Mallory-Weiss tear (MWT) is a frequent cause of acute upper gastrointestinal (AUGI) bleeding and is defined as a longitudial superficial mucosal tear that usually occurs at the gastroesophageal junction. MWT is usually associated with increased abdominal pressure. 50 to 70% of patients diagnosed with MWT have a history of heavy alcohol intake. MWT usually presents with bright red or coffee-ground vomitus, black tar-like stool, signs of anemia, chest pain, abdominal pain, or signs of shock. Bleeding from MWT can stop on its own, however, significant bleeding may require endoscopic management. Here, we present 2 cases of life-threatening upper GI bleeding secondary to MWT. Case 1 is a 55-year-old male with known Obesity Hypoventilation Syndrome who presented with a violent cough and was initially admitted with respiratory distress. He became hypoxic and hypercarbic while on the ward and was transferred to the Intensive care Unit (ICU). A copious amount of fresh blood was drained upon passage of a nasogastric tube. The second case is a 31-year-old male who abuses alcohol. He presented with five episodes of vomiting followed by 4 episodes of hematemesis. Initially, conservative management failed to stop the bleeding in both cases; hence, an upper Gastrointestinal (GI) endoscopy was done, which diagnosed a MWT in both cases. Haemostasis was achieved in both cases using monopolar coagulation forceps. The use of monopolar coagulation forceps is a safe and effective tool in combination with other endoscopic modalities in managing significant bleeding from MWT. Monopolar coagulation forceps are much easier to use over the bipolar heater probe.
| Published in | American Journal of Internal Medicine (Volume 13, Issue 2) |
| DOI | 10.11648/j.ajim.20251302.11 |
| Page(s) | 11-15 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Mallory Weiss Tear, Obesity Hypoventilation Syndrome, Upper Gastrointestinal Bleeding, Endoscopic Hemostasis, Endoscopic Electrocoagulation
Forrest Stage | Re-bleeding risk |
|---|---|
Stage I Active bleeding | |
Ia Spurting haemorrhage | 90-100% |
Ib Oozing haemorrhage | 80-85% |
Stage II Signs of recent bleeding | |
IIa Non-bleeding visible vessel | 40-50% |
IIb Adherent clot on lesion | 20-30% |
IIc Hematin - covered lesion | 5% |
Stage III | |
Lesion without bleeding (flat spot, clean base) | ≤ 3% |
AUGIB | Acute upper Gastrointestinal Bleeding |
GI | Gastrointestinal |
ICU | Intensive Care Unit |
MPEC | Multipolar Electrocoagulation |
MWT | Mallory-Weiss Tear |
| [1] |
Kichler A, Jang S. Endoscopic Hemostasis for Non-Variceal Upper Gastrointestinal Bleeding: New Frontiers. Clin Endosc. 2019 Sep; 52(5): 401-406.
https://doi.org/10.5946/ce.2018.103 Epub 2019 Jul 16. |
| [2] | Antunes C, Tian C, Copelin II EL. Upper Gastrointestinal Bleeding. [Updated 2024 Aug 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: |
| [3] | Cherednikov EF, Kunin AA, Cherednikov EE, Moiseeva NS. The role of etiopathogenetic aspects in prediction and prevention of discontinuous-hemorrhagic (Mallory-Weiss) syndrome. EPMA J. 2016 Mar 20; 7(1): 7. |
| [4] |
Corral JE, Keihanian T, Kröner PT, Dauer R, Lukens FJ, Sussman DA. Mallory Weiss syndrome is not associated with hiatal hernia: a matched case-control study. Scand J Gastroenterol. 2017 Apr; 52(4): 462-464.
