Linear regression analysis of height and insertion depth.
5. Discussion
Various thoracic operations such as lobectomy, esophageal surgery, and mediastinal surgery have increased in recent years. Effective lung isolation technology and high-quality lung collapse are important to ensure the success of thoracic surgery
[10]
Dong Zhao, Na Yang, Chang Xiong, et al. Comparison of the effect between bronchial blocker and double lumen endotracheal tube on pre-thoracotomy lung collapse in thoracoscopic surgery [J]. China Journal of Endoscopy, 2022, 07: 14-20.
Mourisse J, Liesveld J, Verhagen A, et al. Efficiency, efficacy, and safety of EZ-blocker compared with left-sided double-lumen tube for one-lung ventilation. Anesthesiology. 2013; 118(3): 550-561.
. Although DLT intubation is the most commonly used method to implement one-lung ventilation at present, it has the following shortcomings: (1) The lumen of DLT is thick, and it is difficult for some patients with difficult airways to intubate. (2) It is easy to cause airway injury, such as sore throat, hoarseness, and tracheal mucosa injury. (3) It is difficult to use DLT to carry out one-lung ventilation for children with thin trachea and patients with tracheostomy. Compared with DLT, BB is commonly used due to its benefits, which include its easy operation, selective blockage of the left and right bronchi, and less physiological damage
[12]
Risse J, Szeder K, Schubert AK, et al. Comparison of left double lumen tube and y-shaped and double-ended bronchial blocker for one lung ventilation in thoracic surgery-a randomised controlled clinical trial [J]. BMC Anesthesiol. 2022, 22(1): 92.
Liu W, Jin F, Wang HM, et al. The association between double-lumen tube versus bronchial blocker and postoperative pulmonary complications in patients after lung cancer surgery. Front Oncol. 2022; 12: 1011849.
. At present, there are many methods to locate BB after insertion, such as auscultation, positioning according to the partial pressure of carbon dioxide at the end of respiration, airway pressure, etc., but there have been instances of significant inaccuracies in these methods
[14]
Men XQ, Yan XX. Tracheal Ultrasound for the Accurate Confirmation of the Endotracheal Tube Position in Obese Patients [J]. J Ultrasound Med. 2020, 39(3): 509-513.
Wang PK, Lin TY, Su IM, et al. Preoperative lung ultrasound for confirming the double-lumen endotracheal tube position for one-lung ventilation: A systematic review and meta-analysis. Heliyon. 2023; 9(4): e15458.
. Although the video flexible scope confirmation is the gold standard for positioning, it may be difficult to position patients with excessive airway secretions and abnormal airway anatomy.
In recent years, it has been reported that ultrasound is used to evaluate the depth of intubation in children, and the depth of intubation is calculated by body surface markers and other factors, but there are few studies to predict the insertion depth of BB used in thoracic surgery
[16]
Dincer E, Topçuoğlu S, Karatekin G. Ultrasonography for Determining Endotracheal Tube Tip Position in Very Low Birth Weight Infants. J Ultrasound Med. 2023; 42(2): 437-441.
Jang YE, Kim EH, Song IK, et al. Prediction of the mid-tracheal level using surface anatomical landmarks in adults: Clinical implication of endotracheal tube insertion depth [J]. Medicine (Baltimore). 2017, 96(12): e6319.
Eldawlatly AA, El Tahan MR, Kanchi NU, et al. Efficacy of height-based formula to predict insertion depth of left-sided double lumen tube: A prospective observational study [J]. Anaesth Intensive Care. 2020, 48(5): 354-357.
confirmed that the intubation depth of left DLT was significantly related to the height and obtained the equation that predicted the intubation depth of left DLT. Our study analyzed the correlation between height, weight, age, and the insertion depth of BB and found that height was significantly correlated with the insertion depth of BB (r = 0.642). Meanwhile, we performed single-factor linear regression and multi-factor linear regression and obtained the corresponding linear regression equations. This is different from the previous studies in that after determining the correlation between single-factor independent variables and dependent variables, multi-factor independent variables are included for multi-factor linear regression analysis, and it is found that the fitting degree of multi-factor linear regression is better (determination coefficient R2=0.51). On the one hand, it reduces the inaccuracy of a single factor in predicting the insertion depth of BB, on the other hand, it evaluates the insertion depth of BB from multiple factors, which improves the accuracy of prediction results.
