Abstract
Functional decline is common among LTC patients and is linked to poor outcomes, such as higher levels of dependency, hospitalizations, and death. Early phase after admission into facilities can be considered a crucial time frame when residents might have a rapid deterioration. Nevertheless, there is limited knowledge regarding predictors of early functional decline among LTC patients. Main objective of this research is to systematically identify and synthesize prognostic factors associated with early functional decline among long-term care residents. A systematic review was carried out based on PRISMA guidelines. The search strategy involved the use of electronic databases such as PubMed, Embase, Scopus, Web of Science, and Cochrane Library. Studies involving predictors of functional impairment among nursing home residents were included in the review. Extraction and assessment of study data were done using standardized instruments. Heterogeneity across studies led to a narrative synthesis. A total of seven studies with more than 400,000 LTC facility residents were considered. Functional decline was mainly measured using ADL-based measures. Cognitive impairment and preexisting functional state proved to be the most robust and significant predictors of functional decline. Other risk factors like urinary incontinence, co-morbidities, and impaired balance were found to increase the risk. Depression and medication usage showed inconclusive evidence. Geriatrician presence at facilities and disruption at the systems level, like the coronavirus pandemic, decreased and increased functional decline, respectively. The occurrence of functional decline in LTC facilities is complex and results from the interaction between vulnerability and the environment. Early detection of at-risk patients through a thorough assessment can help implement appropriate strategies. There is a need for more studies to validate outcome criteria and modifiable predictors.
Keywords
LTC, Functional Decline, ADL, Prognostic Factors, Nursing Home Residents, Cognitive Impairment, Geriatric Syndromes
1. Introduction
Ageing of the population is a characteristic feature of demographics in the modern world, resulting in a sharp rise in the number of elderly people who require LTC services. Nursing homes and other LTC facilities tend to host patients with complicated health problems such as multimorbidity, frailty, and different levels of cognitive and physical impairment
| [1] | Yuan Y, Lapane KL, Tjia J, Baek J, Liu S-H, Ulbricht CM. Physical frailty and cognitive impairment in older nursing home residents: a latent class analysis. BMC Geriatrics. 2021 Sep 7; 21(1). https://doi.org/10.1186/s12877-021-02433-1 |
| [2] | Carrasco-Ribelles LA, Roso-Llorach A, Cabrera-Bean M, Costa-Garrido A, Zabaleta-Del-Olmo E, Toran-Monserrat P, et al. Dynamics of multimorbidity and frailty, and their contribution to mortality, nursing home and home care need: A primary care cohort of 1 456 052 ageing people. EClinicalMedicine. 2022 Oct 1; 52: 101610.
https://doi.org/10.1016/j.eclinm.2022.101610 |
[1, 2]
. In this regard, functional status and ADLs are considered a marker of independence, quality of life, and health for the target population
| [3] | Kim J-H, Lee SB. Evaluation of Activities of Daily Living: Current Insights and Future Horizons. Annals of Geriatric Medicine and Research. 2025 Feb 6; 29(2).
https://doi.org/10.4235/agmr.24.0172 |
[3]
.
Functional impairment is a common problem in the LTC population and results in several negative consequences, including increased utilization of health services, hospitalizations, institutional dependency, and even mortality. In particular, the transition period after the admission into the facility is a crucial stage where a rapid decline in the functional status can be observed
. This condition is often provoked by environmental changes, accommodation to new living conditions, decreased physical activity, and exacerbation of preexisting diseases
| [5] | Laborde C, Ankri J, Cambois E. Environmental barriers matter from the early stages of functional decline among older adults in France. PLoS ONE [Internet]. 2022 Jun 22 [cited 2023 Apr 3]; 17(6): e0270258.
https://doi.org/10.1371/journal.pone.0270258 |
[5]
.
One of the distinctive features of modern demographics is ageing of the population, causing an increasing number of elderly persons requiring LTC services
| [6] | Jerez-Roig J, de Brito Macedo Ferreira LM, Torres de Araújo JR, Costa Lima K. Functional decline in nursing home residents: A prognostic study. Chen K, editor. PLOS ONE. 2017 May 11; 12(5): e0177353.
https://doi.org/10.1371/journal.pone.0177353 |
| [7] | Tind AM, Hoeck B, Andersen HE, Delmar C. Navigating health inequities in aging: The impact of social determinants on health and homecare nursing for older people. Geriatric Nursing [Internet]. 2025 Nov 13; 67: 103714.
https://doi.org/10.1016/j.gerinurse.2025.103714 |
[6, 7]
. LTC facilities usually serve people with complex clinical conditions, including multimorbidity, frailty, and various degrees of both physical and cognitive impairments
| [8] | Holland E, Matthews K, Macdonald S, Ashworth M, Laidlaw L, Sum K, et al. The impact of living with multiple long-term conditions (multimorbidity) on everyday life – a qualitative evidence synthesis. BMC Public Health [Internet]. 2024 Dec 18; 24(1). https://doi.org/10.1186/s12889-024-20763-8 |
[8]
. In this respect, functional status and ADLs are seen as a reflection of patient autonomy, quality of life, and health status in question.
Functional deficits among LTC clients are widespread phenomenon and lead to a number of adverse effects, among which increased use of medical resources, hospital admissions, dependence on institutions, and even mortality
| [9] | Gentili S, Riccardi F, Gialloreti LE, Scarcella P, Stievano A, Proietti MG, et al. Admission to the Long-Term Care Facilities and Institutionalization Rate in Community-Dwelling Frail Adults: An Observational Longitudinal Cohort Study. Healthcare. 2022 Feb 7; 10(2): 317.
https://doi.org/10.3390/healthcare10020317 |
| [10] | Egbujie BA, Turcotte LA, Heckman G, Hirdes JP. Trajectories of functional decline and predictors in long-term care settings: a retrospective cohort analysis of Canadian nursing home residents. Age and Ageing [Internet]. 2024 Nov 28 [cited 2025 Jan 22]; 53(12). https://doi.org/10.1093/ageing/afae264 |
| [11] | Balqis-Ali NZ, Jawahir S, Chan YM, Lim AW-Y, Azlan UW, Sabila S, et al. The impact of long-term care interventions on healthcare utilisation among older persons: a scoping review of reviews. BMC geriatrics. 2024 Jun 3; 24(1).
https://doi.org/10.1186/s12877-024-05097-9 |
[9-11]
. Importantly, a certain period following the entry to LTC facilities may be especially risky from the perspective of functional deficits, which occur due to adaptation problems to new environment, decreased activity, and aggravations of pre-existing pathologies.
As such, a systematic review is indicated to bring together all the existing information and find the consistent and reliable predictive factors. It will help to fill the gaps in knowledge that exist within the existing literature on this topic.
The objective of this systematic review is to find prognostic factors associated with the early functional decline of newly admitted long-term care patients.
2. Materials and Methods
2.1. Study Design
This systematic review was conducted in accordance with the PRISMA guidelines
| [12] | Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. British Medical Journal [Internet]. 2021; 372(71).
https://doi.org/10.1136/bmj.n71 |
[12]
. The review aimed to identify and synthesize evidence on prognostic factors associated with functional decline among LTC residents.
2.2. Literature Search Strategy
A comprehensive literature search was conducted across multiple electronic databases, including PubMed, Embase, Scopus, Web of Science, and the Cochrane Library. The search strategy combined controlled vocabulary such as MeSH terms and free-text terms related to long-term care, functional decline, and prognostic factors.
Key search terms included combinations of:
a. “long-term care” OR “nursing home” OR “residential care”
b. “functional decline” OR “activities of daily living” OR “ADL decline”
c. “predictor” OR “risk factor” OR “prognostic factor”
d. “admission” OR “newly admitted residents”
Searches were limited to studies published in the ten years to ensure relevance to current clinical practice. Reference lists of included studies were also screened to identify additional relevant articles.
2.3. Eligibility Criteria
Studies were selected based on predefined inclusion and exclusion criteria structured using the PICOS framework.
