Purpose: Esophageal atresia (EA) and tracheoesophageal fistula (TEF) are rare anomalies in neonates that must be surgically repaired by esophageal reconstruction with or without ligation of the fistula. Recurrent tracheoesophageal fistula (rTEF) occurs in 3-15% of primary surgical repairs in esophageal atresia; it is associated with recurrent hospital admissions and up to 27% short term mortality. Dependable reparation very often proves difficult by standard surgical techniques. Using oesophageal fully covered self-expandable metal stents in adult patients yields a <50% efficacy and other endoscopic techniques such as occlusion by clips or glue show no better results. A minimally invasive alternative is the use of vascular plug septal occluders. We report the efficacy of endoscopic placement of a cardiac septal occluder (CSO) in a paediatric patient. Clinical case: A 12-year-old female with recurrent (rTEF) and refractory tracheoesophageal fistula (refTEF) was subjected to an refTEF closure procedure via endoscopic placement of a cardiac septal occlusion device. Conclusion: Debate regarding the gold standard of rTEF treatment closure a hot debate but flexible endoscopy is an accepted alternative. This report describes the successful fixing of a refTEF using a cardiac septal occluder. After four weeks follow up, no re-incidence of the tracheoesophageal fistula was detected. The results advocate for the endoscopic closure of refractory tracheoesophageal fistula with cardiac occluders in children thus establishing a promising therapeutical alternative in refTEF in paediatric population patients.
| Published in | American Journal of Pediatrics (Volume 10, Issue 2) |
| DOI | 10.11648/j.ajp.20241002.15 |
| Page(s) | 75-80 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Tracheoesophageal Fistula, Recurrent Tracheoesophageal Fistula, Refractory Tracheoesophageal Fistula, Endoscopic Interventional Therapies, Treatment, Children, Cardiac Septal Occluder
| [1] | Belle, A., Lorut, C., Lefebvre, A., et al. Amplatzer occluders for refractory esophago-respiratory fistulas: a case series. Endosc Int Open. 2021, 9(9): E1350-E1354, |
| [2] | Debourdeau, A., Gonzalez, J. M., Dutau, H., Benezech, A., Barthet, M. Endoscopic treatment of nonmalignant tracheoesophageal and bronchoesophageal fistula: results and prognostic factors for its success. Surg Endosc. 2019, 33(2): 549-556, |
| [3] | Traina, M., Amata, M., De Monte, L. et al. Chronic tracheoesophageal fistula successfully treated using Amplatzer septal occluder. Endoscopy. 2018, 50(12): 1236-1237, |
| [4] | Aworanti, O., Awadalla, S. Management of recurrent tracheoesophageal fistulas: a systematic review. Eur J Pediatr Surg. 2014, 24(5): 365-375, |
| [5] | Valero Mamani, R. J., Penchyna Grub, J., Blanco Rodriguez, G., Teyssier Morales, G., Pena Garcia, M. Endoscopic management of recurrent tracheoesophageal fistula with trichloroacetic acid in pediatric patients. Cir Pediatr. 2022, 35(3): 113-117, |
| [6] | Smithers, C. J., Hamilton, T. E,. Manfredi, M. A. et al. Categorization and repair of recurrent and acquired tracheoesophageal fistulae occurring after esophageal atresia repair. J Pediatr Surg. 2017, 52(3): 424-430, |
| [7] | Chauhan, SS., Long, JD. Management of Tracheoesophageal Fistulas in Adults. Curr Treat Options Gastroenterol. 2004, 7(1): 31-40, |
