1. Introduction
Cholera remains a major public health problem in low- and middle-income countries, with 1.3 to 4 million cases and 21,000 to 143,000 deaths reported annually worldwide
. In sub-Saharan Africa, this acute diarrhoeal disease remains a major public health challenge, especially in regions with limited access to clean water and sanitation
| [2] | Mengel MA, Delrieu I, Heyerdahl L, Gessner BD. Cholera outbreaks in Africa. Cholera Outbreaks. Springer; 2014. p. 117–44. |
[2]
. Cameroon, like many African countries, is not spared from this epidemiological situation, having experienced recurrent epidemics over the past two decades, with cases in 2010, 2011, and more recently between 2018 and 2022
. The cholera epidemic that struck Cameroon from 2018 to 2022 was notable for its unprecedented geographical spread, affecting nine of the country's ten regions, with a particularly high prevalence in the Littoral and Southwest regions, where attack rates reached 45.2 and 38.7 cases per 100,000 inhabitants, respectively
| [4] | MoH Cameroon. (Annual report on the epidemiological situation of cholera in Cameroon 2018-2022.). |
[4]
. This situation highlights the structural deficiencies of the Cameroonian health system, particularly regarding the ability to respond promptly, adequate health infrastructure, and competent personnel. In light of this health crisis, the organisation of care and its human dimension have proven to be essential aspects, which are relatively understudied in the literature that prioritises the epidemiological and therapeutic dimensions of the disease
| [5] | Gaffga NH, Tauxe RV, Mintz ED. Cholera: a new homeland in Africa? Am J Trop Med Hyg. American Society of Tropical Medicine and Hygiene; 2007; 77: 705. |
| [6] | Sack DA, Sack RB, Nair GB, Siddique AK. Cholera. The Lancet. Elsevier; 2004; 363: 223–33.
https://doi.org/10.1016/S0140-6736(03)15328-7 |
[5, 6]
.
The organisation of healthcare during a cholera epidemicis a challenge that goes beyond the mere establishment of cholera treatment centers (CTCs). It includes intersectoral coordination, efficient logistics, proper resource allocation, continuous training of health personnel, and community integration of interventions
| [7] | Dureab F, Ismail O, Müller O, Jahn A. Cholera outbreak in Yemen: Timeliness of reporting and response in the national electronic disease early warning system. Acta Inform Medica. 2019; 27: 85. |
[7]
. In Africa and more specifically in Cameroon, these organizational challenges are exacerbated by infrastructural constraints, geographical inequalities in access to care, limited financial resources, and deficient health information systems. The studies by Legros et al (1999)
| [8] | Legros D, Paquet C, Perea W, Marty I, Mugisha NK, Royer H, et al. Mass vaccination with a two-dose oral cholera vaccine in a refugee camp. Bull World Health Organ. 1999; 77: 837. |
[8]
have shown that the case fatality rate of cholera, which is less than 1% with adequate management, can exceed 10% when care is poorly organised, hence highlighting the importance of an effective health response. Beyond these organizational imperatives, the humanisation of care is also an ethical and practical challenge, particularly in crisis contexts where dehumanization can creep in under the guise of urgency. The humanization of care, conceptualised in Western countries by Watson and Lévinas
| [9] | Levinas E. Totality and infinity. Essay on exteriority. 1961. |
| [10] | Watson J. The philosophy and science of caring. University Press of Colorado; 1985. |
[9, 10]
, has been adopted in African contexts where community values and human dignity are central to social representations of health and illness
| [11] | Andoh CT. Bioethics and the challenges to its growth in Africa. Open J Philos. Scientific Research Publishing; 2011; 1: 67–75. |
[11]
. For cholera, a highly stigmatising disease due to its specific clinical manifestations and its association with poverty and lack of hygiene, the humanization of care helps preserve patients' dignity, reduce stigmatization, and promote community adherence to preventive measures
| [12] | Farmer P. Infections and inequalities: The modern plagues. Univ of California Press; 2001. |
| [13] | Briggs CL. Stories in the time of cholera: Racial profiling during a medical nightmare. University of California Press; 2019. |
[12, 13]
.