Inclusion Criteria
1) Population: Adults residing in long-term care or nursing home settings
2) Exposure: Prognostic factors or predictors of functional decline
3) Outcome: Functional decline measured using validated tools (e.g., ADL scales, Barthel Index, mobility measures)
4) Study design: Observational studies (e.g., cohort, longitudinal studies)
5) Language: English
6) Publication date: Within the 2016 to 2026
Exclusion Criteria
1) Studies not conducted in LTC or nursing home populations
2) Studies not reporting functional decline outcomes
3) Studies without prognostic or predictor analysis
4) Reviews, case reports, editorials, or non-primary research
Studies lacking sufficient methodological detail or effect size reporting.
2.4. Study Selection Process
All identified records were imported into Covidence systematic review software for screening. Duplicate records were removed automatically and manually verified. Title and abstract screening were conducted independently based on the eligibility criteria. Full-text articles were then assessed for inclusion. Reasons for exclusion at the full-text stage were recorded and categorized. The study selection process was summarized using a PRISMA flow diagram.
2.5. Data Extraction
Data extraction was performed using a structured, pre-defined extraction template developed within Covidence. The following information was extracted from each included study:
1) Study characteristics (author, year, country, design)
2) Population details (sample size, age, gender, setting)
3) Outcome measures (e.g., ADL scales, mobility tests)
4) Predictors of functional decline
5) Measurement methods and timing of predictors
6) Effect sizes (odds ratios, hazard ratios, regression coefficients)
7) Confidence intervals and p-values
8) Adjustment for confounders
Extraction focused on statistically significant predictors, while non-significant findings were also noted where relevant.
2.6. Quality Assessment
The methodological quality of included studies was assessed using domains adapted from the QUIPS tool
| [13] | Grooten WJA, Tseli E, Äng BO, Boersma K, Stålnacke B-M, Gerdle B, et al. Elaborating on the assessment of the risk of bias in prognostic studies in pain rehabilitation using QUIPS—aspects of interrater agreement. Diagnostic and Prognostic Research. 2019 Mar 7;3(1).
https://doi.org/10.1186/s41512-019-0050-0 |
[13]
. The following domains were evaluated:
a. Study participation
b. Study attrition
c. Prognostic factor measurement
d. Outcome measurement
e. Confounding measurement and control
f. Statistical analysis and reporting
Each study was rated as having low, moderate, or high risk of bias across domains. Discrepancies were resolved through discussion.
2.7. Data Synthesis
Due to substantial heterogeneity in study designs, outcome measures, and statistical reporting, a meta-analysis was not feasible. Instead, a narrative synthesis approach was adopted. Predictors of functional decline were grouped into thematic categories:
1) Cognitive factors
2) Functional and mobility-related factors
3) Clinical factors
4) Facility-level factors
Findings were synthesized by comparing the direction, consistency, and strength of associations across studies.
2.8. Data Availability
No supplementary materials were generated for this study. All data analyzed in this systematic review were obtained from previously published studies and are fully presented within the manuscript.
3. Results
3.1. Study Selection
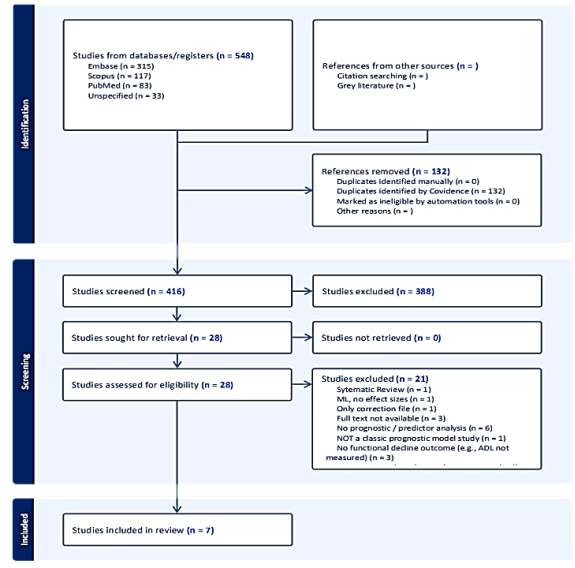
Figure 1. PRISMA flow diagram illustrating the study selection process.
A total of 548 records were identified through database searching, including Embase (n = 315), Scopus (n = 117), PubMed (n = 83), and additional unspecified sources (n = 33). After removal of 132 duplicate records, 416 studies remained for title and abstract screening.
During the screening phase, 388 records were excluded based on irrelevance to the review topic. The remaining 28 studies were assessed for full-text eligibility. All retrieved articles were successfully accessed, with no reports missing.
Of the 28 full-text articles assessed, 21 studies were excluded for the following reasons: lack of prognostic or predictor analysis (n = 6), absence of functional decline outcomes (n = 3), inappropriate study design (n = 2), wrong setting (n = 2), wrong population (n = 1), systematic review (n = 1), methodological limitations such as lack of effect sizes (n = 1), correction-only publication (n = 1), full-text unavailability (n = 3), and not constituting a classical prognostic study (n = 1).
Therefore, seven studies met the inclusion criteria and were included in this systematic review. No additional studies were identified through citation searching or grey literature sources. The study selection process is illustrated in
Figure 1 (PRISMA flow diagram).
3.2. Characteristics of Included Studies
The seven included studies were published between 2016 and 2026 and comprised a combination of longitudinal cohort, retrospective cohort, and prospective observational designs. All studies were conducted in LTC or nursing home settings and focused on older adult populations, often with high levels of baseline functional and cognitive impairment.
The studies were conducted across multiple countries, including Canada, Italy, and Brazil, with Canadian studies representing the majority. Sample sizes varied substantially, ranging from a small prospective cohort of 26 participants
| [14] | Chu CH, Quan AML, McGilton KS. Depression and Functional Mobility Decline in Long Term Care Home Residents with Dementia: a Prospective Cohort Study. Canadian Geriatrics Journal [Internet]. 2021 Dec 1; 24(4): 325–31.
https://doi.org/10.5770/cgj.24.511 |
[14]
to large population-based administrative datasets including over 200,000 residents
| [10] | Egbujie BA, Turcotte LA, Heckman G, Hirdes JP. Trajectories of functional decline and predictors in long-term care settings: a retrospective cohort analysis of Canadian nursing home residents. Age and Ageing [Internet]. 2024 Nov 28 [cited 2025 Jan 22]; 53(12). https://doi.org/10.1093/ageing/afae264 |
[10]
. Across all included studies, a total of over 400,000 long-term care residents were represented.
Follow-up duration varied considerably across studies, ranging from 60 days in short-term prospective analyses to 24–36 months in longitudinal cohort studies. Most studies assessed functional decline over time using repeated measurements.
Functional decline was primarily measured using validated Activities of Daily Living (ADL)-based scales, including the interRAI ADL Hierarchy Scale (0–6) and the ADL Long-Form Scale (0–28). One study utilised the Barthel Index, while another assessed functional mobility using performance-based measures such as the TUG and 2MWT. Despite variation in measurement tools, all studies captured decline in functional ability over time. A summary of the characteristics of the included studies is presented in
Table 1.
Table 1. Characteristics of Included Studies.
Study | Country | Design | Sample Size | Population | Outcome Measure |
Egbujie 10] | Canada | Retrospective cohort | 204,036 | LTC residents | interRAI ADL Hierarchy (0–6) |
Egbujie 15] (COVID) | Canada | Longitudinal cohort | 199,598 | LTC residents | interRAI ADL Hierarchy (0–6) |
Lane 16] | Canada | Longitudinal cohort | 12,334 | Newly admitted LTC residents | ADL Long-Form (0–28) |
Fedecostante 17] | Italy | Cohort study | 1,760 | Nursing home residents | ADL Long-Form (0–28) |
Fedecostante 18] | Italy | Cohort study | 1,263 | Nursing home residents | ADL decline |
Jerez-Roig 6] | Brazil | Longitudinal cohort | 280 | Nursing home residents | Barthel Index (modified) |
3.3. Outcome Measures
Functional decline was assessed across all included studies; however, there was considerable heterogeneity in the measurement tools and operational definitions used.