| [8] | Silva, JC., Braga, P., Coutinho, D., Fernades, C. Refractory tracheoesophageal fistula management with Amplatzer Occluder (R) placement. Rev Esp Enferm Dig. 2020, 112(9): 733-734, |
| [9] | Ersoz, H., Nazli, C. A new method of tracheoesophageal fistula treatment: Using an atrial septal defect occluder device for closure-The first Turkish experience. Gen Thorac Cardiovasc Surg. 2018, 66(11): 679-683, |
| [10] | van Lennep, M., Singendonk, M. M. J., Dall'Oglio, L., et al. Oesophageal atresia. Nat Rev Dis Primers. 2019, 5(1): 26, |
| [11] | Maj, C., Eberts, A., Schumacher, J., Dasmeh, P. Single-cell analysis reveals the spatial-temporal expression of genes associated with esophageal malformations. Sci Rep. 2024, 14(1): 3752, |
| [12] | Hilger, A. C., Halbritter, J., Pennimpede, T., et al. Targeted Resequencing of 29 Candidate Genes and Mouse Expression Studies Implicate ZIC3 and FOXF1 in Human VATER/VACTERL Association. Hum Mutat. 2015, 36(12): 1150-1154, |
| [13] | Sarkar, A., Hochedlinger, K. The sox family of transcription factors: versatile regulators of stem and progenitor cell fate. Cell Stem Cell. 2013, 12(1): 15-30, |
| [14] | Williamson, K. A., Hever, A. M., Rainger, J., et al. Mutations in SOX2 cause anophthalmia-esophageal-genital (AEG) syndrome. Hum Mol Genet. 2006, 15(9): 1413-1422, |
| [15] | Vergouwe, F. W., Gottrand, M., Wijnhoven, B. P., et al. Four cancer cases after esophageal atresia repair: Time to start screening the upper gastrointestinal tract. World J Gastroenterol. 2018, 24(9): 1056-1062, |
| [16] | Miller, PE., Arias, S., Lee, H., Yarmus, L., Feller-Kopman, D. Complications associated with the use of the amplatzer device for the management of tracheoesophageal fistula. Ann Am Thorac Soc. 2014, 11(9): 1507-1509, |
| [17] | Meier, JD., Sulman, CG., Almond, PS., Holinger, LD. Endoscopic management of recurrent congenital tracheoesophageal fistula: a review of techniques and results. Int J Pediatr Otorhinolaryngol. 2007, 71(5): 691-697, |
| [18] | Yankovic, F., Castillo, C., Saenz, R., Navarrete, C. [Endoscopic argon plasma coagulation in recurrent tracheoesophageal fistula. Clinical series and review of the literature]. Gastroenterol Hepatol. 2009, 32(9): 600-604, |
| [19] | Ling, Y., Sun, B., Li, J., et al. Endoscopic interventional therapies for tracheoesophageal fistulas in children: A systematic review. Front Pediatr. 2023, 11; 1121803, |
| [20] | Repici, A., Presbitero, P., Carlino, A., et al. First human case of esophagus-tracheal fistula closure by using a cardiac septal occluder (with video). Gastrointest Endosc. 2010, 71(4): 867-869, |
| [21] | Li, L., Wang, Y., Zhu, C., et al. Endoscopic closure of refractory upper GI-tracheobronchial fistulas with a novel occluder: a prospective, single-arm, single-center study (with video). Gastrointest Endosc. 2023, 97(5): 859-870e855, |
| [22] | Jalal, Z., Boudjemline, Y., Iriart, X., et al. Comparison of Two Percutaneous Atrial Septal Defect Occluders for Device Healing and Nickel Release in a Chronic Porcine Model. J Interv Cardiol. 2020, 2020: 8413831. |
| [23] | Siboni, S., D'Aiello, A. F., Chessa, M., Bonavina, L. Tailored endoscopic treatment of tracheo-oesophageal fistula using preoperative holographic assessment and a cardiac septal occluder. BMJ Case Rep. 2022, 15(3), |
