Abstract
Introduction: Airway remodelling in children with severe recurrent episodes of bronchial obstruction starts very early, from preschool age – a period in which the diagnosis of asthma is not yet confirmed. Assessing these early structural changes presents a challenge in clinical practice. Due to the limitations of invasive methods, reliable noninvasive markers of these changes are sought. Galectin-3 (Gal-3), a regulator of inflammatory and fibrotic processes, and Krebs von den Lungen-6 (KL-6), a marker of alveolar epithelial damage, are considered as indicators of lung remodelling. Methods: Forty-eight children were studied: 26 children under 4 years of age with recurrent episodes of wheezing (RW) and 22 with cystic fibrosis (CF). Children with RW were divided into two subgroups: those with a low frequency (≤3 episodes/year) and those with a high frequency (>6 episodes/year) of bronchoobstructive symptoms. CF patients were stratified according to genotype (ΔF508 homozygous or heterozygous), and all underwent computed tomography (HRCT). Serum Gal-3 and KL-6 levels were measured by the ELISA method. The correlation between Gal-3 and KL-6 and clinical severity in children with recurrent wheezing at preschool age, and between Gal-3 and KL-6 and radiologically confirmed structural lung changes in children with cystic fibrosis, was assessed. Results: Elevated Gal-3 levels were found in children with RW from infancy. Although the differences in median Gal-3 levels did not reach statistical significance in the two RW subgroups, children with a high frequency of wheezing were 1.76 times more likely to have elevated Gal-3 (>26 ng/mL) compared to those with a low frequency of RW (p = 0.02). In CF, Gal-3 levels were significantly higher in children with confirmed structural lung disease on HRCT compared to those without pathological changes (38.35 vs. 11.63 ng/mL, p = 0.001). The highest Gal-3 values were found in ΔF508 homozygous patients with bronchiectasis. KL-6 levels remained within the normal range for the pediatric population across all groups and did not correlate with the frequency of bronchoobstructive manifestations, genotype, or CT findings. Conclusion: Galectin-3 is a reliable biomarker for pediatric pulmonology practice, reflecting early pulmonary changes in children with frequent recurrent bronchoobstructive episodes and a risk of persistent manifestations, and it correlates with structural damage in cystic fibrosis patients. KL-6 has no diagnostic value in the early stages of pulmonary pathology.
Keywords
Galectin-3, KL-6, Recurrent Wheezing, Cystic Fibrosis, Airway Remodelling
1. Introduction
Recurrent episodes of wheezing (RW) in preschool age represent a heterogeneous syndrome. In some children, these episodes are transient, virus-induced bronchial obstructions, while in others, they may be the first manifestation of a persistent asthmatic phenotype with early airway remodelling
| [1] | Saglani S, Payne DN, Zhu J, et al. Early detection of airway wall remodelling and eosinophilic inflammation in preschool wheezers. Am J Respir Crit Care Med. 2007; 176(9): 858-864.
https://doi.org/10.1164/rccm.200702-212OC |
| [2] | Lezmi G, Gosset P, Deschildre A, et al. Airway Remodeling in Preschool Children with Severe Recurrent Wheeze. Am J Respir Crit Care Med. 2015; 192(2): 164-171.
https://doi.org/10.1164/rccm.201411-1958OC |
[1, 2]
. Distinguishing these subgroups at an early age is crucial for choosing appropriate therapy and determining long-term prognosis. To understand why clinical trajectories differ, it is necessary to analyse the structural changes that develop in the airways during early childhood.
Airway remodelling begins at a very early age, even in children between 1 and 3 years of age with severe recurrent episodes of bronchial obstruction, an age at which the diagnosis of asthma is not yet made. These structural changes resemble those observed in older children and adults with asthma, although they are less pronounced. However, assessing these early structural changes remains a challenge in clinical practice.
Bronchial biopsy is the gold standard for assessing remodelling, but its invasive nature makes it unsuitable for children. Furthermore, it is usually performed endobronchially and reflects only changes in the proximal airways, leaving peripheral structures unexamined. High-resolution computed tomography (HRCT) has established itself as a noninvasive method – its three-dimensional visualisation allows measurement of airway cross-sections and assessment of the degree of bronchial wall thickening
. HRCT is not recommended for routine monitoring due to radiation exposure, but helps exclude alternative diagnoses and for characterising structural changes in severe, treatment-resistant asthma. Due to these limitations, noninvasive biomarkers that reflect structural changes are actively sought.
