The combination of pulmonary tuberculosis and type 1 diabetes is a significant public health problem, especially in developing countries, where the incidence of both diseases is rising sharply. According to the World Health Organization (WHO), by 2022, 23% of tuberculosis cases will be in Africa. Morocco is one of the countries with a medium incidence of tuberculosis. The Ministry of Health has launched a national strategic plan for the prevention and control of tuberculosis. However, there is no national study on the prevalence of tuberculosis in diabetic children in Morocco. Several studies in the literature have investigated the specifics of this association, and have shown that there is a two-way association between tuberculosis and type 1 diabetes. Latent tuberculosis is most common in diabetic children, while active tuberculosis can give rise to severe and atypical presentations. In this study 2 cases have been reported of type 1 diabetes associated with pulmonary tuberculosis, of varying severity, in a 15-year-old child known to be diabetic and an 18-month-old infant with inaugural diabetes, in order to determine the clinical, paraclinical, therapeutic and evolutionary particularities of tuberculosis in these children.
| Published in | American Journal of Pediatrics (Volume 10, Issue 3) |
| DOI | 10.11648/j.ajp.20241003.18 |
| Page(s) | 152-157 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Diabetes Type 1, Pulmonary Tuberculosis, Mycobacterium Tuberculosis, Glycemic Imbalance
T1D | Type 1 Diabetes |
MT | Mycobacterium Tuberculosis |
CT | Computed Tomography |
SAP | Self-Pulsing Syringe |
NTCP | National Tuberculosis Control Program |
R | Rifampicin |
H | Isoniazid |
Z | Pyrazinamide |
E | Ethambutol |
HbA1c | Glycated Hemoglobin |
WHO | World Health Organization |
| [1] | Shen TC, Lin CL, Wei CC. Increased risk of tuberculosis in patients with type 1 diabetes mellitus: results from a population-based cohort study in Taiwan. Medicine (Baltimore). 2014 Oct; 93(16): e96. |
| [2] | FOE-ES, Joseph Ro, KENMOE. Diabetes mellitus and tuberculosis, a systematic review and meta-analysis with sensitivity analysis for studies comparable for confounders. PLoS One, 2021, vol. 16, no 12, p. e0261246. |
| [3] | HADJI, W., AMAR, A., ZADOUK, H.. P139 Les particularités de la tuberculose pulmonaire chez les diabètiques [The particularities of pulmonary tuberculosis in diabetics]. Diabetes & Metabolism, 2012, vol. 38, p. A64. |
| [4] | Majaliwa ES, Muze K, Godfrey E, Latent tuberculosis in children and youth with type 1 diabetes mellitus in Dar es Salaam, Tanzania: a cross section survey. BMC Infect Dis. 2023 Oct 3 23) 23(1): 740. |
| [5] |
PLAN STRATÉGIQUE NATIONAL POUR LA PRÉVENTION ET LE CONTRÔLE DE LA TUBERCULOSE AU MAROC 2024-2030. [NATIONAL STRATEGIC PLAN FOR THE PREVENTION AND CONTROL OF TUBERCULOSIS IN MOROCCO 2024-2030 Page 15. URL
https://www.sante.gov.ma (accessed 06 july 2024) |
| [6] | Hayashi S, Chandramohan D. Risk of active tuberculosis among people with diabetes mellitus: systematic review and meta-analysis. Trop Med Int Health. 2018 Oct; 23(10): 105.1070. |
| [7] | Casqueiro J, Alves C. Infections in patients with diabetes mellitus: A review of pathogenesis. Indian J Endocrinol Metab. 2012 Mar; 16 Suppl 1(Suppl1): S27-36. |
| [8] | SHIN HJ, KIM, TO, OH HJ. Impact of diabetes mellitus on in determinate results of the QuantiFERON TB Gold In-Tube test: A propensity score matching analysis. PLoS One, 2017, vol. 12, no 7, p. e0181887. |
| [9] | Walsh MC, Camerlin AJ, Miles R. The sensitivity of interferon-gamma release assays is not compromised in tuberculosis patients with diabetes. Int J Tuberc Lung Dis. 2011 Feb; 15(2): 179-84. |
| [10] | FAURHOLT J, Daniel A, Martine G, et al. Diabetes is associated with lower tuberculosis antigen-specific interferon gamma release in Tanzanian tuberculosis patients and non-tuberculosis controls. Scandinavian journal of infectious diseases, 2014, vol. 46, no 5, p. 384-391. |
| [11] | Hassan H, Komba Y, Etoughe F. The contribution of the Xpert MTB / RIF test in the diagnosis and treatment of tuberculosis. Rev Mali Infect Microbiol 2021, Vol 16 N°2. |
