Introduction: Cerebellitis is an inflammatory pathology of cerebellar structures more common in children, frequently of post-infectious origin or following vaccination, seldom during a viral or bacterial infection. Ataxia is most frequently caused by dysfunction of the complex circuitry connecting the cerebellum, basal ganglia and cerebral cortex. Results: We report the case of 2 patients aged 3 and 10 years presenting acute cerebellitis of infectious origin: Ataxic syndrome associated with balance disorders and speech disorders and fever. The evolution was quickly favorable with corticosteroid therapy and proprioceptive physiotherapy. The absence of fatalities in our case report suggests early diagnosis, and steroid treatment can increase the chance of recovery. Discussion: Clinical presentations are deceptive and variable with cerebellar symptoms of acute kinetic and static ataxia with inflammatory signs. The treatment is based on steroids when symptoms are moderate to severe. Antimicrobial therapy should always be considered, because ataxia can be a presenting sign of both viral encephalitis and bacterial meningitis. The prognosis for acute cerebellitis is generally favorable. The courses vary from what is commonly a benign and self-limiting disease to what occasionally is fulminant disease resulting in several cerebellar damage or even sudden death. Conclusion: Recognizing ataxia in children can be difficult, which is why a lumbar punction should be considered if infectious cerebellitis is suspected. Most people fully recover, however there is a risk of lasting disability.
| Published in | American Journal of Pediatrics (Volume 10, Issue 3) |
| DOI | 10.11648/j.ajp.20241003.11 |
| Page(s) | 112-116 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Lumbar Punction, Magnetic Resonance Imaging, Cerebellitis, Acute Cerebellar Ataxia
Observation | Patient N°1 | Patient N°2 |
|---|---|---|
Age / Gender | 3 Years /Girl | 10 Years /Girl |
Clinical | Disorder Walking Right Paraparesis Fever at 39° (5 days) | CITH syndrome: helmet headache + jet vomiting, Fever at 38.5°. Ataxic walking (7 days) |
LCR | White cells = 233 (95% Lympho) Negative CRP | White cells = 40 (80% Lympho) CRP at 38; PCR: Haemophilus Influenzae. |
CT / Brain MRI | Normal Brain CT | Cerebral CT: cerebellitis with tonsillar ptosis Brain MRI: Infectious cerebellitis of viral origin. |
Treatment | Méthylprednisone Proprioceptive Physiotherapy | Méthylprednisone Proprioceptive Physiotherapy |
Evolution | Favorable | Favorable |
MRI | Magnetic Resonance Imagery |
V4 | Fourth Ventricle |
CSF | Cerebrospinal Fluid |
PCR | Polymerase Chain Reaction |
CRP | C reactive Protein |
ENMG | Electroneuromyogram |
ROT | Osteotendinous Reflex |
Brain CT | Brain Computed Tomography |
EMAD | Acute Disseminated Encephalomyelitis |
| [1] | Emelifeonwu JA, Shetty J, Kaliaperumal C, et al. Acute cerebellitis in children: a variable clinical entity. J Child Neurol. 2018; 33: 675-684. |
| [2] | Bakshi R, Bates VE, Kinkel PR, Mechtler LL, Kinkel WR. Magnetic resonance imaging findings in acute cerebellitis. Clin Imaging 1998; 22: 79–85. |
| [3] | Fenichel GM. Clinical Pediatric Neurology—A Signs and Symptoms Approach. Philadelphia, PA: WB Saunders Company; 1993. |
| [4] | Takanashi J, Miyamoto T, Ando N, et al. Clinical and radiological features of rotavirus cerebellitis. AJNR Am J Neuroradiol. 2010; 31: 1591-1595. |
| [5] | Mahajan SK, Sharma S, Kaushik M, et al. Scrub Typhus Presenting as Acute Cerebellitis. J Assoc Physicians India. 2016; 64: 69-70. PMID: 27730787. |
| [6] | Komatsu H, Kuroki S, Shimizu Y, Takada H, Takeuchi Y. Mucoplasma pneumoniae meningoencephalitis and cerebellitis with antiganglioside antibodies. Pediatr Neuro 1998; 18: 160-164. |
| [7] |
Sawaishi Y, Takahashi I, Hirayama Y, Abe T, Mizutani M, Hirai K, Takada G. Acute cerebellitis caused by Coxiella burnetii. Ann Neurol 1999; 45: 124-127.
