Anomalous coronary artery from the opposite sinus (ACAOS) is a rare congenital abnormality that may be encountered during routine coronary angiography. Clinical manifestations vary depending on the subtype and anatomical course of the anomaly; however, certain potentially malignant trajectories may result in myocardial ischemia, infarction, or sudden cardiac death, particularly in young individuals and athletes. Multiple imaging modalities including coronary angiography, CT angiography, and cardiac MRI are useful in the evaluation of coronary artery anomalies. Accurate delineation of the origin and course of the anomalous vessel is essential for risk stratification and therapeutic planning. Performing percutaneous coronary intervention (PCI) in patients with ACAOS can be technically challenging and often requires modifications in guide catheter selection and procedural technique. In this review, we present a series of patients with anomalous coronary arteries originating from the opposite sinus of Valsalva (ACAOS). We discuss the anatomical variations and courses of these anomalous vessels as defined by angiographic and advanced imaging findings. Particular emphasis is placed on guide catheter selection, technical challenges encountered during selective cannulation, and the strategies employed to achieve successful engagement and intervention.
| Published in | International Journal of Cardiovascular and Thoracic Surgery (Volume 12, Issue 2) |
| DOI | 10.11648/j.ijcts.20261202.14 |
| Page(s) | 40-54 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Anomalous Coronary Artery, ACAOS, Coronary CT Angiography, Percutaneous Coronary Intervention
LMCA |
A. Arising from right sinus of Valsalva |
(1) Interarterial |
(2) Retro aortic |
(3) Septal |
(4) Anterior/pre-pulmonic |
(5) Posterior atrioventricular groove or retrocardiac |
(6) Posteroanterior interventricular groove (wraparound) |
B. Absent left main trunk |
C. Aberrant location in the left sinus of Valsalva (anterior or posterior) |
D. Arising from the pulmonary artery |
LAD |
Arising from right sinus of Valsalva |
Interarterial |
Septal |
Anterior/prepulmonic |
Posteroanterior interventricular groove (wraparound) |
B. Separate ostium of left anterior descending from left sinus of Valsalva |
C. Arising from the pulmonary artery |
LCX |
A. Arising from right sinus of Valsalva |
(1) Posterior atrioventricular groove |
(2) Retro aortic |
B. Separate ostium of left circumflex from left sinus of Valsalva |
C. Rudimentary or absent left circumflex (super-dominant right coronary) |
D. Arising from the pulmonary artery |
RCA |
A. Arising from the left sinus of Valsalva |
(1) Posterior atrioventricular groove or retrocardiac |
(2) Retro aortic |
(3) Interarterial |
(4) Septal |
(5) Anterior/prepulmonic |
(6) Posteroanterior interventricular groove (wraparound) |
B. Posterior location in the right sinus of Valsalva |
C. Absent right coronary artery (super-dominant left circumflex) |
D. Arising from the pulmonary artery |
Relatively benign anomalies | Potentially serious anomalies |
|---|---|
1) Separate origin of left anterior descending and left circumflex from the left sinus of Valsalva | 1) Ectopic coronary origin from the pulmonary artery |
2) Ectopic origin of the circumflex from the right sinus of Valsalva | 2) Ectopic coronary origin from the opposite aortic sinus |
3) Ectopic coronary origin from the posterior sinus of Valsalva | 3) Single coronary artery |
4) Ectopic coronary origin from the ascending aorta | 4) Large coronary artery fistulae |
5) Absent circumflex | 5) Interarterial course |
6) Intercoronary communication | |
7) Small size coronary artery fistulae |