Among the molecules studied to date, Galectin-3 (Gal-3) has emerged as a particularly promising marker due to its central role in inflammation and fibrosis. Gal-3 is a β-galactosidase-binding lectin involved in inflammatory processes, fibrogenesis, cell adhesion, and apoptosis. Elevated levels of Gal-3 have been described in chronic inflammatory and fibrotic lung diseases, including asthma, COPD, and pulmonary fibrosis
. In asthma, Gal-3 promotes eosinophil recruitment, Th2 polarisation, and extracellular matrix deposition, which leads to remodelling
| [6] | Zuberi RI, Hsu DK, Kalayci O, et al. Critical role for galectin-3 in airway inflammation and bronchial hyperresponsiveness in a murine model of asthma. Am J Pathol. 2004; 165(6): 2045-2053. https://doi.org/10.1016/S0002-9440(10)63255-5 |
[6]
. Gal-3 is associated with remodelling by potentiating TGF-β1 activation, binding to integrins, and stimulating profibrotic signals from fibroblasts and macrophages
| [7] | Calver JF, Parmar NR, Harris G, et al. Defining the mechanism of galectin-3-mediated TGF-β1 activation and its role in lung fibrosis. J Biol Chem. 2024; 300(6): 107300.
https://doi.org/10.1016/j.jbc.2024.107300 |
[7]
. The dynamic nature of Gal-3 supports its use as a biomarker of airway remodelling
| [8] | Mauri P, Riccio AM, Rossi R, et al. Proteomics of bronchial biopsies: galectin-3 as a predictive biomarker of airway remodelling modulation in omalizumab-treated severe asthma patients. Immunol Lett. 2014; 162(1 Pt A): 2-10.
https://doi.org/10.1016/j.imlet.2014.08.010 |
| [9] | Riccio AM, Mauri P, De Ferrari L, et al. Galectin-3: an early predictive biomarker of modulation of airway remodeling in patients with severe asthma treated with omalizumab for 36 months. Clin Transl Allergy. 2017; 7: 6. Published 2017 Mar 9. https://doi.org/10.1186/s13601-017-0143-1 |
[8, 9]
. These observations position Gal-3 as a promising indicator of ongoing airway remodelling in children with recurrent wheezing. In adults, a Gal-3 threshold of 17.8 ng/mL is often cited as an upper reference limit for healthy individuals
| [10] | Krintus M, Kozinski M, Fabiszak T, Kubica J, Panteghini M, Sypniewska G. Establishing reference intervals for galectin-3 concentrations in serum requires careful consideration of its biological determinants. Clin Biochem. 2017; 50(10-11): 599-604. https://doi.org/10.1016/j.clinbiochem.2017.03.015 |
[10]
. More recently, pediatric reference data have been published. A 2025 French cohort study established age-specific upper limits for Gal-3 using the Abbott immunoassay: 56 ng/mL for children under 2 years and 26 ng/mL for children older than 2 years
. Another report found the 95th percentile of serum Gal-3 to be 7–33 ng/mL in healthy children aged 2–17 years
. These values are reference intervals, not diagnostic cut-offs, and illustrate that pediatric norms differ substantially from adults. No consensus exists on a pediatric Gal-3 cut-off for clinical decision-making; values must be interpreted in the context of age-specific norms and clinical evidence.
KL-6 (Krebs von den Lungen-6) is another widely discussed candidate, but mainly as a marker of alveolar epithelial damage. It is a mucin-like glycoprotein produced by regenerating type II pneumocytes and is a well-established indicator of diffuse alveolar damage and interstitial fibrosis
. In healthy children, serum KL-6 is usually low, with an upper limit of approximately 250 U/mL
| [14] | Imai T, Takase M, Takeda S, Kougo T. Serum KL-6 levels in pediatric patients: reference values for children and levels in pneumonia, asthma, and measles patients. Pediatr Pulmonol. 2002; 33(2): 135-141. https://doi.org/10.1002/ppul.10044 |
[14]
. Although KL-6 is elevated in severe asthma exacerbations and other diffuse lung damage, it is not specific for airway remodelling and may be increased in various forms of lung injury
| [15] | Vianello A, Guarnieri G, Achille A, et al. Serum biomarkers of remodeling in severe asthma with fixed airway obstruction and the potential role of KL-6. Clin Chem Lab Med. 2023; 61(10): 1679-1687. Published 2023 Mar 30.
https://doi.org/10.1515/cclm-2022-1323 |
| [16] | Xu L, Yan DR, Zhu SL, et al. KL-6 regulated the expression of HGF, collagen and myofibroblast differentiation. Eur Rev Med Pharmacol Sci. 2013; 17(22): 3073-77. |
[15, 16]
.
The objective of this study was to assess the correlation between serum Galectin-3 (Gal-3) and KL-6 levels with clinical severity in children with recurrent wheezing at preschool age and with radiologically confirmed structural lung changes in children with cystic fibrosis.
