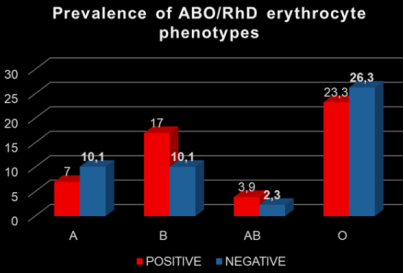
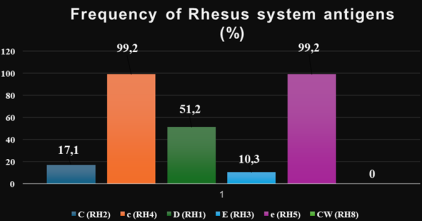
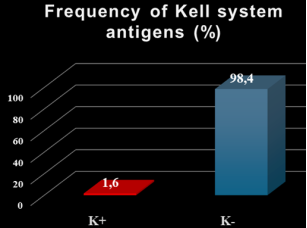
The objective of this study was to catalogue clinically significant antigens of the Rh and Kell blood group systems among regular donors at the Regional Blood Transfusion Center (RBTC) of Bouaké. A total of 129 donors were included. ABO, Rh, and Kell typing were performed on samples collected from these donors using both slide and gel card methods. Among the donors, 120 (93.02%) were male and 9 (6.98%) female, aged between 19 and 58 years, with a mean age of 32.75 ± 7.9 years. The distribution of ABO phenotypes was as follows: O (49.6%, n = 64), A (17.1%, n = 22), B (27.1%, n = 35), and AB (6.2%, n = 8). Regarding the Rhesus (Rh) system, out of the 120 donors typed, 66 (51.2%) were RhD positive and 63 (48.8%) RhD negative. The most prevalent Rh antigens were c and e, each present in 99.2% of donors, followed by D (51.2%), C (17.1%), and E (10.3%). The observed Rh phenotypes were predominantly: ddccee (37.2%), Dccee (35.7%), ddCcee (11.6%), DccEe (8.5%), DCcee (4.6%), DccEE (1.6%), and DCCee (0.8%). The frequency of the Kell antigen (K) among these donors was 1.6%. The associated erythrocyte phenotypes were mainly O- cc dd ee K+ and O+ cc D Ee K+. The establishment of this erythrocyte phenotype database represents a valuable tool to enhance transfusion safety and reduce the risk of post-transfusion complications.
| Published in | International Journal of Immunology (Volume 14, Issue 1) |
| DOI | 10.11648/j.iji.20261401.12 |
| Page(s) | 10-16 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Phenotype, ABO, Rh, Kell, Blood Donor
Number of blood donations | Rh D- n (%) | Rh D+ n (%) | Total n (%) |
|---|---|---|---|
= 1 | 3 (2.33) | 12 (9.30) | 15 (11.63) |
[2-3] | 20 (15.5) | 27 (20.93) | 47 (36.43) |
[4-8] | 40 (31) | 27 (20.93) | 67 (51.94) |
Total | 63 (48.8) | 66 (51.2) | 129 (100) |
Age (Years) | Sex | Total n (%) | |
|---|---|---|---|
Male n (%) | Feminine n (%) | ||
[19-25] | 27 (20.93) | 4 (3.10) | 31 (24.03) |
[25-35] | 46 (35.66) | 2 (1.55) | 48 (37.21) |
[35-45] | 36 (27.91) | 1(0.77) | 37 (28.68) |
[45-55] | 10 (7.75) | 1(0.77) | 11 (8.53) |
[55-65] | 1 (0.77) | 1(0.77) | 2 (1.55) |
ABO RH | A | B | AB | O |
|---|---|---|---|---|
C | 1.6 | 4.7 | 1.6 | 9.3 |
c | 17.1 | 27.1 | 6.2 | 48.8 |
D | 7 | 17.1 | 3.9 | 23.3 |
E | 0.8 | 3.1 | 2.3 | 3.9 |
e | 17.1 | 26.4 | 5.4 | 49.6 |
CW | 0 | 0 | 0 | 0 |
K+ | 0 | 0 | 0 | 1.6 |
Phenotype | Frequency (%) |
|---|---|
DCCee | 0.8 |
DCcee | 4.6 |
Dccee | 35.7 |
DccEE | 1.6 |
DccEe | 8.5 |
ddCcee | 11.6 |
ddccee | 37.2 |
Phenotype | Blood groups | Total | |||
|---|---|---|---|---|---|
A n (%) | B n (%) | AB n (%) | O n (%) | ||
CC D ee K- | 0 | 0 | 0 | 1 (0.77) | 1 (0.77) |
Cc D ee K- | 0 | 3 (2.32) | 1 (0.77) | 2 (1.55) | 6 (4.65) |
cc D ee K- | 8 (6.20) | 15 (11.63) | 1 (0.77) | 22 (17.05) | 46 (35.66) |
cc D EE K- | 0 | 1 (0.77) | 1 (0.77) | 0 | 2 (1.55) |
cc D Ee K- | 1 (0.77) | 3 (2.32) | 2 (1.55) | 4 (3.10) | 10 (7.75) |
cc D Ee K+ | 0 | 0 | 0 | 1 (0.77) | 1 (0.77) |
cc dd ee K+ | 0 | 0 | 0 | 1 (0.77) | 1 (0.77) |
Cc dd ee K- | 2 (1.55) | 3 (2.32) | 1 (0.77) | 9 (6.98) | 15 (11.63) |