This study has some limitations. First of all, our study did not include children patients, so the research conclusion may be more suitable for adults. Secondly, this study did not discuss the influence of the insertion depth of BB on other indexes such as hemodynamics and oxygenation. Thirdly, the airway anatomical characteristics of different patients are different, there may be failure cases of BB insertion.
6. Conclusions
In conclusion, the multi-factor linear regression equation D=2.638+0.158H-0.017W+0.016A with height, weight, and age as independent variables can be used as a rapid method to predict the insertion depth of BB. Future research can explore the influence of more different factors on the insertion depth of BB.
Abbreviations
DLT
Double Lumen Tube
BB
Bronchial Blocker
ECG
Electrocardiogram
HR
Heart Rate
SpO2
Pulse Oxygen Saturation
MAP
Mean Arterial Pressure
ASA
American Society of Anesthesiologists
A
Age
G
Gender
W
Weight
H
Height
D
Depth
Acknowledgments
We would like to express our sincere gratitude to the following in dividuals for their invaluable contributions and support throughout the study process:
Chun Chen, Department of Anesthesiology, Yichang Central People's Hospital, Yichang, China
Mingquan Chen, Department of Anesthesiology, Yichang Central People's Hospital, Yichang, China
Yanjun Liu, Department of Anesthesiology, Yichang Central People's Hospital, Yichang, China
Lei Lin, Department of Anesthesiology, Yichang Central People's Hospital, Yichang, China
Lin Cheng, Department of Anesthesiology, Yichang Central People's Hospital, Yichang, China
Bo Shi, Department of Anesthesiology, Yichang Central People's Hospital, Yichang, China
Ming Zhang, Department of Anesthesiology, Yichang Central People's Hospital, Yichang, China
Author Contributions
Yang Xiao: Writing – review & editing, Writing – original draft, Methodology, Investigation, Formal analysis, Data curation, Conceptualization
Wei Kang: Writing – review & editing, Writing – original draft, Investigation, Formal analysis, Data curation
Yang L, Wei X, Wang B, et al. A comparison between bronchial blockers and double-lumen tubes for patients undergoing lung resection: A propensity score-matched cohort study. Int J Med Sci. 2022, 19(11): 1706-1714.
Nakanishi T, Sento Y, Kamimura Y, et al. Combined use of the ProSeal laryngeal mask airway and a bronchial blocker vs. a double-lumen endobronchial tube in thoracoscopic surgery: A randomized controlled trial [J]. J Clin Anesth. 2023, 88: 111136.
Guoqin Zhao. Comparison of the application effect of double-lumen tracheal catheter and bronchial occluder in thoracic surgery [J]. China Prac Med, 2024, 03: 45-48.
Palaczynski P, Misiolek H, Szarpak L, et al. Systematic Review and Meta-Analysis of Efficiency and Safety of Double-Lumen Tube and Bronchial Blocker for One-Lung Ventilation [J]. J Clin Med. 2023; 12(5): 1877.
Kumar N, Mitchell J, Siemens A, et al. Left-Sided Double-Lumen Tube vs EZ-Blocker for One-Lung Ventilation in Thoracic Surgery: A Systematic Review and Meta-Analysis. Semin Cardiothorac Vasc Anesth. 2023; 27(3): 171-180.
Congedi S, Savio F, Auciello M, et al. Sonographic Evaluation of the Endotracheal Tube Position in the Neonatal Population: A Comprehensive Review and Meta-Analysis. Front Pediatr. 2022; 10: 886450. Published 2022 Jun 2.