In Cameroon, the management of cholera outbreaks takes place within a complex sociocultural and health context, characterised by the coexistence of multiple healthcare systems (biomedical, traditional, religious), diverse etiological beliefs, and caregiver-patient relationships influenced by power dynamics
| [14] | Jaffré Y, Olivier de Sardan J-P. Inhospitable medicine: the difficult relations between caregivers and patients in five West African capitals. No Title. 2002. |
[14]
The work of Eboko et al. (2011) revealed that the quality of the relationship and respect for cultural norms in healthcare provision are key determinants of health facility utilization and the acceptability of health interventions
| [15] | Eboko F, Bourdier F, Broqua C. The Global South and AIDS: When Civil Society Mobilizes. IRD Orstom; 2011. |
[15]
. Despite this recognition, few empirical studies have described the practices of humanization in the management of cholera outbreaks in Cameroon, highlighting the scientific gap that the present study aims to address. Comparing two regions of Cameroon (Littoral and Centre) allows us to observe how different geographical, sociocultural, and political contexts influence the organization and humanization of care during an epidemic.
The Littoral region, with Douala as its economic hub, has fairly developed health infrastructures. However, it faces specific urban challenges. These include high population density (more than 3 million inhabitants in urban areas), the proliferation of informal settlements that accommodate about 60% of the urban population, massive internal migrations, and the proximity of the Wouri River and the Atlantic Ocean. These factors create favorable ecological conditions for the transmission of cholera
| [16] | INS. Statistical Yearbook of Cameroon 2020. INS Cameroon. 2020. |
| [17] | Defo BK. Demographic, epidemiological, and health transitions: are they relevant to population health patterns in Africa? Glob Health Action. Taylor & Francis; 2014; 7: 22443. |
[16, 17]
. The Centre region, home to the political capital Yaoundé, has an estimated population of 4 million inhabitants. It has a concentration of reference health infrastructures, including general hospitals, specialized centers, and better availability of qualified medical personnel. However, disparities exist between Yaoundé and the surrounding rural districts, where access to care remains limited
| [18] | Bigna JJR, Plottel CS, Koulla-Shiro S. Challenges in initiating antiretroviral therapy for all HIV-infected people regardless of CD4 cell count. Infect Dis Poverty. Springer; 2016; 5: 85. |
| [19] | Tandi TE, Cho Y, Akam AJ-C, Afoh CO, Ryu SH, Choi MS, et al. Cameroon public health sector: shortage and inequalities in geographic distribution of health personnel. Int J Equity Health. Springer; 2015; 14: 43. |
[18, 19]
. This inter-regional comparison between the economic hub (Littoral) and the political-administrative hub (Centre) will help identify contextual factors such as resources, health governance, socio-demographics, and urbanization. These factors can either promote or limit an efficient and humanised organization of cholera care. The findings will generate knowledge that is transferable to other similar African urban contexts.
The issue of the organization and humanization of care in the management of cholera is also part of contemporary debates on the quality of healthcare in low-resource countries. It also emphasises the importance of a person-centered approach even in emergency settings
| [20] | Kruk ME, Gage AD, Arsenault C, Jordan K, Leslie HH, Roder-DeWan S, et al. High-quality health systems in the Sustainable Development Goals era: time for a revolution. Lancet Glob Health. Elsevier; 2018; 6: e1196–252. |
[20]
. The Sustainable Development Goals (SDGs) SDG 3: health and well-being for all at all ages and SDG 6: universal access to water and sanitation) constitute the international normative framework for this research
| [21] | United N. Transforming our world: the 2030 Agenda for Sustainable Development. Resolution adopted by the General Assembly No. Y. 2015. |
[21]
. Moreover, the WHO's Global Strategy to End Cholera by 2030 (WHO, 2017) explicitly emphasises the importance of a comprehensive approach to the disease. This approach encompasses biomedical, organizational, and sociocultural dimensions. From this perspective, the present study aims to analyze the organization and humanization of care in cholera management in the Littoral and Centre regions of Cameroon during the epidemic period from 2018 to 2022. Specifically, this research pursues three objectives: (1) to describe and analyse the organizational models of cholera care in these two regions, identifying strengths, weaknesses, and contextual factors that affect their effectiveness; (2) to explore the practices and perceptions of the humanization of care among stakeholders including patients, caregivers, managers, communities; and (3) to formulate contextualised recommendations for improving the organization and humanization of care in the prevention and management of future cholera epidemics in Cameroon and similar contexts. To do this, a mixed approach was adopted, combining quantitative and qualitative methods such as semi-structured interviews, ethnographic observations, and focus groups. This methodological triangulation allows for an understanding of the complexity and multidimensionality of this study by cross-referencing macro-organizational perspectives with the micro-individual experiences of the actors
| [22] | Creswell JW, Clark VLP. Designing and conducting mixed methods research. Sage publications; 2017. |
[22]
. Beyond its scientific interest in understanding cholera management in Central Africa, this research holds practical value for public health decision-makers, humanitarian agencies, and healthcare professionals involved in epidemic preparedness and response. By describing the realities on the ground, highlighting good practices and mistakes to avoid, and proposing adapted avenues for improvement, this study seeks to inform cholera management policies and protocols so that they are more effective, more equitable, and more dignified.