cc dd ee K- | 11 (8.53) | 10 (7.75) | 2 (1.55) | 24 (18.60) | 47 (36.43) |
Total | 22 (17.05) | 35 (27.13) | 8 (6.20) | 64 (49.61) | 129 (100) |
RBTC | Regional Blood Transfusion Center |
Rh | Rhesus |
HIV | Human Immunodeficiency Virus |
EDTA | Ethylenediaminetetraacetic Acid |
| [1] | Booth C., Allard S., Robinson S. Blood transfusion. Medecine. 2025, 25(4), 246-252. |
| [2] | Hyland A. C., Castilho L., Chen Q., Clausen B. F., Denomme A. G., Fichou Y., Flegel A. W., Floch A., Gleadall S. N., Hellberg A., Ji Y., Karamatic V. É., Keller M. A., Lane J. W., Lighthart C. P., Lomas-Francis C., Lopez H. G., Montemayor C., Nogués N., Ochoa G., Olsson L. M., Peyrard T., Srivastava K., Storry R. J., Tani Y., Thornton N., van der Schoot E., Végétarienne S., Veldhuisen B., Wagner F. F., Weinstock C., Wendel S., Westhoff M. C., Yahalom V., Gassner C. International Society of Blood Transfusion Working Party on Red Cell Immunogenetics and Blood Group Terminology Report of Gothenburg, Barcelona and four virtual business meetings: Update on blood group systems. Vox Sang. 2026, 121(2), 202-212. |
| [3] | International Society of Blood Transfusion. Working Party for Red Cell Immunogenetics and Blood Group Terminology. |
| [4] | Cartron, J. P. and Agre, P. Rh Blood Group Antigens: Protein and Gene Structure. Seminars in Hematology., (1993), 30, 193-208. |
| [5] | Kathryn E., Webert James W., Smith Donald M. Red Cell, Platelet, and White Cell Antigens Wintrobeâs Clinical Hematology. (12th edtn.). Lippincott Williams & Wilkins, (2009) 22: 631-638. |
| [6] | Kulkarni S., Choudhary B., Harita Gogri H., Jayashree Sharma J., Madkaikar M. Red cell antigen phenotypes in blood donors & thalassaemia patients for creation of red cell antigen-matched inventory. Indian J Med Res. (2020), 152(3), 273-9. |
| [7] | Yonli Y. D., Nébié K., Yacouba S., Kiba A., Sawadogo S., Sawadogo S. M., Traore Y. Alloimmunisation in polytransfused patients with non-phenotyped red blood cells at the University Hospital Souro Sanou of Bobo Dioulasso (Burkina Faso). Pan Afr Med J. 2022, 24(41), 244. |
| [8] | Daniels G., Poole J., de Silva M. Callaghan T., MacLennan S., Smith N. The clinical significance of blood group antibodies. Transfusion Med. (2002) 12, 287-295. |
| [9] | Sood R., Makroo R. N., Riana V., Rosamma N. L. Detection of alloimmunization to ensure safer transfusion practice. Asian J Transfus Sci. 2013, 2(2), 135–9. |
| [10] | Kangiwa U., Ibegbulam O., Ocheni S., Madu A., Mohammed N. Pattern and prevalence of alloimmunization in multiply transfused patients with sickle cell disease in Nigeria. Biomark Res. 2015, 3, 26 |
| [11] | Chao Y. H., Wu K. H., Lu J. J., Shih M. C., Peng C. T., Chang C. W. Red blood cell alloimmunization among Chinese patients with β-thalassaemia major in Taiwan. Blood Transfus. 2013, 11, 71-74 |
| [12] | Guelsin G. A., Rodrigues C., Visentainer J. E., De Melo Campos P., Traina F., Gilli S. C. O., Saad O. T. S., Castilho L. Molecular matching for Rh and K reduces red blood cell alloimmunization in patients with myelodisplastic syndrome. Blood Transfus. 2015, 13, 53-58. |