APA Style
Alfredo, C. R., Antonio, S., Jesús, G. J., Alejandro, R. R., Servando, G. M., et al. (2024). Endoscopic Repair of Refractory Tracheoesophageal Fistula with a Cardiac Septal Occluder Device in a 12 Years-Old Patient. American Journal of Pediatrics, 10(2), 75-80. https://doi.org/10.11648/j.ajp.20241002.15
ACS Style
Alfredo, C. R.; Antonio, S.; Jesús, G. J.; Alejandro, R. R.; Servando, G. M., et al. Endoscopic Repair of Refractory Tracheoesophageal Fistula with a Cardiac Septal Occluder Device in a 12 Years-Old Patient. Am. J. Pediatr. 2024, 10(2), 75-80. doi: 10.11648/j.ajp.20241002.15
AMA Style
Alfredo CR, Antonio S, Jesús GJ, Alejandro RR, Servando GM, et al. Endoscopic Repair of Refractory Tracheoesophageal Fistula with a Cardiac Septal Occluder Device in a 12 Years-Old Patient. Am J Pediatr. 2024;10(2):75-80. doi: 10.11648/j.ajp.20241002.15
@article{10.11648/j.ajp.20241002.15,
author = {Castañeda-Ortiz Ramon Alfredo and Salgado-Sandoval Antonio and Gutiérrez-Escobedo José Jesús and Rodríguez-Izaguirre Rodrigo Alejandro and Gallardo-Luna Miguel Servando and Meza-Gallegos Analí and Flores-Arizmendi Ramon Alejandro and Montalvo-Aguilar Jesús Francisco and Terriquez-Rodríguez Sergio},
title = {Endoscopic Repair of Refractory Tracheoesophageal Fistula with a Cardiac Septal Occluder Device in a 12 Years-Old Patient
},
journal = {American Journal of Pediatrics},
volume = {10},
number = {2},
pages = {75-80},
doi = {10.11648/j.ajp.20241002.15},
url = {https://doi.org/10.11648/j.ajp.20241002.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20241002.15},
abstract = {Purpose: Esophageal atresia (EA) and tracheoesophageal fistula (TEF) are rare anomalies in neonates that must be surgically repaired by esophageal reconstruction with or without ligation of the fistula. Recurrent tracheoesophageal fistula (rTEF) occurs in 3-15% of primary surgical repairs in esophageal atresia; it is associated with recurrent hospital admissions and up to 27% short term mortality. Dependable reparation very often proves difficult by standard surgical techniques. Using oesophageal fully covered self-expandable metal stents in adult patients yields a <50% efficacy and other endoscopic techniques such as occlusion by clips or glue show no better results. A minimally invasive alternative is the use of vascular plug septal occluders. We report the efficacy of endoscopic placement of a cardiac septal occluder (CSO) in a paediatric patient. Clinical case: A 12-year-old female with recurrent (rTEF) and refractory tracheoesophageal fistula (refTEF) was subjected to an refTEF closure procedure via endoscopic placement of a cardiac septal occlusion device. Conclusion: Debate regarding the gold standard of rTEF treatment closure a hot debate but flexible endoscopy is an accepted alternative. This report describes the successful fixing of a refTEF using a cardiac septal occluder. After four weeks follow up, no re-incidence of the tracheoesophageal fistula was detected. The results advocate for the endoscopic closure of refractory tracheoesophageal fistula with cardiac occluders in children thus establishing a promising therapeutical alternative in refTEF in paediatric population patients.
