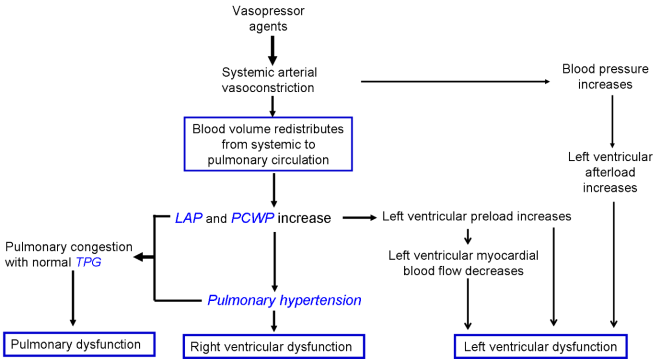
Pulmonary hypertension due to left heart disease (PH-LHD) is the most common form of pulmonary hypertension (PH), accounting for 65–80% of cases, and is associated with significant morbidity and mortality. PH-LHD is traditionally considered a passive condition, primarily driven by elevated left heart pressure, which increases pulmonary venous pressure. However, vasopressors, such as phenylephrine, frequently used in critical care to enhance vascular tone, can induce another form of passive PH. This vasopressor-induced PH shares hemodynamic similarities with PH-LHD, characterized by increased pulmonary blood volume and left atrial pressure, and exerts additive effects on pre-existing PH-LHD, exacerbating pulmonary congestion and worsening clinical outcomes. The interaction between vasopressors and PH-LHD is often overlooked, yet it poses significant risks, particularly in patients with heart failure. This review explores the pathophysiology of passive PH-LHD, the mechanisms of vasopressor-induced PH, and their additive effects. We also highlight the challenges in diagnosing passive PH, which is frequently misclassified as pulmonary arterial hypertension (PAH), leading to inappropriate treatment and potential harm. Current therapeutic strategies, such as diuretics and blood volume management, are discussed as potential approaches to mitigate these effects. Improved understanding of these mechanisms is crucial for optimizing treatment and reducing morbidity and mortality. Future research is needed to develop targeted therapies and improve outcomes for patients with PH-LHD and vasopressor-induced PH.
| Published in | International Journal of Anesthesia and Clinical Medicine (Volume 13, Issue 1) |
| DOI | 10.11648/j.ijacm.20251301.14 |
| Page(s) | 24-29 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Vasopressor Agents, Pulmonary Hypertension, Passive, Left Heart Disease, Pulmonary Circulation, Additive Effects
PH-LHD | Pulmonary Hypertension Due to Left Heart Disease |
PH | pulmonary Hypertension |
PAH | pulmonary Arterial Hypertension |
mPAP | Mean Pulmonary Artery Pressure |
PAWP | Pulmonary Arterial Wedge Pressure |
HF | Heart Failure |
TPG | Transpulmonary Gradient |
PVR | Pulmonary Vascular Resistance |
LAP | Left Atrial Pressure |
PCWP | Pulmonary Capillary Wedge Pressure |
RAP | Right Atrial Pressure |
CVP | Central Venous Pressure |
LV | Left Ventricular |
| [1] | Sommer N, Richter MJ, Tello K, et al. Update pulmonalarterielle Hypertonie: Definitionen, Diagnose, Therapie [Update pulmonary arterial hypertension: Definitions, diagnosis, therapy]. Internist (Berl). 2017; 58(9): 937-957. |
| [2] | Humbert M, Kovacs G, Hoeper MM, et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J 2023; 61: 2200879. |
| [3] | Kovacs G, Bartolome S, Denton CP, Gatzoulis MA, Gu S, Khanna D, Badesch D, Montani D. Definition, classification and diagnosis of pulmonary hypertension. Eur Respir J. 2024 Oct 31; 64(4): 2401324. |
| [4] | Simonneau G, Montani D, Celermajer DS, et al. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J 2019; 53(1). |
| [5] | Rosenkranz S, Gibbs JSR, Wachter R, et al. Left ventricular heart failure and pulmonary hypertension†. Eur Heart J 2016; 37(12): 942-954. |
| [6] | Hoeper MM, Humbert M, Souza R, et al. A global view of pulmonary hypertension. Lancet Respir Med 2016; 4(4): 306-322. |
| [7] | Sabry O, Ahmed Z, Kenneth N. Cardiac vasoplegia syndrome: pathophysiology, risk factors and treatment. American Journal of the Medical Sciences 2015; 349(1): 80-88. |
