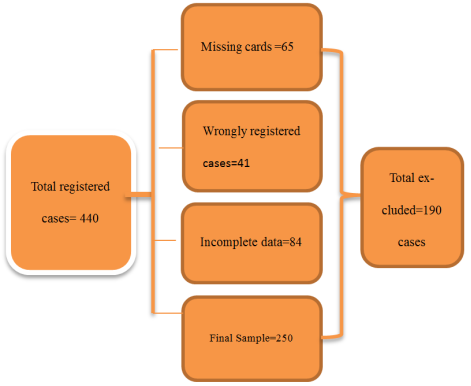
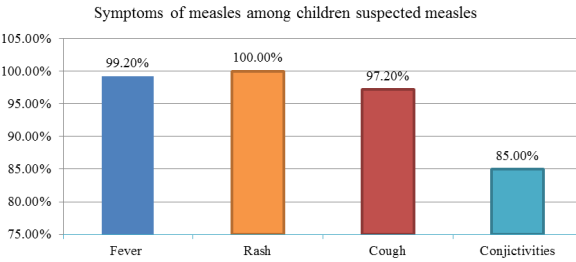
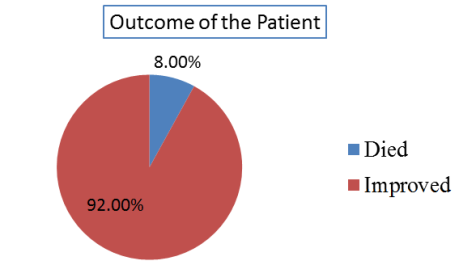
Background: Measles, a highly contagious viral disease, remains a significant cause of morbidity and mortality among children in low-resource settings like Ethiopia. Despite the availability of vaccines, outbreaks persist, particularly in areas with low immunization coverage. This study aims to explore the clinical characteristics and outcomes of children hospitalized with suspected measles at Jimma University Medical Center (JUMC). Understanding these aspects will provide critical insights for improving case management and reducing measles-related complications and deaths. Objectives: The primary objective of this study was to assess the clinical characteristics, complications, and outcomes of children hospitalized with suspected measles at JUMC. Methods: This was a hospital-based retrospective study that involved the review of medical records of children admitted to JUMC with suspected measles over the past five years. Data on demographic characteristics, clinical features, laboratory findings, treatment interventions, and patient outcomes were extracted and analyzed. Descriptive statistics summarized the data, while multivariate analysis was used to identify factors associated with adverse outcomes. Results: A total of 250 children were studied (100% response rate). Slightly over half (51.6%) were from urban areas. Children were predominantly male (57.2%) and mainly aged 5-10 years (50.8%). Common symptoms were rash (100%), fever (99.2%), cough (97.2%), and conjunctivitis (85.2%), while 100% had maculopapular rash, 41.2% had Koplik's spots, and 10.4% had lymphadenopathy on physical examination. 82% of the cases were complicated with severe pneumonia while other complications identified were diarrhea (61.6%), Upper Respiratory Tract Infection (48.4%), dehydration (18.8%), Out of the total cases, 230(92%) had good outcomes, while 20 (8%) cases were died. Regarding factors associated with Poor Outcomes (Multivariable Analysis), being unvaccinated against measles (AOR=4.53, P=0.005), having malnutrition (AOR=4.14, P=0.029) and Laryngotracheobronchitis (Croup) (AOR=11.96, p=0.008) were significantly associated with increased risk of death.