Mitra A, Gave A, Coolahan K, et al. Confirmation of endotracheal tube placement using disposable fiberoptic bronchoscopy in the emergent setting. World J Emerg Med. 2019; 10(4): 210-214.
Dong Zhao, Na Yang, Chang Xiong, et al. Comparison of the effect between bronchial blocker and double lumen endotracheal tube on pre-thoracotomy lung collapse in thoracoscopic surgery [J]. China Journal of Endoscopy, 2022, 07: 14-20.
Mourisse J, Liesveld J, Verhagen A, et al. Efficiency, efficacy, and safety of EZ-blocker compared with left-sided double-lumen tube for one-lung ventilation. Anesthesiology. 2013; 118(3): 550-561.
Risse J, Szeder K, Schubert AK, et al. Comparison of left double lumen tube and y-shaped and double-ended bronchial blocker for one lung ventilation in thoracic surgery-a randomised controlled clinical trial [J]. BMC Anesthesiol. 2022, 22(1): 92.
Liu W, Jin F, Wang HM, et al. The association between double-lumen tube versus bronchial blocker and postoperative pulmonary complications in patients after lung cancer surgery. Front Oncol. 2022; 12: 1011849.
Men XQ, Yan XX. Tracheal Ultrasound for the Accurate Confirmation of the Endotracheal Tube Position in Obese Patients [J]. J Ultrasound Med. 2020, 39(3): 509-513.
Wang PK, Lin TY, Su IM, et al. Preoperative lung ultrasound for confirming the double-lumen endotracheal tube position for one-lung ventilation: A systematic review and meta-analysis. Heliyon. 2023; 9(4): e15458.
Dincer E, Topçuoğlu S, Karatekin G. Ultrasonography for Determining Endotracheal Tube Tip Position in Very Low Birth Weight Infants. J Ultrasound Med. 2023; 42(2): 437-441.
Jang YE, Kim EH, Song IK, et al. Prediction of the mid-tracheal level using surface anatomical landmarks in adults: Clinical implication of endotracheal tube insertion depth [J]. Medicine (Baltimore). 2017, 96(12): e6319.
Eldawlatly AA, El Tahan MR, Kanchi NU, et al. Efficacy of height-based formula to predict insertion depth of left-sided double lumen tube: A prospective observational study [J]. Anaesth Intensive Care. 2020, 48(5): 354-357.
Yang Xiao, Wei Kang, Qibin Ke, Xiaojuan Luo, Jianfeng Wang, et al. (2025). Correlation Analysis of Bronchial Blocker Insertion Depth in Thoracic Surgery: A Prospective Observational Study. American Journal of Clinical and Experimental Medicine, 13(2), 24-28. https://doi.org/10.11648/j.ajcem.20251302.11
@article{10.11648/j.ajcem.20251302.11,
author = {Yang Xiao and Wei Kang and Qibin Ke and Xiaojuan Luo and Jianfeng Wang and Bo Yang and Bo Zhang and Changchang You},
title = {Correlation Analysis of Bronchial Blocker Insertion Depth in Thoracic Surgery: A Prospective Observational Study
},
journal = {American Journal of Clinical and Experimental Medicine},
volume = {13},
number = {2},
pages = {24-28},
doi = {10.11648/j.ajcem.20251302.11},
url = {https://doi.org/10.11648/j.ajcem.20251302.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajcem.20251302.11},
abstract = {Background: The insertion depth of the bronchial blocker demands precise positioning and bronchoscopic confirmation. This study aims to investigate the parameters that influence the insertion depth of bronchial blockers in thoracic surgery. Methods: 110 adult patients receiving thoracic surgery at Yichang Central People's Hospital were recruited as study participants. Age (A), gender (G), weight (W), and height (H) of patients were recorded. Following general anesthesia, a single-lumen tube was intubated. The bronchial blocker was placed using a video flexible scope at the optimal position in the left or right main bronchus, noting the depth (D) of tube insertion. Pearson correlation analysis and linear regression analysis were conducted on the data. Results: There was a significant gender difference in the insertion depth of the bronchial blocker (P 0.05). Height was significantly correlated with the insertion depth of the bronchial blocker (P 0.05). The single-factor linear regression equation for height and the insertion depth was D = 5.841 + 0.138H (coefficient of determination R² = 0.42). The multivariate linear regression equation with height, weight, and age as independent variables was D = 2.638 + 0.158H - 0.017W + 0.016A (coefficient of determination R² = 0.51), indicating a better linear fit than the former. Conclusion: The multivariate linear regression equation D = 2.638 + 0.158H - 0.017W + 0.016A can be used to quickly predict the insertion depth of bronchial blocker, which can then be confirmed visually with flexible scope techniques.