Artery origin | Preferred guide catheters |
|---|---|
RCA | |
A) RCA ostium adjacent to left main coronary artery ostium | Leya catheter, left coronary, Amplatz 45, 90 R-ACAOS Launcher, Ikari |
B) RCA ostium inferior to left main coronary artery ostium | AL, AR |
C) RCA ostium toward the commissure of the right and left cusps | AL, AR |
D) Ostium above the sinotubular plane | JR, MP, Hockey stick |
E) Ostium from right cusp superior and toward the left cusp | AL, AR, Sherpa NX balanced, 3DRC |
F) Usual origin | JR |
G) Shephard crook | AL |
LMCA/LAD | |
A) Posterior origin of the left main from the left cusp or non-coronary cusp | EBU, CLS |
B) Anomalous left main coronary artery from the right cusp | JR4, Hockey stick |
LCX | |
LCX arising from right sinus | AL, AR, JR 4, Hockey stick |
RAC | Retroaortic Anomalous Coronary |
RCA | Right Coronary Artery |
LCX | Left Circumflex (Artery) |
LAO | Left Anterior Oblique |
RAO | Right Anterior Oblique |
CCTA | Coronary Computed Tomography Angiography |
RVOT | Right Ventricular Outflow Tract |
AV | Atrioventricular |
TIMI | Thrombolysis in Myocardial Infarction |
LCA/LMCA | Left Coronary Artery/Left Main Coronary Artery |
LV | Left Ventricle |
R-ACAOS | Right Anomalous Coronary Artery from the Opposite Sinus |
L-ACAOS | Left Anomalous Coronary Artery from the Opposite Sinus |
MRA | Magnetic Resonance Angiography |
ALCAPA | Anomalous Left Coronary Artery from the Pulmonary Artery |
AAOCA | Anomalous Aortic Origin of a Coronary Artery |
ICA | Invasive Coronary Angiography |
FFRCT | Fractional Flow Reserve Derived from Computed Tomography |
IVUS | Intravascular Ultrasound |
FFR | Fractional Flow Reserve |
QFR | Quantitative Flow Ratio |
FSI | Fluid-Structure Interaction |
SCD | Sudden Cardiac Death |
CABG | Coronary Artery Bypass Grafting |
ESC | European Society of Cardiology |
AHA | American Heart Association |
ACC | American College of Cardiology |
AATS | American Association for Thoracic Surgery |
| [1] | Beique F, De Tran QH, Ma F, Rudski L, Daves S, Angelini P. Anomalous right coronary artery originating from the left sinus of Valsalva. J Cardiothorac Vasc Anesth 2004; 18(6): 788-98. |
| [2] | Click RL, Holmes DR, Vlietstra RE, Kosinski AS, Kronmal RA. Anomalous coronary arteries: location, degree of atherosclerosis and effect on survival—a report from the Coronary Artery Surgery Study. Journal of the American College of Cardiology. 1989 Mar 1; 13(3): 531-7. |
| [3] | Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Catheterization and cardiovascular diagnosis. 1990 Sep; 21(1): 28-40. |
| [4] | Alexander RW, Griffith GC. Anomalies of the coronary arteries and their clinical significance. Circulation. 1956 Nov; 14(5): 800–805. |
| [5] | Angelini P, Villason S, Chan AV, Diez JG. Coronary artery anomalies. Baltimore: Lippincott Williams & Wilkins; 1999. |
| [6] | Angelini P. Coronary artery anomalies—current clinical issues: definitions, classification, incidence, clinical relevance, and treatment guidelines. Texas Heart Institute Journal. 2002; 29(4): 271. |
| [7] | Angelini P, Villason S, Chan Jr AV, Diez JG. Normal and anomalous coronary arteries in humans. Part 1: historical background. |
| [8] | Angelini P. Congenital heart disease for the adult cardiologist. Circ. 2007; 115: 1296-305. |
| [9] | Angelini P, Velasco JA, Flamm S. Coronary anomalies: incidence, pathophysiology, and clinical relevance. Circulation. 2002 May 21; 105(20): 2449-54. |
| [10] | Patel S. Normal and anomalous anatomy of the coronary arteries. InSeminars in roentgenology 2008 Apr (Vol. 43, No. 2, pp. 100-112). |
