This work aims to develop a logarithmic barrier based interior point method capable of reconstructing CT images using under-sampled sinogram data. Unlike other compressed sensing methods, the proposed method obviates the need of the regularization parameter in the objective function. Feasibility of the algorithm and quality of the reconstructed images were examined. Methods: The sinogram data were simulated through Radon-transforming clinical CT images. The noise was added based on the Poisson and Gaussian models. The basic elements of the proposed method, logarithmic barrier (LB) method, were introduced. The relative Root-Mean-Squared Error (rRMSE) was used to evaluate the image reconstruction accuracy. The noise of the images was assessed using the Peak Signal-to-Noise Ratio (PSNR) and Mean Squared Error (MSE). Results: The PSNR, rRMSE, MSE were compared among fvFBP (full-view Filtered-Backprojection), svFBP (sparse-view Filtered-Backprojection), BB (Barzilai-Borwein), and LB methods for brain, head and neck, lung, prostate, and leg sites. The reconstructed images from svFBP suffered severe streak artifacts. The LB method was capable of reconstructing images of quality comparable to quality of those images obtained from other compressed sensing-based methods such as the BB method. Conclusion: It has been demonstrated that the compressed sensing technique based on the logatirhmic barrier method is capable of recovering satisfactory images from under-sampled projection data. This method obviates the need of the regularization parameter that specifies the relative weight between the data fidelity and total variation terms in the objective function. Insights have been gained as to implementing the proposed method for clinical imaging applications.
| Published in | International Journal of Medical Imaging (Volume 13, Issue 1) |
| DOI | 10.11648/j.ijmi.20251301.12 |
| Page(s) | 7-19 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Compressed Sensing, CT Reconstruction, Interior Point Method, Medical Imaging
Metrics | Sites | Algorithms | |||
|---|---|---|---|---|---|
fvFBP | svFBP | BB | LB | ||
PSNR | Shepp-Logan | 42.73 | 24.69 | 39.12 | 40.24 |
MSE() | 0.5056 | 0.9229 | 0.2841 | 0.1540 | |
rRMSE | 0.1293 | 0.2360 | 0.0726 | 0.0394 | |
PSNR | Brain | 41.699 | 29.57 | 38.377 | 37.553 |
MSE () | 0.4076 | 1.7387 | 0.6429 | 0.7372 | |
rRMSE | 0.0688 | 0.2778 | 0.1008 | 0.1109 | |
PSNR | Neck | 41.5294 | 29.5787 | 38.0411 | 36.3425 |
MSE () | 0.3846 | 1.6631 | 0.6295 | 0.8429 | |
rRMSE | 0.0681 | 0.2698 | 0.1018 | 0.1238 | |
PSNR | Lung | 42.1023 | 29.6927 | 36.2358 | 36.1369 |
MSE () | 0.1165 | 0.4862 | 0.2289 | 0.2315 | |
rRMSE | 0.0353 | 0.1473 | 0.0693 | 0.0701 | |
PSNR | Prostate | 44.2461 | 31.2153 | 37.8093 | 37.012 |
MSE () | 0.1199 | 0.5376 | 0.2516 | 0.2758 | |
rRMSE | 0.0377 | 0.1690 | 0.0791 | 0.0867 | |
PSNR | Leg | 42.8442 | 30.4144 | 37.7135 | 35.551 |
MSE () | 0.2157 | 0.9022 | 0.3894 | 0.4995 | |
rRMSE | 0.0480 | 0.2009 | 0.0867 | 0.1112 | |
CT | Computed Tomography |
LB | Logarithmic Barrier |
rRMSR | Relative Root-Mean Square Error |
PSNR | Peak Signal-to-Noise Ratio |
MSE | Mean Squared Error |
fvFBP | Full-view Filtered Backprojection |