2. Methods
2.1. Type of Study
This study used a mixed-method design with a descriptive cross-sectional study with qualitative components. The quantitative component of the study made it possible to describe the socio-economic characteristics of the sampled population. The qualitative part made it possible to understand or explain the caregiver-patient relationships.
2.2. Scope of the Study
The choice of the health districts investigated and the health facilities (HFs) was initially guided by the data of Sitrep n° 45, presenting the epidemiological situation of cholera in Cameroon. Subsequently, consultations were held with the communication focal points of the health districts to identify areas and communities considered epidemic hotspots. The study was carried out in areas and communities considered to be hotspots of the épidémique, so the empirical work was carried out in 12 health districts, six of which were in the Centre region and six in the Littoral region.
2.3. Study Population
Primary population: The primary target population consisted of individuals aged 18 years and older residing in the centre and littoral regions.
Secondary population: The secondary target population included various actors present in the sites of investigation, At the community level, these included: religious leaders, traditional leaders, administrative authorities, traders, motorcycle taxi drivers or taximen, recovered cholera patients, household members of former cholera patients (recovered or deceased), members of meighbouring households, ethno-therapists (traditional healers), informal drug sellers, naturopaths, and the heads of CBOs involved in prevention activities.
2.4. Sampling and Sample Size
quantitative component
Three-stage sampling was conducted. The primary sampling units (or clusters) were the health areas from the updated database of the health mapping file. Within each health district, the lighting of the district focal points was carried out with the reasoned selection (outbreaks at high risk of epidemic) of two health areas and two communities within each area. The secondary units were made up of communities or villages/neighbourhoods. A first community was selected from those located within a radius of 5 km to the nearest health facility. And a second community was drawn from those located more than 5 km from the nearest health facility. The tertiary sampling units were households. In each selected community, 30 households were systematically selected. Households were drawn in a sampling step of 1/15 or 20 households, depending on the level of concentration of the households. Within each selected household, a household questionnaire was administered to the Head of Household or his representative, i.e. an adult (18 years and over) capable of providing adequate information on the living conditions of the household. Sample size.
The sample size was calculated using the so-called confidence interval method. Far from a very rigid statistical formula, a sample size was reasonably envisaged based on the principles of feasibility of the study, particularly in terms of time, human and financial resources.
Table 1. Sample size.
Regions | Number of respondents per region |
Center | 743 |
Littoral | 891 |
Total | 1,634 |
qualitative component
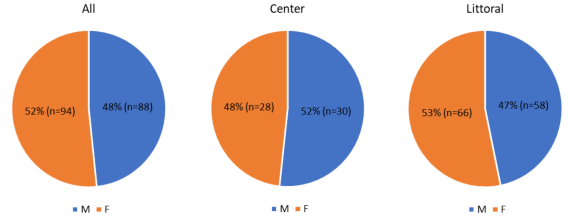
For the qualitative component, the sampling techniques mobilized both purity sampling and snowball sampling. The sample size was decided with the principle of data saturation. The most important thing was also, above all, for the experts to be reassured by the diversified participation of actors with multiple profiles. This has given more account not only to the participatory and inclusive approach of the but also this diversification has been a better strategy of triangulation of sources and Data collected. The qualitative sample covered 182 informants, including 94 women and 88 men.
