Aims: We aimed to evaluate the influence of ostial lesions on the predicted probability of success in patients undergoing percutaneous coronary interventions (PCIs) for chronic total occlusions (CTOs). Methods: 245 consecutive patients who underwent CTO PCIs at Coburg Hospital, Coburg, Germany between 2017 and 2023 were included. Patients with and without ostial lesions were compared. Logistic regression models were used to estimate the potential of ostial lesion as additional predictor for success beside J-Score. Results: 245 patients were included. Of those, 48 Patients (19.6%) had ostial lesions. The ostial lesion group exhibited significantly higher pro-B-type natriuretic peptide levels (1644 pg./ml vs. 963 pg./ml, p=0.034) than the non-ostial lesion group. The final success rate was lower in the ostial lesion group than in the non-ostial lesion group (64.6% vs. 81.7%, p=0.018). The ostial lesion group had higher J-scores than the non-ostial lesion group, indicating more complex lesions (median: 2.5 vs. 2.0, p=0.005). Antegrade access was more applied in non-ostial lesion group (89.8% vs. 68.8% p=0.001), whereas retrograde access was more applied in ostial lesion group. (33.3% vs. 7.6%, p=<0.001) A logistic regression analysis showed a statistically significant association between higher J-scores and ostial lesions (OR, 2.4; p=0.003). Conclusion: The presence of ostial CTO is associated with higher lesion complexity and lower technical and procedural success rates. Presence of ostial CTO might be included as an additional factor in the currently used CTO scores to predict the difficulty and success rate of CTO procedure.
| Published in | International Journal of Cardiovascular and Thoracic Surgery (Volume 11, Issue 5) |
| DOI | 10.11648/j.ijcts.20251105.11 |
| Page(s) | 63-73 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Chronic Total Occlusion, Percutaneous Coronary Intervention, Ostial Lesions, Risk Prediction
Characteristics | Non-ostial lesion | Ostial lesion | Total | p-value | |||
|---|---|---|---|---|---|---|---|
M | SD | M | SD | M | SD | ||
Age of the patient at the intervention (yr) | 67.2 | 10.7 | 67.4 | 10.6 | 67.2 | 10.6 | 0.6 |
Body-Mass-Index (kg/m2) | 30.6 | 6.3 | 31.6 | 5.3 | 30.8 | 6.1 | 0.12 |
Pro-B-Type Natriuretic Peptide (pg/ml) | 2735 | 2682 | 3304 | 6971 | 3188 | 6336 | 0.034 |
Low-density lipoprotein prior to the intervention (mg/dl) | 100.6 | 45.1 | 93.6 | 46.8 | 99.3 | 45.3 | 0.29 |
High-density lipoprotein prior to the intervention (mg/dl) | 44.1 | 13.9 | 39.1 | 13.6 | 43.1 | 13.9 | 0.018 |
Glucose levels at the time of intervention (mg/dl) | 131.4 | 46.9 | 136.4 | 47.5 | 132.4 | 47 | 0.17 |
HbA1c at the time of intervention (%) | 6.4 | 1.4 | 6.5 | 1.5 | 6.4 | 1.5 | 0.24 |
Glomerular filtration rate at the time of intervention (ml/min) | 70.9 | 23.3 | 68.9 | 23 | 70.5 | 23.2 | 0.44 |
Serum Creatinine at the time of intervention (mg/dl) | 1.2 | 0.7 | 1.2 | 0.3 | 1.2 | 0.7 | 0.12 |
Left ventricular ejection fraction at the time of intervention (%) | 51.2 | 12.4 | 49.4 | 13 | 50.8 | 12.5 | 0.4 |
Characteristics | Non-ostial lesion | Ostial lesion | Total | p-value | |||
|---|---|---|---|---|---|---|---|
N | % | N | % | N | % | ||
Male | 146 | 74.1% | 40 | 83.3% | 186 | 75.9% | 0.18 |
Hypertension | 178 | 90.4% | 45 | 93.8% | 223 | 91% | 0.46 |
Diabetes mellitus | 75 | 38% | 20 | 41.7% | 95 | 38.8% | 0.65 |
Insulin dependent diabetes mellitus | 34 | 17.3% | 9 | 18.7% | 43 | 17.5% | 0.81 |