svFBP | Sparse-view Filtered Backprojection |
BB | Barzilai-Borwein |
CBCT | Cone-Beam Computed Tomography |
IGRT | Image Guided Radiation Therapy |
FBP | Filtered Backprojection |
TV | Total Variation |
GPU | Graphics Processing Unit |
GMRES | Generalized Minimal Residual |
| [1] | Liguori C, Frauenfelder G, Massaroni C, Saccomandi P, Giurazza F, Pitocco F, Marano R, Schena E. Emerging clinical applications of computed tomography. Medical Devices: Evidence and Research 2015; 8: 265–78. |
| [2] | Schockel L, Jost G, Seidensticker P, Lengsfeld P, Palkowitsch P, Pietsch H. Developments in X-ray contrast media and the potential impact on computed tomography. Invest Radiol. 2020; 55(9): 592–7. |
| [3] | Gregoire V, Guckenberger M, Haustermans K, Lagendijk JJW, Menard C, Potter R, Slotman BJ, Tanderup K, Thorwarth D, van Herk M, Zips D. Image guidance in radiation therapy for better cure of cancer. Molecular Oncology. 2020; 14(7): 1470–91. |
| [4] | Smith-Bindman R, Lipson J, Marcus R, Kim KP, Mahesh M, Gould R, Berrington de Gonzalez A, Miglioretti DL. Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer. Arch Intern Med. 2009; 169(22): 2078–86. |
| [5] | Kak AC, Slaney M. Principles of computerized tomographic imaging. Switzerland: Society for Industrial and Applied Mathematics; 2001. |
| [6] | Feldkamp LA, Davis LC, Kress JW. Practical cone-beam algorithm. J. Opt. Soc. Am. A. 1984; 1(6): 612–9. |
| [7] | Kwon H, Cho J, Oh J, Kim D, Cho J, Kim S, Lee S, Lee J. The adaptive statistical iterative reconstruction-V technique for radiation dose reduction in abdominal CT: comparison with the adaptive statistical iterative reconstruction technique. Br J Radiol. 2015; 88: 20150463. |
| [8] | Ghetti C, Palleri F, Serreli G, Ortenzia O, Ruffini L. Physical characterization of a new CT iterative reconstruction method operating in sinogram space. J Appl Clin Med Phys. 2013; 14(4): 263–71, |
| [9] | Arapakis I, Efstathopoulos E, Tsitsia V, Kordolaimi S, Economopoulos N, Argentos S, Ploussi A, Alexopoulou E. Using “iDose4” iterative reconstruction algorithm in adults’ chest-abdomen-pelvis CT examinations: effect on image quality in relation to patient radiation exposure, Br J Radiol. 2014; 87: 20130613. |
| [10] | Yu L, Liu X, Leng S, Kofler JM, Ramirez-Giraldo JC, Qu M, Christner J, Fletcher JG, McCollough CH. Radiation dose reduction in computed tomography: techniques and future perspective. Imaging Med. 2009; 1(1): 65–84, |
| [11] | Smith EA, Dillman JR, Goodsitt MM, Christodoulou EG, Keshavarzi N, Strouse P. Model-based iterative reconstruction: effect on patient radiation dose and image quality in pediatric body CT. Radiology. 2014; 270(2): 526–34. |
| [12] | Liu L. Model-based iterative reconstruction: a promising algorithm for today’s computed tomography imaging. Journal of Medical Imaging and Radiation Sciences. 2014, 45: 131-6. |
| [13] | Lu H, Li X, Hsiao IT, Liang Z. Analytical noise treatment for low-dose CT projection data by penalized weighted least-square smoothing in the K-L domain. Proceedings of SPIE, Medical Imaging 2002: Physics of Medical Imaging. 2002; 4682: 146-52. |
| [14] | Wang J, Li T, Lu H, Liang Z. Penalized weighted least-squares approach to sinogram noise reduction and image reconstruction for low-dose X-ray computed tomography. IEEE Trans Med Imaging. 2006; 25(10): 1272–83. |