Figure 1. Gender distribution of the qualitative sample of the two regions.
2.5. Data Collection Tools
Data were collected through questionnaires for the quantitative survey. For the qualitative component, semi-structured interview guides and grids were used.
2.6. Data Analysis
quantitative component
The quantitative data collected through the Kobo Collect app were exported and analyzed with Microsoft Excel for descriptive statistics.
Qualitative component
For qualitative data, a database of verbatim transcripts was established based on the various interviews. A standard transcription template was provided to the transcribers. A qualitative data analysis matrix was developed, and thematic as well as contextual analysis techniques were used through NVivo.
2.7. Ethical Considerations
The field survey was conducted following administrative authorization from the Ministry of Health (ethical committee). Participants were informed in advance of the study objectives, potential risks and benefits, and the intended use of collected data. Enrollment in interviews or focus groups occurred only after participants provided informed consent. At the start of each interview, the interviewers reiterated the objectives of the interview session and obtained the participants' permission to record the conversation.
3. Results
3.1. Sociodemographic Characteristics of Study Participants (Age and Level of Education)
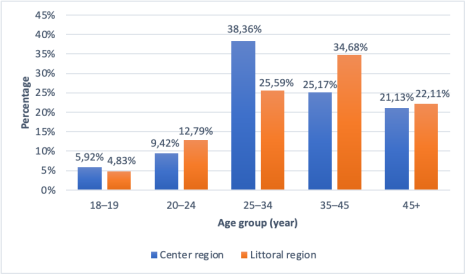
Figure 2. Age group distribution of participants in Center and Littoral regions.
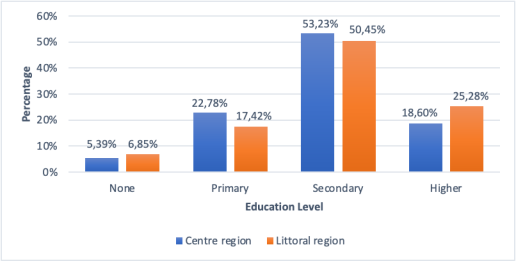
Figure 3. Sociodemographic characteristics of study participants (Age and level of education).
Given the mixed design (quantitative and qualitative), the ages of the respondents are presented according to the different study components. The respondent’s level of education indicates that secondary education is predominant. More than 50% of participants in both regions have completed atleats secondary school education corresponding to a minimum the sixth grade education.
3.2. Socio-environmental Characteristics of the HF Surveyed
Category of HF surveyed
A total of 42 health facilities were visited (
Table 2). These included two District Hospitals (DH), notably in the city of Douala; nine District Medical Centers (DMC), with 2 in Yaoundé and 7 Douala, and 31 Health Centers (HC), including Integrated Health Centers. These structures are the frontline actors in the cholera response. District hospitals are mostly designated as Cholera Treatment Units (CTUs), while health centers, which are closer to population, are primarily responsible for referring suspected cholera cases to CTUs. Among the sampled facilities, 17 are public HFs and 25 are private HFs, which are also highly utilised by the communities.
Table 2. Category of HFs respondents.
HFs categories | Centre | Littoral | TOTAL |
DMC n (%) | 2 (22,2%) | 7 (78,8%) | 9 (100%) |
HC n (%) | 19 (61,3%) | 12 (38,7%) | 31 (100%) |
DH n (%) | 0 (0%) | 2 (100%) | 2 (100%) |
Total n (%) | 21 (83,5%) | 21 (50,0%) | 42 (100%) |
Type of health personnel working in HFs
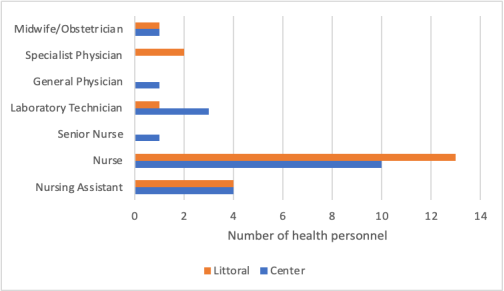
Figure 4. Type of health personnel working in HFs per region.