Smoker | 61 | 31% | 12 | 25% | 73 | 29.8% | 0.42 |
Family history of CTO or CAD | 41 | 20.8% | 10 | 20.8% | 51 | 20.8% | 0.99 |
Hyperlipidemia | 168 | 85.3% | 45 | 93.7% | 213 | 86.9% | 0.12 |
Prior intervention with coronary artery bypass grafting | 14 | 7.1% | 5 | 10.4% | 19 | 7.8% | 0.44 |
Prior percutaneous coronary intervention | 139 | 70.6% | 36 | 75% | 175 | 71.4% | 0.54 |
Prior stroke | 20 | 10.1% | 2 | 4.2% | 22 | 9% | 0.19 |
Chronic kidney disease | 62 | 31.5% | 21 | 43.7% | 83 | 33.9% | 0.11 |
Atrial fibrillation | 45 | 23% | 12 | 25% | 57 | 23.5% | 0.78 |
Existing lung disease prior to the intervention (COPD, Asthma) | 25 | 12.8% | 9 | 18.7% | 34 | 14% | 0.29 |
Left ventricular ejection fraction below 35% | 28 | 14.2% | 9 | 18.7% | 37 | 15.1% | 0.43 |
VES_or_VT at presentation | 23 | 12% | 6 | 13% | 29 | 12% | 0.8 |
Symptoms of angina pectoris | 94 | 47.7% | 28 | 58.3% | 122 | 49.8% | 0.19 |
NYHA Classification - The Stages of Heart Failure | |||||||
NYHA I | 93 | 47.2% | 19 | 40% | 112 | 46% | 0.63 |
NYHA II | 67 | 34% | 21 | 44% | 88 | 36% | 0.63 |
NYHA III | 33 | 17% | 7 | 15% | 40 | 16% | 0.63 |
NYHA IV | 4 | 2% | 1 | 2% | 5 | 2% | 0.63 |
Non-ostial lesion | Ostial lesion | Total | p-value | ||||
|---|---|---|---|---|---|---|---|
N | % | N | % | N | % | ||
Antegrade approach | 177 | 89.8% | 33 | 68.7% | 210 | 85.7% | <0.001 |
Retrograde approach | 15 | 7.6% | 16 | 33.3% | 31 | 12.6% | <0.001 |
Success_1st- Attempt | 129 | 65.5% | 25 | 52.1% | 154 | 62.9% | 0.085 |
Success_2nd- Attempt | 32 | 16.2% | 6 | 12.5% | 38 | 15.5% | 0.52 |
Final Success | 161 | 81.7% | 31 | 64.6% | 192 | 78.4% | 0.01 |
Perforation | 15 | 7.6% | 5 | 10.4% | 20 | 8.2% | 0.53 |
Cardiac tamponade | 2 | 1% | 1 | 2% | 3 | 1.2% | 0.55 |
Myocardial infarction (MI) | 1 | 0.5% | 1 | 2% | 2 | 0.8% | 0.28 |
Side_branch_occlusion | 14 | 7.1% | 6 | 12.5% | 20 | 8.2% | 0.22 |
Stroke | 1 | 0.5% | 0 | 0.0% | 1 | 0.4% | 0.62 |
Cardiopulmonary resuscitation (CPR) | 4 | 2% | 2 | 4.2% | 6 | 2.4% | 0.39 |
Death | 1 | 0.5% | 1 | 2% | 2 | 0.8% | 0.28 |
Acute kidney injury | 9 | 4.6% | 2 | 4.2% | 11 | 4.5% | 0.9 |
Vessel complication | |||||||
Non-Complication | 192 | 97.5% | 47 | 98% | 239 | 97.5% | 0.9 |
Pseudoenurysm | 3 | 1.5% | 1 | 2.1% | 4 | 1.6% | |
Hemorrhagic shock | 1 | 0.5% | 0 | 0% | 1 | 0.4% | |
Vessel occlusion | 1 | 0.5% | 0 | 0% | 1 | 0.4% | |
Graft occlusion within 3 months after intervention | 5 | 2.7% | 2 | 4.3% | 7 | 3% | 0.56 |
In-Stent-Restenosis within 3 months after intervention | 7 | 3.8% | 4 | 8.7% | 11 | 4.8% | 0.16 |
Myocardial infarction within 3 months after intervention | 3 | 1.6% | 1 | 2.2% | 4 | 1.7% | 0.8 |
Angina pectoris after 3 Months | 34 | 18.5% | 10 | 21.7% | 44 | 19.1% | 0.61 |
VES_or_VT after 3 Months | 8 | 4.3% | 1 | 2.2% | 9 | 3.9% | 0.5 |
AKI | Acute Kidney Injury |
AP | Angina Pectoris |
CABG | Coronary Artery Bypass Grafting |
CAD | Coronary Artery Disease |
CASTLE Score | Chronic Total Coronary Occlusion Intervention Procedural Success Score From |
CI | Confidence Interval |
CMRI | Cardiac Magnetic Resonance Imaging |
COPD | Chronic Obstructive Pulmonary Disease |
CPR | Cardiopulmonary Resuscitation |
CTO | Chronic Total Occlusions |
ECG | Electrocardiogram |
J-Score | J-CTO Score (Multicenter CTO Registry of Japan) |
HbA1c | Hemoglobin A1c |
IQR | Interquartile Range |
ISR | Instent-Restenosis |
LAD | Left Ascending Artery |
LVEF | Left Ventricular Ejection Fraction |
MACE | Major Adverse Cardiac Events |
MI | Myocardial Infarction |