| [15] | La Riviere PJ, Bian J, Vargas PA. Penalized-likelihood sonogram restoration for computed tomography. IEEE Trans Med Imaging. 2006; 25: 1022-36. |
| [16] | Zhu L, Wang J, Xing L. Noise suppression in scatter correction for cone-beam CT. Med Phys. 2009; 36(3): 741-52. |
| [17] | Candes EJ, Romberg J, Tao T. Stable signal recovery from incomplete and inaccurate measurements. Communications on Pure and Applied Mathematics. 2006; 59(8): 1207-23. |
| [18] | Candes EJ, Romberg J, Tao T. Robust uncertainty principles: exact signal reconstruction from highly incomplete frequency information. IEEE Transactions on Information Theory. 2006; 52(2): 489-509. |
| [19] | Sidky EY, Pan X, Image reconstruction in circular cone-beam computed tomography by constrained, total-variation minimization. Phys. Med. Biol. 2008; (53): 4777-807. |
| [20] | Chen GH, Tang J, Leng S. Prior image constrained compressed sensing (PICCS). Proc SPIE Int Soc Opt Eng. 2008; 6856: 685618. |
| [21] | Choi K, Fahimian BP, Li T, Suh TS, Xing L. Enhancement of four-dimensional cone-beam computed tomography by compressed sensing with Bregman iteration. J X-ray Sci Technol. 2013; 21(2): 177-92. |
| [22] | Lauzier PT, Tang J, Chen GH. Time-resolved cardiac interventional cone-beam CT reconstruction from fully truncated projections using the prior image constrained compressed sensing (PICCS) algorithm. Phys. Med. Biol. 2012; 57: 2461-76. |
| [23] | Ramirez-Giraldo JC, Trzasko J, Leng S, Yu L, Manduca A, McCollough CH. Nonconvex prior image constrained compressed sensing (NCPICCS): Theory and simulations on perfusion CT. Med Phys. 2011; 38(4) 2157–67. |
| [24] | Ma J, Zhang H, Gao Y, Huang J, Liang Z, Feng Q, Chen W. Iterative image reconstruction for cerebral perfusion CT using pre-contrast scan induced edge-preserving prior. Phys. Med. Biol. 2012; 57(22); 7519-42. |
| [25] | Hu Z, Zheng H. Improved total variation minimization method for few-view computed tomography image reconstruction. Biomedical Engineering Online. 2014; 13: 70. |
| [26] | Huang J, Zhang Y, Ma J, Zeng D, Bian Z, Niu S, Feng Q, Liang Z, Chen W. Iterative image reconstruction for sparse-view CT using normal-dose image induced total variation prior. PLoS ONE. 2013; 8(11): e79709. |
| [27] | Zhang H, Ouyang L, Huang J, Ma J, Chen W, Wang J. Few-view cone-beam CT reconstruction with deformed prior image. Med Phys. 2014; 41(12): 121905, |
| [28] | Donoho DL. Compressed sensing. IEEE Transactions on Information Theory. 2006; 52(4): 1289-306. |
| [29] | Candes EJ, Wakin MB. An introduction to compressive sensing. IEEE Signal Processing Magazine. 2008; 25(2): 21-30. |
| [30] | Kim H, Chen J, Wang A, Chuang C, Held M, Pouliot J. Non-local total-variation (NLTV) minimization combined with reweighted L1-norm for compressed sensing CT reconstruction. Phys. Med. Biol. 2016; 61: 6878-91. |
| [31] | Zhu L, Niu T, Petrongolo M. Iterative CT reconstruction via minimizing adaptively reweighted total variation. Journal of X-Ray Science and Technology. 2014; 22: 227-40. |