2. Methods
A total of 48 children (35 boys and 13 girls) were included in the study and divided into two groups:
Recurrent Wheezing (RW) group: 26 children aged 7 months to 4 years (mean age 2 years and 3 months), with recurrent broncho-obstructive episodes clinically defined as an asthmatic phenotype, but without a confirmed diagnosis of asthma. Depending on the frequency of episodes, the group was divided into two subgroups: children with up to 3 episodes per year (n = 17; low frequency, RW-LF) and children with monthly attacks during the winter season, more than 6 episodes per year (n = 9; high frequency, RW-HF).
Cystic Fibrosis (CF) Group: 22 children with cystic fibrosis aged 2 months to 17 years (mean age 11 years), with clinically significant lung involvement requiring high-resolution computed tomography (HRCT) of the chest to assess the correlation between biomarker levels and the structural changes found (bronchiectasis, atelectasis and fibrosis). Children with CF were stratified by genotype into two subgroups: homozygous for the ΔF508 mutation (n = 9; CF 2× F508del) and heterozygous for ΔF508 (n = 13; carriers of one ΔF508 allele and a second different mutation; CF 1× F508del).
2.1. Laboratory Analyses
Serum Gal-3 and KL-6 were measured by ELISA method according to the manufacturer’s protocols. Galectin-3 levels had an analytical range of 2 –60 ng/mL, and a detection range for KL-6 of 31.25-2000 U/mL. A 1: 2 dilution was used for Gal-3 and a 1: 200 dilution for KL-6. All analyses were performed in duplicate with appropriate calibrators and internal controls. A reference threshold of 26 ng/mL for Gal-3 was used based on the literature
.
2.2. Imaging
All children in the CF group underwent high-resolution chest computed tomography. The extent of structural lung changes was classified based on the presence of bronchiectasis, mucous plugs/obstruction, and consolidations (corresponding to areas of atelectasis).
2.3. Statistical Analysis
Statistical processing was performed with SPSS version 23.0. The following methods were used: descriptive analysis to summarise clinical and biomarker data; analysis of correlation between qualitative variables (cross-tabulation); parametric methods (t-test), and non-parametric methods (Mann-Whitney U test, Kruskal-Wallis H test). The correlation between Gal-3, KL-6 and CT changes was assessed using Spearman’s rank correlation coefficient. Odds ratio (OR) and 95% confidence interval (CI) were reported. A p-value < 0.05 was considered statistically significant.
Institutional Review Board Statement:
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Medical University Sofia (approval code 1185, dated 05.07.2024).
Informed Consent Statement
Informed consent was obtained from all parents of the patients involved in the study. None of the patients can be identified in this publication.
Declaration of generative AI and AI-assisted technologies in the writing process
During the preparation of this manuscript, the authors used OpenAI to assist with language refinement and to create the graphical abstract. The authors carefully reviewed, edited, and verified the accuracy of all content. The authors take full responsibility for the integrity and originality of the manuscript.
3. Results
3.1. Galectin-3 Levels in Children with Recurrent Wheezing
Elevated serum Gal-3 levels were found at a very early age in the RW group, including infants under 1 year of age (median value 22.36 ng/mL in this age subgroup). A significant proportion of children had values above the reference threshold of 26 ng/mL, with the highest level reported reaching 62.95 ng/mL. There was a trend toward increased Gal-3 levels with age (7–12 months: 22.36 ng/mL; 13–23 months: 29.24 ng/mL; >24 months: 33.13 ng/mL; p = 0.01). Galectin-3 concentrations were slightly higher in girls than in boys (25.12 vs. 22.26 ng/mL); however, this difference did not reach statistical significance (p = 0.6).
Similarly, median Gal-3 levels did not differ significantly between children with monthly wheezing episodes (RW-HF) and those experiencing up to three episodes per year (RW-LF) (p > 0.05), as shown in
Table 1.
Table 1. Median (range) levels of Gal-3 (ng/mL) and KL-6 (U/mL) in the studied subgroups of children.
Comparison | Galectin-3 (ng/mL) | KL-6 (U/mL) | p-value Gal-3 | p-value KL-6 |
RW-LF (≤3 episodes/year) | 22.36 [8.96–62.95] | 194.4 [62.6–2000.0] | | |
RW-HF (>6 episodes/year) | 25.13 [10.74–2.95] | 234.6 [103.8–426.2] | > 0.05 | > 0.05 |
CF (ΔF508 homozygous) | 35.23 [2.84–62.95] | 211.8 [170.6–2000.0] | | |
CF (ΔF508 heterozygous) | 20.64 [4.67–62.95] | 196.8 [101.6–469.4] | 0.07 | > 0.05 |
CT-positive | 38.35 [4.67–62.95] | 302.2 [260.0–344.4] | | |
CT-negative | 11.63 [2.84–20.42] | 170.6 [149.8–191.4] | 0.001 | > 0.05 |
Abbreviations: RW – recurrent wheezing; LF – low frequency (≤3 episodes per year); HF – high frequency (>6 episodes per year); CF – cystic fibrosis; delF508 – F508 deletion mutation in the CFTR gene; CT – computed tomography (presence or absence of structural lung changes).