| [8] | Rieg AD, Rossaint R, Uhlig S, et al. Cardiovascular Agents Affect the Tone of Pulmonary Arteries and Veins in Precision-Cut Lung Slices. Plos One 2011; 6(12): e29698. |
| [9] | Werner F, Kojonazarov B, Gaßner B, et al. Endothelial actions of atrial natriuretic peptide prevent pulmonary hypertension in mice. 2016; 111(2): 22. |
| [10] | Morimatsu H, Ishikawa K, May CN, et al. The systemic and regional hemodynamic effects of phenylephrine in sheep under normal conditions and during early hyperdynamic sepsis. 2012; 115(2): 330-342. |
| [11] | Jiang C, Qian H, Luo S, et al. Vasopressors induce passive pulmonary hypertension by blood redistribution from systemic to pulmonary circulation. Basic Research in Cardiology 2017; 112(3): 21. |
| [12] | Vachiery JL, Tedford RJ, Rosenkranz S, et al. Pulmonary hypertension due to left heart disease. Eur Respir J 2019; 53(1). |
| [13] | Vachiéry JL, Al E. Pulmonary hypertension due to left heart diseases. Journal of the American College of Cardiology 2013; 62(25): D100-D108. |
| [14] | Borlaug BA. Discerning pulmonary venous from pulmonary arterial hypertension without the help of a catheter. Circulation Heart Failure 2011; 4(3): 235. |
| [15] | Elliott AR, Fu Z,., Tsukimoto K,., et al. Short-term reversibility of ultrastructural changes in pulmonary capillaries caused by stress failure. Journal of Applied Physiology 1992; 73(3): 1150. |
| [16] | Guazzi M. Alveolar Gas Diffusion Abnormalities in Heart Failure. J Card Fail 2008; 14(8): 695-702. |
| [17] | Alexander K, Jun Y, Kaestle SM, et al. Lung endothelial dysfunction in congestive heart failure: role of impaired Ca2+ signaling and cytoskeletal reorganization. Circulation Research 2010; 106(6): 1103. |
| [18] | Guazzi M,., Pontone G,., Brambilla R,., et al. Alveolar-capillary membrane gas conductance: a novel prognostic indicator in chronic heart failure. Eur Heart J 2002; 23(6): 467-476. |
| [19] | Ten Freyhaus H, Berghausen EM, Janssen W, et al. Genetic Ablation of PDGF-Dependent Signaling Pathways Abolishes Vascular Remodeling and Experimental Pulmonary Hypertension. Arterioscler Thromb Vasc Biol. 2015; 35(5): 1236-1245. |
| [20] | Harvey RM, Enson Y,., Ferrer MI. A reconsideration of the origins of pulmonary hypertension. Chest 1971; 59(1): 82-94. |
| [21] | Robert N, Jean-Luc V, Patrick Y, et al. The transpulmonary pressure gradient for the diagnosis of pulmonary vascular disease. Eur Respir J 2013; 41(1): 217-223. |
| [22] | Yingjie C, Haipeng G, Dachun X, et al. Left ventricular failure produces profound lung remodeling and pulmonary hypertension in mice: heart failure causes severe lung disease. Hypertension 2012; 59(6): 1170-1178. |
| [23] | Christian G, Mario G, Lang MB, et al. Diastolic pulmonary vascular pressure gradient: a predictor of prognosis in "out-of-proportion" pulmonary hypertension. Chest 2013; 143(3): 758-766. |
| [24] | Thiele H, Ohman EM, de Waha-Thiele S, et al. Management of cardiogenic shock complicating myocardial infarction: an update 2019. Eur Heart J 2019. |
| [25] | Holmberg MJ, Issa MS, Moskowitz A, et al. Vasopressors During Adult Cardiac Arrest: A Systematic Review and Meta-Analysis. Resuscitation 2019. |
| [26] | Mentz RJ, Metra M, Cotter G, et al. Early vs. late worsening heart failure during acute heart failure hospitalization: insights from the PROTECT trial. Eur J Heart Fail 2015; 17(7): 697-706. |
