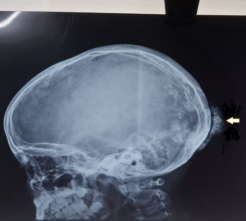
A 8-year-old girl presented with pain in bilateral hip and thigh with progressive difficulty in getting up and walking for last 2 years. Patient had difficulty with activities such as rising from a chair, climbing stairs, lifting objects, or washing her hair. There was no dysphagia, dysphonia, difficulty in swallowing and no weakness in the muscles of respiration. On examination child was very thin with areas of scalp alopecia. Multiple small, flat-topped, reddish-purple, non-tender papules were seen on the back of the hands and fingers indicative of Gottrons papules. Severe muscle wasting in both upper and lower limbs was seen. Gowers sign was positive. Extensive calcifications were seen in bilateral axillary region, around knee, hip and occipital region. ANA (Antinuclear Antibody) test by indirect immunofluorescence on Hep 2 cells showed speckled 2+ positivity (1:80). EMG (Electromyogram) and MRI (Magnetic Resonance Imaging) findings were consistent with dermatomyositis. Child was started on high dose corticosteroids along with oral methotrexate and hydroxychloroquin. Child improved and muscle strength improved. Subsequently child got readmitted in the next 6 months multiple times with cellulitis. Each time Staph aureus was obtained on aspiration and child responded to intravenous vancomycin. Child was started on Pamidronate infused intravenously at 1 mg/kg/day for 3 consecutive days every 3 months. Inaddition child received intravenous immunoglobulin monthly for 6 months. On follow-up after one year, there was complete clearance of calcinosis at all sites and good disease control without signs of myositis. Thus it appears that multiple drugs can resolve extensive calcinosis when used in combination.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Juvenile dermatomyositis (JDM) is a very rare, clinical devastating disease in children and is characterised by a systemic capillary vasculopathy presenting as proximal muscle weakness, elevated muscle enzymes, and pathognomonic heliotrope rash and Gottron’s papules. Important complications are calcinosis, lipodystrophy, and in long standing cases, osteoporosis. Extensive calcinosis in this condition is very difficult to treat as no specific therapy affords complete resolution. There is no standardized recommended treatment of JDM-associated calcinosis. Published literature of treatment outcomes is confined to small series and case reports across the world(1). Choice of drugs is based on clinical experience (1).This case report describes a girl with extensive dystrophic calcinosis due to dermatomyositis which responded to combination therapy with multiple agents.
2. Case Presentation
An eight-year-old girl presented with pain in bilateral hip and thigh with progressive difficulty in getting up and walking for last 2 years. In the preceding 2 months prior to presentation, she gave a history of inability to walk fast and progressive thinness of legs and arms. The patient had limitation of multiple activities including rising from a chair, climbing up the stairs, lifting objects above her head and washing her hair suggestive of proximal muscle weakness. There was difficulty in lifting arm above the head also. head drop. There was no dysphagia, dysphonia, and weakness in the muscles of respiration. Parents gave a history of progressive loss of weight and failure to attain height with time. There was no history of fever, rash, alterations in intellect, difficulty in chewing, swallowing. There was no history of drooping of eyelids or diurnal variation of weakness. Bladder and bowel control was preserved. Birth and development history and family history were unremarkable. Patient had three siblings who were all healthy. There was no family history of consanguinity.
On examination child was very thin with a weight of 16 kg (< 3SD below mean weight for age), height 111 cms (between -2SD to -3SD below mean height for age), Body Mass Index (BMI) of 13kg/metre2 (less than 5 percentile as per BMI percentile chart for girl 2 to 20 years). There were areas of scalp alopecia. Multiple small, flat-topped, reddish-purple, non-tender papules were seen on the back of the hands and fingers indicative of Gottrons papules. There was no pallor, clubbing, icterus, or lymphadenopathy or malar rash. Examination of the Central Nervous System revealed severe muscle wasting in both upper and lower limbs, Gowers sign was positive. Tone was normal in all four limbs. Power was 4/5 in all 4 limbs and Deep tendon reflexes were normal. The plantar reflex was flexor. There was no cranial nerve involvement. There was no sensory system involvement. Examination of the vertebral column revealed no abnormality.