},
year = {2025}
}
TY - JOUR
T1 - Correlation Analysis of Bronchial Blocker Insertion Depth in Thoracic Surgery: A Prospective Observational Study
AU - Yang Xiao
AU - Wei Kang
AU - Qibin Ke
AU - Xiaojuan Luo
AU - Jianfeng Wang
AU - Bo Yang
AU - Bo Zhang
AU - Changchang You
Y1 - 2025/04/14
PY - 2025
N1 - https://doi.org/10.11648/j.ajcem.20251302.11
DO - 10.11648/j.ajcem.20251302.11
T2 - American Journal of Clinical and Experimental Medicine
JF - American Journal of Clinical and Experimental Medicine
JO - American Journal of Clinical and Experimental Medicine
SP - 24
EP - 28
PB - Science Publishing Group
SN - 2330-8133
UR - https://doi.org/10.11648/j.ajcem.20251302.11
AB - Background: The insertion depth of the bronchial blocker demands precise positioning and bronchoscopic confirmation. This study aims to investigate the parameters that influence the insertion depth of bronchial blockers in thoracic surgery. Methods: 110 adult patients receiving thoracic surgery at Yichang Central People's Hospital were recruited as study participants. Age (A), gender (G), weight (W), and height (H) of patients were recorded. Following general anesthesia, a single-lumen tube was intubated. The bronchial blocker was placed using a video flexible scope at the optimal position in the left or right main bronchus, noting the depth (D) of tube insertion. Pearson correlation analysis and linear regression analysis were conducted on the data. Results: There was a significant gender difference in the insertion depth of the bronchial blocker (P 0.05). Height was significantly correlated with the insertion depth of the bronchial blocker (P 0.05). The single-factor linear regression equation for height and the insertion depth was D = 5.841 + 0.138H (coefficient of determination R² = 0.42). The multivariate linear regression equation with height, weight, and age as independent variables was D = 2.638 + 0.158H - 0.017W + 0.016A (coefficient of determination R² = 0.51), indicating a better linear fit than the former. Conclusion: The multivariate linear regression equation D = 2.638 + 0.158H - 0.017W + 0.016A can be used to quickly predict the insertion depth of bronchial blocker, which can then be confirmed visually with flexible scope techniques.