The profiles of the health personnel, particularly the managers encountered in the visited health facilities diverse. They range from the nursing assistants to the doctors, depending on the category of the HFs. Observations indicate that nurses constitute the largest group, representing more than 50% of the staff. This level of training of these providers can play a decisive role in the management and referral of suspected cholera cases.
3.3. Organization and Humanization of Care
Stigma caregiver-patient interactions
According to the respondents from the medical staff of the of Biyem-Assi Health District, efforts are made to improve the quality of interactions with patients. However, initially, health care staff stigmatised cholera patients and instilled fear in them, sometimes refusing to provide care. It was only after the district set up incentives and applied pressure that some staff agreed to administer treatment.
I know health facilities that did not even want to place a venous line for a suspected case of cholera, to the point that the note had to be signed by the delegate instructing the health facilities to lift the emergency before referring. What the health facility did was to immediately refer the cases elsewhere in order to reduce its own caseload, but we later realized that there was also an element of psychosis among the patients. We had to organize working sessions with service providers to explain to them the merits of taking care of the patient first because he himself plays on his psychology." Verbatims: 1.
Informants reported that reception in health facilities remains inadequate, largely because cholera is perceived as a “disease of dirt”. This poor reception contributes to cholera patients feeling stigmatised, which can exacerbate the progression of the disease. "I witnessed this type of behaviour by staff in two HFs where I was present. The patient was not welcomed and there at the triage at the entrance, as soon as we noticed that he had the signs and symptoms of cholera, he and his parents were asked to leave and to go somewhere else. I was so touched, and since I was with one of my colleagues, he said 'no, no, it doesn't happen like that, at least lift the emergency', and on top of that, he was a 13-year-old child in a serious condition." Verbatims: 2.
Cases of satisfaction
Despite some negative experiences, many former patients reported receiving care with the active participation and support of staff. "We arrived and were received like any other patient. There were no problems, so there was a bit of urgency, people moved a little from left to right to support us" (former cholera patient, Mvog-Betsi hospital, Centre). Verbatims: 3.
In the Littoral region, satisfaction was also expressed: "I was satisfied with the staff and the relationship I had with them during my illness. They were so concerned and involved that seeing them work was already the beginning of a cure" (former cholera patient Verbatims: 4). A CHW also emphasised the positive relationships between caregivers and patients: "The relationships of cholera patients and those who treat them are always beautiful because the people who take care of cholera patients take good care of them" (HD Nylon ASC) Verbatims: 5.
3.4. Assessment of Hospital Organisation in Cholera Control Efforts
In terms of organisation, there is a national protocol for the management of cholera and Health Care Unit. For HFs without Health care unit, staff are instructed to provide initial emergency care and refer patients to an appropriate Unit. Surveillance within HFs is generally perceived as rapid.: One example involved a small health facility that received its first cholera case and immediately notified the epidemiological surveillance focal person of the Biyem-Assi Health District: "I was returning from an environmental sample early in the morning when I received the call from the head of the HF, she was panicking on the phone because of the signs and symptoms, she is a pharmacist and she tells me there is a case here with rice-water color, he has cramps, he vomits. So, I give her instructions to follow. I wanted to send the RDTs, but then I said no! I would have to go down personally to take a sample. Since she even made me understand that she doesn't know how to use RDTs. I just dropped off my bag, and then I went to the HF, and when I arrived, I tested it, and it was positive. The patient was really in a severe condition. So, I called my colleague at the Efoulan HD, I referred the patient there urgently, and he was taken care of because we didn't have a space here where we could take care of him, and in the HF there was no space. Afterwards, we disinfected the premises and began the investigation" Verbatims: 6.
As soon as a HF receives a case, they are expected to notify it to the regional level. However, it turned out that HF, which received suspected cases of cholera, did not accept these cases into the HF and referred them elsewhere. Generally, in all healthcare facilities, we observed significant efforts to improve the effectiveness of care, notably through the establishment of dedicated units for cholera patients, such as the unit constructed at the DMC Mvog-Betsi.