https://doi.org/10.1080/00365521.2016.1267793 Epub 2016 Dec 22. |
| [5] | Kortas DY, Haas LS, Simpson WG, Nickl NJ 3rd, Gates LK Jr. Mallory-Weiss tear: predisposing factors and predictors of a complicated course. Am J Gastroenterol. 2001 Oct; 96(10): 2863-5. |
| [6] | Hussein, M. S., Alfaraj, F. A., Alshabwi, A. D., Altheyab, A. A., Alhasan, K. T., Alghamdi, O. M., Ahmed, M. A. J. S., Alamri, A. A., Alhabeeb, M. T., Elsherif, A. A. and Zaki, L. S. (2021) “Evaluation and Management of Mallory – Weiss Syndrome: A Review”, Journal of Pharmaceutical Research International, 33(60A), pp. 788–794. |
| [7] | Yin, A., Li, Y., Jiang, Y., Liu, J., & Luo, H. (2012). Mallory–Weiss syndrome: Clinical and endoscopic characteristics. European Journal of Internal Medicine, 23(4), e92-e96. |
| [8] | Bharucha AE, Gostout CJ, Balm RK. Clinical and endoscopic risk factors in the Mallory-Weiss syndrome. Am J Gastroenterol. 1997 May; 92(5): 805-8. PMID: 9149189. |
| [9] | Kim JW, Kim HS, Byun JW, Won CS, Jee MG, Park YS, Baik SK, Kwon SO, Lee DK. Predictive factors of recurrent bleeding in Mallory-Weiss syndrome. Korean J Gastroenterol. 2005 Dec; 46(6): 447-54. PMID: 16371719. |
| [10] |
Medscape,“Mallory-Weiss Syndrome”. Available from:
https://emedicine.medscape.com/article/931141-treatment#d5 [Accessed 03 June 2025] |
| [11] | Nunoue T, Takenaka R, Hori K, et al. A randomized trial of monopolar soft-mode coagulation versus heater probe thermocoagulation for peptic ulcer bleeding. J Clin Gastroenterol. 2015; 4 9: 472–476. |
| [12] |
Prophylactic injection therapy is necessary for Forrest type 2b duodenal ulcers - Scientific Figure on ResearchGate. Available from:
https://www.researchgate.net/figure/Forrest-classification-for-upper-gastrointesti-nal-bleeding_tbl1_236185556 [accessed 17 Mar 2025] |
APA Style
Hassanein, M. F. K., Larue, K., Sani, A. B., Trotsky, D. R., Philoe, V., et al. (2025). Efficacy and Safety of Mono-polar Coagulation Forceps in the Repair of Large Mallory-Weiss Tear in Patients with Massive Upper Gastrointestinal Bleeding, 2 Case Reports. American Journal of Internal Medicine, 13(2), 11-15. https://doi.org/10.11648/j.ajim.20251302.11
ACS Style
Hassanein, M. F. K.; Larue, K.; Sani, A. B.; Trotsky, D. R.; Philoe, V., et al. Efficacy and Safety of Mono-polar Coagulation Forceps in the Repair of Large Mallory-Weiss Tear in Patients with Massive Upper Gastrointestinal Bleeding, 2 Case Reports. Am. J. Intern. Med. 2025, 13(2), 11-15. doi: 10.11648/j.ajim.20251302.11
AMA Style
Hassanein MFK, Larue K, Sani AB, Trotsky DR, Philoe V, et al. Efficacy and Safety of Mono-polar Coagulation Forceps in the Repair of Large Mallory-Weiss Tear in Patients with Massive Upper Gastrointestinal Bleeding, 2 Case Reports. Am J Intern Med. 2025;13(2):11-15. doi: 10.11648/j.ajim.20251302.11
@article{10.11648/j.ajim.20251302.11,
author = {Mahmoud Farouk Kamel Hassanein and Karine Larue and Abdul Basit Sani and Dhamarah Ranjan Trotsky and Vital Philoe and Nivetha Pandiyan and Sarka Viktorova},
title = {Efficacy and Safety of Mono-polar Coagulation Forceps in the Repair of Large Mallory-Weiss Tear in Patients with Massive Upper Gastrointestinal Bleeding, 2 Case Reports
},
journal = {American Journal of Internal Medicine},
volume = {13},
number = {2},
pages = {11-15},
doi = {10.11648/j.ajim.20251302.11},
url = {https://doi.org/10.11648/j.ajim.20251302.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajim.20251302.11},
abstract = {Mallory-Weiss tear (MWT) is a frequent cause of acute upper gastrointestinal (AUGI) bleeding and is defined as a longitudial superficial mucosal tear that usually occurs at the gastroesophageal junction. MWT is usually associated with increased abdominal pressure. 50 to 70% of patients diagnosed with MWT have a history of heavy alcohol intake. MWT usually presents with bright red or coffee-ground vomitus, black tar-like stool, signs of anemia, chest pain, abdominal pain, or signs of shock. Bleeding from MWT can stop on its own, however, significant bleeding may require endoscopic management. Here, we present 2 cases of life-threatening upper GI bleeding secondary to MWT. Case 1 is a 55-year-old male with known Obesity Hypoventilation Syndrome who presented with a violent cough and was initially admitted with respiratory distress. He became hypoxic and hypercarbic while on the ward and was transferred to the Intensive care Unit (ICU). A copious amount of fresh blood was drained upon passage of a nasogastric tube. The second case is a 31-year-old male who abuses alcohol. He presented with five episodes of vomiting followed by 4 episodes of hematemesis. Initially, conservative management failed to stop the bleeding in both cases; hence, an upper Gastrointestinal (GI) endoscopy was done, which diagnosed a MWT in both cases. Haemostasis was achieved in both cases using monopolar coagulation forceps. The use of monopolar coagulation forceps is a safe and effective tool in combination with other endoscopic modalities in managing significant bleeding from MWT. Monopolar coagulation forceps are much easier to use over the bipolar heater probe.
