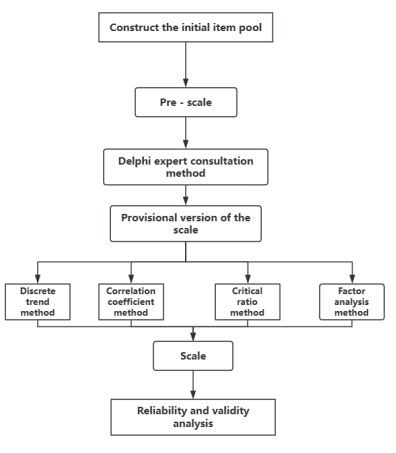
This study aimed to develop and preliminarily validate a Chinese assessment scale for zoster-associated pain (ZAP) based on the Delphi method. A descriptive study was conducted. An initial item pool was developed based on domestic and international guidelines, expert consensus, and professional discussions related to ZAP. The Delphi method was employed in September 2023 to screen and revise the items, forming a preliminary version of the scale. From October 5, 2023, to January 31, 2024, a total of 209 patients with ZAP treated at the Department of Pain Management, The First Affiliated Hospital of Zhejiang University School of Medicine, were surveyed using this scale. Items were excluded using several criteria: standard deviation < 0.7 or coefficient of variation < 0.15 (dispersion trend method), correlation coefficient < 0.2 or non-significant differences (P > 0.05) (correlation analysis), non-significant differences (P > 0.05) (critical ratio method), and factor loadings < 0.4 or cross-loadings > 0.4 on multiple factors (exploratory factor analysis). Reliability was evaluated using internal consistency (Cronbach’s α), and validity was assessed through content and construct validity. Two rounds of Delphi expert consultation were conducted, involving 15 clinical pain specialists. A preliminary 16-item scale was developed based on threshold screening criteria. The response rate for both Delphi rounds was 100%, and the authority coefficients of experts were all > 0.7. Cronbach's α coefficients were 0.847 and 0.909 for the first and second rounds, respectively. Kendall’s W coefficients were 0.259 (χ² = 108.814, P < 0.001) and 0.291 (χ² = 74.130, P < 0.001) across the two rounds. Following item analysis of the 209 patient responses, 15 items were retained. The content validity of the scale was judged to be satisfactory by pain specialists. After further validity testing, 11 items were finally retained. The Kaiser-Meyer-Olkin (KMO) value was 0.837, and Bartlett’s test of sphericity was significant (P < 0.001). Exploratory factor analysis extracted three common factors, accounting for a cumulative variance contribution of 64.791%. The final Cronbach’s α coefficient was 0.808. The developed Chinese version of the ZAP assessment scale consists of 11 items across three dimensions, demonstrating good reliability, validity, and applicability.
| Published in | International Journal of Pain Research (Volume 2, Issue 1) |
| DOI | 10.11648/j.ijpr.20260201.11 |
| Page(s) | 1-14 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Herpes Zoster, Zoster-associated Pain, Delphi Method, Scale Development, Items, Reliability, Validity
Familiarity Level | Score |
|---|---|
Extremely Familiar | 1.00 |
Familiar | 0.75 |
Somewhat Familiar | 0.50 |
Not Familiar | 0.25 |
Judgement Basis | Impact Factor | Large |
|---|---|---|
Practical Experience | 0.5 | Large |
Theoretical Analysis | 0.3 | Medium |
Domestic and International Literature | 0.1 | Small |
Item | Number (%) |
|---|---|
Gender | |
Male | 9 (60%) |
Female | 6 (40%) |
Age (years) | |
40 ~ 50 | 2 (13.3%) |
>50 ~ 60 | 13 (86.7%) |
Position | |
Associate Senior | 1 (6.7%) |
Senior | 14 (93.3%) |
Education | |
Bachelor's Degree | 2 (13.3%) |
Master's Degree | 6 (40.0%) |
Doctorate | 7 (56.7%) |
Years of Work Experience (years) | |
10 ~ 15 | 1 (6.7%) |
>15 ~ 20 | 1 (6.7%) |
>20 | 13 (86.7%) |
Region | |
Secondary Cities | 12 (80.0%) |
Tertiary Cities | 2 (13.3%) |
Cities and Below | (6.7%) |
Round 1 | Round 2 | ||||||