https://doi.org/10.1002/1531-8249(199901)45:1<124::AID-ART19>3.0.CO;2-B |
| [8] | Schmahmann JD, Weilburg JB, Sherman JC. The neuropsychiatry of the cerebellum - insights from the clinic. Cerebellum. 2007; 6(3): 254-67. |
| [9] | Iester A, Alpigiani MG, Franzone G, Cohen A, Puleo MG, Tortori-Donati P. Magnetic resonance imaging in right hemisphere cerebellitis associated with homola- téral hemiparesis. Child’s Nerv Syst 1995; 11: 118-120. |
| [10] | Sékhara T, Christophe C, Christiaens F, Dan B. Hémicerebellite post-infectieuse [Postinfectious hemicerebellitis]. Rev Neurol (Paris). 2001 Jan; 157(1): 84-6. French. PMID: 11240553. |
| [11] | Roulet Perez E, Maeder P, Cotting J, Eskenazy-Cottier AC, Deonna T. Acute fatal parainfections cerebellar swelling in two children. A rare or an over looked situation? Neuropediatrics 1993; 24: 346-351. |
| [12] | V. Soussan, B. Husson, M. Tardieu, Description et valeur pronostique des anomalies cérébelleuses observées en résonance magnétique nucléaire au cours d’ataxies aiguës inflammatoires graves. Arch Pediatr 2003; 10: 604-607. |
| [13] | Barkovitch AJ. Infections of the nervous system In: Barko- vitch AJ. Ed Pediatric Neuroimaging. Philadelphia, PA: Lip- pincott – Raven; 2000; 11: 748-749. |
| [14] | De Bruecker Y, Claus F, Demaerel P, Ballaux F, Sciot R, Lagae L, Buyse G, Wilms G. MRI findings in acute cerebellitis. Eur Radiol 2004; 14: 1478-1483. |
| [15] | Horowitz MB, Pang D, Hirsch W. Acute cerebellitis: case report and review. Pediatr Neurosurg 1991; 17: 142-145. |
| [16] | Kato Z, Shimozawa N, Kokuzawa J, Iwamura M, Hirata T, Yamagishi A, Hayashi T, Motoyoshi T, Kondo N. Magnetic resonance imaging of acute cerebellar ataxia: report of a case with gadolinium enhancement and review of the literature. Acta Pediatr Jpn 1998; 40: 138-142. |
| [17] | Asenbauer B, McConachie NS, Allcutt D, Farrell MA, King MD. Acute near-fatal parainfectious cerebellar swelling with favorable outcome. Neuropediatrics 1997; 28: 122–125. |
| [18] | Schwartz JF. Ataxia in bacterial meningitis. Neurology. 1972; 22: 1071-1074. |
| [19] | Bodegas I, Martínez-Bermejo A, García de Miguel MJ, López-Martín V, de José MI, García-Hortelano J. Encefalitis de tronco cerebral en la infancia [Brain stem encephalitis in childhood]. Rev Neurol. 1998 Jul; 27(155): 71-3. Spanish. PMID: 9674029. |
| [20] | Connolly AM, Dodson WE, Prensky AL, et al. Course and outcome of acute cerebellar ataxia. Ann Neurol 1994; 35: 673–9. |
APA Style
Boussaid, I., Chahid, I., Harim, F., Abkari, A., Bentaleb, D., et al. (2024). Infectious Cerebellitis Rare Entity About Two Cases. American Journal of Pediatrics, 10(3), 112-116. https://doi.org/10.11648/j.ajp.20241003.11
ACS Style
Boussaid, I.; Chahid, I.; Harim, F.; Abkari, A.; Bentaleb, D., et al. Infectious Cerebellitis Rare Entity About Two Cases. Am. J. Pediatr. 2024, 10(3), 112-116. doi: 10.11648/j.ajp.20241003.11
AMA Style
Boussaid I, Chahid I, Harim F, Abkari A, Bentaleb D, et al. Infectious Cerebellitis Rare Entity About Two Cases. Am J Pediatr. 2024;10(3):112-116. doi: 10.11648/j.ajp.20241003.11
@article{10.11648/j.ajp.20241003.11,
author = {Imane Boussaid and Imane Chahid and Fatima Harim and Abdelhak Abkari and Daoud Bentaleb and Wilhem Gilius},
title = {Infectious Cerebellitis Rare Entity About Two Cases
},
journal = {American Journal of Pediatrics},
volume = {10},
number = {3},
pages = {112-116},
doi = {10.11648/j.ajp.20241003.11},
url = {https://doi.org/10.11648/j.ajp.20241003.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20241003.11},
abstract = {Introduction: Cerebellitis is an inflammatory pathology of cerebellar structures more common in children, frequently of post-infectious origin or following vaccination, seldom during a viral or bacterial infection. Ataxia is most frequently caused by dysfunction of the complex circuitry connecting the cerebellum, basal ganglia and cerebral cortex. Results: We report the case of 2 patients aged 3 and 10 years presenting acute cerebellitis of infectious origin: Ataxic syndrome associated with balance disorders and speech disorders and fever. The evolution was quickly favorable with corticosteroid therapy and proprioceptive physiotherapy. The absence of fatalities in our case report suggests early diagnosis, and steroid treatment can increase the chance of recovery. Discussion: Clinical presentations are deceptive and variable with cerebellar symptoms of acute kinetic and static ataxia with inflammatory signs. The treatment is based on steroids when symptoms are moderate to severe. Antimicrobial therapy should always be considered, because ataxia can be a presenting sign of both viral encephalitis and bacterial meningitis. The prognosis for acute cerebellitis is generally favorable. The courses vary from what is commonly a benign and self-limiting disease to what occasionally is fulminant disease resulting in several cerebellar damage or even sudden death. Conclusion: Recognizing ataxia in children can be difficult, which is why a lumbar punction should be considered if infectious cerebellitis is suspected. Most people fully recover, however there is a risk of lasting disability.
