Abstract
Burnout syndrome is a state of emotional, mental, and physical exhaustion resulting from prolonged occupational stress, which is highly prevalent among healthcare professionals. It adversely affects clinical performance, decision-making, and personal well-being. In Sudan, medical doctors face unique stressors, including political instability and extended working hours; however, burnout remains an under-investigated area. This study aims to determine the prevalence of burnout among Sudanese medical doctors, identify its contributing factors, assess its impact on well-being, and explore effective coping mechanisms. A cross-sectional study was conducted using a convenience sample of Sudanese medical doctors. Data collected electronically via standardized questionnaires, capturing demographic information, work-related variables, and burnout symptoms. Data analysis was performed using SPSS to determine burnout prevalence and associated factors. Ethical approval was obtained from Alzaiem Alazhari University. Among the 105 participating doctors, the mean age was 28 years; the majority were female (75.2%) and single (74.3%). Specialists constituted (54.3%) of the sample. Most participants worked 6–12 hours daily, with a significant proportion exceeding 12 hours. While the majority handled fewer than 20 cases per day, a minority reported a high patient load. Key burnout indicators revealed a moderate to high perceived workload (Mean = 10.32, SD = 2.092), low work engagement (Mean = 1.27, SD = 1.085), and a compromised work-life balance (Mean = 5.40, SD = 2.737). The most common physical symptoms were fatigue (62.9%) and headaches (58.1%). Emotional exhaustion (28.6%) and insomnia (22.9%) were also prevalent, while loss of appetite (17.1%), feelings of ineffectiveness (13.3%), and cynicism (3.8%) were reported by smaller but notable proportions. The findings indicate a moderate prevalence of burnout among Sudanese medical doctors, primarily driven by long working hours, high patient loads, and limited engagement in restorative activities. The concurrent pursuit of academic advancement amidst these stressors likely exacerbates emotional exhaustion. This study underscores the urgent need for institutional mental health support, increased awareness, and the implementation of structured coping strategies to mitigate burnout and enhance the overall well-being and professional performance of doctors in Sudan.
Keywords
Prevalence, Burnout, Syndrome, Sudan, Medical Doctors
1. Background
Burnout is recognized by the World Health Organization (WHO) as an occupational phenomenon. Although not classified as a medical condition, it is defined as a syndrome resulting from chronic workplace stress that has not been successfully managed. Burnout is characterized by a state of physical, mental, and emotional exhaustion, leading to feelings of detachment, demotivation, and hopelessness, which significantly impair an individual's ability to function
| [1] | Burnout - Mental Health UK (mentalhealth-uk.org) © Mental Health UK, 28 AlbertEmbankment, London, SE1 7GR. Registered Charity no. 1170815. |
[1]
.
Contributing factors often include long working hours, irregular schedules, a high-stakes and demanding work environment, and insufficient remuneration
| [2] | Gonzales Y, Guevara-Delgado N, Alcahuaman J, Jiménez V, Osorio P. Burnout syndrome and intention to leave: An analysis of its impact through a systematic review 2015–2025. Journal of Ecohumanism. 2025; 4(1): 4370-82. |
[2]
. The syndrome is conceptualized around three core dimensions, namely emotional exhaustion, which involves feelings of being emotionally overextended and depleted; depersonalization, characterized by negative, cynical feelings and detachment from one's job or the people associated with it; and reduced personal accomplishment, which refers to a decline in feelings of competence and achievement at work
| [3] | Treml MF, Sarubbi AV, Madeira ME, Rasoto AW, Schwarzer N. Burnout syndrome in Brazil (2014–2024): regional variations and temporal trends in an epidemiological study. Revista Brasileira de Medicina do Trabalho. 2025 Sep 14; 23(3): e220251479. |
[3]
.
The hospital environment is inherently strenuous, both physically and mentally, placing medical doctors at high risk for burnout. This, in turn, can negatively impact clinical decision-making, patient safety, and the quality of communication with patients and colleagues
| [4] | Symptoms of Burnout Syndrome among Physicians during the Outbreak of COVID-19 Pandemic—A Systematic Literature Review - PMC (nih.gov). |
[4]
. Sudanese medical doctors face significant mental health challenges, exacerbated by the country's political instability. Contributing factors include excessive workloads, difficulties maintaining work-life balance, and personal stressors such as financial burdens and relational pressures
. Furthermore, the evolving dynamics of the medical field itself add another layer of immense pressure.
The prevalence of burnout varies across countries and healthcare settings; for instance, one study reported a prevalence of (59.0%) among doctors in the public sector, associating it with personal factors such as anxiety and depressive symptoms
| [6] | Owuoro, Rosebenter Awuor, et al. Prevalence of burnout among nurses in sub-Saharan Africa: a systematic review. JBI Evidence Synthesis, 2020, 18.6: 1189-1207. |
[6]
. Burnout among healthcare providers is associated with professional and interpersonal conflicts, emotional stress, a demanding work environment, and a lack of social support
| [7] | Dubaled, Benyam W., et al. Systematic review of burnout among healthcare providers in sub-Saharan Africa. BMC public health, 2019, 19.1: 1247. |
[7]
.
The combination of unique stressors, such as political instability and academic demands, with universal pressures like excessive workload and financial burdens, creates a high risk for burnout among Sudanese medical doctors
. However, this critical issue remains severely under-studied, particularly concerning resident physicians, who are among the most vulnerable to these compounding pressures..