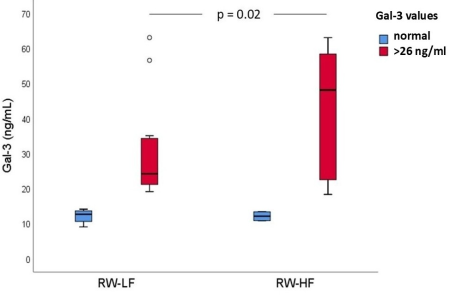
However, the risk of developing airway remodelling – defined as having a serum Gal-3 level above the reference threshold of 26 ng/mL – was 1.76 times higher in the high-frequency subgroup than in the low-frequency subset (95% confidence interval 1.04–5.13; p = 0.02), see
Figure 1. This indicates that levels above 26 ng/mL for serum Gal-3 could be used as marker for risk assessment in children with recurrent wheezing.
Figure 1. Serum Galectin-3 Levels in Low- and High-Frequency Recurrent Wheezing (RW-LF vs. RW-HF).
3.2. Galectin-3 Levels in Children with Cystic Fibrosis
Gal-3 levels varied widely in the CF group. The median Gal-3 level in ΔF508 homozygous children was higher than in the heterozygous subgroup (35.23 vs 20.64 ng/mL, p = 0.07), although this difference did not reach statistical significance due to high heterogeneity within the subgroups.
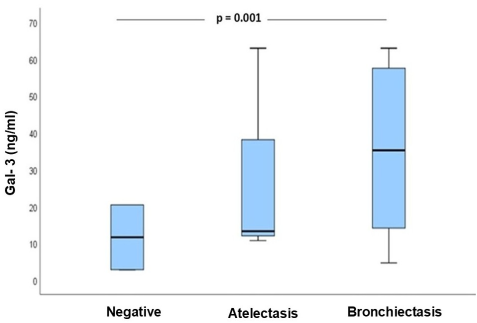
The highest median Gal-3 values were found in CF children with confirmed structural lung changes on CT - 38.35 ng/mL in those with CT-detected abnormalities vs. 11.63 ng/mL in those without CT changes (p = 0.001),
Figure 2.
Figure 2. Galectin-3 Levels in CF Patients with Normal CT, Atelectasis, and Bronchiectasis.
In particular, ΔF508-homozygous patients with bronchiectasis exhibited Gal-3 levels more than double the reference threshold (median 44.28 ng/mL), whereas homozygotes without CT abnormalities had much lower levels (as low as 4.67 ng/mL), a highly significant difference (p < 0.001). By contrast, ΔF508 heterozygotes showed no substantial Gal-3 difference between those with and without bronchiectasis. Overall, Gal-3 levels in CF children tracked closely with the presence and severity of structural lung disease (
Figure 2).
3.3. KL-6 Levels
Serum KL-6 levels did not differ significantly across any subgroups in either cohort. In both RW and CF groups, KL-6 remained within the normal paediatric range and showed no correlation with wheezing frequency, genotype, or CT findings. This consistency suggests that early airway remodelling in these children did not produce substantial alveolar injury. In other words, KL-6 elevations were absent in all subgroups, indicating that KL-6 may rise only in more advanced, fibrosis-predominant lung disease.
4. Discussion
Two specific biomarkers were investigated in the context of airway remodelling - KL-6 and Galectin-3 (Gal-3) - both associated with pathological remodelling and fibrotic changes in lung tissue. Their role in lung remodelling in childhood was assessed by studying two different clinical groups: preschool children with recurrent wheezing and children with cystic fibrosis. This parallel comparison of the two clinical phenotypes allowed us to contrast biomarker behaviour in early versus established structural airway changes.
Elevated Gal-3 levels in children with recurrent bronchial obstruction suggest that Gal-3 may serve as an early prognostic indicator of a pro-remodelling respiratory phenotype. In some children, wheezing episodes may not represent transient manifestations but rather the first signs of a persistent inflammatory process and airway remodelling. The fact that Gal-3 exceeds age-related reference thresholds in infants under 12 months suggests that structural remodelling may begin very early, potentially preceding the clinical diagnosis of asthma.