| [32] | Xu Q, Yang D, Tan J, Sawatzky A, Anastasio MA. Accelerated fast iterative shrinkage thresholding algorithms for sparsity-regularized cone-beam CT image reconstruction. Med. Phys. 2016; 43(4): 1849-72. |
| [33] | Choi K, Wang J, Zhu L, Suh TS, Boyd S, Xing L. Compressed sensing based cone-beam computed tomography reconstruction with a first-order method. Med. Phys. 2010; 37(9): 5113-25, |
| [34] | Sun T, Sun N, Wang J, Tan S. Iterative CBCT reconstruction using Hessian penalty. Phys. Med. Biol. 2015; 60: 1965-87. |
| [35] | Park JC, Song B, Kim JS, Park SH, Kim HK, Liu Z, Suh TS, Song WY. Fast compressed sensing-based CBCT reconstruction using Barzilai-Borwein formulation for application to on-line IGRT. Med. Phys. 2012; 39(3): 1207-17. |
| [36] | Niu T, Zhu L. Accelerated barrier optimization compressed sensing (ABOCS) reconstruction for cone-beam CT: Phantom studies. Med. Phys. 2012; 39970; 4588-98. |
| [37] | Niu T, Ye X, Fruhauf Q, Petrongolo M, Zhu L. Accelerated barrier optimization compressed sensing (ABOCS) for CT reconstruction with improved convergence. Phys. Med. Biol. 2014; 59: 1801-14. |
| [38] | Wieczorek M, Frikel J, Vogel J, Eggl E, Kopp F, Noel PB, Pfeiffer F, Demaret L, Lasser T. X-ray computed tomography using curvelet sparse regularization. Med. Phys. 2015; 42(4): 1555-65. |
| [39] | Xu Q, Yu H, Mou X, Zhang L, Hsieh J, Wang G. Low-dose X-ray CT reconstruction via dictionary learning. IEEE Trans Med Imaging. 2012; 31(9): 1682-97. |
| [40] | Bai J, Liu Y, Yang H. Sparse-view CT reconstruction based on a hybrid domain model with multi-level wavelet transform. Sensors. 2022; 22(9): 3228. |
| [41] | Jia X, Dong B, Lou Y, Jiang S. GPU-based iterative cone-beam CT reconstruction using tight frame regularization. Phys. Med. Biol. 2011; 56(13): 3787-807. |
| [42] | Lohvithee M, Sun W, Chretien S, Soleimani M. Ant colony-based hyperparameter optimisation in total variation reconstruction in X-ray computed tomography. Sensors. 2021; 21: 591. |
| [43] | Adler J, Oktem O. Learned primal-dual reconstruction. IEEE Transactions on Medical Imaging. 2018; 37(6): 1322-32. |
| [44] | Baguer DO, Leuschner J, Schmidt M. Computed tomography reconstruction using deep image prior and learned reconstruction methods. Inverse Problems. 2020; 36: 094004. |
| [45] | Jin KH, McCann MT, Froustey E, Unser M. Deep convolutional neural network for inverse problems in imaging. IEEE Transactions on Image Processing. 2017; 26(9): 4509-22. |
| [46] | Xu H, Sun Q, Luo N, Cao G, Xia D. Iterative nonlocal total variation regularization method for image restoration. PLoS ONE. 2013; 8(6): e65865. |
| [47] | Kamilov U. A parallel proximal algorithm for anisotropic total variation minimization. IEEE Transactions on Image Processing. 2017; 26(2): 539-48. |
| [48] | Xu J, Noo F. Patient-specific hyperparameter learning for optimization-based CT image reconstruction. Phys. Med. Biol. 2021; 66: 19NT01. |
| [49] | Shen C, Gonzalez Y, Chen L, Jiang SB, Jia X. Intelligent parameter tuning in optimization-based iterative CT reconstruction via deep reinforcement learning. IEEE Transactions on Medical Imaging. 2018; 37(6): 1430-9. |
| [50] | Xu H. SU-E-I-45, Reconstruction of CT images from sparsely sampled data using logarithmic barrier method. Med. Phys. 2014; 41(6). |
