Objective: Describe the clinical and therapeutic aspects of septic lateral sinus thrombosis through a case in children. Clinical case: O.C 15 years old, male, shepherd, with history of CME of around 5 years, received urgently for headache, dizziness, vomiting and a notion of fever with purulent and fetid otorrhea on the left associated with otalgia and hypoacusis. Our physical examination found a fever of 39.5°C; neck tightness with pain along the left sternocleidomastoid muscle. Otoscopic examination revealed purulent and fetid otorrhea on the left with a scaly deposit. After aspiration we visualized a subtotal and marginal tympanic perforation with a moist base. The right ear is unremarkable. CT scan showed the Delta sign [Figure 1] as well as associated thromboses of the internal jugular vein [Figure 3] and the transverse sinus [Figure 2]. The treatment consisted of a left masto-atticotomy [Figure 4] with skeletonization of the lateral sinus as well as filling with abdominal fat, a cartilaginous tympanoplasty and 2 months of antibiotic therapy. We did not use anticoagulants. The evolution was marked by the regression of local and general signs without complications or after-effects. Conclusion: lateral sinus thrombosis is a serious complication of otitis media, especially in children, but rare. Its diagnosis is often delayed, hence the importance of emergency imaging in the face of suggestive signs. Early treatment is a prognostic guarantee to reduce morbidity and mortality.
| Published in | International Journal of Otorhinolaryngology (Volume 11, Issue 2) |
| DOI | 10.11648/j.ijo.20251102.16 |
| Page(s) | 32-36 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Lateral Sinus ,Thrombosis, Children, Computed Tomography, Skeletonization
Author/year | Clinique | Paraclinique | Traitement | Evolution |
|---|---|---|---|---|
FI koné /2013 | -Temporal headache with cervical irradiation -Foul otorrhea, EAC polyp, subtotal marginal tympanic perforation -Seizure -Alteration of consciousness -Meningeal syndrome | Anemia 5.1 g/dl Hyperleukocytosis High CRP 10 mg/l CT: delta sign | -Hospitalization/ Resuscitation -Tri-Antibiotherapy (cef, metro, cipro) -Atticomastoidectomy, posterosuperior tympanotomy without action on the thrombosed sinus | -No recurrence in 6 months of control -No after-effects |
Baddouh/2019 | -Convulsive seizures -Diffuse and/or focal neurological signs | HTIC signs -CT: Delta sign, parenchymal lesion (hemorrhagic softening) -MRI if possible | - Antibiotics -Anticoagulant Mastoidectomy without skeletonization | Aftereffects (optic atrophy, paralysis of the VI, epilepsy -Death |
Boumedil/2020 | -Acute febrile convulsion -Convulsive status epilepticus | HTIC signs -Lethargy -Behavioral disorder -Anemia -Thrombocytosis CT/MRI/ CT angiography: thalamic parenchymal lesions, delta sign | Hospitalization -Anticoagulant -Antiepileptic -Antibiotics Mastoidectomy -Sequelae (optic atrophy, epilepsy) -CIVD -Death | Sequelae (optic atrophy, epilepsy) -CIVD -Death |
Meherzi/2022 | -Headache, fever, ear pain -Eye signs Otorrhea, perforated eardrum | -Anémie Hyperleucocytose CT/MRI: Delta sign | Antibiotherapy Anticoagulant Antro-mastoidectomy with skeletonization | No after-effects, No recurrence |
CT | Computer Tomography |
CIVD | Disseminated Intravascular Coagulation |
HTIC | Intracranial Hypertension |
MRI | Magnetic Resonance Imaging |
| [1] | N Baddouh, S Elbakri, G Draiss, Y Mouaffak, N Rada, S Younous, M Bouskraoui Cerebral venous thrombosis in children: about a series of 12 cases. PanAfrican Medical Journal. 2019; 32: 22. |
| [2] | Raja K, Parida PK, Alexender A, Surianarayanan G. Otogenic lateral sinus Thrombis: A review of Fifteen patients and changing trends in the management Int. Arch. Otolaryngol. 2018; 22 (3): 208-213. |