},
year = {2024}
}
TY - JOUR T1 - Endoscopic Repair of Refractory Tracheoesophageal Fistula with a Cardiac Septal Occluder Device in a 12 Years-Old Patient AU - Castañeda-Ortiz Ramon Alfredo AU - Salgado-Sandoval Antonio AU - Gutiérrez-Escobedo José Jesús AU - Rodríguez-Izaguirre Rodrigo Alejandro AU - Gallardo-Luna Miguel Servando AU - Meza-Gallegos Analí AU - Flores-Arizmendi Ramon Alejandro AU - Montalvo-Aguilar Jesús Francisco AU - Terriquez-Rodríguez Sergio Y1 - 2024/04/28 PY - 2024 N1 - https://doi.org/10.11648/j.ajp.20241002.15 DO - 10.11648/j.ajp.20241002.15 T2 - American Journal of Pediatrics JF - American Journal of Pediatrics JO - American Journal of Pediatrics SP - 75 EP - 80 PB - Science Publishing Group SN - 2472-0909 UR - https://doi.org/10.11648/j.ajp.20241002.15 AB - Purpose: Esophageal atresia (EA) and tracheoesophageal fistula (TEF) are rare anomalies in neonates that must be surgically repaired by esophageal reconstruction with or without ligation of the fistula. Recurrent tracheoesophageal fistula (rTEF) occurs in 3-15% of primary surgical repairs in esophageal atresia; it is associated with recurrent hospital admissions and up to 27% short term mortality. Dependable reparation very often proves difficult by standard surgical techniques. Using oesophageal fully covered self-expandable metal stents in adult patients yields a <50% efficacy and other endoscopic techniques such as occlusion by clips or glue show no better results. A minimally invasive alternative is the use of vascular plug septal occluders. We report the efficacy of endoscopic placement of a cardiac septal occluder (CSO) in a paediatric patient. Clinical case: A 12-year-old female with recurrent (rTEF) and refractory tracheoesophageal fistula (refTEF) was subjected to an refTEF closure procedure via endoscopic placement of a cardiac septal occlusion device. Conclusion: Debate regarding the gold standard of rTEF treatment closure a hot debate but flexible endoscopy is an accepted alternative. This report describes the successful fixing of a refTEF using a cardiac septal occluder. After four weeks follow up, no re-incidence of the tracheoesophageal fistula was detected. The results advocate for the endoscopic closure of refractory tracheoesophageal fistula with cardiac occluders in children thus establishing a promising therapeutical alternative in refTEF in paediatric population patients. VL - 10 IS - 2 ER -
Departament of Pediatric Digestive and Respiratory Endoscopic, National Medical Center “20 de Noviembre” ISSSTE, Ciudad de Mexico, Mexico
Departament of Congenital Cardioapathy and Intervention Cardiology, National Medical Center “20 de Noviembre”, ISSSTE, Ciudad de Mexico, Mexico
Departament of Pediatric Surgery, National Medical Center “20 de Noviembre” ISSSTE, Ciudad de Mexico, Mexico
Departament of Pediatric Digestive and Respiratory Endoscopic, National Medical Center “20 de Noviembre” ISSSTE, Ciudad de Mexico, Mexico
Departament of Pediatric Digestive and Respiratory Endoscopic, National Medical Center “20 de Noviembre” ISSSTE, Ciudad de Mexico, Mexico
Departament of Pediatric Digestive and Respiratory Endoscopic, National Medical Center “20 de Noviembre” ISSSTE, Ciudad de Mexico, Mexico
Departament of Congenital Cardioapathy and Intervention Cardiology, National Medical Center “20 de Noviembre”, ISSSTE, Ciudad de Mexico, Mexico
Departament of Congenital Cardioapathy and Intervention Cardiology, National Medical Center “20 de Noviembre”, ISSSTE, Ciudad de Mexico, Mexico
Departament of Pediatric Surgery, National Medical Center “20 de Noviembre” ISSSTE, Ciudad de Mexico, Mexico
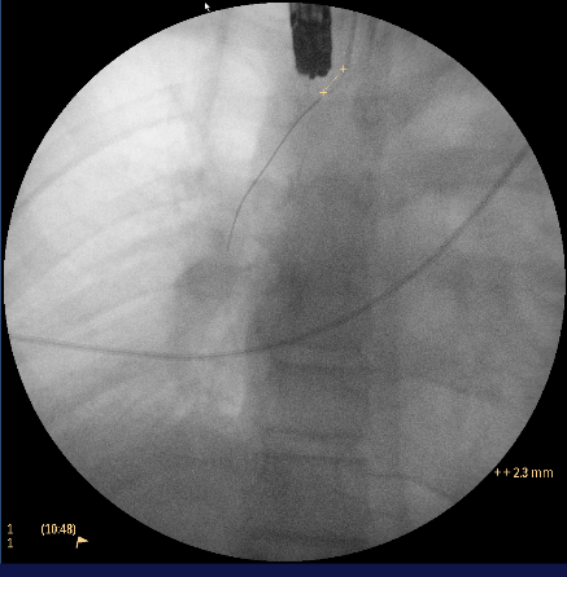
Figure 1. Fistula length by fluoroscopy.
