Obesity hypoventilation syndrome (OHS) is a serious condition characterized by obesity (BMI ≥ 30 kg/m2), daytime hypercapnia (PaCO2 ≥ 45 mmHg), and sleep-disordered breathing, without other identifiable causes of reduced alveolar ventilation, such as lung or neuromuscular disorders. The World Health Organization (WHO) defines morbid obesity as a BMI ≥ 35 kg/m2, which significantly increases the risk of obstructive sleep apnea (OSA) and poses challenges in airway management. This case report discusses the successful management of a morbidly obese patient (BMI = 51.3 kg/m2) suffering from hypoventilation and sleep apnea. Initially, the patient received continuous oxygen therapy via nasal prongs, but as symptoms worsened—marked by poor sleep quality and a significant drop in oxygen saturation at night—non-invasive ventilation (NIV) and high-flow nasal cannula (HFNC) were introduced. Proper positioning was also maintained to optimize breathing and prevent further deterioration. Despite the increased risk of prolonged ICU stays and extended mechanical ventilation in morbidly obese patients, this case demonstrates that a multimodal conservative approach can lead to successful outcomes within a short period. It highlights the effectiveness of non-surgical interventions in managing OHS and OSA while emphasizing the importance of early referral to specialized healthcare centers for timely and effective treatment, ultimately improving patient outcomes.
| Published in | International Journal of Clinical and Experimental Medical Sciences (Volume 11, Issue 3) |
| DOI | 10.11648/j.ijcems.20251103.11 |
| Page(s) | 28-32 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Obesity Hypoventilation Syndrome, Obstructive Sleep Apnea, Morbid Obesity
Test | Result | Normal range |
|---|---|---|
Hemoglobulin | 11.9 mg/dl | 12-16 mg/dl |
Urea | 19.82 mg/dl | 15-45 mg/dl |
Sodium | 142 mmol/L | 135-145 mmol/L |
Potassium | 3.27 mmol/L | 3.5-5.5 mmol/L |
SGPT/ALT | 99 U/L | <45 U/L |
SGOT/AST | 15 U/L | <40 U/L |
Magnesium (serum) | 1.77 mg/dl | 1.8-2.4 mg/dl |
NT-PROBNP | 1717 pg/ml | <300 pg/ml |
Creatinine | 0.74 mg/dl | 0.4-1.4 mg/dl |
Troponin | 0.39 ng/ml | 0-0.04 ng/ml |
Test | During the day of admission | 3rd day | 4th day | Normal range |
|---|---|---|---|---|
pH | 7.56 | 7.327 | 7.304 | 7.35-7.45 |
Pco2 | 41 | 69.8 | 77.8 | 35-35 mm hg |
Po2 | 54 | 38.4 | 32.3 | 80-108 mm hg |
Hco3- | 37.8 | 30.6 | 30.8 | 22-26 mEq/L |
BMI | Body Mass Index |
OHS | Obesity Hypoventilation Syndrome |
PaCO2 | Partial Pressure of Carbon Dioxide in Arterial Blood |
OSA | Obstructive Sleep Apnea |
NIV | Non-Invasive Ventilation |
HFNC | High-Flow Nasal Cannula |
ICU | Intensive Care Unit |
WHO | World Health Organization |
OSAHS | Obstructive Sleep Apnea Hypopnea Syndrome |
PTB | Pulmonary Tuberculosis |
MMRC | Modified Medical Research Council Dyspnea Scale |
MICU | Medical Intensive Care Unit |
GRBS | General Random Blood Sugar |
VBG | Venous Blood Gas Analysis |
MR | Mitral Regurgitation |
TR | Tricuspid Regurgitation |
EF | Ejection Fraction |
CPAP | Continuous Positive Airway Pressure |
BIPAP | Bilevel Positive Airway Pressure |
PAP | Positive Airway Pressure |
SGPT/ALT | Serum Glutamate Pyruvate Transaminase/Alanine Aminotransferase |
SGOT/AST | Serum Glutamic Oxaloacetic Transaminase/Aspartate Aminotransferase |
NT-proBNP | N-Terminal Prohormone of Brain Natriuretic Peptide |
pH | Potential of Hydrogen |
Pco2 | Partial Pressure of Carbon Dioxide |
Po2 | Partial Pressure of Oxygen |
HCO3- | Bicarbonate |
MDI | Metered-Dose Inhaler |
| [1] | Pıhtılı A, Bingöl Z, Kıyan E. The predictors of obesity hypoventilation syndrome in obstructive sleep apnea. Balkan Med J 2017; 34: 41-46. |
| [2] | Basoglu OK, Tasbakan MS. Comparison of clinical characteristics in patients with obesity hypoventilation syndrome and obese obstructive sleep apnea syndrome: A case-control study. Clinical Respiratory Journal 2014; 8: 167-174. |
| [3] | Mokhlesi B, Tulaimat A, Faibussowitsch I, Wang Y, Evans AT. Obesity hypoventilation syndrome: Prevalence and predictors in patients with obstructive sleep apnea. Sleep and Breathing 2007; 11: 117-124. |
| [4] | Park MH, Lee MJ, Kim JS, Park SH, Lee JH, Kim AJ. Veno-venous extracorporeal membrane oxygenation rescue for pulmonary hypertension and hypoxemic respiratory failure to obesity hypoventilation syndrome: a case report. Ann Palliat Med 2022; 11: 3341-3345. |
| [5] | Eldaabossi S, Alrashdan M, Aljanobi G et al. A rare association: Obesity hypoventilation syndrome with myasthenia gravis and systemic lupus erythematosus, case report. Respir Med Case Rep 2023; 44. |