Most studies evaluated functional status using validated ADL-based instruments, including the interRAI ADL Hierarchy Scale (0–6) and the ADL Long-Form Scale (0–28). These measures quantify levels of dependence in daily activities, with higher scores generally indicating greater functional impairment. One study utilized the Barthel Index (modified) to assess functional ability, while another employed performance-based mobility measures, including the TUG and the 2MWT, to capture changes in physical function over time.
Despite differences in scales and scoring systems, all studies assessed decline in functional ability longitudinally, either as a deterioration in ADL scores, increased dependency, or reduced mobility performance. Due to this variability in outcome measures, scales, and reporting methods, quantitative pooling of results was not appropriate, and a narrative synthesis approach was adopted.
3.4. Predictors of Functional Decline
Predictors of functional decline identified across the included studies can be grouped into four main domains: cognitive factors, functional and mobility-related factors, clinical conditions, and facility-level factors.
3.4.1. Cognitive Factors
Cognitive impairment emerged as one of the most consistent and strongest predictors of functional decline, identified in four of the seven included studies.
In a multicenter cohort study, increasing severity of cognitive impairment was associated with significantly higher odds of functional decline, with effect sizes ranging from OR = 1.84 (95% CI: 1.42–2.39) to OR = 2.67 (95% CI: 1.91–3.72). Similarly, Jerez-Roig et al. (2017) reported that severe cognitive impairment nearly doubled the risk of functional decline (HR = 1.96; 95% CI: 1.30–2.94; p = 0.001).
Consistent findings were observed in a large population-based cohort, where cognitive impairment was associated with a faster rate of functional decline over time (β = +0.08 per month; 95% CI: 0.06–0.10; p < 0.001). These findings collectively indicate that cognitive status at baseline is a key determinant of subsequent functional trajectories in long-term care residents.
3.4.2. Functional and Mobility-Related Factors
Baseline functional status was identified as the strongest predictor of functional decline across studies. In a large administrative cohort, severe functional impairment at admission was strongly associated with subsequent decline, with a markedly increased likelihood of adverse functional trajectories (OR = 0.033; 95% CI: 0.031–0.035; p < 0.001), indicating a strong relationship between baseline dependency and future deterioration.
Mobility-related impairments were also significant predictors. Balance impairment was associated with an increased rate of functional decline (β = +0.04 per month; 95% CI: 0.02–0.06; p < 0.05), highlighting the importance of physical stability in maintaining functional independence.
3.4.3. Clinical Factors
Several clinical factors were associated with functional decline, although findings were less consistent across studies.
Urinary incontinence was identified as a significant predictor in three studies, with effect sizes including OR = 1.73 (95% CI: 1.32–2.26) and HR = 1.85 (95% CI: 1.24–2.75; p = 0.002), indicating increased risk of decline among residents with continence issues.
Depression showed mixed evidence. One study reported a significant association between depressive symptoms and functional decline (OR = 1.45; 95% CI: 1.16–1.81; p = 0.005), whereas another found no statistically significant relationship (β = 0.004; 95% CI: −0.018 to 0.026; p > 0.05).
Medication use, particularly antipsychotic use, was associated with increased odds of functional decline in one study (OR = 1.30; 95% CI: 1.06–1.60; p = 0.016), although this association was not consistently observed across all studies.
Comorbidity burden, operationalized through hospitalization, was also associated with increased risk (HR = 1.62; 95% CI: 1.08–2.43; p = 0.002).
3.4.4. Facility-Level Factors
Facility-level characteristics also influenced functional outcomes. The presence of a geriatrician within the care setting was associated with a reduced risk of functional decline, with reported effect sizes of OR = 0.60 (95% CI: 0.41–0.88; p = 0.015) and OR = 0.45 (95% CI: 0.25–0.80; p < 0.05), suggesting a protective effect of specialized geriatric care.
In addition, system-level factors such as the COVID-19 pandemic period were associated with increased odds of functional decline (OR = 1.17; 95% CI: 1.15–1.20; p < 0.001), highlighting the impact of external disruptions on resident outcomes.
Table 2. Summary of Key Predictors of Functional Decline.
Predictor | Study | Effect Size | 95% CI | p-value | Direction |
Cognitive impairment | Fedecostante 17] | OR 2.67 | 1.91–3.72 | <0.001 | decline |
Cognitive impairment | Jerez-Roig 6] | HR 1.96 | 1.30–2.94 | 0.001 | decline |
Cognitive impairment | Lane 16] | β +0.08/month | 0.06–0.10 | <0.001 | decline |
Incontinence | Fedecostante 17] | OR 1.73 | 1.32–2.26 | <0.05 | decline |
Incontinence | Jerez-Roig 6] | HR 1.85 | 1.24–2.75 | 0.002 | decline |
Depression | Fedecostante 18] | OR 1.45 | 1.16–1.81 | 0.005 | decline |
3.5. Summary of Evidence
Across the seven included studies, a range of predictors of functional decline among long-term care residents were identified, spanning cognitive, functional, clinical, and facility-level domains.
Cognitive impairment and baseline functional status emerged as the most consistent and robust predictors; each identified in multiple studies and demonstrating strong associations with subsequent functional decline. In particular, increasing severity of cognitive impairment and higher levels of baseline dependency were associated with significantly greater risk of deterioration over time.
Clinical factors, including urinary incontinence and comorbidity burden, were also consistently associated with increased risk of decline, although the strength of these associations varied across studies. In contrast, evidence for depression and medication use was less consistent, with some studies reporting significant associations while others found no effect.
Facility-level factors, such as the presence of a geriatrician, appeared to have a protective effect on functional outcomes, whereas system-level disruptions, including the COVID-19 pandemic, were associated with increased functional decline.
Despite heterogeneity in study design, outcome measures, and statistical approaches, the findings demonstrate a clear pattern in which individual-level vulnerability (particularly cognitive and functional impairment), combined with clinical and environmental factors, contribute to the risk of functional decline in long-term care settings.
4. Discussion
4.1. Interpretation and Comparison with Existing Literature
This systematic review combined findings from seven research articles that have explored potential predictors of functional decline among residents in LTC settings. Generally, it can be seen that there is a sophisticated nature of the risk factors predicting functional decline within this population, as predictors can be related to cognition, function, clinical conditions, as well as characteristics of the LTC facility itself
| [19] | Hakimjavadi R, Yin CY, Scott M, Talarico R, Ramsay T, Webber C, et al. Cognitive and Functional Decline Among Long-Term Care Residents. JAMA network open [Internet]. 2025 Jan; 8(4): e255635.
https://doi.org/10.1001/jamanetworkopen.2025.5635 |
| [20] | Arora G, Milani C, Tanuseputro P, Tang P, Jeong A, Kobewka D, et al. Identifying predictors of cognitive decline in long-term care: a scoping review. BMC Geriatrics. 2023 Sep 5; 23(1). https://doi.org/10.1186/s12877-023-04193-6 |
| [21] | Ripley S, Alizadehsaravi N, Affoo R, Hunter S, Middleton LE, Moody E, et al. Resident-, family-, and staff-identified goals for rehabilitation of long-term care residents with dementia: a qualitative study. BMC Geriatrics. 2024 Jan 29; 24(1).
https://doi.org/10.1186/s12877-024-04674-2 |
[19-21]
.