| [11] | PAGE JR HL, ENGEL HJ, CAMPBELL WB, THOMAS JR CS. Anomalous origin of the left circumflex coronary artery: recognition, angiographic demonstration and clinical significance. Circulation. 1974 Oct; 50(4): 768-73. |
| [12] | Ishikawa T, Brandt PW. Anomalous origin of the left main coronary artery from the right anterior aortic sinus: angiographic definition of anomalous course. The American journal of cardiology. 1985 Mar 1; 55(6): 770-6. |
| [13] | Serota H, Barth III CW, Seuc CA, Vandormael M, Aguirre F, Kern MJ. Rapid identification of the course of anomalous coronary arteries in adults: the “dot and eye” method. The American journal of cardiology. 1990 Apr 1; 65(13): 891-8. |
| [14] | Sarkar K, Sharma SK, Kini AS. Catheter selection for coronary angiography and intervention in anomalous right coronary arteries. Journal of interventional cardiology. 2009 Jun; 22(3): 234-9. |
| [15] | Frommelt PC, Frommelt MA, Tweddell JS, Jaquiss RD. Prospective echocardiographic diagnosis and surgical repair of anomalous origin of a coronary artery from the opposite sinus with an interarterial course. Journal of the American College of Cardiology. 2003 Jul 2; 42(1): 148-54. |
| [16] | Ghadri JR, Kazakauskaite E, Braunschweig S, et al. Congenital coronary anomalies detected by coronary computed tomography compared to invasive coronary angiography. BMC Cardiovasc Disord 2014; 14: 81. |
| [17] | Bigler MR, Kadner A, Räber L, Ashraf A, Windecker S, Siepe M, Padalino MA, Gräni C. Therapeutic management of anomalous coronary arteries originating from the opposite sinus of Valsalva: current evidence, proposed approach, and the unknowing. Journal of the American Heart Association. 2022 Oct 18; 11(20): e027098. |
| [18] | Gentile F, Castiglione V, De Caterina R. Coronary artery anomalies. Circulation. 2021 Sep 21; 144(12): 983-96. |
| [19] | Molossi S, Doan T, Sachdeva S. Anomalous coronary arteries: a state-of-the-art approach. Cardiac Electrophysiology Clinics. 2024 Mar 1; 16(1): 51-69. |
| [20] | Hutchins GM, Miner MM, Boitnott JK. Vessel caliber and branch-angle of human coronary artery branch-points. Circulation research. 1976 Jun; 38(6): 572-6. |
| [21] | Liu LB. Richardson T, Taylor CB. Atherosclerotic occlusions in anomalous left circumflex coronary-arteries: a report of 2 unusual cases and a review of pertinent literature. Par Arter lY75; 2: 55-9. |
| [22] | Basso C, Corrado D, Thiene G. Congenital coronary anomalies as an important cause of sudden death in the young. Cardiol Rev. 2001; 9: 312-7. |
| [23] | Angelini P, Velasco JA, Ott D, Khoshnevis GR. Anomalous coronary artery arising from the opposite sinus: descriptive features and pathophysiologic mechanisms, as documented by intravascular ultrasonography. J Invasive Cardiol. 2003; 15: 507-14. |
| [24] | Kim D, Jeong MH, Lee KH, Lee MG, Park KH, Sim DS, Yoon NS, Yoon HJ, Kim KH, Hong YJ, Kim JH. Successful primary percutaneous coronary intervention in a patient with acute myocardial infarction and single coronary artery ostium. Korean Circulation Journal. 2012 Apr 26; 42(4): 284. |
| [25] | Young PM, Gerber TC, Williamson EE, et al. Cardiac imaging: part 2, normal, variant, and anomalous configurations of the coronary vasculature. AJR Am J Roentgenol 2011; 197: 816–26. |
| [26] | Arnáiz García ME, González-Santos JM, Pérez-Losada ME, López-Rodríguez J, Arnáiz J. Unexpected entrapment during surgery of anomalous circumflex coronary artery arising from right coronary artery. Turk Kardiyol Dern Ars. 2019 Apr 1; 47(3): 239-42. |
| [27] | Tabachnick D, Obokhae B, Harrington K, Brown DL. Assessing the risk of an anomalous circumflex artery using balloon aortic valvuloplasty prior to transcatheter aortic valve replacement. Catheterization and Cardiovascular Interventions. 2020 Aug; 96(2): 497-9. |