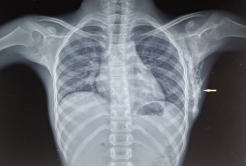
A diagnostic possibility of Juvenile Dermatomyositis was made. Investigations revealed Hemoglobin 12 gm%, Total Leucocyte Count - 4900 cell/dl, Normal Differential Leucocyte Count, Platelet count of 2.2 lakhs/dl, raised serum lactate dehydrogenase 528 units /L, Creatine phosphokinase 3 was 520 U/L) which was elevated. Erythrocyte Sedimentation Rate was elevated (96 mm in first hour). Liver function tests, renal functions and Electrocardiogram was normal. Chest X ray revealed sheet like calcification in bilateral axillary region and soft tissue of lateral chest wall cavity (Figure 1).
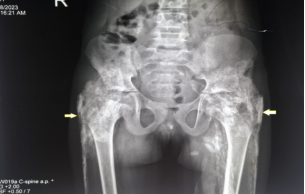
This child had dermal nodules (appearing sponge-like on plain X-ray), tumoral forms (mass-like) and widespread sheet-like calcifications (calcinosis universalis) around the hip region. (Figure 4).
Antinuclear Antibody (ANA) test by indirect immunofluorescence on HEp-2 cells showed speckled 2+ positivity (1:80), Double stranded DNA (Ds DNA) by Enzyme linked Immunosorbent assay (ELISA) was 15 IU/ml (negative) and nuclear antigen line assay was negative indicating connective tissue disorder. Nerve conduction study was normal. The electromyogram revealed an increase in spontaneous and insertional activity, fibrillation potentials, multiple sharp waves, early recruitment, and reduced polyphasic motor potentials. Myositis specific antibodies could not be done due to non - availability in the hospital.
Multiplanar Magnetic Resonance (MRI) imaging of the bilateral thigh was performed on 3T magnet system using body coils. There was evidence of T2/STIR hyperintensity noted symmetrically in the myofascial planes of bilateral anterior compartment of thigh with involvement of the 75-100% of fibres of vastus intermedius, 25-50% of vastus lateralis, <25% of vastus medialis muscles showing post contrast enhancement. Multiple linear which appeared hypointense on all sequences (T1W1/T2W1/STIR) showing blooming on susceptibility sequences and no post contrast enhancement were noted in bilateral vastus intermedius muscles seen in the lower one third of femur extending upto the metaphysis of distal femur suggestive of calcification (Figure 4). Similar T2/STIR hyper intensity was noted in the myofascial planes and muscle fibres of posterior compartment of bilateral thigh predominantly involving biceps femoris muscles. Bilateral knee joints were normal. The MRI findings were consistent with dermatomyositis.
Child was started on high dose corticosteroids along with oral methotrexate and hydroxychloroquine. Sun protection including use of sunblock on sun exposed areas was done. A physiotherapist was involved to as part of multidisciplinary team who instituted a safe exercise program. Child improved and muscle strength improved. Steroids were tapered and child was maintained on oral methotrexate and diltiazem for metastatic calcification. Subsequently child got readmitted in the next six months multiple times with right iliac crest cellulitis, cellulitis of right upper arm, cellulitis of bilateral thighs. Each time Staphylococcus aureus was obtained on aspiration and pus culture sensitivity and the child responded to intravenous vancomycin. In view of dystrophic calcification with superinfection child was started on Pamidronate infusion intravenously at 1 mg/kg/day for 3 days, once every 3 months. Kidney function tests and serum calcium was monitored during the therapy period. In addition, the child received fresh course of oral prednisolone at 2 mg/kg per day for 2 weeks tapered over the subsequent 6 months. In addition, child received intravenous immunoglobulin monthly for 6 months. Also, methotrexate was continued subcutaneously weekly for next 6 months. There was complete resolution of dystrophic calcinosis at all sites after 1year and good disease control without signs of myositis. Child was continued on diltiazem oral therapy, resumed school and was clinically well six months later.
Informed consent was obtained and signed from the patient regarding the use of patient health information for the purposes of writing a case report publication.
3. Discussion
Juvenile Dermatomyositis (JDM) is a rare autoimmune disorder with varied clinical presentation. It is characterised by skin manifestations, proximal myopathy, arthritis, calcinosis, interstitial lung disease and rarely gastrointestinal involvement
[2]
Sitthi C, Khaosut P. Characteristics and Outcomes of Juvenile Dermatomyositis (JDM) in Thai Children: Experience from a Tertiary Referral Center. J Med Assoc Thai 2023; 106: 867-74.