Galectin-3 is an immunoregulatory protein with a dual, context-dependent role. Although studies employing Gal-3 gene transfer in murine models have demonstrated an anti-inflammatory effect, these results are considered not to reflect the physiological function of endogenous Gal-3
. Endogenous Gal-3 has a well-documented pro-inflammatory role in numerous in vivo and in vitro studies; however, its diagnostic performance for discriminating inflammatory asthma phenotypes has not yet been systematically established
. These discrepancies may be explained by the heterogeneity of airway inflammation in asthma.
The observed relationship between the frequency of wheezing episodes and Gal-3 levels suggests a cumulative burden of remodelling. Children with frequent (approximately monthly) wheezing episodes were 1.76 times more likely to have elevated Gal-3 levels than those with infrequent episodes, highlighting a dose–response relationship between clinical severity and molecular remodelling activity. This suggests that frequent exacerbations may increase the risk of persistent obstruction and progressive lung function impairment.
Comparison between the RW and CF cohorts further supports a role for Gal-3 in airway remodelling
. In the RW group, Gal-3 serves as an early indicator of airway involvement, whereas in CF it reflects already established structural remodelling. In particular, ΔF508-homozygous CF patients with bronchiectasis showed highly elevated Gal-3 levels, significantly exceeding reference threshold, while children in the RW group showed only moderate increases. This dual model suggests that Gal-3 represents a biological link between functional symptoms and underlying structural damage – sensitive to both early inflammatory remodelling processes and and advanced anatomical changes such as bronchiectasis. Normal Gal-3 levels in CF patients without CT-confirmed structural abnormalities further support its potential specificity for structural lung disease. The marked contrast between CF patients with verified CT structural changes and those with negative imaging findings (median 38.35 ng/mL vs. 11.63 ng/mL) provides compelling evidence that Gal-3 elevation is associated with airway structural damage, rather than with the CF diagnosis per se. Moreover, Gal-3 may rise prior to overt structural changes and decrease in response to treatment, correlating with improved lung function in patients with asthma
| [8] | Mauri P, Riccio AM, Rossi R, et al. Proteomics of bronchial biopsies: galectin-3 as a predictive biomarker of airway remodelling modulation in omalizumab-treated severe asthma patients. Immunol Lett. 2014; 162(1 Pt A): 2-10.
https://doi.org/10.1016/j.imlet.2014.08.010 |
[8]
. In adults with severe asthma, baseline Gal-3 expression in bronchial tissue has been shown to predict long-term reductions in airway wall thickness following anti-inflammatory biologic therapy
| [9] | Riccio AM, Mauri P, De Ferrari L, et al. Galectin-3: an early predictive biomarker of modulation of airway remodeling in patients with severe asthma treated with omalizumab for 36 months. Clin Transl Allergy. 2017; 7: 6. Published 2017 Mar 9. https://doi.org/10.1186/s13601-017-0143-1 |
[9]
, supporting its potential utility for monitoring disease progression and therapeutic response.
Based on the data from the study, we propose the following practical approach to clinical management:
Low-risk profile: Children with normal or mildly elevated Gal-3 levels (below 26 ng/mL) and infrequent episodes (≤3 per year) appear to be at low risk of early airway remodelling. Standard treatment and routine follow-up are appropriate for them.
High-risk profile: Children with severely elevated Gal-3 (several times above 26 ng/mL) and frequent episodes (>6 per year) appear to be at high risk of initiating remodelling. In these patients, earlier and more aggressive treatment, including biologic therapy targeting their asthma phenotype, may be considered. Measurement of Gal-3 may help identify high-risk children before irreversible structural damage occurs, providing an opportunity for effective prevention.
KL-6 did not show clear clinical relevance in our study. Its values remained within the expected normal range for children and showed no relationship with clinical severity, genotype, or CT findings. This is consistent with the literature, which indicates that KL-6 is mainly elevated in cases of significant alveolar damage and interstitial fibrosis
. Persistently normal KL-6 levels, even in children with CT-proven bronchiectasis, suggest minimal alveolar involvement and limited informativeness
| [15] | Vianello A, Guarnieri G, Achille A, et al. Serum biomarkers of remodeling in severe asthma with fixed airway obstruction and the potential role of KL-6. Clin Chem Lab Med. 2023; 61(10): 1679-1687. Published 2023 Mar 30.
https://doi.org/10.1515/cclm-2022-1323 |
[15]
.
Several significant limitations should be noted, including the relatively small sample size and subgrouping that reduced statistical power. The absence of a healthy control group prevents a direct comparison with normative values. The wide age range of the patients leads to pronounced heterogeneity, making intergroup comparisons difficult. These factors limit the evaluation of the results. Future longitudinal studies are needed to validate the dynamics of the biomarkers and to define clinically relevant cut-off values for routine practice.
