Minor bleeding after internal urethrotomy is quite common and often subsides spontaneously. Mild to moderate persistent bleeding responds well with conservative management. Severe, life-threatening bleeding that necessitates invasive intervention is seldom seen these days. Selective or super-selective angioembolization is highly effective in these cases and has minimal associated morbidity. Here, we present a case of refractory urethral bleeding after optical internal urethrotomy (OIU) successfully managed by super-selective angioembolization. A 59-year-old man was referred to us with massive pericather bleeding after a cold knife internal urethrotomy done at a peripheral center 5 days ago. There was recurrent clot retention and a clinically significant drop in hemoglobin while on conservative management. Two units of LDPRBC were transfused. There was no history of chronic liver or kidney disease or any coagulation disorders. After Initial conservative measures failed, the patient underwent a computed tomography angiogram of the pelvis, which revealed a pseudoaneurysm arising from the bulbourethral artery. Different invasive management approaches like endoscopic fulguration, angioembolization, and open surgical repair have been explained and discussed with the patient and their relatives. Following shared decision-making and informed consent, angioembolization of the bulbourethral artery was performed. The bleeding stopped after the procedure, and the patient was discharged after 24 hours of observation. The present report highlights the use of super-selective embolization in severe urethral bleeding if initial conservative measures failed.
| Published in | International Journal of Clinical Urology (Volume 9, Issue 1) |
| DOI | 10.11648/j.ijcu.20250901.21 |
| Page(s) | 68-72 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Optical Internal Urethrotomy (OIU), Bleeding Per Urethra, Angioembolization, Case Report
OIU | Optical Internal Urethrotomy |
PVA | Polyvinyl Alcohol |
USG | Ultrasonography |
DSA | Digital Subtraction Angiography |
LDPRBC | leucodeplated Packed RBC |
CT | Computed Tomogram |
| [1] | Attri V, Parmar K, Dewana S, Sharma G, Chandna A. Massive bleed following optical internal urethrotomy: an unforeseen doom discussing the unique management technique. Journal of endourology case reports. 2018 Nov 1; 4(1): 179-82. |
| [2] | Dhabalia J, Nelivigi G, Punia M, Kumar V. RefracTory post visual internal urethrotomy bleeding managed by angioembolization. Indian Journal of Radiology and Imaging. 2010 Jan 1; 20(1): 37-37. |
| [3] | Chiou RK, Donovan JM, Anderson JC, Matamoros A, Wobig RK, Taylor RJ. Color Doppler ultrasound assessment of urethral artery location: potential implication for the technique of visual internal urethrotomy. The Journal of Urology. 1998 Mar; 159(3): 796-9. |
| [4] | Kishore TA, Bhat S, John RP. Color Doppler ultrasonographic location of the bulbourethral artery and its impact on surgical outcome. BJU Int 2003; 96: 624-8. |
| [5] | Mabjeesh NJ, Shemesh D, Abramowitz HB. Posttraumatic high flow priapism: Successful management using duplex guided compression. J Urol 1999; 161: 215–216. |
| [6] | Tritschler S, Beck V. Management of urethral stricture. Der Urologe. Ausg. A. 2021 Oct 12; 60(11): 1473-9. |
| [7] | Wessells H, Morey A, Souter L, Rahimi L, Vanni A. Urethral stricture disease guideline amendment (2023). The Journal of Urology. 2023 Jul; 210(1): 64-71. |
| [8] | Liu JS, Walker K, Stein D, Prabhu S, Hofer MD, Han J, Yang XJ, Gonzalez CM. Lichen sclerosus and isolated bulbar urethral stricture disease. The Journal of urology. 2014 Sep; 192(3): 775-9. |
| [9] | Sa Y, Wang L, Lv R, Wang J, Chen G, Jin C, Feng C. Transperineal anastomotic urethroplasty for the treatment of pelvic fracture urethral distraction defects: a progressive surgical strategy. World Journal of Urology. 2021 Dec; 39: 4435-41. |
| [10] | Webster GD, Peterson AC. Simple perineal and elaborated perineal posterior urethroplasty. Arab journal of urology. 2015 Mar 1; 13(1): 17-23. |
| [11] | Devries CR, Anderson RU. Endoscopic urethroplasty: an improved technique. The Journal of urology. 1990 Jun 1; 143(6): 1225-6. |
| [12] | Dogra PN, Ansari MS, Gupta NP, Tandon S. Holmium laser core-through urethrotomy for traumatic obliterative strictures of urethra: initial experience. Urology. 2004 Aug 1; 64(2): 232-5. |