| [51] | La Riviere PJ, Billmire DM. Reduction of noise induced streak artifacts in x ray CT through spline based penalized likelihood sinogram smoothing. IEEE Transactions on Medical Imaging. 2005; 24(1): 105-11. |
| [52] | Boyd S, Vandenberghe L. Convex Optimization, Cambridge University Press; 2004. |
| [53] | Barzilai J, Borwein JM. Two-point step size gradient methods. IMA Journal of Numerical Analysis. 1998; 8: 141-8. |
| [54] | He K, Tan SXD, Zhao H, Liu XX, Wang H, Shi G. Parallel GMRES solver for fast analysis of large linear dynamic systems on GPU platforms. INTEGRATION, the VLSI journal. 2016; 52: 10-22. |
APA Style
Xu, H. (2025). Sparse-view CT Image Reconstruction Using the Logarithmic Barrier Based Interior Point Method. International Journal of Medical Imaging, 13(1), 7-19. https://doi.org/10.11648/j.ijmi.20251301.12
ACS Style
Xu, H. Sparse-view CT Image Reconstruction Using the Logarithmic Barrier Based Interior Point Method. Int. J. Med. Imaging 2025, 13(1), 7-19. doi: 10.11648/j.ijmi.20251301.12
@article{10.11648/j.ijmi.20251301.12,
author = {Heping Xu},
title = {Sparse-view CT Image Reconstruction Using the Logarithmic Barrier Based Interior Point Method
},
journal = {International Journal of Medical Imaging},
volume = {13},
number = {1},
pages = {7-19},
doi = {10.11648/j.ijmi.20251301.12},
url = {https://doi.org/10.11648/j.ijmi.20251301.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmi.20251301.12},
abstract = {This work aims to develop a logarithmic barrier based interior point method capable of reconstructing CT images using under-sampled sinogram data. Unlike other compressed sensing methods, the proposed method obviates the need of the regularization parameter in the objective function. Feasibility of the algorithm and quality of the reconstructed images were examined. Methods: The sinogram data were simulated through Radon-transforming clinical CT images. The noise was added based on the Poisson and Gaussian models. The basic elements of the proposed method, logarithmic barrier (LB) method, were introduced. The relative Root-Mean-Squared Error (rRMSE) was used to evaluate the image reconstruction accuracy. The noise of the images was assessed using the Peak Signal-to-Noise Ratio (PSNR) and Mean Squared Error (MSE). Results: The PSNR, rRMSE, MSE were compared among fvFBP (full-view Filtered-Backprojection), svFBP (sparse-view Filtered-Backprojection), BB (Barzilai-Borwein), and LB methods for brain, head and neck, lung, prostate, and leg sites. The reconstructed images from svFBP suffered severe streak artifacts. The LB method was capable of reconstructing images of quality comparable to quality of those images obtained from other compressed sensing-based methods such as the BB method. Conclusion: It has been demonstrated that the compressed sensing technique based on the logatirhmic barrier method is capable of recovering satisfactory images from under-sampled projection data. This method obviates the need of the regularization parameter that specifies the relative weight between the data fidelity and total variation terms in the objective function. Insights have been gained as to implementing the proposed method for clinical imaging applications.