|---|---|---|---|---|---|---|---|
No. | Item | Importance Score (M±SD) | Full Score Ratio | CV | Importance Score (M±SD) | Full Score Ratio | CV |
1 | Pain distribution location | 4.67±0.60 | 0.73 | 0.13 | 4.73±0.57 | 0.80 | 0.12 |
2 | Area of skin lesions/pigmentation | 4.13±0.81 | 0.40 | 0.19 | 3.80±0.75 | 0.20 | 0.20 |
3 | Depth of pain location | 3.87±1.09 | 0.33 | 0.28 | 4.13±0.96 | 0.47 | 0.23 |
4 | Nature of pain | 4.53±0.88 | 0.73 | 0.20 | 4.47±0.88 | 0.67 | 0.20 |
5 | Pain attack pattern | 4.13±0.88 | 0.40 | 0.21 | 4.07±1.00 | 0.40 | 0.25 |
6 | Verbal pain intensity rating | 4.73±0.44 | 0.73 | 0.09 | 4.67±0.70 | 0.80 | 0.15 |
7 | VAS pain intensity rating | 4.26±0.85 | 0.47 | 0.20 | — | — | — |
8 | NRS pain intensity rating | 4.73±0.44 | 0.73 | 0.09 | 4.80±0.54 | 0.87 | 0.11 |
9 | Current pain level | 3.73±1.00 | 0.27 | 0.27 | 4.00±0.63 | 0.20 | 0.16 |
10 | 24-hour pain level | 4.20±0.75 | 0.40 | 0.18 | — | — | — |
11 | 72-hour pain level | 4.27±0.77 | 0.47 | 0.18 | — | — | — |
12 | Peak pain level | 4.13±0.96 | 0.47 | 0.23 | 4.60±0.61 | 0.67 | 0.13 |
13 | Average pain level | 3.93±0.85 | 0.27 | 0.22 | 4.20±0.75 | 0.40 | 0.18 |
14 | Pain duration | 4.27±0.77 | 0.47 | 0.18 | 4.33±0.70 | 0.47 | 0.16 |
15 | Breakthrough pain frequency/hour | 4.33±0.94 | 0.60 | 0.22 | 4.73±0.57 | 0.80 | 0.12 |
16 | Weather-induced pain exacerbation | 3.07±0.85 | 0.07 | 0.28 | — | — | — |
17 | Touch-evoked pain | 4.67±0.47 | 0.67 | 0.10 | 4.53±0.62 | 0.60 | 0.14 |
18 | Lesion area numbness | 3.80±0.98 | 0.27 | 0.26 | 3.47±1.02 | 0.20 | 0.30 |
19 | Lesion area itching | 3.67±1.25 | 0.33 | 0.34 | — | — | — |
20 | Muscle weakness/abdominal distension | 3.47±1.15 | 0.20 | 0.33 | — | — | — |
21 | Life/work impact | 4.40±0.61 | 0.47 | 0.14 | 4.73±0.57 | 0.80 | 0.12 |
22 | Mobility impact | 3.67±0.94 | 0.13 | 0.26 | — | — | — |
23 | Sleep impact | 4.80±0.40 | 0.80 | 0.08 | 4.80±0.54 | 0.87 | 0.11 |
24 | Anxiety impact | 4.33±0.79 | 0.53 | 0.18 | 4.47±0.81 | 0.60 | 0.18 |
25 | Depression impact | 4.33±0.67 | 0.47 | 0.16 | 4.53±0.81 | 0.67 | 0.18 |
26 | Appetite impact | 3.80±0.91 | 0.20 | 0.24 | — | — | — |
27 | Health status score | 3.73±0.85 | 0.20 | 0.23 | — | — | — |
28 | Allodynia test | 4.67±0.47 | 0.67 | 0.10 | — | — | — |
29 | Pinprick threshold change | 4.13±0.88 | 0.40 | 0.21 | — | — | — |
Item | Round 1 (M ± SD) | Threshold | Round 2 (M ± SD) | Threshold |
|---|---|---|---|---|
Importance Score | 4.15 ± 0.42 | 3.74 | 4.39 ± 0.37 | 4.03 |
Full Score Ratio | 0.44 ± 0.20 | 0.25 | 0.58 ± 0.22 | 0.36 |
Coefficient of Variation (CV) | 0.20 ± 0.07 | 0.27 | 0.17 ± 0.05 | 0.22 |
No. | Item | Options | Score |
|---|---|---|---|
1 | Primary location of pain in herpes zoster lesions? | None | 0 |
Lower limbs, upper limbs, perineum, other areas | 5 | ||
Head/face, neck, chest/back, waist/abdomen | 10 | ||
2 | Area of herpes zoster lesions/pigmentation (cm²)? | 0 | 0 |
<10 (≈1 palm size) | 2.5 | ||
10–30 | 5.0 | ||
>30–50 | 7.5 | ||
>50 | 10.0 | ||
3 | Depth of herpes zoster-associated pain? | No pain | 0 |
Superficial or deep pain only | 5 | ||
Both superficial and deep pain | 10 | ||
4 | Nature of herpes zoster-associated pain? | Abnormal sensation | 0 |
Other types of pain | 5 | ||
Burning, electric-shock, stabbing, lancinating, tearing pain | 10 | ||
5 | Pattern of herpes zoster-associated pain attacks? | Complete relief after episodes | 0 |
Partial relief after episodes | 3.3 | ||
Persistent pain with mild fluctuations | 6.7 | ||
Persistent pain with acute attacks | 10.0 | ||
6 | Verbal description of pain intensity? | No pain | 0 |