NT-Pro-BNP | N-terminal pro–B-type Natriuretic Peptide |
NYHA | New York Heart Association |
OCT | Optical Coherence Tomography |
OR | Odds Ratio |
PCI | Percutaneous Coronary Interventions |
PROGRESS-CTO | Prospective Global Registry for the Study of Chronic Total Occlusion Intervention |
ROC | Receiver Operating Characteristic |
SYNTAX Score | Synergy Between PCI With Taxus and Cardiac Surgery |
TIMI | Thrombolysis in Myocardial Infarction |
VES | Ventricular Extrasystole |
VT | Ventricular Tachycardia |
| [1] | Brilakis ES, Mashayekhi K, Tsuchikane E, Abi Rafeh N, Alaswad K, Araya M, et al. Guiding Principles for Chronic Total Occlusion Percutaneous Coronary Intervention. Circulation. 2019; 140(5): 420-33. |
| [2] | Azzalini L, Jolicoeur EM, Pighi M, Millan X, Picard F, Tadros VX, et al. Epidemiology, Management Strategies, and Outcomes of Patients With Chronic Total Coronary Occlusion. Am J Cardiol. 2016; 118(8): 1128-35. |
| [3] | Jeroudi OM, Alomar ME, Michael TT, El Sabbagh A, Patel VG, Mogabgab O, et al. Prevalence and management of coronary chronic total occlusions in a tertiary Veterans Affairs hospital. Catheter Cardiovasc Interv. 2014; 84(4): 637-43. |
| [4] | Werner GS, Martin-Yuste V, Hildick-Smith D, Boudou N, Sianos G, Gelev V, et al. A randomized multicentre trial to compare revascularization with optimal medical therapy for the treatment of chronic total coronary occlusions. Eur Heart J. 2018; 39(26): 2484-93. |
| [5] | Obedinskiy AA, Kretov EI, Boukhris M, Kurbatov VP, Osiev AG, Ibn Elhadj Z, et al. The IMPACTOR-CTO Trial. JACC Cardiovasc Interv. 2018; 11(13): 1309-11. |
| [6] | Azzalini L, Karmpaliotis D, Santiago R, Mashayekhi K, Di Mario C, Rinfret S, et al. Contemporary Issues in Chronic Total Occlusion Percutaneous Coronary Intervention. JACC Cardiovasc Interv. 2022; 15(1): 1-21. |
| [7] | Azzalini L, Vo M, Dens J, and Agostoni P. Myths to Debunk to Improve Management, Referral, and Outcomes in Patients With Chronic Total Occlusion of an Epicardial Coronary Artery. Am J Cardiol. 2015; 116(11): 1774-80. |
| [8] | Azzalini L, Dautov R, Ojeda S, Benincasa S, Bellini B, Giannini F, et al. Procedural and Long-Term Outcomes of Percutaneous Coronary Intervention for In-Stent Chronic Total Occlusion. JACC Cardiovasc Interv. 2017; 10(9): 892-902. |
| [9] | Ojeda S, Azzalini L, Chavarria J, Serra A, Hidalgo F, Benincasa S, et al. One Versus 2-stent Strategy for the Treatment of Bifurcation Lesions in the Context of a Coronary Chronic Total Occlusion. A Multicenter Registry. Rev Esp Cardiol (Engl Ed). 2018; 71(6): 432-9. |
| [10] | Azzalini L, Ojeda S, Karatasakis A, Maeremans J, Tanabe M, La Manna A, et al. Long-Term Outcomes of Percutaneous Coronary Intervention for Chronic Total Occlusion in Patients Who Have Undergone Coronary Artery Bypass Grafting vs Those Who Have Not. Can J Cardiol. 2018; 34(3): 310-8. |
| [11] | Sianos G, Morel MA, Kappetein AP, Morice MC, Colombo A, Dawkins K, et al. The SYNTAX Score: an angiographic tool grading the complexity of coronary artery disease. EuroIntervention. 2005; 1(2): 219-27. |
| [12] | Fang HY, Lu SY, Lee WC, Lin YS, Cheng CI, Chen CJ, et al. The predictors of successful percutaneous coronary intervention in ostial left anterior descending artery chronic total occlusion. Catheter Cardiovasc Interv. 2014; 84(4): E30-7. |
| [13] | Galassi AR, Boukhris M, Azzarelli S, Castaing M, Marza F, and Tomasello SD. Percutaneous Coronary Revascularization for Chronic Total Occlusions: A Novel Predictive Score of Technical Failure Using Advanced Technologies. JACC Cardiovasc Interv. 2016; 9(9): 911-22. |