},
year = {2025}
}
TY - JOUR T1 - Sparse-view CT Image Reconstruction Using the Logarithmic Barrier Based Interior Point Method AU - Heping Xu Y1 - 2025/02/20 PY - 2025 N1 - https://doi.org/10.11648/j.ijmi.20251301.12 DO - 10.11648/j.ijmi.20251301.12 T2 - International Journal of Medical Imaging JF - International Journal of Medical Imaging JO - International Journal of Medical Imaging SP - 7 EP - 19 PB - Science Publishing Group SN - 2330-832X UR - https://doi.org/10.11648/j.ijmi.20251301.12 AB - This work aims to develop a logarithmic barrier based interior point method capable of reconstructing CT images using under-sampled sinogram data. Unlike other compressed sensing methods, the proposed method obviates the need of the regularization parameter in the objective function. Feasibility of the algorithm and quality of the reconstructed images were examined. Methods: The sinogram data were simulated through Radon-transforming clinical CT images. The noise was added based on the Poisson and Gaussian models. The basic elements of the proposed method, logarithmic barrier (LB) method, were introduced. The relative Root-Mean-Squared Error (rRMSE) was used to evaluate the image reconstruction accuracy. The noise of the images was assessed using the Peak Signal-to-Noise Ratio (PSNR) and Mean Squared Error (MSE). Results: The PSNR, rRMSE, MSE were compared among fvFBP (full-view Filtered-Backprojection), svFBP (sparse-view Filtered-Backprojection), BB (Barzilai-Borwein), and LB methods for brain, head and neck, lung, prostate, and leg sites. The reconstructed images from svFBP suffered severe streak artifacts. The LB method was capable of reconstructing images of quality comparable to quality of those images obtained from other compressed sensing-based methods such as the BB method. Conclusion: It has been demonstrated that the compressed sensing technique based on the logatirhmic barrier method is capable of recovering satisfactory images from under-sampled projection data. This method obviates the need of the regularization parameter that specifies the relative weight between the data fidelity and total variation terms in the objective function. Insights have been gained as to implementing the proposed method for clinical imaging applications. VL - 13 IS - 1 ER -
Department of Radiation Oncology, Indiana University, Indianapolis, USA
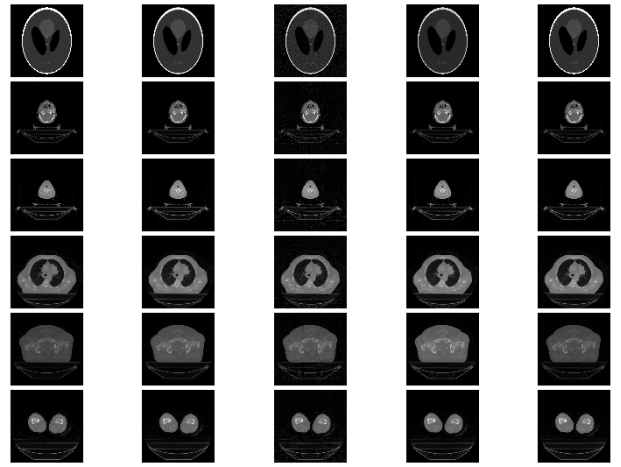
Figure 1. The image reconstruction results from noiseless projection data for Shepp-Logan phantom (1st row), brain image (2nd row), head-and-neck image (3rd row), lung image (4th row), prostate image (5th row), and leg image (6th row). The first column shows the ground truth images. The second column shows the result from the full-view FBP (937 projections). The third column shows the result from the sparse-view FBP (67 projections). The fourth column shows the result from the Barzilai-Borwein method (67 projections). The fifth row shows the result from the log-barrier based interior point method (67 projections).
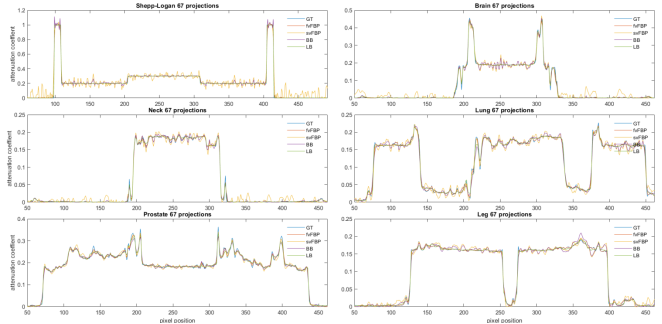
Figure 2. Horizontal profiles through the center of the images (same images in Figure 1). The ground truth and the results from four methods are represented by different colors. (Images are reconstructed from noiseless data of 67 projections except those reconstructed from fvFBP which uses 937 projections).