Mild pain | 2 | ||
Uncomfortable | 4 | ||
Distressing | 6 | ||
Horrible | 8 | ||
Excruciating | 10 | ||
7 | Current pain intensity (0–10)? | No pain → Excruciating (as above) | 0–10 |
8 | Peak pain intensity in past 24h (0–10)? | (Same as Item 6) | 0–10 |
9 | Average pain intensity in past 24h (mean of AM/noon/PM scores)? | (Same as Item 6) | 0–10 |
10 | Duration of persistent pain in past 24h (hours)? | 0 | 0 |
>0–3 | 2.5 | ||
>3–7 | 5.0 | ||
>7–12 | 7.5 | ||
>12 | 10.0 | ||
11 | Frequency of breakthrough pain per hour in past 24h? | 0 | 0 |
1–6 | 3.3 | ||
>6–12 | 6.7 | ||
>12 | 10.0 | ||
12 | Does touching the painful area (e.g., with fingers/clothes/bedding/wind/vibration) induce or worsen pain compared to non-painful areas (0–10)? | 0–10 | 0–10 |
13 | Impact of pain on daily activities/work (0–10)? | 0–10 | 0–10 |
14 | Impact of pain on sleep (0–10)? | 0–10 | 0–10 |
15 | Does the pain cause anxiety/worry/irritability (0–10)? | 0–10 | 0–10 |
16 | Does the pain cause depression/feeling life is meaningless (0–10)? | 0–10 | 0–10 |
Disease Name | Gender (n, Male/Female) | Age [years, Median (IQR)] | Height (cm, Mean ± SD) | Weight (kg, Mean ± SD) |
|---|---|---|---|---|
Herpes Zoster | 108/101 | 66.0 (58.5–72.0) | 163 ± 8 | 62 ± 12 |
Item | Mean | SD | CV | Correlation Coefficient | Z-score |
|---|---|---|---|---|---|
1 | 9.35 | 1.68 | 0.18 | 0.099 | -1.138 |
2 | 4.65 | 2.32 | 0.50 | 0.249* | -3.550* |
3 | 7.80 | 2.49 | 0.32 | 0.332* | -4.836* |
4 | 9.62 | 1.50 | 0.16 | 0.266* | -3.298# |
5 | 6.35 | 4.30 | 0.68 | 0.443* | -5.962* |
6 | 5.54 | 2.11 | 0.38 | 0.552* | -6.865* |
7 | 3.84 | 2.02 | 0.53 | 0.712* | -8.319* |
8 | 5.63 | 2.12 | 0.38 | 0.715* | -8.396* |
9 | 4.68 | 1.89 | 0.40 | 0.774* | -8.988* |
10 | 6.87 | 3.20 | 0.47 | 0.482* | -5.897* |
11 | 4.63 | 3.09 | 0.67 | 0.504* | -5.619* |
12 | 4.23 | 2.32 | 0.55 | 0.582* | -6.465* |
13 | 4.93 | 2.65 | 0.54 | 0.779* | -8.956* |
14 | 5.52 | 2.97 | 0.54 | 0.762* | -8.753* |
15 | 3.44 | 2.89 | 0.84 | 0.666* | -7.794* |
16 | 2.80 | 2.72 | 0.97 | 0.613* | -7.089* |
Factor | Initial Eigenvalues | Extraction Sums of Squared Loadings | Rotation Sums of Squared Loadings | ||||||
|---|---|---|---|---|---|---|---|---|---|
Eigen-value | Variance Explained (%) | Cumulative (%) | Eigen-value | Variance Explained (%) | Cumulative (%) | Eigen-value | Variance Explained (%) | Cumulative (%) | |
1 | 4.574 | 41.583 | 41.583 | 4.574 | 41.583 | 41.583 | 4.238 | 38.529 | 38.529 |
2 | 1.476 | 13.414 | 54.998 | 1.476 | 13.414 | 54.998 | 1.611 | 14.643 | 53.173 |
3 | 1.077 | 9.793 | 64.791 | 1.077 | 9.793 | 64.791 | 1.278 | 11.618 | 64.791 |
Item | Factor | ||
|---|---|---|---|
F1 | F2 | F3 | |
15 | 0.827 | - | - |
13 | 0.815 | - | - |
9 | 0.785 | - | - |
16 | 0.780 | - | - |
14 | 0.777 | - | - |
6 | 0.731 | - | - |
7 | 0.690 | - | - |
5 | - | 0.872 | - |
10 | - | 0.833 | - |
4 | - | - | 0.759 |
3 | - | - | 0.750 |
No. | Item | Option | Score |
|---|---|---|---|
1 | Depth of pain | No pain | 0 |
Superficial or deep | 5 | ||
Both exist | 10 | ||
2 | Characteristics of pain | Abnormal sensation | 0 |
Other characteristics | 5 | ||
Burning, lightning, knife-like, prickling-like, tearing | 10 | ||
3 | Pattern of attack | Pain completely relieved after attack | 0 |
Pain partially relieved after attack | 3.3 | ||
Persistent pain with slight fluctuation | 6.7 | ||
Persistent pain with paroxysmal exacerbation | 10 | ||
4 | Verbal description of pain intensity | No pain | 0 |
Mild | 2 | ||
Unbearable | 4 | ||
Agonizing | 6 | ||
Dreadful | 8 | ||