| [28] | Formato GM, Agnifili ML, Arzuffi L, Rosato A, Ceserani V, Zuniga Olaya KG, Secchi F, Deamici M, Conti M, Auricchio F, Bedogni F. Morphological changes of anomalous coronary arteries from the aorta during the cardiac cycle assessed by IVUS in resting conditions. Circulation: Cardiovascular Interventions. 2023 Jul; 16(7): e012636. |
| [29] | Fretay XHD, Boudvillain O, Koutsoukis A, Degrell P, Dupouy P, Aubry P. Catheterization Techniques for Anomalous Aortic Origin of Coronary Arteries. Catheter Cardiovasc Interv. 2025 Mar; 105(4): 825-837. |
| [30] | Ben-Dor I, Weissman G, Rogers T, Slack M, Pichard A, Ben-Dor N, Hashim H, Bernardo N, Satler LF, Waksman R. Catheter selection and angiographic views for anomalous coronary arteries: a practical guide. Cardiovascular Interventions. 2021 May 10; 14(9): 995-1008. |
APA Style
Saha, S., Jha, A., Tiwari, B. C., Bharali, A., Yadaw, M. (2026). Anomalous Coronary Arteries from the Opposite Sinus of Valsalva: A Case Series and Comprehensive Review. International Journal of Cardiovascular and Thoracic Surgery, 12(2), 40-54. https://doi.org/10.11648/j.ijcts.20261202.14
ACS Style
Saha, S.; Jha, A.; Tiwari, B. C.; Bharali, A.; Yadaw, M. Anomalous Coronary Arteries from the Opposite Sinus of Valsalva: A Case Series and Comprehensive Review. Int. J. Cardiovasc. Thorac. Surg. 2026, 12(2), 40-54. doi: 10.11648/j.ijcts.20261202.14
@article{10.11648/j.ijcts.20261202.14,
author = {Sandeepan Saha and Ashish Jha and Bhuwan Chandra Tiwari and Abhijit Bharali and Mithilesh Yadaw},
title = {Anomalous Coronary Arteries from the Opposite Sinus of Valsalva: A Case Series and Comprehensive Review},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {12},
number = {2},
pages = {40-54},
doi = {10.11648/j.ijcts.20261202.14},
url = {https://doi.org/10.11648/j.ijcts.20261202.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20261202.14},
abstract = {Anomalous coronary artery from the opposite sinus (ACAOS) is a rare congenital abnormality that may be encountered during routine coronary angiography. Clinical manifestations vary depending on the subtype and anatomical course of the anomaly; however, certain potentially malignant trajectories may result in myocardial ischemia, infarction, or sudden cardiac death, particularly in young individuals and athletes. Multiple imaging modalities including coronary angiography, CT angiography, and cardiac MRI are useful in the evaluation of coronary artery anomalies. Accurate delineation of the origin and course of the anomalous vessel is essential for risk stratification and therapeutic planning. Performing percutaneous coronary intervention (PCI) in patients with ACAOS can be technically challenging and often requires modifications in guide catheter selection and procedural technique. In this review, we present a series of patients with anomalous coronary arteries originating from the opposite sinus of Valsalva (ACAOS). We discuss the anatomical variations and courses of these anomalous vessels as defined by angiographic and advanced imaging findings. Particular emphasis is placed on guide catheter selection, technical challenges encountered during selective cannulation, and the strategies employed to achieve successful engagement and intervention.},
year = {2026}
}