| [13] | Chou S. T., Liem R. I., Thompson A. A. Challenges of alloimmunization in patients with haemoglobinopathies. Br J Haematol. (2012) 159(4), 394-404. |
| [14] | Klein H. G., Anstee D. J. Mollison’s Blood Transfusion in Clinical Medicine. (2005) 11th edn. Oxford: Blackwell Science. |
| [15] | Pachaury R., Arya D. R., Lai Mahawar N., Bharti A., Kumar Das P. Frequency of Rh Phenotypes in voluntary Blood Donors. JMSCR (2017), 05(07), 25083-8. |
| [16] | Loua, A., Lamah, M. R., Haba, N. Y. and Camara, M. Frequency of Blood Groups ABO and Rhesus D in the Guinean Population. Transfusion Clinique et Biologique., (2007), 14, 435-439. |
| [17] | Randriamanantany Z. A., Rajaonatahina D. H., Razafimanantsoa F. E., Rasamindrakotroka M. T., Andriamahenina R., Rasoarilalamanarivo F. B. Hanitriniala S. P., Herisoa F. R., Rasamindrakotroka A., Rakoto Alson O. A. Phenotypic and Allelic Profile of ABO and Rhesus D Blood Group System among Blood Donor in Antananarivo. International Journal of Immunogenetics (2012), 39, 477-479. |
| [18] | Chandra, T. and Gupta, A. Frequency of ABO and Rhesus Blood Groups in Blood Donors. Asian Journal of Transfusion Science. (2012) 6, 52-53. |
| [19] | Apecu, R. O., Mulogo, E. M., Bagenda, F. and Byamungu, A. ABO and Rhesus (D) Blood Group Distribution among Blood Donors in Rural South-Western Uganda: A Retrospective Study. BMC Research Notes. (2016), 9, 513. |
| [20] | Tesfaye, K., Petros, Y. and Andargie, M. Frequency Distribution of ABO and Rh (D) Blood Group Alleles in Silte Zone, Ethiopia. Egyptian Journal of Medical Human Genetics.,(2015) 16, (1), 71-76. |
| [21] | Ndoula, S. T., Noubiap, J. J. N., Nansseu, J. R. N. and Wonkam, A. Phenotypic and Allelic Distribution of the ABO and Rhesus (D) Blood Groups in the Cameroonian Population. International Journal of Immunogenetics. (2014), 41, 206-210. |
| [22] | Said, N., Ben Ahmed, F., Doghri, A., Ghazouani, E., Layouni, S., Gritli, N. The ABO System Polymorphism in Tunisian Blood. Transfusion Clinique et Biologique. 2003, 10, 331-334. |
| [23] | Bukasa H. K., Kabobo I. K., Tchoni S. M., Mposhi D. N., Nsomue G. K., Tshinkobo C. K., Kabiswe J. P., Ebondo P. K. Frequency of Erythrocyte Phenotypes in Blood Group Systems ABO and Rhesus at Moba, Province of Tanganyika, Democratic Republic of Congo. Library Journal. 2017, 4, e3421. |
| [24] | Ristovska E., Bojadjieva Т. M., Velkova Е., Dimceva А. H., Todorovski B., Tashkovska M., Rastvorceva R. G. & Bosevski M. Rare blood groups in ABO, Rh, kell systems –biological and clinical significance. Sec. of Med. Sci. 2022, 2, 1857-9345. |
| [25] | Bogui L. S., Dembele B., Sekongo Y., Abisse S., Konaté S., & Sombo M. Phenotypic Profile of Rh and Kell Blood Group Systems among Blood Donors in Cote d’Ivoire, West Africa. Journal of Blood Transfusion, 2014, 309817 |
| [26] | Shahata W. M., Khalil H. B., Abass A-E., Adam I., Hussien S. M. Blood group and Rhesus antigens among blood donors attending central blood bank in Sudan. Sudan JMS. (2012), 7(4), 245–8. |
| [27] | Dipankar Baruah, Gitali Devi, Jabin Musfique, Abhijit Bharali, Umesh Chandra Dutta. Distribution and frequency of principal Rh blood group antigens (D, C, c, E, and e) and their phenotypes in the blood donors attending blood bank in a tertiary care hospital in Barpeta district of Assam. Asian J Transfus Sci. 2022, 16(2), 167-174. |