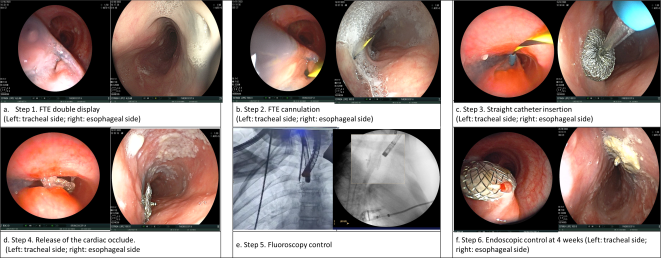
Figure 2. Endoscopic procedure. Placement of cardiac septal occluder step by step.
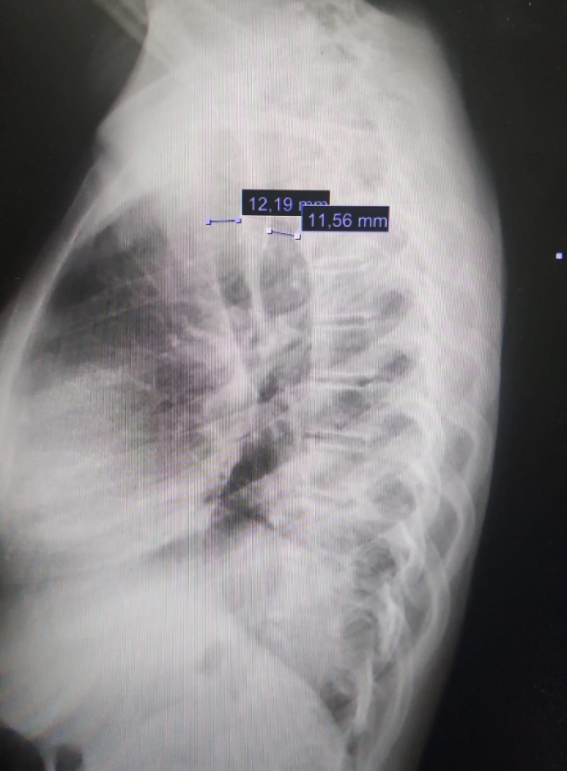
Figure 3. Lateral chest x-ray with measurement of the tracheal lumen 12.19mm and esophageal lumen 11.56mm, cardiac occluder in adequate position.
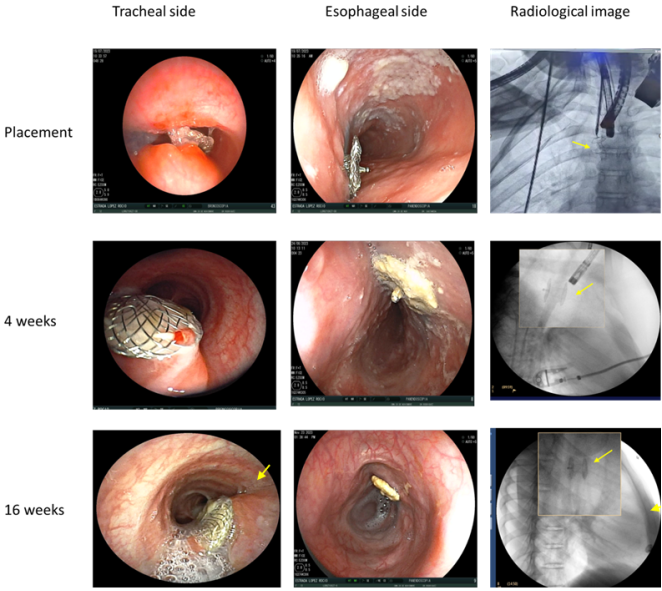
Figure 4. Endoscopic and fluoroscopic follow-up of the patient. Healing tissue is observed at week 16 (see arrow). Radiological images show the proper position of the cardiac occluder (see arrow).
Information