VL - 13
IS - 2
ER -
Department of Anesthesiology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Department of Anesthesiology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Qibin Ke
Department of Anesthesiology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Department of Anesthesiology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Jianfeng Wang
Department of Anesthesiology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Bo Yang
Department of Anesthesiology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Bo Zhang
Department of Anesthesiology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Changchang You
Department of Anesthesiology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Yang Xiao, Wei Kang, Qibin Ke, Xiaojuan Luo, Jianfeng Wang, et al. (2025). Correlation Analysis of Bronchial Blocker Insertion Depth in Thoracic Surgery: A Prospective Observational Study. American Journal of Clinical and Experimental Medicine, 13(2), 24-28. https://doi.org/10.11648/j.ajcem.20251302.11
@article{10.11648/j.ajcem.20251302.11,
author = {Yang Xiao and Wei Kang and Qibin Ke and Xiaojuan Luo and Jianfeng Wang and Bo Yang and Bo Zhang and Changchang You},
title = {Correlation Analysis of Bronchial Blocker Insertion Depth in Thoracic Surgery: A Prospective Observational Study
},
journal = {American Journal of Clinical and Experimental Medicine},
volume = {13},
number = {2},
pages = {24-28},
doi = {10.11648/j.ajcem.20251302.11},
url = {https://doi.org/10.11648/j.ajcem.20251302.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajcem.20251302.11},
abstract = {Background: The insertion depth of the bronchial blocker demands precise positioning and bronchoscopic confirmation. This study aims to investigate the parameters that influence the insertion depth of bronchial blockers in thoracic surgery. Methods: 110 adult patients receiving thoracic surgery at Yichang Central People's Hospital were recruited as study participants. Age (A), gender (G), weight (W), and height (H) of patients were recorded. Following general anesthesia, a single-lumen tube was intubated. The bronchial blocker was placed using a video flexible scope at the optimal position in the left or right main bronchus, noting the depth (D) of tube insertion. Pearson correlation analysis and linear regression analysis were conducted on the data. Results: There was a significant gender difference in the insertion depth of the bronchial blocker (P 0.05). Height was significantly correlated with the insertion depth of the bronchial blocker (P 0.05). The single-factor linear regression equation for height and the insertion depth was D = 5.841 + 0.138H (coefficient of determination R² = 0.42). The multivariate linear regression equation with height, weight, and age as independent variables was D = 2.638 + 0.158H - 0.017W + 0.016A (coefficient of determination R² = 0.51), indicating a better linear fit than the former. Conclusion: The multivariate linear regression equation D = 2.638 + 0.158H - 0.017W + 0.016A can be used to quickly predict the insertion depth of bronchial blocker, which can then be confirmed visually with flexible scope techniques.
},
year = {2025}
}
TY - JOUR
T1 - Correlation Analysis of Bronchial Blocker Insertion Depth in Thoracic Surgery: A Prospective Observational Study
AU - Yang Xiao
AU - Wei Kang
AU - Qibin Ke
AU - Xiaojuan Luo
AU - Jianfeng Wang
AU - Bo Yang
AU - Bo Zhang
AU - Changchang You
Y1 - 2025/04/14
PY - 2025
N1 - https://doi.org/10.11648/j.ajcem.20251302.11
DO - 10.11648/j.ajcem.20251302.11
T2 - American Journal of Clinical and Experimental Medicine
JF - American Journal of Clinical and Experimental Medicine
JO - American Journal of Clinical and Experimental Medicine
SP - 24
EP - 28
PB - Science Publishing Group
SN - 2330-8133
UR - https://doi.org/10.11648/j.ajcem.20251302.11
AB - Background: The insertion depth of the bronchial blocker demands precise positioning and bronchoscopic confirmation. This study aims to investigate the parameters that influence the insertion depth of bronchial blockers in thoracic surgery. Methods: 110 adult patients receiving thoracic surgery at Yichang Central People's Hospital were recruited as study participants. Age (A), gender (G), weight (W), and height (H) of patients were recorded. Following general anesthesia, a single-lumen tube was intubated. The bronchial blocker was placed using a video flexible scope at the optimal position in the left or right main bronchus, noting the depth (D) of tube insertion. Pearson correlation analysis and linear regression analysis were conducted on the data. Results: There was a significant gender difference in the insertion depth of the bronchial blocker (P 0.05). Height was significantly correlated with the insertion depth of the bronchial blocker (P 0.05). The single-factor linear regression equation for height and the insertion depth was D = 5.841 + 0.138H (coefficient of determination R² = 0.42). The multivariate linear regression equation with height, weight, and age as independent variables was D = 2.638 + 0.158H - 0.017W + 0.016A (coefficient of determination R² = 0.51), indicating a better linear fit than the former. Conclusion: The multivariate linear regression equation D = 2.638 + 0.158H - 0.017W + 0.016A can be used to quickly predict the insertion depth of bronchial blocker, which can then be confirmed visually with flexible scope techniques.
VL - 13
IS - 2
ER -