| [14] | Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. EuroIntervention. 2019; 14(14): 1435-534. |
| [15] | Kern MJ, Moore JA, Aguirre FV, Bach RG, Caracciolo EA, Wolford T, et al. Determination of angiographic (TIMI grade) blood flow by intracoronary Doppler flow velocity during acute myocardial infarction. Circulation. 1996; 94(7): 1545-52. |
| [16] | Galassi AR, Tomasello SD, Reifart N, Werner GS, Sianos G, Bonnier H, et al. In-hospital outcomes of percutaneous coronary intervention in patients with chronic total occlusion: insights from the ERCTO (European Registry of Chronic Total Occlusion) registry. EuroIntervention. 2011; 7(4): 472-9. |
| [17] | Galassi AR, Sianos G, Werner GS, Escaned J, Tomasello SD, Boukhris M, et al. Retrograde Recanalization of Chronic Total Occlusions in Europe: Procedural, In-Hospital, and Long-Term Outcomes From the Multicenter ERCTO Registry. J Am Coll Cardiol. 2015; 65(22): 2388-400. |
| [18] | Christopoulos G, Wyman RM, Alaswad K, Karmpaliotis D, Lombardi W, Grantham JA, et al. Clinical Utility of the Japan-Chronic Total Occlusion Score in Coronary Chronic Total Occlusion Interventions: Results from a Multicenter Registry. Circ Cardiovasc Interv. 2015; 8(7): e002171. |
| [19] | Morino Y, Abe M, Morimoto T, Kimura T, Hayashi Y, Muramatsu T, et al. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes: the J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc Interv. 2011; 4(2): 213-21. |
| [20] | Christopoulos G, Kandzari DE, Yeh RW, Jaffer FA, Karmpaliotis D, Wyman MR, et al. Development and Validation of a Novel Scoring System for Predicting Technical Success of Chronic Total Occlusion Percutaneous Coronary Interventions: The PROGRESS CTO (Prospective Global Registry for the Study of Chronic Total Occlusion Intervention) Score. JACC Cardiovasc Interv. 2016; 9(1): 1-9. |
| [21] | Szijgyarto Z, Rampat R, Werner GS, Ho C, Reifart N, Lefevre T, et al. Derivation and Validation of a Chronic Total Coronary Occlusion Intervention Procedural Success Score From the 20,000-Patient EuroCTO Registry: The EuroCTO (CASTLE) Score. JACC Cardiovasc Interv. 2019; 12(4): 335-42. |
| [22] | Tajti P, Burke MN, Karmpaliotis D, Alaswad K, Jaffer FA, Yeh RW, et al. Prevalence and Outcomes of Percutaneous Coronary Interventions for Ostial Chronic Total Occlusions: Insights From a Multicenter Chronic Total Occlusion Registry. Can J Cardiol. 2018; 34(10): 1264-74. |
| [23] | Garcia S, Alraies MC, Karatasakis A, Yannopoulos D, Karmpaliotis D, Alaswad K, et al. Coronary artery spatial distribution of chronic total occlusions: Insights from a large US registry. Catheter Cardiovasc Interv. 2017; 90(1): 23-30. |
| [24] | Megaly M, Ali A, Saad M, Omer M, Xenogiannis I, Werner GS, et al. Outcomes with retrograde versus antegrade chronic total occlusion revascularization. Catheter Cardiovasc Interv. 2020; 96(5): 1037-43. |
| [25] | Karacsonyi J, Stanberry L, Alaswad K, Krestyaninov O, Choi JW, Rangan BV, et al. Predicting Technical Success of Chronic Total Occlusion Percutaneous Coronary Intervention: Comparison of 3 Scores. Circ Cardiovasc Interv. 2021; 14(1): e009860. |
| [26] | Allana SS, Kostantinis S, Simsek B, Karacsonyi J, Rempakos A, Alaswad K, et al. Lesion complexity and procedural outcomes associated with ostial chronic total occlusions: Insights from the PROGRESS-CTO Registry. J Invasive Cardiol. 2023; 35(12). |