. The calcinosis is classically described as “dystrophic” and, insoluble calcium hydroxyapatite and carbonate-apatite get deposited in the skin and subcutaneous tissues.
[3]
Mormile I, Mosella F, Turco P, Napolitano F, de Paulis A, Rossi FW. Calcinosis Cutis and Calciphylaxis in Autoimmune Connective Tissue Diseases. Vaccines (Basel). 2023 Apr 25; 11(5): 898.
. The serum calcium and phosphorus levels in these children are normal. Its occurrence varies from 20 to 75%, depending on the racial characteristics and other unknown factors.
[4]
Cakmak F, Yener GO, Ozturk K, Baglan E, Sonmez HE, Demir F, Sozeri B, Ayaz NA. Initial manifestations and risk factors for calcinosis in juvenile dermatomyositis: A retrospective multicenter study. North Clin Istanb. 2023 Jun 21; 10(3): 298-305.
. Although calcinosis is much more frequent in JDM compared to adult dermatomyositis patients, it is frequently associated with prolonged state of persistent active disease and severe disease activity. Delay in diagnosis further adds to this risk especially in juvenile. In one of the largest series of JDM involving 48 children, the mean age at the onset of the disease was 7.6±3.6 years
[4]
Cakmak F, Yener GO, Ozturk K, Baglan E, Sonmez HE, Demir F, Sozeri B, Ayaz NA. Initial manifestations and risk factors for calcinosis in juvenile dermatomyositis: A retrospective multicenter study. North Clin Istanb. 2023 Jun 21; 10(3): 298-305.
. Monocyclic (60.4%), Polycyclic (14.6%), and Chronic persistent disease (25%) have been reported. In this series, 22.9% patients developed calcinosis. The presence of myalgia, livedo racemosa, skin hypopigmentation, and lower alanine aminotransferase (ALT) were associated with higher risk for calcinosis. A long duration of active, persistent disease is one of the important risk factors for calcinosis.
The exact pathogenetic mechanisms of calcinosis are poorly understood. Recently, neutrophil activation
[6]
Duvvuri B, Pachman LM, Morgan G, et al.: Neutrophil extracellular traps in tissue and periphery in juvenile dermatomyositis. Arthritis Rheumatol. 2020, 72: 348-358.
Duvvuri B, Pachman LM, Hermanson P, Wang T, Moore R, Ding-Hwa Wang D, Long A, Morgan GA, Doty S, Tian R, Sancak Y, Lood C. Role of mitochondria in the myopathy of juvenile dermatomyositis and implications for skeletal muscle calcinosis. J Autoimmun. 2023 Jul; 138: 103061.
, are gaining interest in disease pathogenesis. Calcinosis is reported to be common in young girls (usually of five years of age). The osteoarticular, cutaneous, pulmonary manifestations, and fever are seen in disease duration of around 3 years. Interleukin 1 and 6, tumour necrosis factor alpha, and innate immunity dysregulation are implicated in the pathogenesis. The ideal treatment of calcinosis in JDM is still unclear. The management of Calcinosis in dermatomyositis continues to be challenging. The lack of evidence in form of controlled clinical trials complicates the issue.
Bisphosphonates reduce bone turnover and inhibit macrophage activity reducing inflammation. Improvement of calcinosis in JDM patients treated with intravenous pamidronate or oral alendronate (70 mg weekly for 3 months) has recently been reported
[8]
Tayfur AC, Topaloglu R, Gulhan B, Bilginer Y. Bisphosphonates in juvenile dermatomyositis with dystrophic calcinosis. Mod Rheumatol. 2015 Jul; 25(4): 615-20.
. The disease activity has been demonstrated to be reduced with the use of Intravenous immunoglobulin (IVIG) by decreasing the deposition of membrane attack complex in the tissues and reducing T-cell activation. Among the different available therapies, IVIG has shown greatest therapeutic potential for calcinosis as per a recent retrospective analysis of the CARRA (Childhood Arthritis and Rheumatology Research Alliance) registry
[9]
Yi B, Wahezi D, Covert L, et al.: Treatment response and outcomes of 63 cases of juvenile dermatomyositis-associated calcinosis. Arthritis Rheumatol. 2023, 75: 18-20.