| [27] | Sarkar J, Golden PJ, Kajiura LN, et al. Vasopressin decreases pulmonary-to-systemic vascular resistance ratio in a porcine model of severe hemorrhagic shock. Shock 2015; 43(5): 475-482. |
| [28] | Sugawara Y, Mizuno Y, Oku S, et al. Effects of vasopressin during a pulmonary hypertensive crisis induced by acute hypoxia in a rat model of pulmonary hypertension. Br J Anaesth 2019; 122(4): 437-447. |
| [29] | Hussain MB, Marshall I,. Characterization of alpha1-adrenoceptor subtypes mediating contractions to phenylephrine in rat thoracic aorta, mesenteric artery and pulmonary artery. British Journal of Pharmacology 2010; 122(5): 849-858. |
| [30] | Caldini P,., Permutt S,., Waddell JA, et al. Effect of epinephrine on pressure, flow, and volume relationships in the systemic circulation of dogs. Circulation Research 1974; 34(5): 606-23. |
| [31] | Russell JA, Walley KR, Joel S, et al. Vasopressin versus norepinephrine infusion in patients with septic shock. N Engl J Med 2008; 358(9): 877-887. |
| [32] | Guazzi M, Borlaug BA. Pulmonary hypertension due to left heart disease. Circulation 2012; 126(8): 975-90. |
| [33] | Abraham WT, Adamson PB, Bourge RC, et al. Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: a randomised controlled trial. Lancet 2011; 377(9766): 658-666. |
| [34] | Salem M, Al-Saffar F, Hall S. Management of Pulmonary Hypertension in Patients on Left Ventricular Assist Device Support. Rev Cardiovasc Med. 2022; 23(9): 308. Published 2022 Sep 13. |
| [35] | Torre-Amione G, Southard RE, Loebe MM, et al. Reversal of secondary pulmonary hypertension by axial and pulsatile mechanical circulatory support. The Journal of Heart and Lung Transplantation 2010; 29(2): 195-200. |
APA Style
Xiao, X., Xu, Y., Jiang, C. (2025). Vasopressors Aggravate Passive Pulmonary Hypertension Due to Left Heart Disease, from Basic Pathophysiology to Clinical Management. International Journal of Anesthesia and Clinical Medicine, 13(1), 24-29. https://doi.org/10.11648/j.ijacm.20251301.14
ACS Style
Xiao, X.; Xu, Y.; Jiang, C. Vasopressors Aggravate Passive Pulmonary Hypertension Due to Left Heart Disease, from Basic Pathophysiology to Clinical Management. Int. J. Anesth. Clin. Med. 2025, 13(1), 24-29. doi: 10.11648/j.ijacm.20251301.14
@article{10.11648/j.ijacm.20251301.14,
author = {Xiao Xiao and Yan Xu and Chunling Jiang},
title = {Vasopressors Aggravate Passive Pulmonary Hypertension Due to Left Heart Disease, from Basic Pathophysiology to Clinical Management},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {13},
number = {1},
pages = {24-29},
doi = {10.11648/j.ijacm.20251301.14},
url = {https://doi.org/10.11648/j.ijacm.20251301.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20251301.14},
abstract = {Pulmonary hypertension due to left heart disease (PH-LHD) is the most common form of pulmonary hypertension (PH), accounting for 65–80% of cases, and is associated with significant morbidity and mortality. PH-LHD is traditionally considered a passive condition, primarily driven by elevated left heart pressure, which increases pulmonary venous pressure. However, vasopressors, such as phenylephrine, frequently used in critical care to enhance vascular tone, can induce another form of passive PH. This vasopressor-induced PH shares hemodynamic similarities with PH-LHD, characterized by increased pulmonary blood volume and left atrial pressure, and exerts additive effects on pre-existing PH-LHD, exacerbating pulmonary congestion and worsening clinical outcomes. The