5. Conclusion
Gal-3 and KL-6 reflect different aspects of lung remodelling. KL-6 is primarily a marker of epithelial damage and regeneration in the alveoli, typical of advanced, fibrotic-dominant stages. In contrast, Gal-3 reflects the intensity of pro-fibrotic inflammation at a time when structural changes are still minimal. Our results highlight Gal-3 as an early measurable signal of remodelling risk in young children, at a stage when imaging methods may not yet detect structural changes. This supports its inclusion in the evaluation of children with recurrent wheezing with the aim of early identification of high-risk patients.
Abbreviations
RW | Recurrent Wheezing |
RW-LF | Recurrent Low-frequency Wheezing |
RW-HF | Recurrent High-frequency Wheezing |
CF | Cystic Fibrosis |
HRCT | High-Resolution Computed Tomography |
Gal-3 | Galectin-3 |
KL-6 | Krebs Von Den Lungen-6 |
CFTR | Cystic Fibrosis Transmembrane Conductance Regulator |
ILD | Interstitial Lung Disease |
TGF-β | Transforming Growth Factor-β |
Author Contributions
Polina Kostova: conceptualization; validation; investigation; resources; data curation; writing - original draft; visualization; project administration; funding acquisition
Julieta Hristova: methodology; validation; resources
Bilyana Georgieva: validation; investigation
Gergana Petrova: validation; investigation; supervision
Sirma Mileva: conceptualization; methodology; validation; formal analysis; investigation; resources; data curation; writing - original draft; writing – review & editing; visualization; project administration
Funding
This work was supported by the National Programme “Young Scientists and Postdoctoral Fellows – 2”, Postdoctoral Module, CC-175/01.10.2024.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to restrictions, e.g., privacy or ethics.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Saglani S, Payne DN, Zhu J, et al. Early detection of airway wall remodelling and eosinophilic inflammation in preschool wheezers. Am J Respir Crit Care Med. 2007; 176(9): 858-864.
https://doi.org/10.1164/rccm.200702-212OC
|
| [2] |
Lezmi G, Gosset P, Deschildre A, et al. Airway Remodeling in Preschool Children with Severe Recurrent Wheeze. Am J Respir Crit Care Med. 2015; 192(2): 164-171.
https://doi.org/10.1164/rccm.201411-1958OC
|
| [3] |
Silva TKBD, Zanon M, Altmayer S, et al. High-resolution CT pulmonary findings in children with severe asthma. J Pediatr (Rio J). 2021; 97(1): 37-43.
https://doi.org/10.1016/j.jped.2019.10.011
|
| [4] |
Portacci A, Iorillo I, Maselli L, et al. The Role of Galectins in Asthma Pathophysiology: A Comprehensive Review. Curr Issues Mol Biol. 2024; 46(5): 4271-4285. Published 2024 May 3.
https://doi.org/10.3390/cimb46050260
|
| [5] |
Henderson, NC, Sethi T. The regulation of inflammation by galectin-3. Immunol Rev. 2009; 230(1): 160-171.
https://doi.org/10.1111/j.1600-065X.2009.00794.x
|
| [6] |
Zuberi RI, Hsu DK, Kalayci O, et al. Critical role for galectin-3 in airway inflammation and bronchial hyperresponsiveness in a murine model of asthma. Am J Pathol. 2004; 165(6): 2045-2053.
https://doi.org/10.1016/S0002-9440(10)63255-5
|
| [7] |
Calver JF, Parmar NR, Harris G, et al. Defining the mechanism of galectin-3-mediated TGF-β1 activation and its role in lung fibrosis. J Biol Chem. 2024; 300(6): 107300.
https://doi.org/10.1016/j.jbc.2024.107300
|
| [8] |
Mauri P, Riccio AM, Rossi R, et al. Proteomics of bronchial biopsies: galectin-3 as a predictive biomarker of airway remodelling modulation in omalizumab-treated severe asthma patients. Immunol Lett. 2014; 162(1 Pt A): 2-10.
https://doi.org/10.1016/j.imlet.2014.08.010
|
| [9] |
Riccio AM, Mauri P, De Ferrari L, et al. Galectin-3: an early predictive biomarker of modulation of airway remodeling in patients with severe asthma treated with omalizumab for 36 months. Clin Transl Allergy. 2017; 7: 6. Published 2017 Mar 9.
https://doi.org/10.1186/s13601-017-0143-1
|
| [10] |
Krintus M, Kozinski M, Fabiszak T, Kubica J, Panteghini M, Sypniewska G. Establishing reference intervals for galectin-3 concentrations in serum requires careful consideration of its biological determinants. Clin Biochem. 2017; 50(10-11): 599-604.
https://doi.org/10.1016/j.clinbiochem.2017.03.015
|
| [11] |
Gravrand V, Lefebvre CS, Hamza F, et al. Pediatric reference values of NT-proBNP and Galectin-3 based on a French cohort. Clin Chim Acta. 2025; 564: 119925.