However, cognitive decline and baseline function level turned out to be the strongest predictors for functional decline. Thus, it has been repeatedly demonstrated across several studies that increasing levels of cognitive dysfunction are positively correlated with higher risks of functional decline in LTC facilities
| [6] | Jerez-Roig J, de Brito Macedo Ferreira LM, Torres de Araújo JR, Costa Lima K. Functional decline in nursing home residents: A prognostic study. Chen K, editor. PLOS ONE. 2017 May 11; 12(5): e0177353.
https://doi.org/10.1371/journal.pone.0177353 |
| [19] | Hakimjavadi R, Yin CY, Scott M, Talarico R, Ramsay T, Webber C, et al. Cognitive and Functional Decline Among Long-Term Care Residents. JAMA network open [Internet]. 2025 Jan; 8(4): e255635.
https://doi.org/10.1001/jamanetworkopen.2025.5635 |
| [22] | Webber C, Milani C, Pugliese M, Lawlor PG, Bush SH, Watt C, et al. Long‐term cognitive impairment after probable delirium in long‐term care residents: A population‐based retrospective cohort study. Journal of the American Geriatrics Society. 2023 Nov 19; 72(4): 1183–90.
https://doi.org/10.1111/jgs.18675 |
[6, 19, 22]
. Moreover, the more dependent the resident was at baseline, the higher the chances of experiencing functional decline
| [6] | Jerez-Roig J, de Brito Macedo Ferreira LM, Torres de Araújo JR, Costa Lima K. Functional decline in nursing home residents: A prognostic study. Chen K, editor. PLOS ONE. 2017 May 11; 12(5): e0177353.
https://doi.org/10.1371/journal.pone.0177353 |
[6]
.
The clinical factors, such as incontinence and comorbidities, were also associated with an increased risk of decline, although their impact was more limited and diverse among different studies
| [2] | Carrasco-Ribelles LA, Roso-Llorach A, Cabrera-Bean M, Costa-Garrido A, Zabaleta-Del-Olmo E, Toran-Monserrat P, et al. Dynamics of multimorbidity and frailty, and their contribution to mortality, nursing home and home care need: A primary care cohort of 1 456 052 ageing people. EClinicalMedicine. 2022 Oct 1; 52: 101610.
https://doi.org/10.1016/j.eclinm.2022.101610 |
| [6] | Jerez-Roig J, de Brito Macedo Ferreira LM, Torres de Araújo JR, Costa Lima K. Functional decline in nursing home residents: A prognostic study. Chen K, editor. PLOS ONE. 2017 May 11; 12(5): e0177353.
https://doi.org/10.1371/journal.pone.0177353 |
| [23] | Dasdelen MF, Dasdelen ZB, Almas F, Cokkececi B, Laguna P, de la Rosette J, et al. Exploring the Association Between Urinary Incontinence and Depression Based on a Series of Large-Scale National Health Studies in Türkiye. Journal of Clinical Medicine [Internet]. 2025 Jul 23 [cited 2026 Feb 9]; 14(15): 5213. https://doi.org/10.3390/jcm14155213 |
| [24] | Bakhsh A, Alnazawi H, Alsehli O, Almuzaini M, Aloufi H, Alahmadi A, et al. The burden of urinary incontinence and its association with knowledge, practices, and comorbidities among women in Madinah, Saudi Arabia: a cross-sectional study. Frontiers in Medicine. 2026 Jan 12; 12.
https://doi.org/10.3389/fmed.2025.1726741 |
[2, 6, 23, 24]
. At the same time, the role of depression and medication in declining outcomes proved to be inconsistent, with some researchers finding the effect of both variables to be statistically significant, and others arguing there was no any significant connection
| [25] | Niarchou E, Roberts L, Naughton BD. What is the impact of antidepressant side effects on medication adherence among adult patients diagnosed with depressive disorder: A systematic review. Journal of Psychopharmacology. 2024 Feb 1; 38(2): 127–36.
https://doi.org/10.1177/02698811231224171 |
[25]
.
The significance of this study was based on identification of the impact of facility-related factors such as availability of geriatricians as well as the role played by such system-level factors as the COVID-19 pandemic
| [4] | Kleinpell RM, Fletcher K, Jennings BM. Reducing Functional Decline in Hospitalized Elderly [Internet]. Nih. gov. Agency for Healthcare Research and Quality (US); 2008.
https://www.ncbi.nlm.nih.gov/books/NBK2629/ |
| [26] | Dyer AH, Fallon A, Noonan C, Dolphin H, O’Farrelly C, Bourke NM, et al. Managing the Impact of COVID-19 in Nursing Homes and Long-Term Care Facilities: An Update. Journal of the American Medical Directors Association [Internet]. 2022 Sep 1; 23(9): 1590–602.
https://doi.org/10.1016/j.jamda.2022.06.028 |
[4, 26]
. The results indicated that the functioning of people receiving LTC could not be explained exclusively through individual characteristics, since facility and system-related factors also affected their functioning
| [5] | Laborde C, Ankri J, Cambois E. Environmental barriers matter from the early stages of functional decline among older adults in France. PLoS ONE [Internet]. 2022 Jun 22 [cited 2023 Apr 3]; 17(6): e0270258.
https://doi.org/10.1371/journal.pone.0270258 |
| [7] | Tind AM, Hoeck B, Andersen HE, Delmar C. Navigating health inequities in aging: The impact of social determinants on health and homecare nursing for older people. Geriatric Nursing [Internet]. 2025 Nov 13; 67: 103714.
https://doi.org/10.1016/j.gerinurse.2025.103714 |
[5, 7]
. As a result, these results suggest that functional decline in LTC residents is associated with the interaction of two main elements: the individual's own vulnerability and the effect of the surrounding
| [5] | Laborde C, Ankri J, Cambois E. Environmental barriers matter from the early stages of functional decline among older adults in France. PLoS ONE [Internet]. 2022 Jun 22 [cited 2023 Apr 3]; 17(6): e0270258.
https://doi.org/10.1371/journal.pone.0270258 |
| [7] | Tind AM, Hoeck B, Andersen HE, Delmar C. Navigating health inequities in aging: The impact of social determinants on health and homecare nursing for older people. Geriatric Nursing [Internet]. 2025 Nov 13; 67: 103714.
https://doi.org/10.1016/j.gerinurse.2025.103714 |
| [14] | Chu CH, Quan AML, McGilton KS. Depression and Functional Mobility Decline in Long Term Care Home Residents with Dementia: a Prospective Cohort Study. Canadian Geriatrics Journal [Internet]. 2021 Dec 1; 24(4): 325–31.
https://doi.org/10.5770/cgj.24.511 |
| [19] | Hakimjavadi R, Yin CY, Scott M, Talarico R, Ramsay T, Webber C, et al. Cognitive and Functional Decline Among Long-Term Care Residents. JAMA network open [Internet]. 2025 Jan; 8(4): e255635.
https://doi.org/10.1001/jamanetworkopen.2025.5635 |
[5, 7, 14, 19]
.
4.2. Strengths and Limitations of the Review
There are a number of strengths in this systematic review. First, it adhered to an evidence-based approach using sound methodology, consistent with the principles of a systematic review by performing a comprehensive search, developing selection criteria, and using Covidence software to screen the articles
| [11] | Balqis-Ali NZ, Jawahir S, Chan YM, Lim AW-Y, Azlan UW, Sabila S, et al. The impact of long-term care interventions on healthcare utilisation among older persons: a scoping review of reviews. BMC geriatrics. 2024 Jun 3; 24(1).
https://doi.org/10.1186/s12877-024-05097-9 |
| [27] | Shaheen N, Shaheen A, Ramadan A, Hefnawy MT, Ramadan A, Ibrahim I, et al. Appraising Systematic reviews: a Comprehensive Guide to Ensuring Validity and Reliability. Frontiers in Research Metrics and Analytics. 2023 Dec 21; 8(8).
https://doi.org/10.3389/frma.2023.1268045 |
[11, 27]
. The inclusion of studies from a wide variety of geographic regions, including Canada, Italy, and Brazil, improves the external validity of the study.