| Published in | International Journal of Clinical and Experimental Medical Sciences (Volume 11, Issue 5) |
| DOI | 10.11648/j.ijcems.20251105.12 |
| Page(s) | 64-76 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Measles, Clinical Characteristics, Outcomes, Children, Hospitalization, Jimma University Medical Center, Ethiopia
Study variables | Categories | Frequency | Percent% |
|---|---|---|---|
Age of the children | Less than 6 Months | 23 | 9.2 |
6 - < 12months | 33 | 13.2 | |
1 to <5 years | 50 | 20 | |
5 to <10 years | 127 | 50.8 | |
Greater than 10 years | 17 | 6.8 | |
Gender | Male | 140 | 56 |
Female | 110 | 44 | |
Religion of care giver | Muslim | 218 | 87.2 |
Orthodox | 17 | 6.8 | |
Protestant | 15 | 6.0 | |
Education of care giver | Cannot read write | 39 | 15.6 |
Elementary | 19 | 7.6 | |
High school | 95 | 38.0 | |
College and above | 97 | 38.8 | |
Residency | Urban | 129 | 51.6 |
Rural | 121 | 48.4 | |
Marital status of care giver | Single | 3 | 1.2 |
Married | 246 | 98.4 | |
Divorced | 1 | 0.4 | |
Education of the children | Not started | 170 | 68 |
Kindergarten | 30 | 12 | |
Elementary | 50 | 20 | |
Child care givers | Mother | 244 | 97.6 |
Father | 2 | 0.8 | |
Other | 4 | 1.6 | |
Occupation of care givers | Farmers | 42 | 16.8 |
Government employee | 24 | 9.6 | |
Daily labourer | 5 | 2.0 | |
Merchant | 25 | 10.0 | |
House wife | 153 | 61.2 | |
Maid | 1 | 0.4 | |
The care giver heard about measles previously | Yes | 50 | 20 |
No | 200 | 80 |
Study variables | Categories | Frequency | Percent% |
|---|---|---|---|
Was the child immunized? | Yes | 104 | 41.6 |
No | 119 | 47.6 | |
Unknown | 27 | 10.8 | |
If immunized, how many doses? (N=104) | MV1 only | 22 | 21.2 |
Both MV1 and MV2 | 82 | 78.8 | |
Contact history with the same illness? | Yes | 31 | 12.4 |
No | 56 | 22.4 | |
Unknown | 163 | 65.2 | |
Place of contact (N=31) | Home | 28 | 90.3 |
School | 3 | 9.7 | |
Visit to other health facility before visiting JUMC? | Yes | 145 | 58 |
No | 105 | 42 | |
Use of medication before visiting JUMC? | Yes | 108 | 43.2 |
No | 142 | 56.8 | |
Type of used medication | Ceftriaxone | 68 | 62.9 |
Ampicillin and gentamycin | 40 | 37.1 | |
Number of visits to JUMC hospital | First visit | 228 | 91.2 |
Revisit | 22 | 8.8 |
Study variables | Categories | Frequency | Percent% |
|---|---|---|---|
Rash | Yes | 250 | 100 |
No | 0 | 0 | |
Fever | Yes | 248 | 99.2 |
No | 2 | 0.8 | |
Cough | Yes | 243 | 97.2 |
No | 7 | 2.8 | |
Coryza | Yes | 187 | 74.8 |
No | 63 | 25.2 | |
Diarrhoea | Yes | 170 | 68 |
No | 80 | 32 | |
Conjunctivitis | Yes | 213 | 85.2 |
No | 37 | 14.8 | |
Convulsion | Yes | 7 | 2.8 |
No | 243 | 97.2 | |
Stridor | Yes | 15 | 6 |
No | 235 | 94 | |
Epistaxis | Yes | 2 | 0.8 |
No | 248 | 99.2 | |