TY - JOUR T1 - Anomalous Coronary Arteries from the Opposite Sinus of Valsalva: A Case Series and Comprehensive Review AU - Sandeepan Saha AU - Ashish Jha AU - Bhuwan Chandra Tiwari AU - Abhijit Bharali AU - Mithilesh Yadaw Y1 - 2026/03/19 PY - 2026 N1 - https://doi.org/10.11648/j.ijcts.20261202.14 DO - 10.11648/j.ijcts.20261202.14 T2 - International Journal of Cardiovascular and Thoracic Surgery JF - International Journal of Cardiovascular and Thoracic Surgery JO - International Journal of Cardiovascular and Thoracic Surgery SP - 40 EP - 54 PB - Science Publishing Group SN - 2575-4882 UR - https://doi.org/10.11648/j.ijcts.20261202.14 AB - Anomalous coronary artery from the opposite sinus (ACAOS) is a rare congenital abnormality that may be encountered during routine coronary angiography. Clinical manifestations vary depending on the subtype and anatomical course of the anomaly; however, certain potentially malignant trajectories may result in myocardial ischemia, infarction, or sudden cardiac death, particularly in young individuals and athletes. Multiple imaging modalities including coronary angiography, CT angiography, and cardiac MRI are useful in the evaluation of coronary artery anomalies. Accurate delineation of the origin and course of the anomalous vessel is essential for risk stratification and therapeutic planning. Performing percutaneous coronary intervention (PCI) in patients with ACAOS can be technically challenging and often requires modifications in guide catheter selection and procedural technique. In this review, we present a series of patients with anomalous coronary arteries originating from the opposite sinus of Valsalva (ACAOS). We discuss the anatomical variations and courses of these anomalous vessels as defined by angiographic and advanced imaging findings. Particular emphasis is placed on guide catheter selection, technical challenges encountered during selective cannulation, and the strategies employed to achieve successful engagement and intervention. VL - 12 IS - 2 ER -
Department of Cardiology, Dr. Ram Manohar Lohia Institute of Medical Sciences, Lucknow, India
Department of Cardiology, Dr. Ram Manohar Lohia Institute of Medical Sciences, Lucknow, India
Department of Cardiology, Dr. Ram Manohar Lohia Institute of Medical Sciences, Lucknow, India
Department of Cardiology, Dr. Ram Manohar Lohia Institute of Medical Sciences, Lucknow, India
Department of Cardiology, Dr. Ram Manohar Lohia Institute of Medical Sciences, Lucknow, India
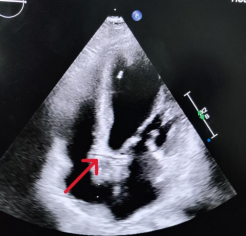
Figure 1. Transthoracic echocardiogram demonstrating the retroaortic anomalous coronary (RAC) sign in the apical four-chamber view (red arrow).
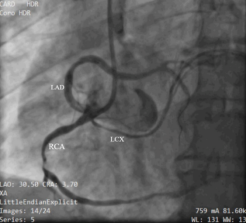
Figure 2. Coronary angiography. LAO view showing mid-discrete critical disease in RCA while LAD (originating from right aortic sinus) had a proximal 70% disease. LCX was also originating from right sinus. LAD, left anterior descending; LCX, left circumflex; RCA, right coronary artery, LAO, left anterior oblique.
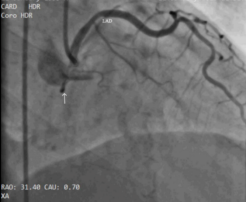
Figure 3. Coronary angiography. Injection in RAO 30 view showing a cranial anterior loop of LAD (anterior course) and LCX appearing as a dot (arrow) behind the aorta (retroaortic course).
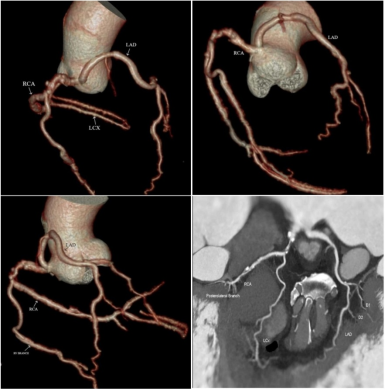
Figure 4. Reconstructed CT coronary angiography showing all three coronary arteries originating separately from the right aortic sinus of Valsalva. LAD, left anterior descending; LCX, left circumflex; RCA, right coronary artery.
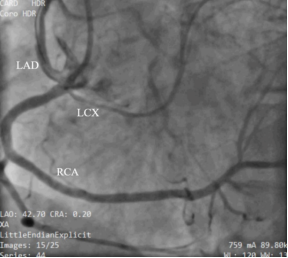
Figure 5. Percutaneous coronary intervention to left anterior descending artery and right coronary artery was done demonstrating good angiographic result with Thrombolysis in Myocardial Infarction 3 flow.
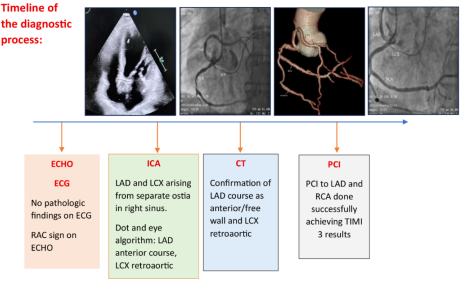
Figure 6. A timeline of the diagnostic process.

Figure 7. Coronary angiography. RCA originating from left sinus above the level of LCA.