| [6] | Feng H-S, Xie M-R, Meng Y, Pei H-S, Yu J-J. Successful use of remimazolam combined with remifentanil for painless gastroscopy in a patient with morbid obesity: a case report. Front Oncol 2024; 14. |
| [7] | Takaryanto D, Erna A, Suryadinata H. Pulmonary Hypertension in Obesity Hypoventilation Syndrome: A Case Report. 2017. |
| [8] | Utpat K, Desai U, Joshi JM, Bharmal RN. Obesity Hypoventilation Syndrome: New Insights in Diagnosis and Management. Indian J Sleep Med 2020; 15: 9-14. |
| [9] | Nacif SR, Aguiar IC, Fernandes De Oliveira E et al. Obesity-hypoventilation syndrome: Early diagnosis and immediate intervention-a case report. |
| [10] |
Liu C, Chen M-S, Yu H. Oncotarget 93168
www.impactjournals.com/oncotarget The relationship between obstructive sleep apnea and obesity hypoventilation syndrome: a systematic review and meta-analysis. 2017. |
| [11] | Heryana OM, Wijono H. Clinical condition of patients with Obesity Hypoventilation Syndrome (OHS): case report. Jurnal Teknologi Laboratorium 2023. |
| [12] | Saka DDS, Novida H. An Indonesian adult with obesity hypoventilation syndrome: a case report. Annals of Medicine & Surgery 2023; 85: 2169-2172. |
| [13] | Masa JF, Pépin JL, Borel JC, Mokhlesi B, Murphy PB, Sánchez-Quiroga MÁ. Obesity hypoventilation syndrome. European Respiratory Review 2019; 28. |
| [14] | Terla V, Rajbhandari GL, Kurian D, Pesola GR. A case of right ventricular dysfunction with right ventricular failure secondary to obesity hypoventilation syndrome. American Journal of Case Reports 2019; 20: 1487-1491. |
| [15] | Ozturk TC, Unluer E, Denizbasi A, Guneysel O, Onur O. Can NT-proBNP be used as a criterion for heart failure hospitalization in emergency room? 2011. |
| [16] | Tatusov M, Joseph JJ, Cuneo BM. A case report of malignant obesity hypoventilation syndrome: A weighty problem in our ICUs. Respir Med Case Rep 2017; 20: 38-41. |
APA Style
Shahi, A., Adhikari, B., Syangtan, B. B., Adhikari, U., Kafle, N. (2025). Management of Referred Case of Obesity Hypoventilation Syndrome with Obstructive Sleep Apnea of Morbidly Obese Patient: A Case Report. International Journal of Clinical and Experimental Medical Sciences, 11(3), 28-32. https://doi.org/10.11648/j.ijcems.20251103.11
ACS Style
Shahi, A.; Adhikari, B.; Syangtan, B. B.; Adhikari, U.; Kafle, N. Management of Referred Case of Obesity Hypoventilation Syndrome with Obstructive Sleep Apnea of Morbidly Obese Patient: A Case Report. Int. J. Clin. Exp. Med. Sci. 2025, 11(3), 28-32. doi: 10.11648/j.ijcems.20251103.11
@article{10.11648/j.ijcems.20251103.11,
author = {Anil Shahi and Bishaka Adhikari and Bir Bahadur Syangtan and Ulid Adhikari and Nischal Kafle},
title = {Management of Referred Case of Obesity Hypoventilation Syndrome with Obstructive Sleep Apnea of Morbidly Obese Patient: A Case Report
},
journal = {International Journal of Clinical and Experimental Medical Sciences},
volume = {11},
number = {3},
pages = {28-32},
doi = {10.11648/j.ijcems.20251103.11},
url = {https://doi.org/10.11648/j.ijcems.20251103.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcems.20251103.11},
abstract = {Obesity hypoventilation syndrome (OHS) is a serious condition characterized by obesity (BMI ≥ 30 kg/m2), daytime hypercapnia (PaCO2 ≥ 45 mmHg), and sleep-disordered breathing, without other identifiable causes of reduced alveolar ventilation, such as lung or neuromuscular disorders. The World Health Organization (WHO) defines morbid obesity as a BMI ≥ 35 kg/m2, which significantly increases the risk of obstructive sleep apnea (OSA) and poses challenges in airway management. This case report discusses the successful management of a morbidly obese patient (BMI = 51.3 kg/m2) suffering from hypoventilation and sleep apnea. Initially, the patient received continuous oxygen therapy via nasal prongs, but as symptoms worsened—marked by poor sleep quality and a significant drop in oxygen saturation at night—non-invasive ventilation (NIV) and high-flow nasal cannula (HFNC) were introduced. Proper positioning was also maintained to optimize breathing and prevent further deterioration. Despite the increased risk of prolonged ICU stays and extended mechanical ventilation in morbidly obese patients, this case demonstrates that a multimodal conservative approach can lead to successful outcomes within a short period. It highlights the effectiveness of non-surgical interventions in managing OHS and OSA while emphasizing the importance of early referral to specialized healthcare centers for timely and effective treatment, ultimately improving patient outcomes.