The second strength is that this review did not focus on interventions but on predictors of functional decline, allowing the synthesis of a better set of predictors to help in predicting prognosis. The use of structured data collection techniques and a quality assessment based on the domains of prognostic studies adds credibility to the results
| [28] | Matino D, Chai-Adisaksopha C, Iorio A. Systematic reviews of prognosis studies: a critical appraisal of five core clinical journals. Diagnostic and Prognostic Research. 2017 Mar 16; 1(1). https://doi.org/10.1186/s41512-017-0008-z |
[28]
. Furthermore, the inclusion of large-scale population studies, which include over 200,000 patients, ensures adequate statistical power and credibility
| [10] | Egbujie BA, Turcotte LA, Heckman G, Hirdes JP. Trajectories of functional decline and predictors in long-term care settings: a retrospective cohort analysis of Canadian nursing home residents. Age and Ageing [Internet]. 2024 Nov 28 [cited 2025 Jan 22]; 53(12). https://doi.org/10.1093/ageing/afae264 |
| [15] | Egbujie BA, Turcotte LA, Heckman GA, Morris JN, Hirdes JP. Functional Decline in Long-Term Care Homes in the First Wave of the COVID-19 Pandemic: A Population-based Longitudinal Study in Five Canadian Provinces. Journal of the American Medical Directors Association. 2024 Feb 1; 25(2): 282–9.
https://doi.org/10.1016/j.jamda.2023.09.007 |
[10, 15]
.
However, there are some weaknesses that must be considered. For example, the heterogeneity between the studies, especially concerning the outcome measure, length of follow-up, and statistical method. Functional decline was measured using several instruments, such as different ADL scales and performance measures, which reduced the possibility of comparing the findings and conducting a meta-analysis
| [3] | Kim J-H, Lee SB. Evaluation of Activities of Daily Living: Current Insights and Future Horizons. Annals of Geriatric Medicine and Research. 2025 Feb 6; 29(2).
https://doi.org/10.4235/agmr.24.0172 |
| [29] | Liebzeit D, King B, Bratzke L. Measurement of function in older adults transitioning from hospital to home: an integrative review. Geriatric Nursing. 2018 May; 39(3): 336–43.
https://doi.org/10.1016/j.gerinurse.2017.11.003 |
[3, 29]
. In turn, a narrative synthesis strategy was employed, which might be prone to biases and subjective evaluations
.
Moreover, variations regarding the reporting of effect size within the articles made synthesis difficult. Some articles presented odds ratio or hazard ratio, while others utilized regression coefficients or even lacked quantitative estimations of the impact of predictor variables on functional decline, making comparison impossible
| [17] | Fedecostante M, Onder G, Eusebi P, Dell’Aquila G, Zengarini E, Carrieri B, et al. Predictors of Functional Decline in Nursing Home Residents: The Shelter Project. 2019 Dec 20; 75(8): 1600–5.
https://doi.org/10.1093/gerona/glz296 |
| [18] | Fedecostante M, Dell’Aquila G, Eusebi P, Volpato S, Zuliani G, Abete P, et al. Predictors of Functional Changes in Italian Nursing Home Residents: The U. L. I. S. S. E. Study. Journal of the American Medical Directors Association [Internet]. 2016 Apr [cited 2026 Apr 7]; 17(4): 306–11.
https://doi.org/10.1016/j.jamda.2015.11.004 |
[17, 18]
.
All the studies included had an observational study design, which makes it prone to residual confounding. While most of the studies adjusted for relevant covariates, there may be other unknowns that affected the results, including staffing, quality of care, or social activity
| [5] | Laborde C, Ankri J, Cambois E. Environmental barriers matter from the early stages of functional decline among older adults in France. PLoS ONE [Internet]. 2022 Jun 22 [cited 2023 Apr 3]; 17(6): e0270258.
https://doi.org/10.1371/journal.pone.0270258 |
| [7] | Tind AM, Hoeck B, Andersen HE, Delmar C. Navigating health inequities in aging: The impact of social determinants on health and homecare nursing for older people. Geriatric Nursing [Internet]. 2025 Nov 13; 67: 103714.
https://doi.org/10.1016/j.gerinurse.2025.103714 |
[5, 7]
. Moreover, some studies had a high risk of bias, especially concerning selection and loss to follow-up, impacting the internal validity of the research
| [13] | Grooten WJA, Tseli E, Äng BO, Boersma K, Stålnacke B-M, Gerdle B, et al. Elaborating on the assessment of the risk of bias in prognostic studies in pain rehabilitation using QUIPS—aspects of interrater agreement. Diagnostic and Prognostic Research. 2019 Mar 7;3(1).
https://doi.org/10.1186/s41512-019-0050-0 |
[13]
. Lastly, even though this systematic review concentrated on newly admitted or early-stage residents of LTC facilities, some studies may not have specifically restricted themselves to such patients.
4.3. Implications for Practice and Research
The conclusions from this systematic review will have significant clinical and research implications within the LTC setting.
On the one hand, clinicians should recognize the importance of early detection of cognitive impairments and baseline functioning in determining functional outcomes
| [3] | Kim J-H, Lee SB. Evaluation of Activities of Daily Living: Current Insights and Future Horizons. Annals of Geriatric Medicine and Research. 2025 Feb 6; 29(2).
https://doi.org/10.4235/agmr.24.0172 |
| [10] | Egbujie BA, Turcotte LA, Heckman G, Hirdes JP. Trajectories of functional decline and predictors in long-term care settings: a retrospective cohort analysis of Canadian nursing home residents. Age and Ageing [Internet]. 2024 Nov 28 [cited 2025 Jan 22]; 53(12). https://doi.org/10.1093/ageing/afae264 |
| [16] | Lane NE, Stukel TA, Boyd CM, Wodchis WP. Long-Term Care Residents’ Geriatric Syndromes at Admission and Disablement Over Time: An Observational Cohort Study. The Journals of Gerontology: Series A. 2018 Jun 27; 74(6): 917–23.
https://doi.org/10.1093/gerona/gly151 |
[3, 10, 16]
. In other words, the identification of risk factors should occur immediately upon admission to the LTC facility through the use of evidence-based assessment tools such as interRAI instruments
| [3] | Kim J-H, Lee SB. Evaluation of Activities of Daily Living: Current Insights and Future Horizons. Annals of Geriatric Medicine and Research. 2025 Feb 6; 29(2).
https://doi.org/10.4235/agmr.24.0172 |
[3]
. These assessments allow clinicians to identify patients at high risk of deterioration and develop individualized treatment plans. Thus, interventions aimed at supporting cognition, physical functioning, and independence should be prioritized for patients at high risk.
The role of modifiable clinical factors like urinary incontinence and potentially inappropriate medications suggests the potential for preventive measures that target these variables and decrease the risk of functional deterioration
| [2] | Carrasco-Ribelles LA, Roso-Llorach A, Cabrera-Bean M, Costa-Garrido A, Zabaleta-Del-Olmo E, Toran-Monserrat P, et al. Dynamics of multimorbidity and frailty, and their contribution to mortality, nursing home and home care need: A primary care cohort of 1 456 052 ageing people. EClinicalMedicine. 2022 Oct 1; 52: 101610.
https://doi.org/10.1016/j.eclinm.2022.101610 |
| [6] | Jerez-Roig J, de Brito Macedo Ferreira LM, Torres de Araújo JR, Costa Lima K. Functional decline in nursing home residents: A prognostic study. Chen K, editor. PLOS ONE. 2017 May 11; 12(5): e0177353.
https://doi.org/10.1371/journal.pone.0177353 |
[2, 6]
. Additionally, the observed protective effect of having a geriatrician emphasizes the importance of multidisciplinary care within LTC facilities
| [15] | Egbujie BA, Turcotte LA, Heckman GA, Morris JN, Hirdes JP. Functional Decline in Long-Term Care Homes in the First Wave of the COVID-19 Pandemic: A Population-based Longitudinal Study in Five Canadian Provinces. Journal of the American Medical Directors Association. 2024 Feb 1; 25(2): 282–9.
https://doi.org/10.1016/j.jamda.2023.09.007 |
[15]
.