Extremely painful | 10 | ||
5 | The current pain intensity? (Score) | 0-10 | 0-10 |
6 | The average pain intensity in the past 24 h? (h) | 0-10 | 0-10 |
7 | The duration of persistent pain in the past 24 h? (h) | 0 | 0 |
>0-3 | 2.5 | ||
>3-7 | 5 | ||
>7-12 | 7.5 | ||
>12 | 10 | ||
8 | Impact of pain at the herpes site on daily activities or work? (Score) | 0-10 | 0-10 |
9 | Impact of pain at the herpes site on sleep? (Score) | 0-10 | 0-10 |
10 | Whether feeling uneasy, worried, anxious and irritable due to pain at the herpes site? (Score) | 0-10 | 0-10 |
11 | Whether feeling unhappy, depressed, or even hopeless due to pain at the herpes site? (Score) | 0-10 | 0-10 |
ZAP | Zoster-Associated Pain |
KMO | The Kaiser-Meyer-Olkin Value |
PHN | Postherpetic Neuralgia |
VAS | The Visual Analogue Scale |
NRS | The Numerical Rating Scale |
DN4 | The Douleur Neuropathique 4 |
SD | Standard Deviation |
CV | Coefficient of Variation |
EFA | Exploratory Factor Analysis |
CV | Coefficient of Variation |
PCA | Principal Component Analysis |
| [1] | Cohen JI. Clinical practice: Herpes zoster. N Engl J Med. 2013; 369(3): 255-63. |
| [2] | Johnson RW, Rice AS. Clinical practice. Postherpetic neuralgia. N Engl J Med. 2014; 371(16): 1526-33. |
| [3] | Chen LK, Arai H, Chen LY, Chou MY, Djauzi S, Dong B, et al. Looking back to move forward: a twenty-year audit of herpes zoster in Asia-Pacific. BMC Infect Dis. 2017; 17(1): 213. Epub 20170315. |
| [4] | Yang F, Yu S, Fan B, Liu Y, Chen YX, Kudel I, et al. The Epidemiology of Herpes Zoster and Postherpetic Neuralgia in China: Results from a Cross-Sectional Study. Pain Ther. 2019; 8(2): 249-59. Epub 20190619. |
| [5] | Peng Z, Guo J, Zhang Y, Guo X, Huang W, Li Y, et al. Development of a Model for Predicting the Effectiveness of Pulsed Radiofrequency on Zoster-Associated Pain. Pain Ther. 2022; 11(1): 253-67. Epub 20220130. |
| [6] | Sun X, Wei Z, Lin H, Jit M, Li Z, Fu C. Incidence and disease burden of herpes zoster in the population aged ≥50 years in China: Data from an integrated health care network. J Infect. 2021; 82(2): 253-60. Epub 20210106. |
| [7] | Thompson RR, Kong CL, Porco TC, Kim E, Ebert CD, Acharya NR. Herpes Zoster and Postherpetic Neuralgia: Changing Incidence Rates From 1994 to 2018 in the United States. Clin Infect Dis. 2021; 73(9): e3210-e7. |
| [8] | Bricout H, Haugh M, Olatunde O, Prieto RG. Herpes zoster-associated mortality in Europe: a systematic review. BMC Public Health. 2015; 15: 466. Epub 20150505. |
| [9] | Gross GE, Eisert L, Doerr HW, Fickenscher H, Knuf M, Maier P, et al. S2k guidelines for the diagnosis and treatment of herpes zoster and postherpetic neuralgia. J Dtsch Dermatol Ges. 2020; 18(1): 55-78. Epub 20200117. |
| [10] | Wu CY, Lin HC, Chen SF, Chang WP, Wang CH, Tsai JC, et al. Efficacy of Pulsed Radiofrequency in Herpetic Neuralgia: A Meta-Analysis of Randomized Controlled Trials. Clin J Pain. 2020; 36(11): 887-95. |
| [11] | Huang J, Yang S, Yang J, Sun W, Jiang C, Zhou J, et al. Early Treatment with Temporary Spinal Cord Stimulation Effectively Prevents Development of Postherpetic Neuralgia. Pain Physician. 2020; 23(2): E219-e30. |
| [12] | Galer BS, Jensen MP. Development and preliminary validation of a pain measure specific to neuropathic pain: the Neuropathic Pain Scale. Neurology. 1997; 48(2): 332-8. |
| [13] | Portenoy R. Development and testing of a neuropathic pain screening questionnaire: ID Pain. Curr Med Res Opin. 2006; 22(8): 1555-65. |