| [27] | Ellis SG, Burke MN, Murad MB, Graham JJ, Badawi R, Toma C, et al. Predictors of Successful Hybrid-Approach Chronic Total Coronary Artery Occlusion Stenting: An Improved Model With Novel Correlates. JACC Cardiovasc Interv. 2017; 10(11): 1089-98. |
| [28] | Nombela-Franco L, Urena M, Jerez-Valero M, Nguyen CM, Ribeiro HB, Bataille Y, et al. Validation of the J-chronic total occlusion score for chronic total occlusion percutaneous coronary intervention in an independent contemporary cohort. Circ Cardiovasc Interv. 2013; 6(6): 635-43. |
APA Style
Salloum, B., Koc, Y., Schnupp, S., Mady, H., Mahnkopf, C. (2025). Ostial Lesions Are Associated with More Complexity and Lower Success Rate in Chronic Total Occlusion Percutaneous Interventions. International Journal of Cardiovascular and Thoracic Surgery, 11(5), 63-73. https://doi.org/10.11648/j.ijcts.20251105.11
ACS Style
Salloum, B.; Koc, Y.; Schnupp, S.; Mady, H.; Mahnkopf, C. Ostial Lesions Are Associated with More Complexity and Lower Success Rate in Chronic Total Occlusion Percutaneous Interventions. Int. J. Cardiovasc. Thorac. Surg. 2025, 11(5), 63-73. doi: 10.11648/j.ijcts.20251105.11
AMA Style
Salloum B, Koc Y, Schnupp S, Mady H, Mahnkopf C. Ostial Lesions Are Associated with More Complexity and Lower Success Rate in Chronic Total Occlusion Percutaneous Interventions. Int J Cardiovasc Thorac Surg. 2025;11(5):63-73. doi: 10.11648/j.ijcts.20251105.11
@article{10.11648/j.ijcts.20251105.11,
author = {Basem Salloum and Yeliz Koc and Steffen Schnupp and Hesham Mady and Christian Mahnkopf},
title = {Ostial Lesions Are Associated with More Complexity and Lower Success Rate in Chronic Total Occlusion Percutaneous Interventions
},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {11},
number = {5},
pages = {63-73},
doi = {10.11648/j.ijcts.20251105.11},
url = {https://doi.org/10.11648/j.ijcts.20251105.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20251105.11},
abstract = {Aims: We aimed to evaluate the influence of ostial lesions on the predicted probability of success in patients undergoing percutaneous coronary interventions (PCIs) for chronic total occlusions (CTOs). Methods: 245 consecutive patients who underwent CTO PCIs at Coburg Hospital, Coburg, Germany between 2017 and 2023 were included. Patients with and without ostial lesions were compared. Logistic regression models were used to estimate the potential of ostial lesion as additional predictor for success beside J-Score. Results: 245 patients were included. Of those, 48 Patients (19.6%) had ostial lesions. The ostial lesion group exhibited significantly higher pro-B-type natriuretic peptide levels (1644 pg./ml vs. 963 pg./ml, p=0.034) than the non-ostial lesion group. The final success rate was lower in the ostial lesion group than in the non-ostial lesion group (64.6% vs. 81.7%, p=0.018). The ostial lesion group had higher J-scores than the non-ostial lesion group, indicating more complex lesions (median: 2.5 vs. 2.0, p=0.005). Antegrade access was more applied in non-ostial lesion group (89.8% vs. 68.8% p=0.001), whereas retrograde access was more applied in ostial lesion group. (33.3% vs. 7.6%, p=Conclusion: The presence of ostial CTO is associated with higher lesion complexity and lower technical and procedural success rates. Presence of ostial CTO might be included as an additional factor in the currently used CTO scores to predict the difficulty and success rate of CTO procedure.