This hospital provides free treatment to all children referred from many smaller hospitals across North India. The following drugs were used as they were freely available at our centre. In our case we employed a combination of intravenous pamidronate 1 mg/kg/day for 3 consecutive days given 3 monthly for one year along with monthly intravenous immunoglobulin 2 gm/kg/month for 6 months along with subcutaneous methotrexate7.5 mg weekly as the child had extensive calcinosis which was very disabling. In addition, the child was getting repeated infections with Staphylococcus aureus and presenting with multiple abscesses. A repeat course of prednisolone 2 mg /kg/day was administered for 2 weeks followed by tapering by 5 mg every 2 weeks. Hydroxychloroquine 100 mg per day was also given along with oral diltiazem for one year. Diltiazem, a calcium channel blocker, is used in dermatomyositis to treat dystrophic calcinosis. particularly in juvenile dermatomyositis. It works by inhibiting calcium channels, which may prevent new calcium deposits from forming. While standard immunosuppressants do not always resolve calcinosis, diltiazem has been shown in case studies to reduce existing calcifications, improve function, and relieve symptoms. The child had complete resolution of the myositis and calcinosis by one year. She gained weight and height and started attending regular school after one year. Thus, it appears that multiple drugs can resolve extensive calcinosis specially when used in combination.
4. Conclusions
First line therapy for juvenile dermatomyositis includes steroids and methotrexate as a steroid sparing agent. In difficult cases, intravenous methylprednisolone has been tried. Dystrophic calcinosis is usually resistant to treatment. Other medications used are intravenous immunoglobulins, pamidronate, diltiazem and hydroxychloroquine. Our case did not respond to steroids and methotrexate treatment. A combination therapy including pamidronate, monthly intravenous immunoglobulin for 6 months and oral diltiazem provided complete, rapid and long-lasting resolution. Maintenance therapy with hydroxychloroquine and diltiazem for one more year provided complete relief and recovery from the disease. Thus, combination therapy appears to be promising in providing rapid remission without any adverse effects especially in challenging situations.
Abbreviations
ANA
Antinuclear Antibody
EMG
Electromyogram
MRI
Magnetic Resonance Imaging
JDM
Juvenile Dermatomyositis
BMI
Body Mass Index
ALT
Alanine Aminotransferase
Author Contributions
Ragini Ram:Data curation, Writing – original draft
Sumeet Singla:Conceptualization, Investigation and Supervision
Subramanian Anuradha: Data curation, Writing – review &editing
Krishnan Rajeshwari: Conceptualization, Conceptualization, Data curation, Writing –review & editing
Sitthi C, Khaosut P. Characteristics and Outcomes of Juvenile Dermatomyositis (JDM) in Thai Children: Experience from a Tertiary Referral Center. J Med Assoc Thai 2023; 106: 867-74.
Cakmak F, Yener GO, Ozturk K, Baglan E, Sonmez HE, Demir F, Sozeri B, Ayaz NA. Initial manifestations and risk factors for calcinosis in juvenile dermatomyositis: A retrospective multicenter study. North Clin Istanb. 2023 Jun 21; 10(3): 298-305.
Duvvuri B, Pachman LM, Morgan G, et al.: Neutrophil extracellular traps in tissue and periphery in juvenile dermatomyositis. Arthritis Rheumatol. 2020, 72: 348-358.
Duvvuri B, Pachman LM, Hermanson P, Wang T, Moore R, Ding-Hwa Wang D, Long A, Morgan GA, Doty S, Tian R, Sancak Y, Lood C. Role of mitochondria in the myopathy of juvenile dermatomyositis and implications for skeletal muscle calcinosis. J Autoimmun. 2023 Jul; 138: 103061.
Yi B, Wahezi D, Covert L, et al.: Treatment response and outcomes of 63 cases of juvenile dermatomyositis-associated calcinosis. Arthritis Rheumatol. 2023, 75: 18-20.