Vomiting | Yes | 15 | 6 |
No | 235 | 94 |
Study variables | Categories | Frequency | Percent% |
|---|---|---|---|
Maculopapular rash | Yes | 250 | 100 |
No | 0 | 0 | |
Koplik’s spot | Yes | 103 | 41.2 |
No | 147 | 58.8 | |
Lymphadenopathy | Yes | 26 | 10.4 |
No | 224 | 89.6 | |
Pallor | Yes | 9 | 3.6 |
No | 241 | 96.4 | |
Stridor | Yes | 24 | 9.6 |
No | 226 | 90.4 |
Study variables | Categories | Frequency | Percent% | |
|---|---|---|---|---|
Had complication (N=250) | Yes | 250 | 100 | |
No | 0 | 0 | ||
Complications identified | Upper respiratory tract infection | Yes | 121 | 48.4 |
No | 129 | 51.6 | ||
Laryngotracheobronchitis | Yes | 24 | 9.6 | |
No | 228 | 91.2 | ||
Pneumonia/severe Pneumonia | Yes | 205 | 82 | |
No | 45 | 18 | ||
Acute otitis media | Yes | 4 | 1.6 | |
No | 246 | 98.4 | ||
Ophthalmic | Yes | 24 | 9.6 | |
No | 226 | 90.4 | ||
Encephalitis | Yes | 7 | 2.8 | |
No | 243 | 97.2 | ||
Febrile seizure | Yes | 0 | 0 | |
No | 250 | 100 | ||
AGE | Yes | 154 | 61.6 | |
No | 96 | 38.4 | ||
Dehydration due to AGE | Yes | 47 | 30.5 | |
No | 203 | 69.5 | ||
Comorbid illness | Yes | 68 | 27.2 | |
No | 182 | 78.2 | ||
Comorbidities | Malnutrition (N=68) | Yes | 42 | 61.7 |
No | 26 | 38.3 | ||
Others | Cardiac | 7 | 10.29 | |
Renal | 3 | 4.4 | ||
Malaria | 6 | 8.82 | ||
Others* | 10 | 14.7 | ||
Type of Malnutrition | MAM | 14 | 33.3 | |
SAM | 20 | 47.6 | ||
Stunted | 8 | 19.1 | ||
Study variables | Categories | Frequency | Percent% |
|---|---|---|---|
Vitamin A given | Yes | 245 | 98 |
No | 5 | 2 | |
Hydration fluid given | Yes | 155 | 62 |
No | 95 | 38 | |
Types of fluid given (N=155) | ORS | 130 | 83.9 |
IV | 5 | 3.2 | |
Both | 20 | 12.9 | |
Treated with antibiotics | Yes | 232 | 92.8 |
No | 18 | 7.2 | |
Types of antibiotics (N=232) | Ceftriaxone | 192 | 82.7 |
Amoxicillin | 12 | 5.2 | |
Ampicillin and gentamycin | 19 | 8.2 | |
Others * | 9 | 3.9 | |
Length of stay | <3 Days | 15 | 6 |
3-7 Days | 49 | 19.6 | |
>7 Days | 186 | 74.4 | |
Outcomes | Improved | 230 | 92 |
Died | 20 | 8 |
Variables | Categories | Outcomes | COR (95%, CI) | AOR (95%, CI) | P-value | |
|---|---|---|---|---|---|---|
Died (poor) | Improved (Good) | |||||
Gender | Female | 13(5.2%) | 97(38.8%) | 2.55(0.98-6.62) | 3.01(0.713-12.7) | 0.134 |
Male | 7(2.8%) | 133(53.2%) | 1 | |||
Preexisting comorbidity | No | 7(2.8%) | 17(570%) | 1 | ||
Yes | 13(5.2%) | 55(22%) | 5.91(2.25-45.5) | 1.54(0.3-7.91) | 0.605 | |
Malnutrition | No | 8(3.2%) | 200(80%) | 1 | ||
Yes | 12(4.8%) | 30(12%) | 10(3.78-26.5) | 4.14(1.16-14.83) | 0.029* | |
Diarrhea | No | 11(4.4%) | 88(35.2%) | 1 | ||
Yes | 9(3.6%) | 142(56.8%) | 0.51(0.2-1.27) | 0.77(0.19-23.16) | 0.715 | |
Visit to health facility before arrival | No | 12(4.8%) | 93(37.2%) | 1 | ||