| [14] | Bouhassira D, Attal N, Alchaar H, Boureau F, Brochet B, Bruxelle J, et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain. 2005; 114(1-2): 29-36. Epub 20050126. |
| [15] | Freynhagen R, Baron R, Gockel U, Tölle TR. painDETECT: a new screening questionnaire to identify neuropathic components in patients with back pain. Curr Med Res Opin. 2006; 22(10): 1911-20. |
| [16] | Melzack R. The McGill Pain Questionnaire: major properties and scoring methods. Pain. 1975; 1(3): 277-99. |
| [17] | Marsden J, Dolan B, Holt L. Nurse practitioner practice and deployment: electronic mail Delphi study. J Adv Nurs. 2003; 43(6): 595-605. |
| [18] | Magnolini R, Senn O, Neuner-Jehle S, Bruggmann P. Best Practice Guidance for Male Individuals Using Anabolic Androgenic Steroids in Recreational Sports Within Primary Care: Protocol for a Modified Delphi Consensus Study. JMIR Res Protoc. 2025; 14: e65233. Epub 20250818. |
| [19] | Kura K, Oba J, Amano S, Takahashi K. Development of Goal-Achievement Support App to Assist Children and Families in Participating in Meaningful Occupations: Content Validation Using Delphi Method. JMIR Rehabil Assist Technol. 2025; 12: e73430. Epub 20250820. |
| [20] | Demangeot Y, O'Neill S, Degache F, Rapin A, Asgher U, Alfredson H, et al. Exercise parameters to consider for Achilles tendinopathy: a modified Delphi study with international experts. Br J Sports Med. 2025. Epub 20250828. |
| [21] | Qin W, Dai X, Huang P, Luo J, Shen Y, Zhu Q. Development of a core competency evaluation index system for specialist nurses in robot-assisted surgery: a Delphi study. BMC Nurs. 2025; 24(1): 1063. Epub 20250812. |
| [22] | McPherson S, Reese C, Wendler MC. Methodology Update: Delphi Studies. Nurs Res. 2018; 67(5): 404-10. |
| [23] | Makhmutov R. The Delphi method at a glance. Pflege. 2021; 34(4): 221. |
| [24] | Giroux CM, Zomahoun HTV, Boies S, Bush P, Alkhaldi M, Kengne Talla P, et al. Assessing healthcare organisations' readiness to implement a learning health system: protocol for questionnaire validation using a Delphi method. BMJ Open. 2025; 15(8): e088720. Epub 20250825. |
| [25] | Li F, Shang J, Li Y, Liu G, Zhao S, Wu J, et al. A new evaluation methodology study - Integrating 'ancient literature - clinical research - expert consensus' firstly proposes eight elements for taking Chinese medicine decoctions. Front Pharmacol. 2025; 16: 1585428. Epub 20250808. |
| [26] | An Y, Xu H, Ma Q, Wang X, Ding Y, Yang R, et al. A study on the construction of a nurse refresher training system in traditional Chinese medicine hospitals using the Delphi method. Front Public Health. 2025; 13: 1618002. Epub 20250723. |
| [27] | Raza S, Saleem F, Alwi S, Haider S, Iqbal Q, Wahid A, et al. Translation and Psychometric Validation of Brief Illness Perception Questionnaire: The Urdu Version for Facilitating Multidisciplinary Research in Pakistan. J Multidiscip Healthc. 2025; 18: 5075-88. Epub 20250820. |
| [28] | Wan X, Yang J, Pan Y. Developing and Validating the Scale of Organizational Support Needs for Nurses Returning to Work After Childbirth. J Nurs Manag. 2025; 2025: 5842526. Epub 20250818. |
| [29] | Ahmed I, Ishtiaq S. Reliability and validity: Importance in Medical Research. J Pak Med Assoc. 2021; 71(10): 2401-6. |
| [30] |
Shaw M, Dent J, Beebe T, Junghard O, Wiklund I, Lind T, et al. The Reflux Disease Questionnaire: a measure for assessment of treatment response in clinical trials. Health Qual Life Outcomes. 2008; 6: 31. Epub 20080430.
HYPERLINK "
https://doi.org/10.1186/1477-7525-6" https://doi.org/10.1186/1477-7525-6-31 |