| [28] | Daniels G. Human Blood Groups. Second ed. Blackwell Science. (2002) 295-324. |
| [29] | Dean L. Blood Groups and Red Cell Antigens. National Center for Biotechnology Information (US). (2005) Chapter 7 and Chapter 10. |
| [30] | Harmening Denise M. Modern blood banking and transfusion practices. 5th ed. Philadelphia: FA Davis Company. (2005) p. 163-90. |
| [31] | Garg N, Singh DK, Tomar R, Singh B. Phenotype Prevalence of Blood Group Systems (ABO, Rh, Kell) in Voluntary, Healthy Donors-Experience of a Tertiary Care Hospital in Delhi, North India. J Blood Disord Transfus. (2015), 6, 297. |
| [32] | Kahar M. A. & Patel R. D. Phenotype frequencies of blood group systems (Rh, Kell, Kidd, Duffy, MNS, P, Lewis, and Lutheran) in blood donors of south Gujarat, India. Asian J Transfus Sci. (2014), 8(1), 51–55. |
| [33] | Reid M. E., Lomas-Francis C. The Blood Group Antigen Facts Book. Second ed. New York: Elsevier Academic Press. (2004). |
| [34] | Makroo R. N., Bahtia A., Gupta R., Philip J. Prevalence of Rh, Duffy, Kell, Kidd & MNSs blood group antigens in the Indian blood donor population. Indian J Med Res. (2013), 137(3), 521–526. |
APA Style
N’gou, M. E. R. E., Kouame, K. E., Nenelou, N. F., Siransy, L., Kabore, S., et al. (2026). Erythrocyte Phenotype Profiling in Repeat Blood Donors: A Cross-sectional Study in the Gbêkê Region, Côte d’Ivoire. International Journal of Immunology, 14(1), 10-16. https://doi.org/10.11648/j.iji.20261401.12
ACS Style
N’gou, M. E. R. E.; Kouame, K. E.; Nenelou, N. F.; Siransy, L.; Kabore, S., et al. Erythrocyte Phenotype Profiling in Repeat Blood Donors: A Cross-sectional Study in the Gbêkê Region, Côte d’Ivoire. Int. J. Immunol. 2026, 14(1), 10-16. doi: 10.11648/j.iji.20261401.12
@article{10.11648/j.iji.20261401.12,
author = {M’boh Epi Reine Elisabeth N’gou and Konan Eugène Kouame and Natacha Fleur Nenelou and Liliane Siransy and Saydou Kabore and Bamory Dembele and Mamadou Yassongui Sekongo},
title = {Erythrocyte Phenotype Profiling in Repeat Blood Donors:
A Cross-sectional Study in the Gbêkê Region, Côte d’Ivoire},
journal = {International Journal of Immunology},
volume = {14},
number = {1},
pages = {10-16},
doi = {10.11648/j.iji.20261401.12},
url = {https://doi.org/10.11648/j.iji.20261401.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.iji.20261401.12},
abstract = {The objective of this study was to catalogue clinically significant antigens of the Rh and Kell blood group systems among regular donors at the Regional Blood Transfusion Center (RBTC) of Bouaké. A total of 129 donors were included. ABO, Rh, and Kell typing were performed on samples collected from these donors using both slide and gel card methods. Among the donors, 120 (93.02%) were male and 9 (6.98%) female, aged between 19 and 58 years, with a mean age of 32.75 ± 7.9 years. The distribution of ABO phenotypes was as follows: O (49.6%, n = 64), A (17.1%, n = 22), B (27.1%, n = 35), and AB (6.2%, n = 8). Regarding the Rhesus (Rh) system, out of the 120 donors typed, 66 (51.2%) were RhD positive and 