Yes | 8(3.2%) | 137(54.8%) | 0.45(0.18-1.15) | 1.19(0.27-5.31) | 0.813 | |
Croup | No | 13(5.2%) | 213(85.2) | 1 | ||
Yes | 7(2.8%) | 17(6.8%) | 6.75(2.37-19.2) | 11.96(1.89-75.4) | 0.008* | |
Vaccination for measles | No | 13(5.2%) | 110(44%) | 3.86(1.07-13.9) | 4.53(1.07-19.12) | 0.04* |
Unknown | 4(1.6%) | 22(8.8%) | 5.94(1.24-28.5) | 3.08(0.43-22.1) | 0.263 | |
Yes | 3(1.2%) | 98(39.2%) | 1 | |||
AGE | Acute Gastroenteritis |
AR | Attack Rate |
CDC | Center of Disease Control and Prevention |
CFR | Case Fatality Rate |
CKD | Chronic Kidney Disease |
EPI | Expanded Programme on Immunization |
HIV/AIDS | Human Immunodeficiency Virus/ Acquired Immunodeficiency Syndrome |
JUMC | Jimma University Medical Center |
LTB | Laryngotracheobronchitis |
MCH | Maternal and Child Health |
MCV | Measles Containing Vaccine |
OPD | Out Patient Department |
PICU | Pediatric Intensive Care Unit |
PI | Principal Investigator |
SPSS | Statistical Package for the Social Sciences |
WHO | World Health Organization |
| [1] | Nazir A, Oduoye MO, Tunde AM, Hafsat A, Guta JG, Akilimali A, et al. Measles outbreak in Ethiopia amid COVID-19: an effect of war-induced hampering of vaccination and pandemic. Annals of Medicine & Surgery. 2023 Apr; 85(4): 1336-9. |
| [2] | Tefera SF, Admasu N, Abebe H, Feyisa GC, Midaksa G. Measles outbreak investigation in Tocha district, southwestern Ethiopia: an unmatched case-control study. Front Public Health. 2024 Apr 10; 12: 1331798. |
| [3] | Poletti P, Parlamento S, Fayyisaa T, Feyyiss R, Lusiani M, Tsegaye A, et al. The hidden burden of measles in Ethiopia: how distance to hospital shapes the disease mortality rate. BMC Med. 2018 Dec; 16(1): 177. |
| [4] | Mohamud AK, Ahmed OA, Ali IA, Dirie NI. Demographical, clinical, and complication differences between vaccinated and unvaccinated hospitalized children with measles in mogadishu somalia: a hospital-based retrospective cohort study. Annals of Medicine & Surgery. 2023 May; 85(5): 1550-5. |
| [5] | Salman Y, Shaeen SK, Khan HA, Islam Z, Essar MY. The effect of child malnourishment on measles spread amidst the COVID-19 pandemic in Afghanistan. Annals of Medicine & Surgery [Internet]. 2022 Jun [cited 2024 Sep 10]; 78. Available from: |
| [6] | Tsegaye G, Gezahegn Y, Tesfaye A, Mulatu G, Bulcha GG, Berhanu N. Measles Outbreak Investigation in Guradamole District of Bale Zone, South Eastern Ethiopia, 2021. IDR. 2022 Feb; Volume 15: 669-83. |
| [7] | Auwal BM, Adegoke AA, Zafar H, Noor Z, Oduoye MO. Breaking the vaccination challenges to fight measles in Ethiopia. International Journal of Surgery: Global Health [Internet]. 2024 Jan [cited 2024 Sep 13]; 7(1). |
| [8] |
WHO. Measles - Ethiopia. World Health Organization. 2023; 9291 (May): 1-6.