| [12] | BAGAYOKO K, Samake EKZ, AHOU TD, et al. Accès universel aux tests de sensibilité aux antituberculeux: cas du GeneXpert à Abidjan [Universal access to anti-tuberculosis drug susceptibility testing: the case of GeneXpert in Abidjan]. Revue des Maladies Respiratoires Actualités, 2021, vol. 13, no 1, p. 232. |
| [13] | WATANABE N, SAITO K, KIRITANI A. A case of invasive pulmonary aspergillosis diagnosed by transbronchial lung biopsy during treatment for diabetic ketoacidosis in a type 1 diabetic patient. Journal of Infection and Chemotherapy, 2020, vol. 26, no 2, p. 274-278. |
| [14] | BLAIZE M, JABET A, PIARROUX R. Infections fongiques pulmonaires (à l’exception de la pneumocystose) [Pulmonary fungal infections (except pneumocystis)]. Revue Francophone des Laboratoires, 2024, vol. 2024, no 559, p. 51-62. |
| [15] | Miora MA, Arielle R, Rija. Epidemiologic-clinical, biological and radiological features of pulmonary tuberculosis in patients with diabetes in Antananarivo, Madagascar. The Pan African Medical Journal, 2022, vol. 42, p. 49-49. |
| [16] | GETAHUN, Haileyesus, MATTEELLI, Alberto, ABUBAKAR, Ibrahim, et al. Management of latent Mycobacterium tuberculosis infection: WHO guidelines for low tuberculosis burden countries. European Respiratory Journal, 2015, vol. 46, no 6, p. 1563-1576. |
| [17] | Gautam S, Shrestha N, Mahato S. Diabetes among tuberculosis patients and its impact on tuberculosis treatment in South Asia: a systematic review and meta-analysis. Sci Rep. 2021 Jan 22; 11(1): 2113. |
APA Style
Bouarab, I., Yakine, F. Z., Tyhami, S., Inboui, F. Z. A., Slaoui, B. (2024). The Particularities of Pulmonary Tuberculosis in Children with Type 1 Diabetes: About 2 Cases. American Journal of Pediatrics, 10(3), 152-157. https://doi.org/10.11648/j.ajp.20241003.18
ACS Style
Bouarab, I.; Yakine, F. Z.; Tyhami, S.; Inboui, F. Z. A.; Slaoui, B. The Particularities of Pulmonary Tuberculosis in Children with Type 1 Diabetes: About 2 Cases. Am. J. Pediatr. 2024, 10(3), 152-157. doi: 10.11648/j.ajp.20241003.18
AMA Style
Bouarab I, Yakine FZ, Tyhami S, Inboui FZA, Slaoui B. The Particularities of Pulmonary Tuberculosis in Children with Type 1 Diabetes: About 2 Cases. Am J Pediatr. 2024;10(3):152-157. doi: 10.11648/j.ajp.20241003.18
@article{10.11648/j.ajp.20241003.18,
author = {Ilham Bouarab and Fatima Zahra Yakine and Salma Tyhami and Fatim Zahra Alaoui Inboui and Bouchra Slaoui},
title = {The Particularities of Pulmonary Tuberculosis in Children with Type 1 Diabetes: About 2 Cases
},
journal = {American Journal of Pediatrics},
volume = {10},
number = {3},
pages = {152-157},
doi = {10.11648/j.ajp.20241003.18},
url = {https://doi.org/10.11648/j.ajp.20241003.18},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20241003.18},
abstract = {The combination of pulmonary tuberculosis and type 1 diabetes is a significant public health problem, especially in developing countries, where the incidence of both diseases is rising sharply. According to the World Health Organization (WHO), by 2022, 23% of tuberculosis cases will be in Africa. Morocco is one of the countries with a medium incidence of tuberculosis. The Ministry of Health has launched a national strategic plan for the prevention and control of tuberculosis. However, there is no national study on the prevalence of tuberculosis in diabetic children in Morocco. Several studies in the literature have investigated the specifics of this association, and have shown that there is a two-way association between tuberculosis and type 1 diabetes. Latent tuberculosis is most common in diabetic children, while active tuberculosis can give rise to severe and atypical presentations. In this study 2 cases have been reported of type 1 diabetes associated with pulmonary tuberculosis, of varying severity, in a 15-year-old child known to be diabetic and an 18-month-old infant with inaugural diabetes, in order to determine the clinical, paraclinical, therapeutic and evolutionary particularities of tuberculosis in these children.