},
year = {2025}
}
TY - JOUR T1 - Ostial Lesions Are Associated with More Complexity and Lower Success Rate in Chronic Total Occlusion Percutaneous Interventions AU - Basem Salloum AU - Yeliz Koc AU - Steffen Schnupp AU - Hesham Mady AU - Christian Mahnkopf Y1 - 2025/10/10 PY - 2025 N1 - https://doi.org/10.11648/j.ijcts.20251105.11 DO - 10.11648/j.ijcts.20251105.11 T2 - International Journal of Cardiovascular and Thoracic Surgery JF - International Journal of Cardiovascular and Thoracic Surgery JO - International Journal of Cardiovascular and Thoracic Surgery SP - 63 EP - 73 PB - Science Publishing Group SN - 2575-4882 UR - https://doi.org/10.11648/j.ijcts.20251105.11 AB - Aims: We aimed to evaluate the influence of ostial lesions on the predicted probability of success in patients undergoing percutaneous coronary interventions (PCIs) for chronic total occlusions (CTOs). Methods: 245 consecutive patients who underwent CTO PCIs at Coburg Hospital, Coburg, Germany between 2017 and 2023 were included. Patients with and without ostial lesions were compared. Logistic regression models were used to estimate the potential of ostial lesion as additional predictor for success beside J-Score. Results: 245 patients were included. Of those, 48 Patients (19.6%) had ostial lesions. The ostial lesion group exhibited significantly higher pro-B-type natriuretic peptide levels (1644 pg./ml vs. 963 pg./ml, p=0.034) than the non-ostial lesion group. The final success rate was lower in the ostial lesion group than in the non-ostial lesion group (64.6% vs. 81.7%, p=0.018). The ostial lesion group had higher J-scores than the non-ostial lesion group, indicating more complex lesions (median: 2.5 vs. 2.0, p=0.005). Antegrade access was more applied in non-ostial lesion group (89.8% vs. 68.8% p=0.001), whereas retrograde access was more applied in ostial lesion group. (33.3% vs. 7.6%, p=Conclusion: The presence of ostial CTO is associated with higher lesion complexity and lower technical and procedural success rates. Presence of ostial CTO might be included as an additional factor in the currently used CTO scores to predict the difficulty and success rate of CTO procedure. VL - 11 IS - 5 ER -
Department of Cardiology, Klinikum Coburg, Coburg, Germany
Department of Gastroenterology, Klinikum Lichtenfels, Lichtenfels, Germany
Department of Cardiology, Klinikum Coburg, Coburg, Germany
Department of Cardiology, Klinikum Coburg, Coburg, Germany
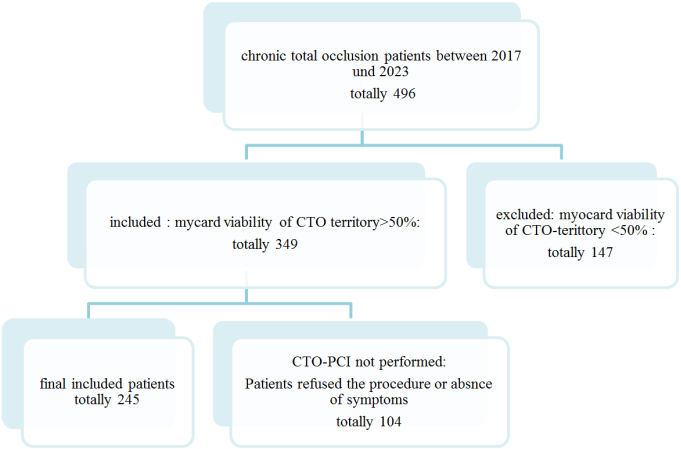
Figure 1. Consort Flow Chart.