| [3] | Abir M, Amal G, Mouna B, et al. Clinical characteristics of otogenic cerebral sinovenous thrombosis: Our experience and review of literature. Clin Case Rep. 2022; 10: e06475. |
| [4] | M. Lezreg, M. chenguir, R. Abada, S. Rouadi, M. Mahtar. Lateral sinus thrombosis of otogenic origin in children: report of 3 cases. French Annal of Otorhinolaryngology and Cerico-facial Pathology. Volume 131, issue, October 201, Page A163. |
| [5] | M. François. Complications of acute and chronic otitis media. EMC Otolaryngology 2005; 20-135-A-10 |
| [6] | Mustafa A, Tiçi B, Thaçi H, Gjikolli B, Baftiu N. Acute Mastoidis complicated with concomitant Bezold’s Abscess and Lateral Sinus Thrombis. 2018 Mar 20; 2018: 8702532. |
| [7] | D Boumendil, D Batouche, D Batouche, A Sellam. Cerebral Venous Thrombosis in children: about a series hospitalized in Pediatric Intensive Care. GSJ 2020; 8(6): 1492-1510. |
| [8] | FI Kone, SK Timbo, K Singaré, S Dao, S Soumaoro, B Guindo, M Keïta, A G Mohamed Thrombophlebitis of the lateral sinus: A lethal pathology. The African journal of ENT and head and neck surgery 2013; 13(1, 2, 3): 55-59. |
APA Style
Camara, N., Issa, K. F., Samaké, H., Neuilly, N. T., Alima, T., et al. (2025). Lateral Sinus Thrombosis in a Children. International Journal of Otorhinolaryngology, 11(2), 32-36. https://doi.org/10.11648/j.ijo.20251102.16
ACS Style
Camara, N.; Issa, K. F.; Samaké, H.; Neuilly, N. T.; Alima, T., et al. Lateral Sinus Thrombosis in a Children. Int. J. Otorhinolaryngol. 2025, 11(2), 32-36. doi: 10.11648/j.ijo.20251102.16
@article{10.11648/j.ijo.20251102.16,
author = {Nagnouma Camara and Koné Fatogoma Issa and Hélène Samaké and Ngniée Tafo Neuilly and Tarata Alima and Dicko Ibrahim and Ganaba Abdoulaye Modibo and Touré Tata and Nouhoum Traoré and Barry Sadou and Konaté Drissa and Konaté Oumar and Samaké Djibril and Bakayoko Drissa Kaloga and Mariam Sangaré and Koïta Mamadou and Samba Karim Timbo and Keita Mohamed Amadou},
title = {Lateral Sinus Thrombosis in a Children
},
journal = {International Journal of Otorhinolaryngology},
volume = {11},
number = {2},
pages = {32-36},
doi = {10.11648/j.ijo.20251102.16},
url = {https://doi.org/10.11648/j.ijo.20251102.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijo.20251102.16},
abstract = {Objective: Describe the clinical and therapeutic aspects of septic lateral sinus thrombosis through a case in children. Clinical case: O.C 15 years old, male, shepherd, with history of CME of around 5 years, received urgently for headache, dizziness, vomiting and a notion of fever with purulent and fetid otorrhea on the left associated with otalgia and hypoacusis. Our physical examination found a fever of 39.5°C; neck tightness with pain along the left sternocleidomastoid muscle. Otoscopic examination revealed purulent and fetid otorrhea on the left with a scaly deposit. After aspiration we visualized a subtotal and marginal tympanic perforation with a moist base. The right ear is unremarkable. CT scan showed the Delta sign [Figure 1] as well as associated thromboses of the internal jugular vein [Figure 3] and the transverse sinus [Figure 2]. The treatment consisted of a left masto-atticotomy [Figure 4] with skeletonization of the lateral sinus as well as filling with abdominal fat, a cartilaginous tympanoplasty and 2 months of antibiotic therapy. We did not use anticoagulants. The evolution was marked by the regression of local and general signs without complications or after-effects. Conclusion: lateral sinus thrombosis is a serious complication of otitis media, especially in children, but rare. Its diagnosis is often delayed, hence the importance of emergency imaging in the face of suggestive signs. Early treatment is a prognostic guarantee to reduce morbidity and mortality.