https://www.who.int/emergencies/disease-outbreak-news/item/2023-DON460 |
| [9] | World Health Organization. Guide for clinical case management and infection prevention and control during a measles outbreak [Internet]. Geneva: World Health Organization; 2020 [cited 2024 Aug 31]. |
| [10] | Moss WJ. Measles. The Lancet. 2017 Dec; 390(10111): 2490-502. |
| [11] | Stein CE, Birmingham M, Kurian M, Duclos P, Strebel P. The Global Burden of Measles in the Year 2000-A Model that Uses Country‐Specific Indicators. J INFECT DIS. 2003 May 15; 187(s1): S8-14. |
| [12] | M. U. I, S. S. E, U. A. I, B. N. M, S. S. U, M. N. The Reemergence of Measles: Epidemiology, Pathogenesis, Laboratory Diagnosis and Management. S Asian J Res Microbiol. 2024 Aug 7; 18(8): 8-17. |
| [13] | Hassan MY, Mohamud RYH, Kassim MM, Hussein AI, Adam MK, Akbulut UE, et al. Clinical characteristics and outcomes of patients hospitalized with measles during an outbreak in Somalia. IJID Regions. 2023 Sep; 8: 31-5. |
| [14] | Masresha BG, Hatcher C, Lebo E, Tanifum P, Bwaka AM, Minta AA, et al. Progress Toward Measles Elimination - African Region, 2017-2021. MMWR Morb Mortal Wkly Rep. 2023 Sep 8; 72(36): 985-91. |
| [15] | Kalil FS, Gemeda DH, Bedaso MH, Wario SK. Measles outbreak investigation in Ginnir district of Bale zone, Oromia region, Southeast Ethiopia, May 2019. Pan Afr Med J [Internet]. 2020 May 14 [cited 2024 Sep 4]; 36. |
| [16] | Kalil FS, Bedaso MH, Abdulle MS, Mohammed NU. Evaluation of Measles Surveillance Systems in Ginnir District, Bale Zone, Southeast Ethiopia: A Concurrent Embedded Mixed Quantitative/Qualitative Study. RMHP. 2021 Mar; Volume 14: 997-1008. |
| [17] | Yitbarek K, Tilahun T, Debela T, Abdena D, Girma T. Measles epidemiology and vaccination coverage in Oromia Region, Ethiopia: Evidence from surveillance, 2011-2018. Vaccine. 2021 Jul; 39(31): 4351-8. |
| [18] | Wudu H, Alemu C, Minalu W, Berelie H, Bantie D. Trend and forecast of measles disease, in East Gojjam Zone, Amhara Region, Northwest Ethiopia, 2023: a crossectional study. BMC Res Notes. 2024 Dec 24; 17(1): 383. |
| [19] | Shimelis Y, Asrat A, Tadege T, Feleke SF. Measles outbreak investigation in Berhet District, North Shewa, Ethiopia. Front Public Health. 2024 May 2; 12: 1330205. |
| [20] | Patel M, Lee AD, Clemmons NS, Redd SB, Poser S, Blog D, et al. National Update on Measles Cases and Outbreaks - United States, January 1-October 1, 2019. MMWR Morb Mortal Wkly Rep. 2019 Oct 11; 68(40): 893-6. |
| [21] | Isezuo K, Yusuf T, Ibitoye P, Sanni M, Jiya N, Sani U, et al. A 5-year review of measles cases admitted into the emergency paediatric unit of a tertiary hospital in Sokoto, North-Western Nigeria. Sahel Med J. 2018; 21(3): 122. |
| [22] | Commey JOO, Richardson JE. Measles in Ghana-1973-1982. Annals of Tropical Paediatrics. 1984 Sep; 4(3): 189-94. |
| [23] | Alsulaiman J, Kheirallah K, Alrawashdeh A, Abu Sanad Z, Al-Mnayyis A, Yassin A, et al. Clinical and Demographic Characteristics of Hospitalized Pediatric Measles Cases; The 2023 Outbreak in Northern Jordan. IDR. 2025 Apr; Volume 18: 1773-83. |
| [24] | Sbarra AN, Mosser JF, Jit M, Ferrari M, Ramshaw RE, O’Connor P, et al. Estimating national-level measles case-fatality ratios in low-income and middle-income countries: an updated systematic review and modelling study. The Lancet Global Health. 2023 Apr; 11(4): e516-24. |
| [25] | Mehta KP, Patel AM, Patel A. Clinical Profile, Complications and Outcomes of Measles among Children: An Observational Study from a Tertiary Care Hospital, South Gujarat, India. JCDR [Internet]. 2023 [cited 2024 Aug 31]. |
| [26] | Fortenberry JD. Severe Laryngotracheobronchitis Complicating Measles. Arch Pediatr Adolesc Med. 1992 Sep 1; 146(9): 1040. |
| [27] | Arya LS, Taana I, Tahiri C, Saidali A, Singh M. Spectrum of complications of measles in Afghanistan: a study of 784 cases. J Trop Med Hyg. 1987 Jun; 90(3): 117-22. |