| [31] | Lin Y, Yu Y, Zeng J, Zhao X, Wan C. Comparing the reliability and validity of the SF-36 and SF-12 in measuring quality of life among adolescents in China: a large sample cross-sectional study. Health Qual Life Outcomes. 2020; 18(1): 360. Epub 20201109. |
APA Style
Siyao, Z., Liu, C., Yifu, L., Yunze, L., Li, Z., et al. (2026). Construction and Preliminary Validation of the Chinese Assessment Scale for Zoster-associated Pain Based on the Delphi Method. International Journal of Pain Research, 2(1), 1-14. https://doi.org/10.11648/j.ijpr.20260201.11
ACS Style
Siyao, Z.; Liu, C.; Yifu, L.; Yunze, L.; Li, Z., et al. Construction and Preliminary Validation of the Chinese Assessment Scale for Zoster-associated Pain Based on the Delphi Method. . 2026, 2(1), 1-14. doi: 10.11648/j.ijpr.20260201.11
@article{10.11648/j.ijpr.20260201.11,
author = {Zheng Siyao and Chengjiang Liu and Liang Yifu and Li Yunze and Zhou Li and Feng Zhiying},
title = {Construction and Preliminary Validation of the Chinese Assessment Scale for Zoster-associated Pain Based on the Delphi Method},
journal = {International Journal of Pain Research},
volume = {2},
number = {1},
pages = {1-14},
doi = {10.11648/j.ijpr.20260201.11},
url = {https://doi.org/10.11648/j.ijpr.20260201.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijpr.20260201.11},
abstract = {This study aimed to develop and preliminarily validate a Chinese assessment scale for zoster-associated pain (ZAP) based on the Delphi method. A descriptive study was conducted. An initial item pool was developed based on domestic and international guidelines, expert consensus, and professional discussions related to ZAP. The Delphi method was employed in September 2023 to screen and revise the items, forming a preliminary version of the scale. From October 5, 2023, to January 31, 2024, a total of 209 patients with ZAP treated at the Department of Pain Management, The First Affiliated Hospital of Zhejiang University School of Medicine, were surveyed using this scale. Items were excluded using several criteria: standard deviation 0.05) (correlation analysis), non-significant differences (P > 0.05) (critical ratio method), and factor loadings 0.4 on multiple factors (exploratory factor analysis). Reliability was evaluated using internal consistency (Cronbach’s α), and validity was assessed through content and construct validity. Two rounds of Delphi expert consultation were conducted, involving 15 clinical pain specialists. A preliminary 16-item scale was developed based on threshold screening criteria. The response rate for both Delphi rounds was 100%, and the authority coefficients of experts were all > 0.7. Cronbach's α coefficients were 0.847 and 0.909 for the first and second rounds, respectively. Kendall’s W coefficients were 0.259 (χ² = 108.814, P < 0.001) and 0.291 (χ² = 74.130, P < 0.001) across the two rounds. Following item analysis of the 209 patient responses, 15 items were retained. The content validity of the scale was judged to be satisfactory by pain specialists. After further validity testing, 11 items were finally retained. The Kaiser-Meyer-Olkin (KMO) value was 0.837, and Bartlett’s test of sphericity was significant (P < 0.001). Exploratory factor analysis extracted three common factors, accounting for a cumulative variance contribution of 64.791%. The final Cronbach’s α coefficient was 0.808. The developed Chinese version of the ZAP assessment scale consists of 11 items across three dimensions, demonstrating good reliability, validity, and applicability.},
year = {2026}
}