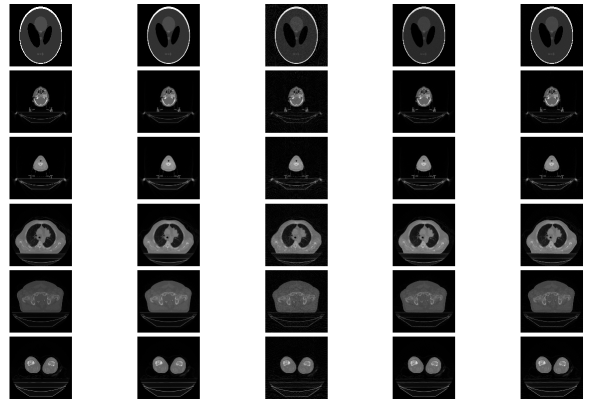
Figure 3. The image reconstruction results from noisy projection data for Shepp-Logan phantom (1st row), brain image (2nd row), head-and-neck image (3rd row), prostate image (4th row), prostate image (5th row), and leg image (6th row). The first column shows the ground truth images. The second column shows the result from the full-view FBP (937 projections). The third column shows the result from the sparse-view FBP (67 projections). The fourth column shows the result from the Barzilai-Borwein method (67 projections). The fifth row shows the result from the log-barrier based interior point method (67 projections).
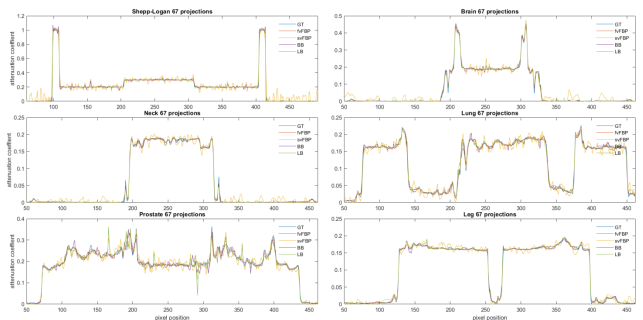
Figure 4. Horizontal profiles through the center of the images (same images in Figure 3). The ground truth and the results from four methods are represented by different colors. (Images are reconstructed from noisy data of 67 projections except those reconstructed from fvFBP which uses 937 projections).
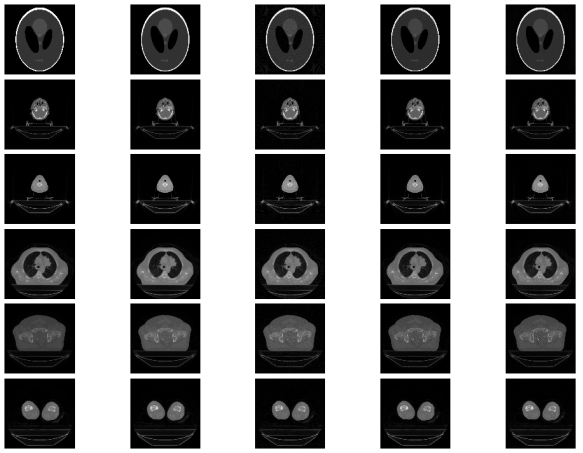
Figure 5. The image reconstruction results from noisy projection data for Shepp-Logan phantom (1st row), brain image (2nd row), head-and-neck image (3rd row), prostate image (4th row), prostate image (5th row), and leg image (6th row). The first column shows the ground truth images. The second column shows the result from the full-view FBP (937 projections). The third column shows the result from the sparse-view FBP (137 projections). The fourth column shows the result from the Barzilai-Borwein method (137 projections). The fifth row shows the result from the log-barrier based interior point method (137 projections).
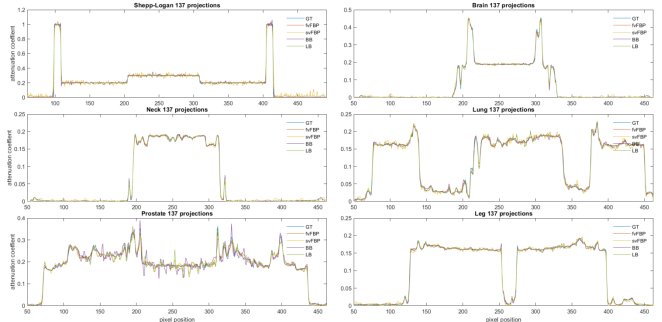
Figure 6. Horizontal profiles through the center of the images (same images in Figure 5). The ground truth and the results from four methods are represented by different colors. (Images are reconstructed from noisy data of 137 projections except those reconstructed from fvFBP which uses 937 projections).