},
year = {2024}
}
TY - JOUR T1 - The Particularities of Pulmonary Tuberculosis in Children with Type 1 Diabetes: About 2 Cases AU - Ilham Bouarab AU - Fatima Zahra Yakine AU - Salma Tyhami AU - Fatim Zahra Alaoui Inboui AU - Bouchra Slaoui Y1 - 2024/08/27 PY - 2024 N1 - https://doi.org/10.11648/j.ajp.20241003.18 DO - 10.11648/j.ajp.20241003.18 T2 - American Journal of Pediatrics JF - American Journal of Pediatrics JO - American Journal of Pediatrics SP - 152 EP - 157 PB - Science Publishing Group SN - 2472-0909 UR - https://doi.org/10.11648/j.ajp.20241003.18 AB - The combination of pulmonary tuberculosis and type 1 diabetes is a significant public health problem, especially in developing countries, where the incidence of both diseases is rising sharply. According to the World Health Organization (WHO), by 2022, 23% of tuberculosis cases will be in Africa. Morocco is one of the countries with a medium incidence of tuberculosis. The Ministry of Health has launched a national strategic plan for the prevention and control of tuberculosis. However, there is no national study on the prevalence of tuberculosis in diabetic children in Morocco. Several studies in the literature have investigated the specifics of this association, and have shown that there is a two-way association between tuberculosis and type 1 diabetes. Latent tuberculosis is most common in diabetic children, while active tuberculosis can give rise to severe and atypical presentations. In this study 2 cases have been reported of type 1 diabetes associated with pulmonary tuberculosis, of varying severity, in a 15-year-old child known to be diabetic and an 18-month-old infant with inaugural diabetes, in order to determine the clinical, paraclinical, therapeutic and evolutionary particularities of tuberculosis in these children. VL - 10 IS - 3 ER -
Department of Childhood Diseases, Abderrahim Harouchi Mother-Child Hospital, Casablanca, Morocco
Department of Childhood Diseases, Abderrahim Harouchi Mother-Child Hospital, Casablanca, Morocco
Department of Childhood Diseases, Abderrahim Harouchi Mother-Child Hospital, Casablanca, Morocco
Department of Childhood Diseases, Abderrahim Harouchi Mother-Child Hospital, Casablanca, Morocco
Department of Childhood Diseases, Abderrahim Harouchi Mother-Child Hospital, Casablanca, Morocco
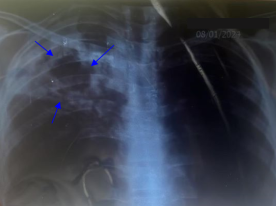
Figure 1. A thoracic radiograph revealed an interstitial syndrome and an excavated pulmonary opacity.
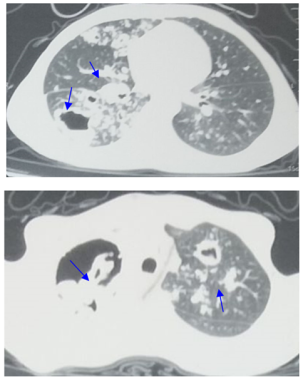
Figure 2. Thoracic CT scan showing multiple lesions excavated from the two upper lobes of the lung, the largest of which is in the right upper lobe measuring approximately 64×48 mm. Hyperdense material was seen in two of these cavities, bilaterally, measuring 24×14 mm on the right and 25×16 mm on the left. Multiple scattered micronodular and reticular infiltrates are present in both lung fields, giving the appearance of a tree-in-bud pattern. Scattered bilateral cylindrical and cystic foci of bronchiectasis associated with peribronchovascular thickening, some of which are the site of mucoid impaction. Multiple basal cervical and mediastinal adenopathies, the largest of which is subcarinal, measuring 10.5 mm in its minor axis.
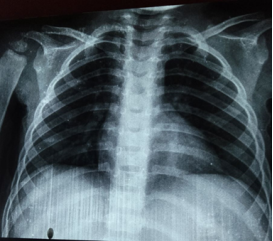
Figure 3. Front chest X-ray without abnormalities.
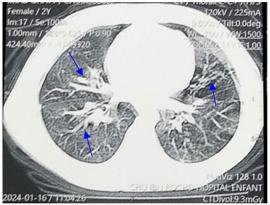
Figure 4. Thoracic CT scan showing retractile moniliform bronchiectasis of the middle lobe and left posterobasal lobes, associated with peribronchial thickening, with left posterobasal branching micronodules, pre-aortic calcified nodes, lingular and middle lobar band atelectasis.
Information