Not all the health facilities surveyed in the Odza HD had an effective organization to manage cholera outbreaks. Some limited themselves to simply referring cases. When a patient is found to present symptoms of cholera, he is isolated, first aid is administered, and he is referred. However, Field data and direct observation of cholera patients within the health care unit suggest that care is well organized. "When you arrive at the hospital and have symptoms such as diarrhea and profuse vomiting, they quickly do the tests and transfer you to the emergency ward. They start the treatment without asking anything from you." Former Patient. Verbatims: 7.
3.5. Assessment of Patients' Attendance at Cholera Control Services
We obtained a Positive assessment of the cholera control unit despite some inconveniences and efforts that still need to be made. For the most part, patients who decided to go to a health facility for treatment had first been delayed at home. When the signs and symptoms began, they postponed the decision to go to the health center, often remaining at home for several hours. After a day of illness, they arrived already in a serious condition. This could be because cholera is mostly perceived as a disease of dirt, nevertheless, others quickly found the courage to go to a HF for treatment.
It should be noted that cholera control services in private HFs are not in high demand as cholera treatment is not free of charge. According to former patients, the cholera wards are sufficiently crowded with people. This could be explained by the scale of the outbreaks. The unpredictable and rapid nature of cholera leads to a large influx of patients, resulting in massive attendance at cholera control services. Although these private cholera services are less known by the population, those who are aware of them go directly there instead of visitingthe nearest public health center, or are referred there by medical staff: "because there are many persons there and managing people is complicated because humans are difficult" (Former cholera patient taken to the Nicola Barre health center and transferred to the hospital of Djoungolo). Verbatims: 8.
We have had a lot of patients, but as I said, we have always referred after the emergency has been lifted?" (EI-HF Coordinator - Nicolas Barre). "As my wife was tired at first, she was already in bed and I asked her to go outside to lie down because the room itself looks like cholera. After the maintenance service arrived and they cleaned up and we went in. Right away, the doctors and nurses concerned were asking us questions and everything. (Former cholera patient, Mvog-Betsi hospital). Verbatims: 9.
3.6. Assessment of the Treatment of Cholera Patients
Positive assessment due to free treatment
During community investigations, the CHWs raised awareness among the population and also encouraged them to raise awareness among others in their surroundings. This awareness consistently included communication that cholera treatment is free of charge. This free service also appeared in the discourse of medical staff: "The government is clear. Cholera treatment is free of charge. This means that everything related to cholera they receive care for free. Head of the DMC area of Mvog-Betsi. Verbatims: 10.
"Anyone suffering from cholera doesn't even pay five francs for treatment. The care is free," says the representative of the district health officer of Bonassama. Verbatims: 11.
It also appears in the accounts of former patients: "Yes, the treatment was free, there were some medications that were administered, and we were told that we would try to pay for them as well as the hospitalization costs, but the cholera treatment was free" (former patient, DMC of MvogBetsi). Verbatims: 12.
Positive assessment of the care system
The testimony of former patients shows that despite the stigmatisation and high patient load, cholera patients are well treated during their hospital stay. The relationship between caregivers and patients has a considerable influence on patient care, especially cholera patients. Attendance at a health facility and treatment adherence depend largely on how patients are treated during their care. The emergence of cholera requires rapid and correct care of the patient.
"When the patient arrives, we welcome them and begin triage immediately. If the patient already shows one or two signs of the disease, they are sent directly to the treatment room. Solutes are administered according to the person's state of hydration. If the patient has mild dehydration, they are started on ORS, provided they are not too weak. For moderate or severe dehydration without confirmed infection, we use IPE. If the infection is confirmed, administer antibiotic directly: doxycycline for adults and azithromycin for children" Head of the DMC area of Mvog-Betsi. Verbatims: 13.