63 (48.8%) RhD negative. The most prevalent Rh antigens were c and e, each present in 99.2% of donors, followed by D (51.2%), C (17.1%), and E (10.3%). The observed Rh phenotypes were predominantly: ddccee (37.2%), Dccee (35.7%), ddCcee (11.6%), DccEe (8.5%), DCcee (4.6%), DccEE (1.6%), and DCCee (0.8%). The frequency of the Kell antigen (K) among these donors was 1.6%. The associated erythrocyte phenotypes were mainly O- cc dd ee K+ and O+ cc D Ee K+. The establishment of this erythrocyte phenotype database represents a valuable tool to enhance transfusion safety and reduce the risk of post-transfusion complications.},
year = {2026}
}
TY - JOUR T1 - Erythrocyte Phenotype Profiling in Repeat Blood Donors: A Cross-sectional Study in the Gbêkê Region, Côte d’Ivoire AU - M’boh Epi Reine Elisabeth N’gou AU - Konan Eugène Kouame AU - Natacha Fleur Nenelou AU - Liliane Siransy AU - Saydou Kabore AU - Bamory Dembele AU - Mamadou Yassongui Sekongo Y1 - 2026/02/26 PY - 2026 N1 - https://doi.org/10.11648/j.iji.20261401.12 DO - 10.11648/j.iji.20261401.12 T2 - International Journal of Immunology JF - International Journal of Immunology JO - International Journal of Immunology SP - 10 EP - 16 PB - Science Publishing Group SN - 2329-1753 UR - https://doi.org/10.11648/j.iji.20261401.12 AB - The objective of this study was to catalogue clinically significant antigens of the Rh and Kell blood group systems among regular donors at the Regional Blood Transfusion Center (RBTC) of Bouaké. A total of 129 donors were included. ABO, Rh, and Kell typing were performed on samples collected from these donors using both slide and gel card methods. Among the donors, 120 (93.02%) were male and 9 (6.98%) female, aged between 19 and 58 years, with a mean age of 32.75 ± 7.9 years. The distribution of ABO phenotypes was as follows: O (49.6%, n = 64), A (17.1%, n = 22), B (27.1%, n = 35), and AB (6.2%, n = 8). Regarding the Rhesus (Rh) system, out of the 120 donors typed, 66 (51.2%) were RhD positive and 63 (48.8%) RhD negative. The most prevalent Rh antigens were c and e, each present in 99.2% of donors, followed by D (51.2%), C (17.1%), and E (10.3%). The observed Rh phenotypes were predominantly: ddccee (37.2%), Dccee (35.7%), ddCcee (11.6%), DccEe (8.5%), DCcee (4.6%), DccEE (1.6%), and DCCee (0.8%). The frequency of the Kell antigen (K) among these donors was 1.6%. The associated erythrocyte phenotypes were mainly O- cc dd ee K+ and O+ cc D Ee K+. The establishment of this erythrocyte phenotype database represents a valuable tool to enhance transfusion safety and reduce the risk of post-transfusion complications. VL - 14 IS - 1 ER -
National Blood Transfusion Center, Abidjan, Côte d’Ivoire
National Blood Transfusion Center, Abidjan, Côte d’Ivoire;Faculty of Medicine and Biomedical Sciences, Félix Houphouët-Boigny University (UFHB), Abidjan, Côte d’Ivoire
National Blood Transfusion Center, Abidjan, Côte d’Ivoire
National Blood Transfusion Center, Abidjan, Côte d’Ivoire;Faculty of Pharmaceutical and Biological Sciences, Félix Houphouët-Boigny-Boigny University (UFHB), Abidjan, Côte d’Ivoire
National Blood Transfusion Center, Abidjan, Côte d’Ivoire
Information