| [28] | Domai FM, Agrupis KA, Han SM, Sayo AR, Ramirez JS, Nepomuceno R, et al. Measles outbreak in the Philippines: epidemiological and clinical characteristics of hospitalized children, 2016-2019. The Lancet Regional Health - Western Pacific. 2022 Feb; 19: 100334. |
| [29] | Tariku MK, Worede DT, Belete AH, Bante SA, Misikir SW. Attack rate, case fatality rate and determinants of measles infection during a measles outbreak in Ethiopia: systematic review and meta-analysis. BMC Infect Dis. 2023 Nov 2; 23(1): 756. |
APA Style
Tolera, B., Fentie, K., Lemessa, S. (2025). Clinical Characteristics and Outcomes of Children Hospitalized with Suspected Measles at Jimma University Medical Center, Ethiopia, Cross Sectional Study. International Journal of Clinical and Experimental Medical Sciences, 11(5), 64-76. https://doi.org/10.11648/j.ijcems.20251105.12
ACS Style
Tolera, B.; Fentie, K.; Lemessa, S. Clinical Characteristics and Outcomes of Children Hospitalized with Suspected Measles at Jimma University Medical Center, Ethiopia, Cross Sectional Study. Int. J. Clin. Exp. Med. Sci. 2025, 11(5), 64-76. doi: 10.11648/j.ijcems.20251105.12
@article{10.11648/j.ijcems.20251105.12,
author = {Birhanu Tolera and Kelemu Fentie and Sabona Lemessa},
title = {Clinical Characteristics and Outcomes of Children Hospitalized with Suspected Measles at Jimma University Medical Center, Ethiopia, Cross Sectional Study
},
journal = {International Journal of Clinical and Experimental Medical Sciences},
volume = {11},
number = {5},
pages = {64-76},
doi = {10.11648/j.ijcems.20251105.12},
url = {https://doi.org/10.11648/j.ijcems.20251105.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcems.20251105.12},
abstract = {Background: Measles, a highly contagious viral disease, remains a significant cause of morbidity and mortality among children in low-resource settings like Ethiopia. Despite the availability of vaccines, outbreaks persist, particularly in areas with low immunization coverage. This study aims to explore the clinical characteristics and outcomes of children hospitalized with suspected measles at Jimma University Medical Center (JUMC). Understanding these aspects will provide critical insights for improving case management and reducing measles-related complications and deaths. Objectives: The primary objective of this study was to assess the clinical characteristics, complications, and outcomes of children hospitalized with suspected measles at JUMC. Methods: This was a hospital-based retrospective study that involved the review of medical records of children admitted to JUMC with suspected measles over the past five years. Data on demographic characteristics, clinical features, laboratory findings, treatment interventions, and patient outcomes were extracted and analyzed. Descriptive statistics summarized the data, while multivariate analysis was used to identify factors associated with adverse outcomes. Results: A total of 250 children were studied (100% response rate). Slightly over half (51.6%) were from urban areas. Children were predominantly male (57.2%) and mainly aged 5-10 years (50.8%). Common symptoms were rash (100%), fever (99.2%), cough (97.2%), and conjunctivitis (85.2%), while 100% had maculopapular rash, 41.2% had Koplik's spots, and 10.4% had lymphadenopathy on physical examination. 82% of the cases were complicated with severe pneumonia while other complications identified were diarrhea (61.6%), Upper Respiratory Tract Infection (48.4%), dehydration (18.8%), Out of the total cases, 230(92%) had good outcomes, while 20 (8%) cases were died. Regarding factors associated with Poor Outcomes (Multivariable Analysis), being unvaccinated against measles (AOR=4.53, P=0.005), having malnutrition (AOR=4.14, P=0.029) and Laryngotracheobronchitis (Croup) (AOR=11.96, p=0.008) were significantly associated with increased risk of death.