TY - JOUR T1 - Construction and Preliminary Validation of the Chinese Assessment Scale for Zoster-associated Pain Based on the Delphi Method AU - Zheng Siyao AU - Chengjiang Liu AU - Liang Yifu AU - Li Yunze AU - Zhou Li AU - Feng Zhiying Y1 - 2026/02/04 PY - 2026 N1 - https://doi.org/10.11648/j.ijpr.20260201.11 DO - 10.11648/j.ijpr.20260201.11 T2 - International Journal of Pain Research JF - International Journal of Pain Research JO - International Journal of Pain Research SP - 1 EP - 14 PB - Science Publishing Group SN - 3070-1562 UR - https://doi.org/10.11648/j.ijpr.20260201.11 AB - This study aimed to develop and preliminarily validate a Chinese assessment scale for zoster-associated pain (ZAP) based on the Delphi method. A descriptive study was conducted. An initial item pool was developed based on domestic and international guidelines, expert consensus, and professional discussions related to ZAP. The Delphi method was employed in September 2023 to screen and revise the items, forming a preliminary version of the scale. From October 5, 2023, to January 31, 2024, a total of 209 patients with ZAP treated at the Department of Pain Management, The First Affiliated Hospital of Zhejiang University School of Medicine, were surveyed using this scale. Items were excluded using several criteria: standard deviation 0.05) (correlation analysis), non-significant differences (P > 0.05) (critical ratio method), and factor loadings 0.4 on multiple factors (exploratory factor analysis). Reliability was evaluated using internal consistency (Cronbach’s α), and validity was assessed through content and construct validity. Two rounds of Delphi expert consultation were conducted, involving 15 clinical pain specialists. A preliminary 16-item scale was developed based on threshold screening criteria. The response rate for both Delphi rounds was 100%, and the authority coefficients of experts were all > 0.7. Cronbach's α coefficients were 0.847 and 0.909 for the first and second rounds, respectively. Kendall’s W coefficients were 0.259 (χ² = 108.814, P < 0.001) and 0.291 (χ² = 74.130, P < 0.001) across the two rounds. Following item analysis of the 209 patient responses, 15 items were retained. The content validity of the scale was judged to be satisfactory by pain specialists. After further validity testing, 11 items were finally retained. The Kaiser-Meyer-Olkin (KMO) value was 0.837, and Bartlett’s test of sphericity was significant (P < 0.001). Exploratory factor analysis extracted three common factors, accounting for a cumulative variance contribution of 64.791%. The final Cronbach’s α coefficient was 0.808. The developed Chinese version of the ZAP assessment scale consists of 11 items across three dimensions, demonstrating good reliability, validity, and applicability. VL - 2 IS - 1 ER -
Department of Painology, The First Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, China
Department of Painology, The First Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, China
Department of Painology, The First Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, China; Department of Anesthesiology, The First Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, China
Department of Painology, The First Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, China
Department of Painology, The First Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, China; Department of Emergency, Ningbo NO. 6 Hospital, Ningbo, China
Department of Painology, The First Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, China
Information