},
year = {2024}
}
TY - JOUR T1 - Infectious Cerebellitis Rare Entity About Two Cases AU - Imane Boussaid AU - Imane Chahid AU - Fatima Harim AU - Abdelhak Abkari AU - Daoud Bentaleb AU - Wilhem Gilius Y1 - 2024/07/08 PY - 2024 N1 - https://doi.org/10.11648/j.ajp.20241003.11 DO - 10.11648/j.ajp.20241003.11 T2 - American Journal of Pediatrics JF - American Journal of Pediatrics JO - American Journal of Pediatrics SP - 112 EP - 116 PB - Science Publishing Group SN - 2472-0909 UR - https://doi.org/10.11648/j.ajp.20241003.11 AB - Introduction: Cerebellitis is an inflammatory pathology of cerebellar structures more common in children, frequently of post-infectious origin or following vaccination, seldom during a viral or bacterial infection. Ataxia is most frequently caused by dysfunction of the complex circuitry connecting the cerebellum, basal ganglia and cerebral cortex. Results: We report the case of 2 patients aged 3 and 10 years presenting acute cerebellitis of infectious origin: Ataxic syndrome associated with balance disorders and speech disorders and fever. The evolution was quickly favorable with corticosteroid therapy and proprioceptive physiotherapy. The absence of fatalities in our case report suggests early diagnosis, and steroid treatment can increase the chance of recovery. Discussion: Clinical presentations are deceptive and variable with cerebellar symptoms of acute kinetic and static ataxia with inflammatory signs. The treatment is based on steroids when symptoms are moderate to severe. Antimicrobial therapy should always be considered, because ataxia can be a presenting sign of both viral encephalitis and bacterial meningitis. The prognosis for acute cerebellitis is generally favorable. The courses vary from what is commonly a benign and self-limiting disease to what occasionally is fulminant disease resulting in several cerebellar damage or even sudden death. Conclusion: Recognizing ataxia in children can be difficult, which is why a lumbar punction should be considered if infectious cerebellitis is suspected. Most people fully recover, however there is a risk of lasting disability. VL - 10 IS - 3 ER -
Neuropediatrics Unit, Paediatrics’ 3, Children’s Hospital A. Harouchi, Casablanca, Morocco
Neuropediatrics Unit, Paediatrics’ 3, Children’s Hospital A. Harouchi, Casablanca, Morocco
Neuropediatrics Unit, Paediatrics’ 3, Children’s Hospital A. Harouchi, Casablanca, Morocco
Neuropediatrics Unit, Paediatrics’ 3, Children’s Hospital A. Harouchi, Casablanca, Morocco
Pediatrics Radiology Unit, Radiology, Children’s Hospital A. Harouchi, Casablanca, Morocco
Pediatrics Radiology Unit, Radiology, Children’s Hospital A. Harouchi, Casablanca, Morocco
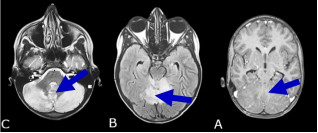
Figure 1. Magnetic resonance imaging (MRI) axial cut. Patient 2. (A) T1 injected, (B) T2 FLAIR Sequence, (C) T2 Sequence. Bilateral and asymmetrical diffuse cerebellar cortical thickening without systematized character, in discrete T1 hypo signal, T2 hypersignal and FLAIR, with discrete meningeal contrast taking in front of it, a mass effect on the brainstem and V4 without upstream dilation and ptosis of the cerebellar tonsils at the level of the Mc Rae line.
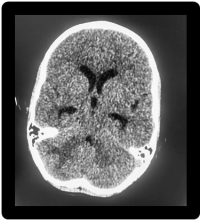
Figure 2. Brain CT scan. Helical acquisition without contrast injection. Ranges of right cerebellar hypodensities repressing V4 with ptosis of cerebellar tonsils.
Information