},
year = {2025}
}
TY - JOUR T1 - Clinical Characteristics and Outcomes of Children Hospitalized with Suspected Measles at Jimma University Medical Center, Ethiopia, Cross Sectional Study AU - Birhanu Tolera AU - Kelemu Fentie AU - Sabona Lemessa Y1 - 2025/09/23 PY - 2025 N1 - https://doi.org/10.11648/j.ijcems.20251105.12 DO - 10.11648/j.ijcems.20251105.12 T2 - International Journal of Clinical and Experimental Medical Sciences JF - International Journal of Clinical and Experimental Medical Sciences JO - International Journal of Clinical and Experimental Medical Sciences SP - 64 EP - 76 PB - Science Publishing Group SN - 2469-8032 UR - https://doi.org/10.11648/j.ijcems.20251105.12 AB - Background: Measles, a highly contagious viral disease, remains a significant cause of morbidity and mortality among children in low-resource settings like Ethiopia. Despite the availability of vaccines, outbreaks persist, particularly in areas with low immunization coverage. This study aims to explore the clinical characteristics and outcomes of children hospitalized with suspected measles at Jimma University Medical Center (JUMC). Understanding these aspects will provide critical insights for improving case management and reducing measles-related complications and deaths. Objectives: The primary objective of this study was to assess the clinical characteristics, complications, and outcomes of children hospitalized with suspected measles at JUMC. Methods: This was a hospital-based retrospective study that involved the review of medical records of children admitted to JUMC with suspected measles over the past five years. Data on demographic characteristics, clinical features, laboratory findings, treatment interventions, and patient outcomes were extracted and analyzed. Descriptive statistics summarized the data, while multivariate analysis was used to identify factors associated with adverse outcomes. Results: A total of 250 children were studied (100% response rate). Slightly over half (51.6%) were from urban areas. Children were predominantly male (57.2%) and mainly aged 5-10 years (50.8%). Common symptoms were rash (100%), fever (99.2%), cough (97.2%), and conjunctivitis (85.2%), while 100% had maculopapular rash, 41.2% had Koplik's spots, and 10.4% had lymphadenopathy on physical examination. 82% of the cases were complicated with severe pneumonia while other complications identified were diarrhea (61.6%), Upper Respiratory Tract Infection (48.4%), dehydration (18.8%), Out of the total cases, 230(92%) had good outcomes, while 20 (8%) cases were died. Regarding factors associated with Poor Outcomes (Multivariable Analysis), being unvaccinated against measles (AOR=4.53, P=0.005), having malnutrition (AOR=4.14, P=0.029) and Laryngotracheobronchitis (Croup) (AOR=11.96, p=0.008) were significantly associated with increased risk of death. VL - 11 IS - 5 ER -
Department of Pediatric and Child Health Institute of Health, Jimma University, Jimma, Ethiopia
Jimma University Medical Center, Jimma, Ethiopia
Department of Pediatric and Child Health Institute of Health, Jimma University, Jimma, Ethiopia
Information