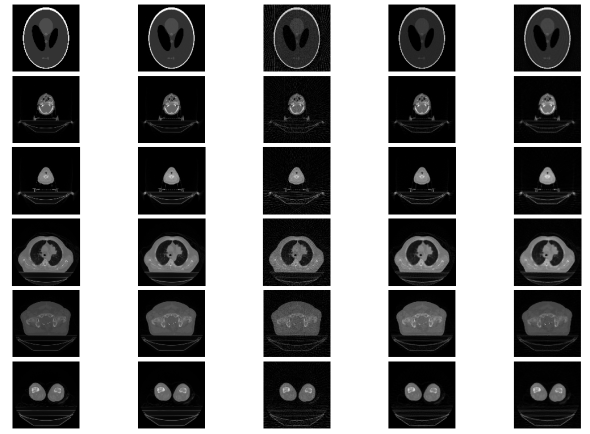
Figure 7. The image reconstruction results from noisy projection data for Shepp-Logan phantom (1st row), brain image (2nd row), head-and-neck image (3rd row), prostate image (4th row), prostate image (5th row), and leg image (6th row). The first column shows the ground truth images. The second column shows the result from the full-view FBP (937 views). The third column shows the result from the sparse-view FBP (47 projections). The fourth column shows the result from the Barzilai-Borwein method (47 projections). The fifth row shows the result from the log-barrier based interior point method (47 projections).
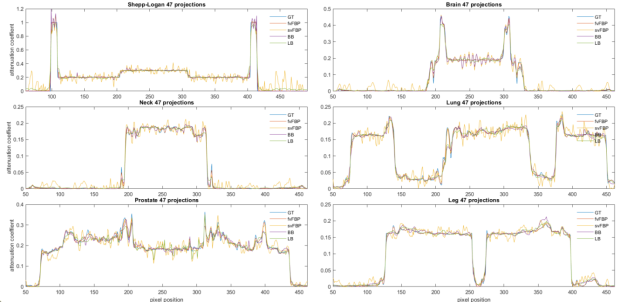
Figure 8. Horizontal profiles through the middle of the images (same images in Figure 7). The ground truth and the results from four methods are represented by different colors. (Images are reconstructed from noisy data of 47 projections except those reconstructed from fvFBP which uses 937 projections).
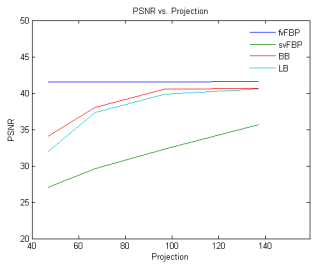
Figure 9. Comparison of PSNR of the images reconstructed from svFBP, BB, and LB against that of the images reconstructed from fvFBP as a function of the number of noisy data projections for head and neck site.
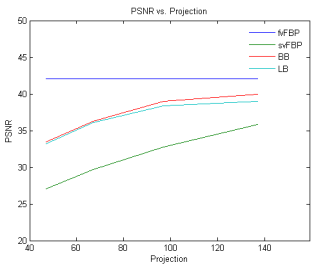
Figure 10. Comparison of PSNR of the images reconstructed from svFBP, BB, and LB against that of the images reconstructed from fvFBP as a function of the number of noisy data projections for lung site.
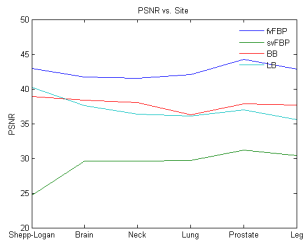
Figure 11. Comparison of PSNR of the images reconstructed from svFBP, BB, and LB against that of the images reconstructed from fvFBP as a function of various sites. The number of the noisy data projections used for image reconstruction is 67.
Information