https://doi.org/10.1016/j.cca.2024.119925
|
| [12] |
Meeusen JW, Johnson JN, Gray A, et al. Soluble ST2 and galectin-3 in pediatric patients without heart failure. Clin Biochem. 2015; 48(18): 1337-1340.
https://doi.org/10.1016/j.clinbiochem.2015.08.007
|
| [13] |
Wang C, Wang Q, Liu T, Zhu J, Zhang B. Krebs von den Lungen-6 (KL-6) as a diagnostic marker for pulmonary fibrosis: A systematic review and meta-analysis. Clin Biochem. 2023; 114: 30-38.
https://doi.org/10.1016/j.clinbiochem.2023.01.010
|
| [14] |
Imai T, Takase M, Takeda S, Kougo T. Serum KL-6 levels in pediatric patients: reference values for children and levels in pneumonia, asthma, and measles patients. Pediatr Pulmonol. 2002; 33(2): 135-141.
https://doi.org/10.1002/ppul.10044
|
| [15] |
Vianello A, Guarnieri G, Achille A, et al. Serum biomarkers of remodeling in severe asthma with fixed airway obstruction and the potential role of KL-6. Clin Chem Lab Med. 2023; 61(10): 1679-1687. Published 2023 Mar 30.
https://doi.org/10.1515/cclm-2022-1323
|
| [16] |
Xu L, Yan DR, Zhu SL, et al. KL-6 regulated the expression of HGF, collagen and myofibroblast differentiation. Eur Rev Med Pharmacol Sci. 2013; 17(22): 3073-77.
|
| [17] |
Gao P, Simpson JL, Zhang J, Gibson PG. Galectin-3: its role in asthma and potential as an anti-inflammatory target. Respir Res. 2013 Dec 9; 14(1): 136.
https://doi.org/10.1186/1465-9921-14-136
|
| [18] |
Ademhan Tural D, Emiralioglu N, Akin S, et al. Galectin-3 levels in children with cystic fibrosis. Eur J Pediatr. 2024; 183(5): 2333-2342.
https://doi.org/10.1007/s00431-024-05479-6
|
| [19] |
Hilliard TN, Regamey N, Shute JK, et al. Airway remodelling in children with cystic fibrosis. Thorax. 2007; 62(12): 1074-1080.
https://doi.org/10.1136/thx.2006.074641
|
Cite This Article
-
APA Style
Kostova, P., Hristova, J., Georgieva, B., Petrova, G., Mileva, S. (2026). Galectin-3 and KL-6 as Biomarkers of Airway Remodelling and Fibrosis in Children with Chronic Lung Diseases. American Journal of Pediatrics, 12(1), 14-19. https://doi.org/10.11648/j.ajp.20261201.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Kostova, P.; Hristova, J.; Georgieva, B.; Petrova, G.; Mileva, S. Galectin-3 and KL-6 as Biomarkers of Airway Remodelling and Fibrosis in Children with Chronic Lung Diseases. Am. J. Pediatr. 2026, 12(1), 14-19. doi: 10.11648/j.ajp.20261201.13
Copy
|
Download
AMA Style
Kostova P, Hristova J, Georgieva B, Petrova G, Mileva S. Galectin-3 and KL-6 as Biomarkers of Airway Remodelling and Fibrosis in Children with Chronic Lung Diseases. Am J Pediatr. 2026;12(1):14-19. doi: 10.11648/j.ajp.20261201.13
Copy
|
Download
-
@article{10.11648/j.ajp.20261201.13,
author = {Polina Kostova and Julieta Hristova and Bilyana Georgieva and Gergana Petrova and Sirma Mileva},
title = {Galectin-3 and KL-6 as Biomarkers of Airway Remodelling and Fibrosis in Children with Chronic Lung Diseases},
journal = {American Journal of Pediatrics},
volume = {12},
number = {1},
pages = {14-19},
doi = {10.11648/j.ajp.20261201.13},
url = {https://doi.org/10.11648/j.ajp.20261201.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20261201.13},
abstract = {Introduction: Airway remodelling in children with severe recurrent episodes of bronchial obstruction starts very early, from preschool age – a period in which the diagnosis of asthma is not yet confirmed. Assessing these early structural changes presents a challenge in clinical practice. Due to the limitations of invasive methods, reliable noninvasive markers of these changes are sought. Galectin-3 (Gal-3), a regulator of inflammatory and fibrotic processes, and Krebs von den Lungen-6 (KL-6), a marker of alveolar epithelial damage, are considered as indicators of lung remodelling. Methods: Forty-eight children were studied: 26 children under 4 years of age with recurrent episodes of wheezing (RW) and 22 with cystic fibrosis (CF). Children with RW were divided into two subgroups: those with a low frequency (≤3 episodes/year) and those with a high frequency (>6 episodes/year) of bronchoobstructive symptoms. CF patients were stratified according to genotype (ΔF508 homozygous or heterozygous), and all underwent computed tomography (HRCT). Serum Gal-3 and KL-6 levels were measured by the ELISA method. The correlation between Gal-3 and KL-6 and clinical severity in children with recurrent wheezing at preschool age, and between Gal-3 and KL-6 and radiologically confirmed