| [13] | Podesta M, Podesta Jr M. Delayed surgical repair of posttraumatic posterior urethral distraction defects in children and adolescents: long-term results. Journal of Pediatric Urology. 2015 Apr 1; 11(2): 67-e1. |
| [14] | Barbagli G, Bandini M, Balò S, Sansalone S, Butnaru D, Lazzeri M. Surgical treatment of bulbar urethral strictures: tips and tricks. International braz j urol. 2020 Jun 1; 46(4): 511-8. |
| [15] | Oszczudlowski M, Yepes C, Dobruch J, Martins FE. Outcomes of transecting versus non‐transecting urethroplasty for bulbar urethral stricture: a meta‐analysis. BJU international. 2023 Sep; 132(3): 252-61. |
| [16] | Memon I, Soomro KQ, Rajpar ZH, Abdullah A. Non-transecting anastomotic bulbar urethroplasty for urethral stricture disease-experience from a high-volume specialist centre. Journal of Ayub Medical College Abbottabad. 2020 Feb 18; 32(1): 99-103. |
| [17] | Ballesteros Ruiz C, Bandini M, Joshi PM, Bafna S, Sharma V, Yatam SL, Bhadranavar S, Patil A, Kulkarni SB. Dorsal approach for double-face bulbar urethroplasty: ventral inlay plus dorsal onlay using Kulkarni one-side dissection. International Urology and Nephrology. 2022 May; 54(5): 1039-45. |
| [18] | Enganti B, Reddy MS, Chiruvella M, Bendigeri MT, Ragoori D, Ghouse SM, Reddy P. Double-face augmentation urethroplasty for bulbar urethral strictures: analysis of short-term outcomes. Turkish Journal of Urology. 2020 Jun 1; 46(5): 383. |
APA Style
Ranja, S., Kumar, A., Ranjan, P. (2025). Life-threatening Bleeding After Optical Internal Urethrotomy: Successfully Managed by Super- Selective Angioembolization, a Case Report and Review of Literature. International Journal of Clinical Urology, 9(1), 68-72. https://doi.org/10.11648/j.ijcu.20250901.21
ACS Style
Ranja, S.; Kumar, A.; Ranjan, P. Life-threatening Bleeding After Optical Internal Urethrotomy: Successfully Managed by Super- Selective Angioembolization, a Case Report and Review of Literature. Int. J. Clin. Urol. 2025, 9(1), 68-72. doi: 10.11648/j.ijcu.20250901.21
@article{10.11648/j.ijcu.20250901.21,
author = {Satish Ranja and Avinash Kumar and Prabhat Ranjan},
title = {Life-threatening Bleeding After Optical Internal Urethrotomy: Successfully Managed by Super- Selective Angioembolization, a Case Report and Review of Literature
},
journal = {International Journal of Clinical Urology},
volume = {9},
number = {1},
pages = {68-72},
doi = {10.11648/j.ijcu.20250901.21},
url = {https://doi.org/10.11648/j.ijcu.20250901.21},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20250901.21},
abstract = {Minor bleeding after internal urethrotomy is quite common and often subsides spontaneously. Mild to moderate persistent bleeding responds well with conservative management. Severe, life-threatening bleeding that necessitates invasive intervention is seldom seen these days. Selective or super-selective angioembolization is highly effective in these cases and has minimal associated morbidity. Here, we present a case of refractory urethral bleeding after optical internal urethrotomy (OIU) successfully managed by super-selective angioembolization. A 59-year-old man was referred to us with massive pericather bleeding after a cold knife internal urethrotomy done at a peripheral center 5 days ago. There was recurrent clot retention and a clinically significant drop in hemoglobin while on conservative management. Two units of LDPRBC were transfused. There was no history of chronic liver or kidney disease or any coagulation disorders. After Initial conservative measures failed, the patient underwent a computed tomography angiogram of the pelvis, which revealed a pseudoaneurysm arising from the bulbourethral artery. Different invasive management approaches like endoscopic fulguration, angioembolization, and open surgical repair have been explained and discussed with the patient and their relatives. Following shared decision-making and informed consent, angioembolization of the bulbourethral artery was performed. The bleeding stopped after the procedure, and the patient was discharged after 24 hours of observation. The present report highlights the use of super-selective embolization in severe urethral bleeding if initial conservative measures failed.