4. Discussion
The results of this research are consistent with those of Edouard Guevart et al. (2008)
| [23] | Edouard Guevart, Armand Ekambi, Juergen Noeske et al. Formative supervision: the experience of cholera treatment units during the Douala Cameroon epidemic. Public Health; 2008; 20: 39-57. |
[23]
on formative supervision, which examined the experience of cholera treatment units during the Douala-Cameroon epidemic. Both studies highlight the human and organizational challenges observed in the management of cholera. Guevart et al. noted that "in a cholera treatment unit, two doctors had to be transferred per measure disciplinary". Similarly, in our study, several health workers initially refused to take care of suspected cases of cholera: As reported by the head of the Biyem-Assi Health District, "I say that the reluctance was that of the staff. Because it was the same staff who frightened the patients, and then they became even more reluctant. But we did everything, and then they also started to get into it". "We were then obliged to disinfect the HF because some staff do not want to be involved in all this. They say, " Oh, I'm still young, I don't want to die, I want to see my children grow up" (PF surveillance, Centre). The results are also consistent with those of Emma Kamel et al.
| [26] | Eman Kamel Hossny, Sahar Mohamed Morsy, Asmaa Mohamed Ahmed, Manal Saleh Moustafa Saleh, Atallah Alenezi and Marwa Samir Sorour (2022) Management of the COVID-19 pandemic: challenges, practices, and organizational support, BMC, Nurcing 2022/ vol. 21, P 21-27. |
[26]
on Management of the COVID-19 pandemic: challenges, practices, and organizational support. The study highlights the shortage in nursing staff during the Covid 19 outbreak.
However, our result are not consistent with those of Hasan Erbay
| [27] | Elbably N. Corona crisis management: Cause of success and failure. Istanbul, Turkey: Egyptian institute for studies; 2020. |
[27]
on the Covid 19 pandemic response and its impact on post corona health emergency and disaster risk management in turkiye concening the management of the pandemic is not only related to physicians, but also nurses, prehospital emergency teams, intensive care personnel, hospital cleaning/hygiene staff, social workers, filiation staff, family physicians, administrative officials, etc. It is a complex system that requires many human resources. But in our study, we found that only physicians and nurses are involved in cholera management.
Regarding the satisfaction of patients and households with the management of cholera in terms of reception and compliance with the protocol developed by WHO (2024), our results corroborated those of Justin Ndié, Isaak Bayoro et al (2016)
| [24] | Ndié, J., Bayoro, I., Takoukam, I., & Wina, P. (2016). Study of the epidemiological aspects of cholera in the health district of Tcholliré (northern Cameroon). European Scientific Journal, ESJ, 12(15), 278. |
[24]
who studied the epidemiological aspects of cholera in the Tcholliré Health District. Their study reported that the use of a 0.9% sodium chloride solution, oral rehydration salt (ORS), and antibiotic prophylaxis allowed optimal patient care, which contributed to a significant reduction in the death rate and reassured patients about the quality of care. As described by the head of the DMC area of Mvog-Betsi: “When the patient arrives, we welcome him, we already triage. If the patient already shows one or two signs of the disease, he or she is sent directly to the treatment room. It is already given solutes according to the person's state of hydration to raise his/her level of electrolytes. If the person has a mild defamation, they start giving the ORS first, if they are not tired. If he has a moderate or severe defamation, we give only ORS and not antibiotics. If we have confirmed, we give him the antibiotic directly. If it is an adult, it is doxycycline and in children azithromycin". Patient satisfaction was also reported in the Littoral region: "I was satisfied with the staff and the relationship I had with them during my illness. They were so concerned and involved that seeing them work was already the beginning of a cure" (former cholera patient). Regarding delay in care, our study revealed that in some health facilities, the time taken to provide care was prolonged due to the reluctance of health personnel and stigmatisation of cholera patients. These findings are consistent with those of Bbary AR, Dossou JP et al (2008)
| [25] | Akpa Raphaël Gbary, Roch Aristide Sossou, Jean-Paul Dossou, Virginie Mongbo, Achille Massougbodji. (2008). The determinants of the low lethality of the cholera epidemic in the Littoral region of Benin in 2008. Public Health 2011/5 Vol. 23, pp. 345-358. |
[25]
in his work on the epidemiological and medico-clinical aspects of the cholera epidemic in the Littoral department of Benin. In this study, one case of death was recorded in a treatment centre due to late admission. In the centre region, for example, the behaviour of the healthcare staff was particularly decisive for patient care. In response to delays and reluctance, the Regional Delegate of Public Health of the Centre issued a letter instructing all health facilities receiving patients with cholera symptoms to immediately provide emergency care to people with signs and symptoms of the cholera and to refer cases to designated health care unit, ensuring timely and appropriate management.