structural lung changes in children with cystic fibrosis, was assessed. Results: Elevated Gal-3 levels were found in children with RW from infancy. Although the differences in median Gal-3 levels did not reach statistical significance in the two RW subgroups, children with a high frequency of wheezing were 1.76 times more likely to have elevated Gal-3 (>26 ng/mL) compared to those with a low frequency of RW (p = 0.02). In CF, Gal-3 levels were significantly higher in children with confirmed structural lung disease on HRCT compared to those without pathological changes (38.35 vs. 11.63 ng/mL, p = 0.001). The highest Gal-3 values were found in ΔF508 homozygous patients with bronchiectasis. KL-6 levels remained within the normal range for the pediatric population across all groups and did not correlate with the frequency of bronchoobstructive manifestations, genotype, or CT findings. Conclusion: Galectin-3 is a reliable biomarker for pediatric pulmonology practice, reflecting early pulmonary changes in children with frequent recurrent bronchoobstructive episodes and a risk of persistent manifestations, and it correlates with structural damage in cystic fibrosis patients. KL-6 has no diagnostic value in the early stages of pulmonary pathology.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Galectin-3 and KL-6 as Biomarkers of Airway Remodelling and Fibrosis in Children with Chronic Lung Diseases
AU - Polina Kostova
AU - Julieta Hristova
AU - Bilyana Georgieva
AU - Gergana Petrova
AU - Sirma Mileva
Y1 - 2026/01/30
PY - 2026
N1 - https://doi.org/10.11648/j.ajp.20261201.13
DO - 10.11648/j.ajp.20261201.13
T2 - American Journal of Pediatrics
JF - American Journal of Pediatrics
JO - American Journal of Pediatrics
SP - 14
EP - 19
PB - Science Publishing Group
SN - 2472-0909
UR - https://doi.org/10.11648/j.ajp.20261201.13
AB - Introduction: Airway remodelling in children with severe recurrent episodes of bronchial obstruction starts very early, from preschool age – a period in which the diagnosis of asthma is not yet confirmed. Assessing these early structural changes presents a challenge in clinical practice. Due to the limitations of invasive methods, reliable noninvasive markers of these changes are sought. Galectin-3 (Gal-3), a regulator of inflammatory and fibrotic processes, and Krebs von den Lungen-6 (KL-6), a marker of alveolar epithelial damage, are considered as indicators of lung remodelling. Methods: Forty-eight children were studied: 26 children under 4 years of age with recurrent episodes of wheezing (RW) and 22 with cystic fibrosis (CF). Children with RW were divided into two subgroups: those with a low frequency (≤3 episodes/year) and those with a high frequency (>6 episodes/year) of bronchoobstructive symptoms. CF patients were stratified according to genotype (ΔF508 homozygous or heterozygous), and all underwent computed tomography (HRCT). Serum Gal-3 and KL-6 levels were measured by the ELISA method. The correlation between Gal-3 and KL-6 and clinical severity in children with recurrent wheezing at preschool age, and between Gal-3 and KL-6 and radiologically confirmed structural lung changes in children with cystic fibrosis, was assessed. Results: Elevated Gal-3 levels were found in children with RW from infancy. Although the differences in median Gal-3 levels did not reach statistical significance in the two RW subgroups, children with a high frequency of wheezing were 1.76 times more likely to have elevated Gal-3 (>26 ng/mL) compared to those with a low frequency of RW (p = 0.02). In CF, Gal-3 levels were significantly higher in children with confirmed structural lung disease on HRCT compared to those without pathological changes (38.35 vs. 11.63 ng/mL, p = 0.001). The highest Gal-3 values were found in ΔF508 homozygous patients with bronchiectasis. KL-6 levels remained within the normal range for the pediatric population across all groups and did not correlate with the frequency of bronchoobstructive manifestations, genotype, or CT findings. Conclusion: Galectin-3 is a reliable biomarker for pediatric pulmonology practice, reflecting early pulmonary changes in children with frequent recurrent bronchoobstructive episodes and a risk of persistent manifestations, and it correlates with structural damage in cystic fibrosis patients. KL-6 has no diagnostic value in the early stages of pulmonary pathology.
VL - 12
IS - 1
ER -
Copy
|
Download