In terms of systems, the results of this review demonstrate the vulnerability of LTC residents to the influence of external events, like the COVID-19 pandemic, and thus underline the necessity of developing resilient care systems focused on maintaining continuity of care, engagement in social life, and participation in physical activities even in critical situations
| [12] | Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. British Medical Journal [Internet]. 2021; 372(71).
https://doi.org/10.1136/bmj.n71 |
| [15] | Egbujie BA, Turcotte LA, Heckman GA, Morris JN, Hirdes JP. Functional Decline in Long-Term Care Homes in the First Wave of the COVID-19 Pandemic: A Population-based Longitudinal Study in Five Canadian Provinces. Journal of the American Medical Directors Association. 2024 Feb 1; 25(2): 282–9.
https://doi.org/10.1016/j.jamda.2023.09.007 |
[12, 15]
.
The research gaps identified through analyzing the selected studies point out to some important aspects that require further attention from scholars. First, there is a clear necessity to develop better standardization of measures used for evaluating outcomes, especially in terms of functional assessment tests
| [32] | Rodríguez‐Violante M, Hernández‐Medrano AJ, Cervantes‐Arriaga A. The Importance of Standardized Assessment. Movement Disorders Clinical Practice. 2024 May 26; 11(S3). https://doi.org/10.1002/mdc3.14085 |
[32]
. Another gap concerns the lack of uniformity in presenting effect sizes and statistical estimates which can be very helpful in quantitative synthesis of findings.
Finally, there is a requirement to conduct more research related to the role of interactions between predictors and their effects. In particular, longitudinal studies focused on new admissions to LTC facilities will help identify early changes in functionality in older patients and define the most important stages for interventions
| [9] | Gentili S, Riccardi F, Gialloreti LE, Scarcella P, Stievano A, Proietti MG, et al. Admission to the Long-Term Care Facilities and Institutionalization Rate in Community-Dwelling Frail Adults: An Observational Longitudinal Cohort Study. Healthcare. 2022 Feb 7; 10(2): 317.
https://doi.org/10.3390/healthcare10020317 |
| [11] | Balqis-Ali NZ, Jawahir S, Chan YM, Lim AW-Y, Azlan UW, Sabila S, et al. The impact of long-term care interventions on healthcare utilisation among older persons: a scoping review of reviews. BMC geriatrics. 2024 Jun 3; 24(1).
https://doi.org/10.1186/s12877-024-05097-9 |
[9, 11]
.
5. Conclusions
This review provides evidence showing that the decline of functions of LTCF residents depends on a combination of factors, which are cognitive, functional, clinical, and environmental
| [10] | Egbujie BA, Turcotte LA, Heckman G, Hirdes JP. Trajectories of functional decline and predictors in long-term care settings: a retrospective cohort analysis of Canadian nursing home residents. Age and Ageing [Internet]. 2024 Nov 28 [cited 2025 Jan 22]; 53(12). https://doi.org/10.1093/ageing/afae264 |
| [16] | Lane NE, Stukel TA, Boyd CM, Wodchis WP. Long-Term Care Residents’ Geriatric Syndromes at Admission and Disablement Over Time: An Observational Cohort Study. The Journals of Gerontology: Series A. 2018 Jun 27; 74(6): 917–23.
https://doi.org/10.1093/gerona/gly151 |
| [17] | Fedecostante M, Onder G, Eusebi P, Dell’Aquila G, Zengarini E, Carrieri B, et al. Predictors of Functional Decline in Nursing Home Residents: The Shelter Project. 2019 Dec 20; 75(8): 1600–5.
https://doi.org/10.1093/gerona/glz296 |
[10, 16, 17]
. Cognitive decline and initial functional status appear to be the strongest predictors of the outcomes under consideration, which indicates their critical importance for the assessment and management of functional decline. While clinical factors such as incontinence and comorbidity contribute to risk, and facility-level characteristics may modify outcomes, the findings highlight the importance of early identification and comprehensive, multidimensional care approaches
| [2] | Carrasco-Ribelles LA, Roso-Llorach A, Cabrera-Bean M, Costa-Garrido A, Zabaleta-Del-Olmo E, Toran-Monserrat P, et al. Dynamics of multimorbidity and frailty, and their contribution to mortality, nursing home and home care need: A primary care cohort of 1 456 052 ageing people. EClinicalMedicine. 2022 Oct 1; 52: 101610.
https://doi.org/10.1016/j.eclinm.2022.101610 |
| [5] | Laborde C, Ankri J, Cambois E. Environmental barriers matter from the early stages of functional decline among older adults in France. PLoS ONE [Internet]. 2022 Jun 22 [cited 2023 Apr 3]; 17(6): e0270258.
https://doi.org/10.1371/journal.pone.0270258 |
[2, 5]
. Addressing these factors has the potential to improve functional outcomes and quality of life for residents in long-term care settings.
Abbreviations
ADL | Activities of Daily Living |
CI | Confidence Interval |
CPS | Cognitive Performance Scale |
LTC | Long-Term Care |
LTCF | Long-Term Care Facility |
MDS | Minimum Data Set |
OR | Odds Ratio |
HR | Hazard Ratio |
β | Bets Coefficient |
PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
QUIPS | Quality In Prognosis Studies |
TUG | Timed up and Go Test |
2MWT | 2-Minute Walk Test |
COVID-19 | Coronavirus Disease 2019 |
Acknowledgments
The authors would like to acknowledge the support of the School of Medicine, Rio Grande, USA for providing an academic environment that facilitated the completion of this study. We also appreciate access to scientific databases and research tools that supported the systematic literature search and analysis conducted in this review.
The authors further acknowledge the collaborative contribution of Thomas Afriye, a Master’s nursing student at the University of Rio Grande, United States, whose involvement was integral to the completion of this work.
Erastus Kihali expresses sincere gratitude to his family for their continuous emotional and financial support throughout the course of this research.
Author Contributions
Erastus Kihali: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing
Thomas Afriyie: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing
Funding
This research received no external funding.
Data Availability Statement
All data used in this study are derived from published literature and are available within the cited references.
Conflicts of Interest
The author declares no conflict of interest.
Appendix
Database Search Strategy
A comprehensive search strategy was developed to identify studies examining prognostic factors associated with functional decline among long-term care residents. The search combined controlled vocabulary (e.g., MeSH terms) and free-text terms related to long-term care settings, functional decline, and prognostic factors.
The following core concepts were used:
Concept 1: Long-Term Care Setting
("long-term care" OR "nursing home*" OR "care home*" OR "residential care" OR "long term care facility*" OR LTC OR LTCF)
Concept 2: Functional Decline
("functional decline" OR "functional deterioration" OR "activities of daily living" OR ADL OR "ADL decline" OR "functional impairment" OR "mobility decline")
Concept 4: Prognostic Factors
("predictor*" OR "risk factor*" OR "prognostic factor*" OR determinant* OR "associated factor*")
Concept 5: Admission / Early Phase
("admission" OR "newly admitted" OR "incident resident*" OR baseline OR "early decline")
Final Combined Search Strategy
(c1) AND (c2) AND (c3) AND (c4)
Example (PubMed Search Strategy)
(("long-term care" [Title/Abstract] OR "nursing home*" [Title/Abstract] OR "care home*" [Title/Abstract] OR "residential care" [Title/Abstract])
AND
("functional decline" [Title/Abstract] OR "activities of daily living" [Title/Abstract] OR ADL [Title/Abstract] OR "functional impairment" [Title/Abstract])
AND
("predictor*" [Title/Abstract] OR "risk factor*" [Title/Abstract] OR "prognostic factor*" [Title/Abstract])
AND
("admission" [Title/Abstract] OR "newly admitted" [Title/Abstract] OR baseline [Title/Abstract]))
Filters: English, last 5–10 years
Database Adaptation (IMPORTANT FOR METHODS)
The search strategy was adapted for each database:
Table A1. Search Vocabulary on each Database.