},
year = {2025}
}
TY - JOUR T1 - Lateral Sinus Thrombosis in a Children AU - Nagnouma Camara AU - Koné Fatogoma Issa AU - Hélène Samaké AU - Ngniée Tafo Neuilly AU - Tarata Alima AU - Dicko Ibrahim AU - Ganaba Abdoulaye Modibo AU - Touré Tata AU - Nouhoum Traoré AU - Barry Sadou AU - Konaté Drissa AU - Konaté Oumar AU - Samaké Djibril AU - Bakayoko Drissa Kaloga AU - Mariam Sangaré AU - Koïta Mamadou AU - Samba Karim Timbo AU - Keita Mohamed Amadou Y1 - 2025/09/23 PY - 2025 N1 - https://doi.org/10.11648/j.ijo.20251102.16 DO - 10.11648/j.ijo.20251102.16 T2 - International Journal of Otorhinolaryngology JF - International Journal of Otorhinolaryngology JO - International Journal of Otorhinolaryngology SP - 32 EP - 36 PB - Science Publishing Group SN - 2472-2413 UR - https://doi.org/10.11648/j.ijo.20251102.16 AB - Objective: Describe the clinical and therapeutic aspects of septic lateral sinus thrombosis through a case in children. Clinical case: O.C 15 years old, male, shepherd, with history of CME of around 5 years, received urgently for headache, dizziness, vomiting and a notion of fever with purulent and fetid otorrhea on the left associated with otalgia and hypoacusis. Our physical examination found a fever of 39.5°C; neck tightness with pain along the left sternocleidomastoid muscle. Otoscopic examination revealed purulent and fetid otorrhea on the left with a scaly deposit. After aspiration we visualized a subtotal and marginal tympanic perforation with a moist base. The right ear is unremarkable. CT scan showed the Delta sign [Figure 1] as well as associated thromboses of the internal jugular vein [Figure 3] and the transverse sinus [Figure 2]. The treatment consisted of a left masto-atticotomy [Figure 4] with skeletonization of the lateral sinus as well as filling with abdominal fat, a cartilaginous tympanoplasty and 2 months of antibiotic therapy. We did not use anticoagulants. The evolution was marked by the regression of local and general signs without complications or after-effects. Conclusion: lateral sinus thrombosis is a serious complication of otitis media, especially in children, but rare. Its diagnosis is often delayed, hence the importance of emergency imaging in the face of suggestive signs. Early treatment is a prognostic guarantee to reduce morbidity and mortality. VL - 11 IS - 2 ER -
Commune III Reference Health Center, Bamako, Mali
Gabriel Touré University Hospital Center, Bamako, Mali
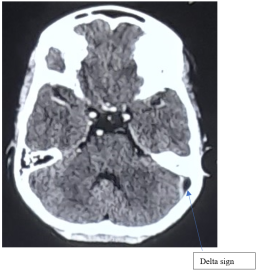
Figure 1. Axial CT brain section (filling of the mastoid cells with absence of contrast enhancement of the thrombosed lateral sinus: Delta sign).
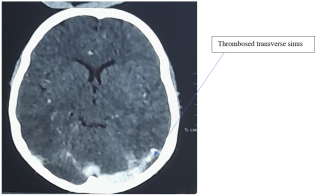
Figure 2. Axial CT brain section: transverse sinus thrombosis.
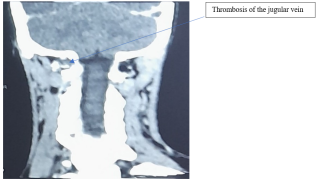
Figure 3. Frontal cervical CT showing thrombosis of the jugular vein.
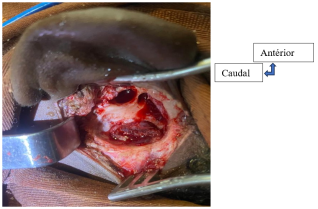
Figure 4. Surgical field: skeletonization of the thrombosed lateral sinus (Masto-atticotomy G with skeletonization of the lateral sinus, Cartilaginous tympanoplasty, Filling with abdominal fat).
Information