},
year = {2025}
}
TY - JOUR T1 - Management of Referred Case of Obesity Hypoventilation Syndrome with Obstructive Sleep Apnea of Morbidly Obese Patient: A Case Report AU - Anil Shahi AU - Bishaka Adhikari AU - Bir Bahadur Syangtan AU - Ulid Adhikari AU - Nischal Kafle Y1 - 2025/09/02 PY - 2025 N1 - https://doi.org/10.11648/j.ijcems.20251103.11 DO - 10.11648/j.ijcems.20251103.11 T2 - International Journal of Clinical and Experimental Medical Sciences JF - International Journal of Clinical and Experimental Medical Sciences JO - International Journal of Clinical and Experimental Medical Sciences SP - 28 EP - 32 PB - Science Publishing Group SN - 2469-8032 UR - https://doi.org/10.11648/j.ijcems.20251103.11 AB - Obesity hypoventilation syndrome (OHS) is a serious condition characterized by obesity (BMI ≥ 30 kg/m2), daytime hypercapnia (PaCO2 ≥ 45 mmHg), and sleep-disordered breathing, without other identifiable causes of reduced alveolar ventilation, such as lung or neuromuscular disorders. The World Health Organization (WHO) defines morbid obesity as a BMI ≥ 35 kg/m2, which significantly increases the risk of obstructive sleep apnea (OSA) and poses challenges in airway management. This case report discusses the successful management of a morbidly obese patient (BMI = 51.3 kg/m2) suffering from hypoventilation and sleep apnea. Initially, the patient received continuous oxygen therapy via nasal prongs, but as symptoms worsened—marked by poor sleep quality and a significant drop in oxygen saturation at night—non-invasive ventilation (NIV) and high-flow nasal cannula (HFNC) were introduced. Proper positioning was also maintained to optimize breathing and prevent further deterioration. Despite the increased risk of prolonged ICU stays and extended mechanical ventilation in morbidly obese patients, this case demonstrates that a multimodal conservative approach can lead to successful outcomes within a short period. It highlights the effectiveness of non-surgical interventions in managing OHS and OSA while emphasizing the importance of early referral to specialized healthcare centers for timely and effective treatment, ultimately improving patient outcomes. VL - 11 IS - 3 ER -
Chitwan Medical College, Tribhuvan University, Kirtipur, Nepal
Chitwan Medical College, Tribhuvan University, Kirtipur, Nepal
Chitwan Medical College, Tribhuvan University, Kirtipur, Nepal
Chitwan Medical College, Tribhuvan University, Kirtipur, Nepal
Chitwan Medical College, Tribhuvan University, Kirtipur, Nepal
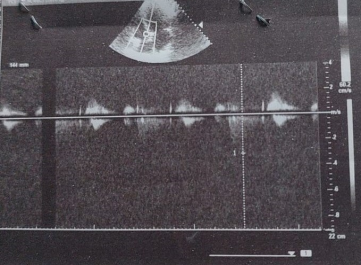
Figure 1. Echocardiographic results of the patient. (mitral regurgitation (MR), moderate tricuspid regurgitation (TR).
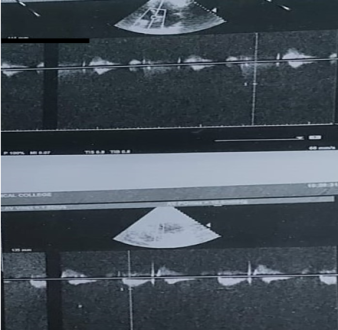
Figure 2. Echocardiographic results of the patient. (mitral regurgitation (MR), moderate tricuspid regurgitation (TR), and a dilated left atrium with a left ventricular ejection fraction of 60%).
Information