Ram, R., Singla, S., Anuradha, S., Rajeshwari, K. (2026). Combination Therapy for Extensive Tumoral Calcinosis in Juvenile Dermatomyositis. International Journal of Clinical Dermatology, 9(1), 29-33. https://doi.org/10.11648/j.ijcd.20260901.14
@article{10.11648/j.ijcd.20260901.14,
author = {Ragini Ram and Sumeet Singla and Subramanian Anuradha and Krishnan Rajeshwari},
title = {Combination Therapy for Extensive Tumoral Calcinosis in Juvenile Dermatomyositis},
journal = {International Journal of Clinical Dermatology},
volume = {9},
number = {1},
pages = {29-33},
doi = {10.11648/j.ijcd.20260901.14},
url = {https://doi.org/10.11648/j.ijcd.20260901.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcd.20260901.14},
abstract = {A 8-year-old girl presented with pain in bilateral hip and thigh with progressive difficulty in getting up and walking for last 2 years. Patient had difficulty with activities such as rising from a chair, climbing stairs, lifting objects, or washing her hair. There was no dysphagia, dysphonia, difficulty in swallowing and no weakness in the muscles of respiration. On examination child was very thin with areas of scalp alopecia. Multiple small, flat-topped, reddish-purple, non-tender papules were seen on the back of the hands and fingers indicative of Gottrons papules. Severe muscle wasting in both upper and lower limbs was seen. Gowers sign was positive. Extensive calcifications were seen in bilateral axillary region, around knee, hip and occipital region. ANA (Antinuclear Antibody) test by indirect immunofluorescence on Hep 2 cells showed speckled 2+ positivity (1:80). EMG (Electromyogram) and MRI (Magnetic Resonance Imaging) findings were consistent with dermatomyositis. Child was started on high dose corticosteroids along with oral methotrexate and hydroxychloroquin. Child improved and muscle strength improved. Subsequently child got readmitted in the next 6 months multiple times with cellulitis. Each time Staph aureus was obtained on aspiration and child responded to intravenous vancomycin. Child was started on Pamidronate infused intravenously at 1 mg/kg/day for 3 consecutive days every 3 months. Inaddition child received intravenous immunoglobulin monthly for 6 months. On follow-up after one year, there was complete clearance of calcinosis at all sites and good disease control without signs of myositis. Thus it appears that multiple drugs can resolve extensive calcinosis when used in combination.},
year = {2026}
}
TY - JOUR
T1 - Combination Therapy for Extensive Tumoral Calcinosis in Juvenile Dermatomyositis
AU - Ragini Ram
AU - Sumeet Singla
AU - Subramanian Anuradha
AU - Krishnan Rajeshwari
Y1 - 2026/02/26
PY - 2026
N1 - https://doi.org/10.11648/j.ijcd.20260901.14
DO - 10.11648/j.ijcd.20260901.14
T2 - International Journal of Clinical Dermatology
JF - International Journal of Clinical Dermatology
JO - International Journal of Clinical Dermatology
SP - 29
EP - 33
PB - Science Publishing Group
SN - 2995-1305
UR - https://doi.org/10.11648/j.ijcd.20260901.14
AB - A 8-year-old girl presented with pain in bilateral hip and thigh with progressive difficulty in getting up and walking for last 2 years. Patient had difficulty with activities such as rising from a chair, climbing stairs, lifting objects, or washing her hair. There was no dysphagia, dysphonia, difficulty in swallowing and no weakness in the muscles of respiration. On examination child was very thin with areas of scalp alopecia. Multiple small, flat-topped, reddish-purple, non-tender papules were seen on the back of the hands and fingers indicative of Gottrons papules. Severe muscle wasting in both upper and lower limbs was seen. Gowers sign was positive. Extensive calcifications were seen in bilateral axillary region, around knee, hip and occipital region. ANA (Antinuclear Antibody) test by indirect immunofluorescence on Hep 2 cells showed speckled 2+ positivity (1:80). EMG (Electromyogram) and MRI (Magnetic Resonance Imaging) findings were consistent with dermatomyositis. Child was started on high dose corticosteroids along with oral methotrexate and hydroxychloroquin. Child improved and muscle strength improved. Subsequently child got readmitted in the next 6 months multiple times with cellulitis. Each time Staph aureus was obtained on aspiration and child responded to intravenous vancomycin. Child was started on Pamidronate infused intravenously at 1 mg/kg/day for 3 consecutive days every 3 months. Inaddition child received intravenous immunoglobulin monthly for 6 months. On follow-up after one year, there was complete clearance of calcinosis at all sites and good disease control without signs of myositis. Thus it appears that multiple drugs can resolve extensive calcinosis when used in combination.