interaction between vasopressors and PH-LHD is often overlooked, yet it poses significant risks, particularly in patients with heart failure. This review explores the pathophysiology of passive PH-LHD, the mechanisms of vasopressor-induced PH, and their additive effects. We also highlight the challenges in diagnosing passive PH, which is frequently misclassified as pulmonary arterial hypertension (PAH), leading to inappropriate treatment and potential harm. Current therapeutic strategies, such as diuretics and blood volume management, are discussed as potential approaches to mitigate these effects. Improved understanding of these mechanisms is crucial for optimizing treatment and reducing morbidity and mortality. Future research is needed to develop targeted therapies and improve outcomes for patients with PH-LHD and vasopressor-induced PH.},
year = {2025}
}
TY - JOUR T1 - Vasopressors Aggravate Passive Pulmonary Hypertension Due to Left Heart Disease, from Basic Pathophysiology to Clinical Management AU - Xiao Xiao AU - Yan Xu AU - Chunling Jiang Y1 - 2025/03/28 PY - 2025 N1 - https://doi.org/10.11648/j.ijacm.20251301.14 DO - 10.11648/j.ijacm.20251301.14 T2 - International Journal of Anesthesia and Clinical Medicine JF - International Journal of Anesthesia and Clinical Medicine JO - International Journal of Anesthesia and Clinical Medicine SP - 24 EP - 29 PB - Science Publishing Group SN - 2997-2698 UR - https://doi.org/10.11648/j.ijacm.20251301.14 AB - Pulmonary hypertension due to left heart disease (PH-LHD) is the most common form of pulmonary hypertension (PH), accounting for 65–80% of cases, and is associated with significant morbidity and mortality. PH-LHD is traditionally considered a passive condition, primarily driven by elevated left heart pressure, which increases pulmonary venous pressure. However, vasopressors, such as phenylephrine, frequently used in critical care to enhance vascular tone, can induce another form of passive PH. This vasopressor-induced PH shares hemodynamic similarities with PH-LHD, characterized by increased pulmonary blood volume and left atrial pressure, and exerts additive effects on pre-existing PH-LHD, exacerbating pulmonary congestion and worsening clinical outcomes. The interaction between vasopressors and PH-LHD is often overlooked, yet it poses significant risks, particularly in patients with heart failure. This review explores the pathophysiology of passive PH-LHD, the mechanisms of vasopressor-induced PH, and their additive effects. We also highlight the challenges in diagnosing passive PH, which is frequently misclassified as pulmonary arterial hypertension (PAH), leading to inappropriate treatment and potential harm. Current therapeutic strategies, such as diuretics and blood volume management, are discussed as potential approaches to mitigate these effects. Improved understanding of these mechanisms is crucial for optimizing treatment and reducing morbidity and mortality. Future research is needed to develop targeted therapies and improve outcomes for patients with PH-LHD and vasopressor-induced PH. VL - 13 IS - 1 ER -
Department of Anesthesiology and Translational Neuroscience Center, West China Hospital, Sichuan University, Chengdu, China
Department of Anesthesiology and Translational Neuroscience Center, West China Hospital, Sichuan University, Chengdu, China
Department of Anesthesiology and Translational Neuroscience Center, West China Hospital, Sichuan University, Chengdu, China
Information