Database | Adaptation |
PubMed | MeSH + Title/Abstract |
Embase | Emtree + keywords |
Scopus | TITLE-ABS-KEY |
Web of Science | Topic search |
Cochrane | Keywords only |
References
| [1] |
Yuan Y, Lapane KL, Tjia J, Baek J, Liu S-H, Ulbricht CM. Physical frailty and cognitive impairment in older nursing home residents: a latent class analysis. BMC Geriatrics. 2021 Sep 7; 21(1).
https://doi.org/10.1186/s12877-021-02433-1
|
| [2] |
Carrasco-Ribelles LA, Roso-Llorach A, Cabrera-Bean M, Costa-Garrido A, Zabaleta-Del-Olmo E, Toran-Monserrat P, et al. Dynamics of multimorbidity and frailty, and their contribution to mortality, nursing home and home care need: A primary care cohort of 1 456 052 ageing people. EClinicalMedicine. 2022 Oct 1; 52: 101610.
https://doi.org/10.1016/j.eclinm.2022.101610
|
| [3] |
Kim J-H, Lee SB. Evaluation of Activities of Daily Living: Current Insights and Future Horizons. Annals of Geriatric Medicine and Research. 2025 Feb 6; 29(2).
https://doi.org/10.4235/agmr.24.0172
|
| [4] |
Kleinpell RM, Fletcher K, Jennings BM. Reducing Functional Decline in Hospitalized Elderly [Internet]. Nih. gov. Agency for Healthcare Research and Quality (US); 2008.
https://www.ncbi.nlm.nih.gov/books/NBK2629/
|
| [5] |
Laborde C, Ankri J, Cambois E. Environmental barriers matter from the early stages of functional decline among older adults in France. PLoS ONE [Internet]. 2022 Jun 22 [cited 2023 Apr 3]; 17(6): e0270258.
https://doi.org/10.1371/journal.pone.0270258
|
| [6] |
Jerez-Roig J, de Brito Macedo Ferreira LM, Torres de Araújo JR, Costa Lima K. Functional decline in nursing home residents: A prognostic study. Chen K, editor. PLOS ONE. 2017 May 11; 12(5): e0177353.
https://doi.org/10.1371/journal.pone.0177353
|
| [7] |
Tind AM, Hoeck B, Andersen HE, Delmar C. Navigating health inequities in aging: The impact of social determinants on health and homecare nursing for older people. Geriatric Nursing [Internet]. 2025 Nov 13; 67: 103714.
https://doi.org/10.1016/j.gerinurse.2025.103714
|
| [8] |
Holland E, Matthews K, Macdonald S, Ashworth M, Laidlaw L, Sum K, et al. The impact of living with multiple long-term conditions (multimorbidity) on everyday life – a qualitative evidence synthesis. BMC Public Health [Internet]. 2024 Dec 18; 24(1).
https://doi.org/10.1186/s12889-024-20763-8
|
| [9] |
Gentili S, Riccardi F, Gialloreti LE, Scarcella P, Stievano A, Proietti MG, et al. Admission to the Long-Term Care Facilities and Institutionalization Rate in Community-Dwelling Frail Adults: An Observational Longitudinal Cohort Study. Healthcare. 2022 Feb 7; 10(2): 317.
https://doi.org/10.3390/healthcare10020317
|
| [10] |
Egbujie BA, Turcotte LA, Heckman G, Hirdes JP. Trajectories of functional decline and predictors in long-term care settings: a retrospective cohort analysis of Canadian nursing home residents. Age and Ageing [Internet]. 2024 Nov 28 [cited 2025 Jan 22]; 53(12).
https://doi.org/10.1093/ageing/afae264
|
| [11] |
Balqis-Ali NZ, Jawahir S, Chan YM, Lim AW-Y, Azlan UW, Sabila S, et al. The impact of long-term care interventions on healthcare utilisation among older persons: a scoping review of reviews. BMC geriatrics. 2024 Jun 3; 24(1).
https://doi.org/10.1186/s12877-024-05097-9
|
| [12] |
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. British Medical Journal [Internet]. 2021; 372(71).
https://doi.org/10.1136/bmj.n71
|
| [13] |
Grooten WJA, Tseli E, Äng BO, Boersma K, Stålnacke B-M, Gerdle B, et al. Elaborating on the assessment of the risk of bias in prognostic studies in pain rehabilitation using QUIPS—aspects of interrater agreement. Diagnostic and Prognostic Research. 2019 Mar 7;3(1).
https://doi.org/10.1186/s41512-019-0050-0
|
| [14] |
Chu CH, Quan AML, McGilton KS. Depression and Functional Mobility Decline in Long Term Care Home Residents with Dementia: a Prospective Cohort Study. Canadian Geriatrics Journal [Internet]. 2021 Dec 1; 24(4): 325–31.
https://doi.org/10.5770/cgj.24.511
|
| [15] |
Egbujie BA, Turcotte LA, Heckman GA, Morris JN, Hirdes JP. Functional Decline in Long-Term Care Homes in the First Wave of the COVID-19 Pandemic: A Population-based Longitudinal Study in Five Canadian Provinces. Journal of the American Medical Directors Association. 2024 Feb 1; 25(2): 282–9.
https://doi.org/10.1016/j.jamda.2023.09.007
|
| [16] |
Lane NE, Stukel TA, Boyd CM, Wodchis WP. Long-Term Care Residents’ Geriatric Syndromes at Admission and Disablement Over Time: An Observational Cohort Study. The Journals of Gerontology: Series A. 2018 Jun 27; 74(6): 917–23.
https://doi.org/10.1093/gerona/gly151
|
| [17] |
Fedecostante M, Onder G, Eusebi P, Dell’Aquila G, Zengarini E, Carrieri B, et al. Predictors of Functional Decline in Nursing Home Residents: The Shelter Project. 2019 Dec 20; 75(8): 1600–5.
https://doi.org/10.1093/gerona/glz296
|
| [18] |
Fedecostante M, Dell’Aquila G, Eusebi P, Volpato S, Zuliani G, Abete P, et al. Predictors of Functional Changes in Italian Nursing Home Residents: The U. L. I. S. S. E. Study. Journal of the American Medical Directors Association [Internet]. 2016 Apr [cited 2026 Apr 7]; 17(4): 306–11.
https://doi.org/10.1016/j.jamda.2015.11.004
|
| [19] |
Hakimjavadi R, Yin CY, Scott M, Talarico R, Ramsay T, Webber C, et al. Cognitive and Functional Decline Among Long-Term Care Residents. JAMA network open [Internet]. 2025 Jan; 8(4): e255635.
https://doi.org/10.1001/jamanetworkopen.2025.5635
|
| [20] |
Arora G, Milani C, Tanuseputro P, Tang P, Jeong A, Kobewka D, et al. Identifying predictors of cognitive decline in long-term care: a scoping review. BMC Geriatrics. 2023 Sep 5; 23(1).
https://doi.org/10.1186/s12877-023-04193-6
|
| [21] |
Ripley S, Alizadehsaravi N, Affoo R, Hunter S, Middleton LE, Moody E, et al. Resident-, family-, and staff-identified goals for rehabilitation of long-term care residents with dementia: a qualitative study. BMC Geriatrics. 2024 Jan 29; 24(1).
https://doi.org/10.1186/s12877-024-04674-2
|
| [22] |
Webber C, Milani C, Pugliese M, Lawlor PG, Bush SH, Watt C, et al. Long‐term cognitive impairment after probable delirium in long‐term care residents: A population‐based retrospective cohort study. Journal of the American Geriatrics Society. 2023 Nov 19; 72(4): 1183–90.
https://doi.org/10.1111/jgs.18675
|
| [23] |
Dasdelen MF, Dasdelen ZB, Almas F, Cokkececi B, Laguna P, de la Rosette J, et al. Exploring the Association Between Urinary Incontinence and Depression Based on a Series of Large-Scale National Health Studies in Türkiye. Journal of Clinical Medicine [Internet]. 2025 Jul 23 [cited 2026 Feb 9]; 14(15): 5213.