},
year = {2025}
}
TY - JOUR T1 - Efficacy and Safety of Mono-polar Coagulation Forceps in the Repair of Large Mallory-Weiss Tear in Patients with Massive Upper Gastrointestinal Bleeding, 2 Case Reports AU - Mahmoud Farouk Kamel Hassanein AU - Karine Larue AU - Abdul Basit Sani AU - Dhamarah Ranjan Trotsky AU - Vital Philoe AU - Nivetha Pandiyan AU - Sarka Viktorova Y1 - 2025/06/22 PY - 2025 N1 - https://doi.org/10.11648/j.ajim.20251302.11 DO - 10.11648/j.ajim.20251302.11 T2 - American Journal of Internal Medicine JF - American Journal of Internal Medicine JO - American Journal of Internal Medicine SP - 11 EP - 15 PB - Science Publishing Group SN - 2330-4324 UR - https://doi.org/10.11648/j.ajim.20251302.11 AB - Mallory-Weiss tear (MWT) is a frequent cause of acute upper gastrointestinal (AUGI) bleeding and is defined as a longitudial superficial mucosal tear that usually occurs at the gastroesophageal junction. MWT is usually associated with increased abdominal pressure. 50 to 70% of patients diagnosed with MWT have a history of heavy alcohol intake. MWT usually presents with bright red or coffee-ground vomitus, black tar-like stool, signs of anemia, chest pain, abdominal pain, or signs of shock. Bleeding from MWT can stop on its own, however, significant bleeding may require endoscopic management. Here, we present 2 cases of life-threatening upper GI bleeding secondary to MWT. Case 1 is a 55-year-old male with known Obesity Hypoventilation Syndrome who presented with a violent cough and was initially admitted with respiratory distress. He became hypoxic and hypercarbic while on the ward and was transferred to the Intensive care Unit (ICU). A copious amount of fresh blood was drained upon passage of a nasogastric tube. The second case is a 31-year-old male who abuses alcohol. He presented with five episodes of vomiting followed by 4 episodes of hematemesis. Initially, conservative management failed to stop the bleeding in both cases; hence, an upper Gastrointestinal (GI) endoscopy was done, which diagnosed a MWT in both cases. Haemostasis was achieved in both cases using monopolar coagulation forceps. The use of monopolar coagulation forceps is a safe and effective tool in combination with other endoscopic modalities in managing significant bleeding from MWT. Monopolar coagulation forceps are much easier to use over the bipolar heater probe. VL - 13 IS - 2 ER -
Department of Internal Medicine, Gastroenterology Division, Seychelles Hospital, Healthcare Agency, Seychelles
Department of Internal Medicine, Gastroenterology Division, Seychelles Hospital, Healthcare Agency, Seychelles
Department of Internal Medicine, Gastroenterology Division, Seychelles Hospital, Healthcare Agency, Seychelles
Department of Internal Medicine, Gastroenterology Division, Seychelles Hospital, Healthcare Agency, Seychelles
Department of Internal Medicine, Gastroenterology Division, Seychelles Hospital, Healthcare Agency, Seychelles
Department of Internal Medicine, Gastroenterology Division, Seychelles Hospital, Healthcare Agency, Seychelles
Department of Intensive Care, Seychelles Hospital, Healthcare Agency, Seychelles
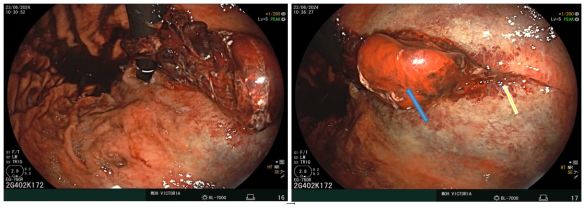
Figure 1. Retroversion view of the stomach shows blood at the fundus with giant sub-cardia blood clot (blue arrow) covering a large tear on the lesser curvature (Yellow arrows).
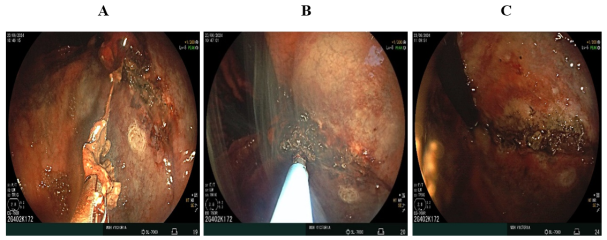
Figure 2. A. Separation of the blood clot, B. coagulating the base and edges of the tear using the monopolar coagulation forceps (the co-grasper), C. The tear after complete coagulation.

Figure 3. Closure of the tear using multiple through-the-scope clips (Blue arrows).
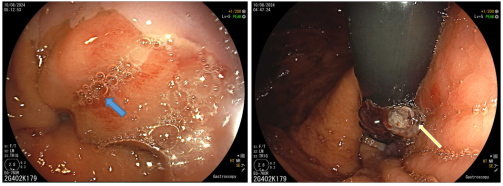
Figure 4. Mucosal Tear from the Esophageal side (Blue arrow) and retroversion view of the stomach shows a blood clot overlying a small sub-cardia tear (Yellow arrows).
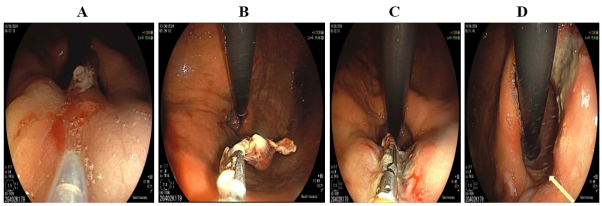
Figure 5. A. Injection of epinephrine, B. Separation of the blood clot using the monopolar coagulation forceps, C. Coagulating the base and edges of the tear, D. The tear after complete hemostasi), notice the Hiatus hernia ( Yellow arrow).
Information