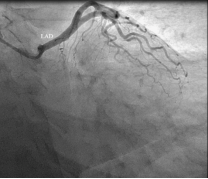
Figure 8. Coronary angiography. LAD originating from left sinus, LCX is not visualised.

Figure 9. Coronary angiography. LCX originating from right sinus sharing same ostia with RCA.
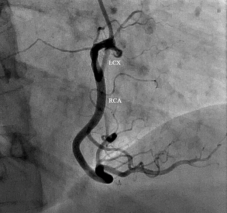
Figure 10. Coronary angiography. In the RAO 30 view, LCX coursing caudal and posterior (retroaortic course).
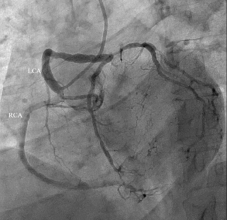
Figure 11. Coronary angiography. RCA and LCA originated from a common ostium in the right aortic sinus.
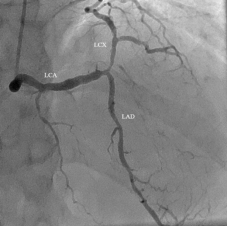
Figure 12. In the RAO 30 view, the LCA followed a caudal and anterior course, indicating a benign anatomical pattern. As per the dot and eye algorithm, the superior border of the eye is formed by LCX and inferior border by LCA, suggestive of a septal course. The left main coronary artery then emerged on the left side of the aortic root and bifurcated into the LAD and LCX, both demonstrating a normal course.

Figure 13. Coronary angiography. LAD originating from left sinus, LCX is not visualised.

Figure 14. LCX arising from non-coronary sinus and coursed retro aortic.
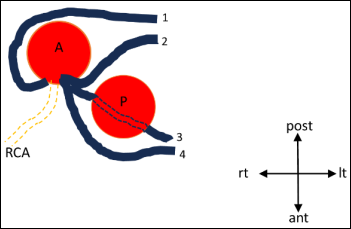
Figure 15. Diagrammatic representation of the four possible pathways for the anomalous left main coronary artery (LMCA) arising from the right coronary cusp or the right coronary artery (RCA): 1, retroaortic course; 2, interarterial course; 3, septal course; 4, anterior free wall course. A, aortic valve; P, pulmonary valve; ant = anterior; It = left; post = posterior; rt = right.
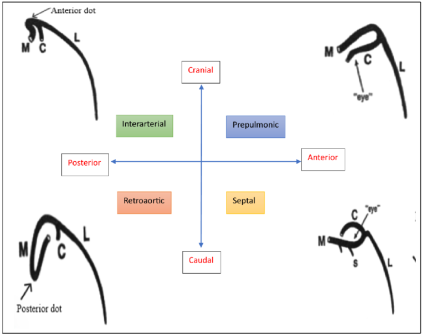
Figure 16. A simplified technique to identify the anomalous LMCA courses at a quick glance. A cranial, anterior loop indicates a prepulmonic course, forming an “eye” with the LMCA as the superior border and the LCx as the inferior border. A caudal, anterior loop suggests a septal course, forming an “eye” with the LMCA as the inferior border and the LCx as the superior border. A cranial, posterior loop corresponds to an interarterial course, visualized as a dot anterior to the aorta. A caudal, posterior loop indicates a retroaortic course, visualized as a dot posterior to the aorta. Abbreviations: M, left main coronary artery; L, left anterior descending artery; C, left circumflex artery.
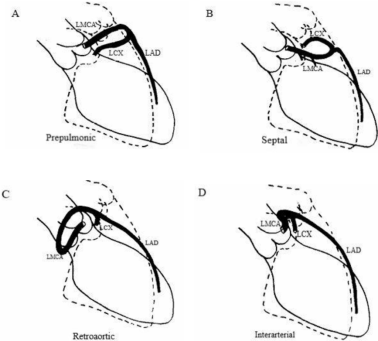
Figure 17. Diagrammatic angiographic illustration of the four possible left main coronary artery courses arising from the right coronary cusp. Illustration of the coronary angiographic images in right anterior oblique projection (redrawn from Ishikawa) showing the four possible courses of an aberrant left main coronary artery (LMCA) arising from the right coronary cusp or the right coronary artery. (LAD, left anterior descending; LCx, left circumflex).
Information