VL - 9
IS - 1
ER -
Ram, R., Singla, S., Anuradha, S., Rajeshwari, K. (2026). Combination Therapy for Extensive Tumoral Calcinosis in Juvenile Dermatomyositis. International Journal of Clinical Dermatology, 9(1), 29-33. https://doi.org/10.11648/j.ijcd.20260901.14
@article{10.11648/j.ijcd.20260901.14,
author = {Ragini Ram and Sumeet Singla and Subramanian Anuradha and Krishnan Rajeshwari},
title = {Combination Therapy for Extensive Tumoral Calcinosis in Juvenile Dermatomyositis},
journal = {International Journal of Clinical Dermatology},
volume = {9},
number = {1},
pages = {29-33},
doi = {10.11648/j.ijcd.20260901.14},
url = {https://doi.org/10.11648/j.ijcd.20260901.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcd.20260901.14},
abstract = {A 8-year-old girl presented with pain in bilateral hip and thigh with progressive difficulty in getting up and walking for last 2 years. Patient had difficulty with activities such as rising from a chair, climbing stairs, lifting objects, or washing her hair. There was no dysphagia, dysphonia, difficulty in swallowing and no weakness in the muscles of respiration. On examination child was very thin with areas of scalp alopecia. Multiple small, flat-topped, reddish-purple, non-tender papules were seen on the back of the hands and fingers indicative of Gottrons papules. Severe muscle wasting in both upper and lower limbs was seen. Gowers sign was positive. Extensive calcifications were seen in bilateral axillary region, around knee, hip and occipital region. ANA (Antinuclear Antibody) test by indirect immunofluorescence on Hep 2 cells showed speckled 2+ positivity (1:80). EMG (Electromyogram) and MRI (Magnetic Resonance Imaging) findings were consistent with dermatomyositis. Child was started on high dose corticosteroids along with oral methotrexate and hydroxychloroquin. Child improved and muscle strength improved. Subsequently child got readmitted in the next 6 months multiple times with cellulitis. Each time Staph aureus was obtained on aspiration and child responded to intravenous vancomycin. Child was started on Pamidronate infused intravenously at 1 mg/kg/day for 3 consecutive days every 3 months. Inaddition child received intravenous immunoglobulin monthly for 6 months. On follow-up after one year, there was complete clearance of calcinosis at all sites and good disease control without signs of myositis. Thus it appears that multiple drugs can resolve extensive calcinosis when used in combination.},
year = {2026}
}
TY - JOUR
T1 - Combination Therapy for Extensive Tumoral Calcinosis in Juvenile Dermatomyositis
AU - Ragini Ram
AU - Sumeet Singla
AU - Subramanian Anuradha
AU - Krishnan Rajeshwari
Y1 - 2026/02/26
PY - 2026
N1 - https://doi.org/10.11648/j.ijcd.20260901.14
DO - 10.11648/j.ijcd.20260901.14
T2 - International Journal of Clinical Dermatology
JF - International Journal of Clinical Dermatology
JO - International Journal of Clinical Dermatology
SP - 29
EP - 33
PB - Science Publishing Group
SN - 2995-1305
UR - https://doi.org/10.11648/j.ijcd.20260901.14
AB - A 8-year-old girl presented with pain in bilateral hip and thigh with progressive difficulty in getting up and walking for last 2 years. Patient had difficulty with activities such as rising from a chair, climbing stairs, lifting objects, or washing her hair. There was no dysphagia, dysphonia, difficulty in swallowing and no weakness in the muscles of respiration. On examination child was very thin with areas of scalp alopecia. Multiple small, flat-topped, reddish-purple, non-tender papules were seen on the back of the hands and fingers indicative of Gottrons papules. Severe muscle wasting in both upper and lower limbs was seen. Gowers sign was positive. Extensive calcifications were seen in bilateral axillary region, around knee, hip and occipital region. ANA (Antinuclear Antibody) test by indirect immunofluorescence on Hep 2 cells showed speckled 2+ positivity (1:80). EMG (Electromyogram) and MRI (Magnetic Resonance Imaging) findings were consistent with dermatomyositis. Child was started on high dose corticosteroids along with oral methotrexate and hydroxychloroquin. Child improved and muscle strength improved. Subsequently child got readmitted in the next 6 months multiple times with cellulitis. Each time Staph aureus was obtained on aspiration and child responded to intravenous vancomycin. Child was started on Pamidronate infused intravenously at 1 mg/kg/day for 3 consecutive days every 3 months. Inaddition child received intravenous immunoglobulin monthly for 6 months. On follow-up after one year, there was complete clearance of calcinosis at all sites and good disease control without signs of myositis. Thus it appears that multiple drugs can resolve extensive calcinosis when used in combination.
VL - 9
IS - 1
ER -