https://doi.org/10.3390/jcm14155213
|
| [24] |
Bakhsh A, Alnazawi H, Alsehli O, Almuzaini M, Aloufi H, Alahmadi A, et al. The burden of urinary incontinence and its association with knowledge, practices, and comorbidities among women in Madinah, Saudi Arabia: a cross-sectional study. Frontiers in Medicine. 2026 Jan 12; 12.
https://doi.org/10.3389/fmed.2025.1726741
|
| [25] |
Niarchou E, Roberts L, Naughton BD. What is the impact of antidepressant side effects on medication adherence among adult patients diagnosed with depressive disorder: A systematic review. Journal of Psychopharmacology. 2024 Feb 1; 38(2): 127–36.
https://doi.org/10.1177/02698811231224171
|
| [26] |
Dyer AH, Fallon A, Noonan C, Dolphin H, O’Farrelly C, Bourke NM, et al. Managing the Impact of COVID-19 in Nursing Homes and Long-Term Care Facilities: An Update. Journal of the American Medical Directors Association [Internet]. 2022 Sep 1; 23(9): 1590–602.
https://doi.org/10.1016/j.jamda.2022.06.028
|
| [27] |
Shaheen N, Shaheen A, Ramadan A, Hefnawy MT, Ramadan A, Ibrahim I, et al. Appraising Systematic reviews: a Comprehensive Guide to Ensuring Validity and Reliability. Frontiers in Research Metrics and Analytics. 2023 Dec 21; 8(8).
https://doi.org/10.3389/frma.2023.1268045
|
| [28] |
Matino D, Chai-Adisaksopha C, Iorio A. Systematic reviews of prognosis studies: a critical appraisal of five core clinical journals. Diagnostic and Prognostic Research. 2017 Mar 16; 1(1).
https://doi.org/10.1186/s41512-017-0008-z
|
| [29] |
Liebzeit D, King B, Bratzke L. Measurement of function in older adults transitioning from hospital to home: an integrative review. Geriatric Nursing. 2018 May; 39(3): 336–43.
https://doi.org/10.1016/j.gerinurse.2017.11.003
|
| [30] |
Randles R, Finnegan A. Guidelines for Writing a Systematic Review. Nurse Education Today [Internet]. 2023 Mar 1; 125(125): 105803–3.
https://doi.org/10.1016/j.nedt.2023.105803
|
| [31] |
Ghosh A, Choudhury S. Understanding different types of review articles: A primer for early career researchers. Indian Journal of Psychiatry [Internet]. 2025 May 1; 67(5): 535–41.
https://doi.org/10.4103/indianjpsychiatry.indianjpsychiatry_373_25
|
| [32] |
Rodríguez‐Violante M, Hernández‐Medrano AJ, Cervantes‐Arriaga A. The Importance of Standardized Assessment. Movement Disorders Clinical Practice. 2024 May 26; 11(S3).
https://doi.org/10.1002/mdc3.14085
|
Cite This Article
-
APA Style
Kihali, E., Afriyie, T. (2026). Prognostic Factors Associated with Functional Decline Among Long-Term Care Residents: A Systematic Review. International Journal of Gerontology and Geriatrics, 1(1), 25-34. https://doi.org/10.11648/j.ijgege.20260101.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Kihali, E.; Afriyie, T. Prognostic Factors Associated with Functional Decline Among Long-Term Care Residents: A Systematic Review. Int. J. Gerontol. Geriatr. 2026, 1(1), 25-34. doi: 10.11648/j.ijgege.20260101.13
Copy
|
Download
AMA Style
Kihali E, Afriyie T. Prognostic Factors Associated with Functional Decline Among Long-Term Care Residents: A Systematic Review. Int J Gerontol Geriatr. 2026;1(1):25-34. doi: 10.11648/j.ijgege.20260101.13
Copy
|
Download
-
@article{10.11648/j.ijgege.20260101.13,
author = {Erastus Kihali and Thomas Afriyie},
title = {Prognostic Factors Associated with Functional Decline Among Long-Term Care Residents: A Systematic Review},
journal = {International Journal of Gerontology and Geriatrics},
volume = {1},
number = {1},
pages = {25-34},
doi = {10.11648/j.ijgege.20260101.13},
url = {https://doi.org/10.11648/j.ijgege.20260101.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijgege.20260101.13},
abstract = {Functional decline is common among LTC patients and is linked to poor outcomes, such as higher levels of dependency, hospitalizations, and death. Early phase after admission into facilities can be considered a crucial time frame when residents might have a rapid deterioration. Nevertheless, there is limited knowledge regarding predictors of early functional decline among LTC patients. Main objective of this research is to systematically identify and synthesize prognostic factors associated with early functional decline among long-term care residents. A systematic review was carried out based on PRISMA guidelines. The search strategy involved the use of electronic databases such as PubMed, Embase, Scopus, Web of Science, and Cochrane Library. Studies involving predictors of functional impairment among nursing home residents were included in the review. Extraction and assessment of study data were done using standardized instruments. Heterogeneity across studies led to a narrative synthesis. A total of seven studies with more than 400,000 LTC facility residents were considered. Functional decline was mainly measured using ADL-based measures. Cognitive impairment and preexisting functional state proved to be the most robust and significant predictors of functional decline. Other risk factors like urinary incontinence, co-morbidities, and impaired balance were found to increase the risk. Depression and medication usage showed inconclusive evidence. Geriatrician presence at facilities and disruption at the systems level, like the coronavirus pandemic, decreased and increased functional decline, respectively. The occurrence of functional decline in LTC facilities is complex and results from the interaction between vulnerability and the environment. Early detection of at-risk patients through a thorough assessment can help implement appropriate strategies. There is a need for more studies to validate outcome criteria and modifiable predictors.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Prognostic Factors Associated with Functional Decline Among Long-Term Care Residents: A Systematic Review
AU - Erastus Kihali
AU - Thomas Afriyie
Y1 - 2026/05/11
PY - 2026
N1 - https://doi.org/10.11648/j.ijgege.20260101.13
DO - 10.11648/j.ijgege.20260101.13
T2 - International Journal of Gerontology and Geriatrics
JF - International Journal of Gerontology and Geriatrics
JO - International Journal of Gerontology and Geriatrics
SP - 25
EP - 34
PB - Science Publishing Group
UR - https://doi.org/10.11648/j.ijgege.20260101.13
AB - Functional decline is common among LTC patients and is linked to poor outcomes, such as higher levels of dependency, hospitalizations, and death. Early phase after admission into facilities can be considered a crucial time frame when residents might have a rapid deterioration. Nevertheless, there is limited knowledge regarding predictors of early functional decline among LTC patients. Main objective of this research is to systematically identify and synthesize prognostic factors associated with early functional decline among long-term care residents. A systematic review was carried out based on PRISMA guidelines. The search strategy involved the use of electronic databases such as PubMed, Embase, Scopus, Web of Science, and Cochrane Library. Studies involving predictors of functional impairment among nursing home residents were included in the review. Extraction and assessment of study data were done using standardized instruments. Heterogeneity across studies led to a narrative synthesis. A total of seven studies with more than 400,000 LTC facility residents were considered. Functional decline was mainly measured using ADL-based measures. Cognitive impairment and preexisting functional state proved to be the most robust and significant predictors of functional decline. Other risk factors like urinary incontinence, co-morbidities, and impaired balance were found to increase the risk. Depression and medication usage showed inconclusive evidence. Geriatrician presence at facilities and disruption at the systems level, like the coronavirus pandemic, decreased and increased functional decline, respectively. The occurrence of functional decline in LTC facilities is complex and results from the interaction between vulnerability and the environment. Early detection of at-risk patients through a thorough assessment can help implement appropriate strategies. There is a need for more studies to validate outcome criteria and modifiable predictors.
VL - 1
IS - 1
ER -
Copy
|
Download