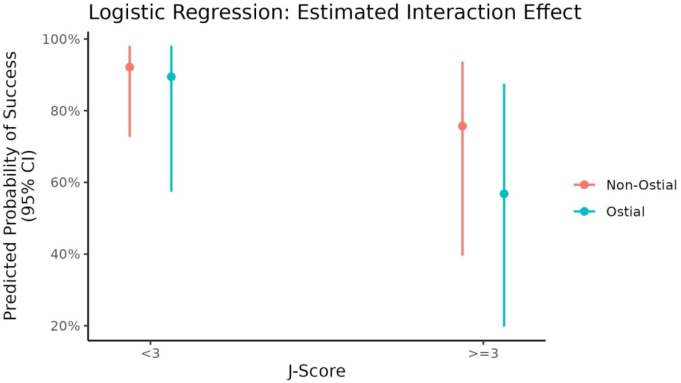
Figure 2. Illustrates a logistic regression model with a interaction term between J-score and the presence of an ostial lesion.
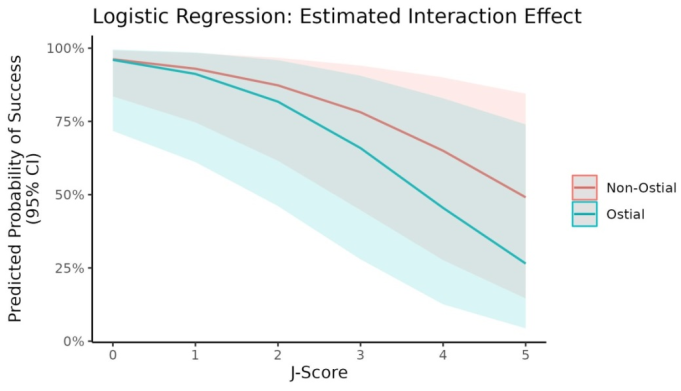
Figure 3. Illustrates the predicted probability of success with 95% CIs for each J-score category and each level of the ostial lesion variable.
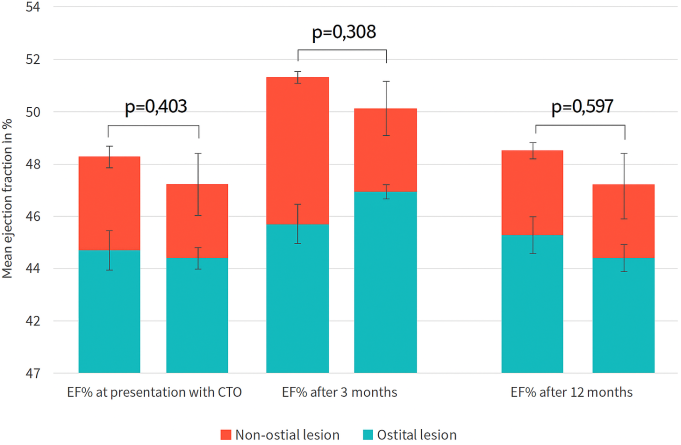
Figure 4. Illustrates the difference in the improvement of LVEF between ostial lesions and non-ostial lesions after CTO-PCI.
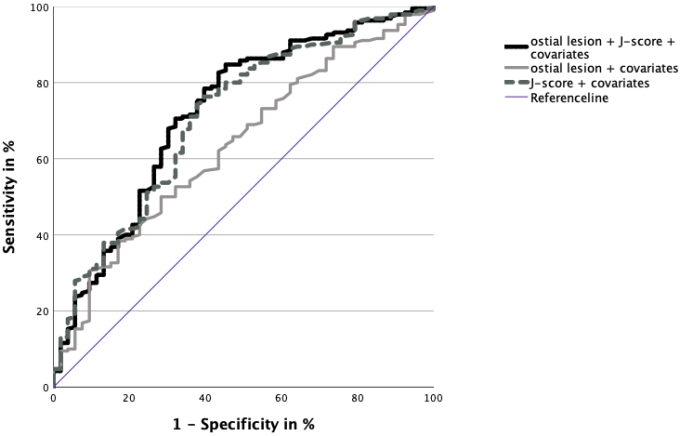
Figure 5. ROC-Analyses incorporating ostial lesion additionally to the established J-Score.
Information