},
year = {2025}
}
TY - JOUR T1 - Life-threatening Bleeding After Optical Internal Urethrotomy: Successfully Managed by Super- Selective Angioembolization, a Case Report and Review of Literature AU - Satish Ranja AU - Avinash Kumar AU - Prabhat Ranjan Y1 - 2025/04/27 PY - 2025 N1 - https://doi.org/10.11648/j.ijcu.20250901.21 DO - 10.11648/j.ijcu.20250901.21 T2 - International Journal of Clinical Urology JF - International Journal of Clinical Urology JO - International Journal of Clinical Urology SP - 68 EP - 72 PB - Science Publishing Group SN - 2640-1355 UR - https://doi.org/10.11648/j.ijcu.20250901.21 AB - Minor bleeding after internal urethrotomy is quite common and often subsides spontaneously. Mild to moderate persistent bleeding responds well with conservative management. Severe, life-threatening bleeding that necessitates invasive intervention is seldom seen these days. Selective or super-selective angioembolization is highly effective in these cases and has minimal associated morbidity. Here, we present a case of refractory urethral bleeding after optical internal urethrotomy (OIU) successfully managed by super-selective angioembolization. A 59-year-old man was referred to us with massive pericather bleeding after a cold knife internal urethrotomy done at a peripheral center 5 days ago. There was recurrent clot retention and a clinically significant drop in hemoglobin while on conservative management. Two units of LDPRBC were transfused. There was no history of chronic liver or kidney disease or any coagulation disorders. After Initial conservative measures failed, the patient underwent a computed tomography angiogram of the pelvis, which revealed a pseudoaneurysm arising from the bulbourethral artery. Different invasive management approaches like endoscopic fulguration, angioembolization, and open surgical repair have been explained and discussed with the patient and their relatives. Following shared decision-making and informed consent, angioembolization of the bulbourethral artery was performed. The bleeding stopped after the procedure, and the patient was discharged after 24 hours of observation. The present report highlights the use of super-selective embolization in severe urethral bleeding if initial conservative measures failed. VL - 9 IS - 1 ER -
Department of Urology and Kidney Transplantation, Jayprabha Medanta Superspeciality Hospital, Patna, India
Department of Radiodiagnosis and Imaging, Jayprabha Medanta Superspeciality Hospital, Patna, India
Department of Urology and Kidney Transplantation, Jayprabha Medanta Superspeciality Hospital, Patna, India
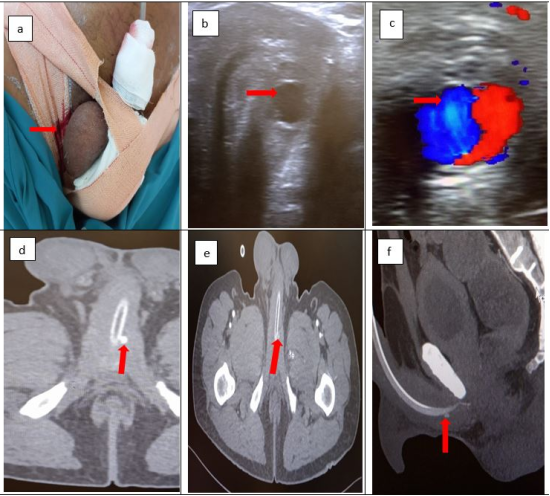
Figure 1. a. Perineal and penile compression, note the bleeding (red arrow), b. grey scale ultrasonography showed a hypoechoic area surrounding the bulbar urethra, c. color Doppler showed pseudoaneurysm, d, e, f. CT angiogram of pelvis suggestive of pseudo aneurysm of the bulbourethral artery (red arrow).
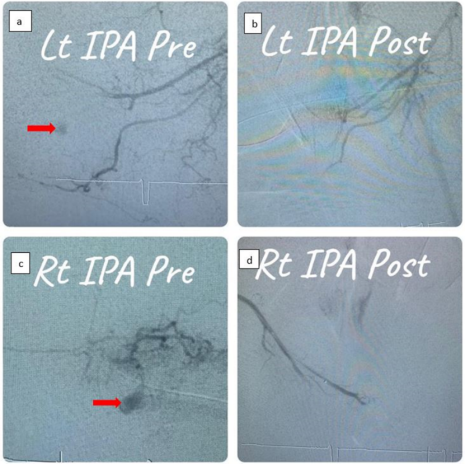
Figure 2. Digital subtraction angiography. A, c. contrast extravasation from the branches of the internal pudendal artery, likely bulbourethral artery (red arrow). b. d. No extravasation after embolization.
Information