Therefore, this study aims to estimate the prevalence of burnout and identify its associated factors among Sudanese resident physicians. The findings are intended to inform government and health sector administrators in developing targeted legislation and policies to address this pressing occupational health issue.
2. Methodology
A descriptive cross-sectional study was conducted from January to June 2025. The study targeted Sudanese medical doctors working in Sudan. A convenience sampling technique was employed, resulting in a sample of 105 doctors who participated over a three-month data collection period. Data were collected online using a pre-coded and pre-tested structured questionnaire distributed via Google Forms.
3. Data Analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 23. Numerical data were summarized using descriptive statistics (mean, standard deviation), and categorical data were presented in frequency tables and percentages. The Chi-square (χ²) test was used to assess relationships between categorical variables. Burnout levels were measured using a scale adapted from established instruments.
To compare burnout levels across different groups, inferential statistical tests were employed. Independent samples t-tests were used to compare mean total burnout scores between two groups. One-way Analysis of Variance (ANOVA) was conducted to compare burnout scores across three or more groups. To identify the key predictors of burnout, a standard multiple regression analysis was performed. The assumptions of linearity, homoscedasticity, and independence of residuals were checked and met prior to the analysis. For all inferential tests, a p-value of less than 0.05 was considered statistically significant.
4. Ethical Approval and Consent to Participate
Ethical approval for this study was granted by the Institutional Review Board (IRB) of Alzaiem Alazhari University. Prior to participation, all respondents were provided with a detailed information sheet and provided written informed consent. The consent process emphasized the voluntary nature of participation, the confidentiality of all collected data, and the right to withdraw at any time without penalty. All data were anonymized and used exclusively for the purposes of this research, in strict compliance with established ethical principles for data privacy and confidentiality.
5. Results
A total of 105 doctors participated in the study. The demographic and occupational characteristics of the participants are summarized in
Table 1. The mean age of respondents was 28 (±8.7) years. The majority were female (75.2%), and most participants were single (74.3%).
Regarding professional status, (54.3%) were specialists, while (45.7%) were general practitioners. Work hours varied among participants, with the majority (69.5%) reporting shifts of 6 to 12 hours per day. A notable proportion (15.2%) worked more than 12 hours daily, which is a potential risk factor for increased stress and burnout. The remaining (15.2%) worked less than 6 hours per day.
Table 1. The demographic and Occupational Characteristics of the Participants (n=105).
Variable | Category | Frequency | Percent (%) |
Gender | Male | 26 | 24.8 |
| Female | 79 | 75.2 |
Marital Status | Single | 78 | 74.3 |
| Married | 21 | 20.0 |
| Divorced | 5 | 4.8 |
| Widowed | 1 | 1.0 |
Specialization | Generalist | 48 | 45.7 |
| Specialist | 57 | 54.3 |
Work Hours | < 6 hours | 16 | 15.2 |
| 6 - 12 hours | 73 | 69.5 |
| > 12 hours | 16 | 15.2 |
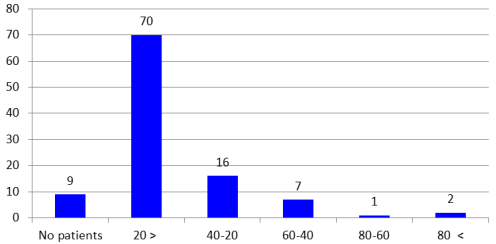
As shown in
Figure 1, the daily patient load among the surveyed doctors was also assessed. The majority (70, 66.6%) reported examining fewer than 20 patients per day. A smaller proportion (16, 15.2%) handled 20 to 40 patients, and (7, 6.6%) reported a caseload ranging between 40 and 60 patients per day.
Figure 1. Distribution of Study Participants According to Number of Cases Encountered Per Day (n=105).
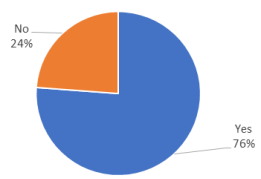
A large majority of doctors (76.2%) reported actively pursuing further studies and research, while (23.8%) were not engaged in such activities,
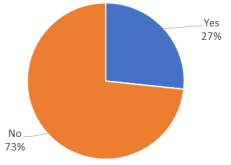
Figure 2. Conversely, most participants (73.3%) reported not engaging in any extracurricular activities, with only (26.7%) participating in activities outside their regular work,
Figure 3.
The analysis of burnout indicators, as detailed in
Table 2, revealed several key findings. Workload and job demands were perceived as moderate to high, with a mean score of 10.32 (SD = 2.092). In contrast, work engagement and attendance were notably low, with a mean score of 1.27 (SD = 1.085). Levels of emotional exhaustion and cynicism were moderate, with a mean score of 5.48 (SD = 1.814). The mean score for work-life balance and personal well-being was 5.40 (SD = 2.737), indicating moderate difficulties in this area. The overall total burnout score averaged 26.86 (SD = 5.283).
Figure 2. Participation of Study Participants in Studies and Research (n=105).
Table 2. Descriptive Statistics of Burnout Indicators (n=105).
Indicator | Minimum | Maximum | Mean ± SD |
Workload and Job Demands | 5 | 15 | 10.32 ± 2.092 |
Work Engagement and Attendance | 0 | 5 | 1.27 ± 1.085 |
Emotional Exhaustion and Cynicism | 1 | 10 | 5.48 ± 1.814 |
Work-Life Balance and Personal Well-Being | 1 | 13 | 5.40 ± 2.737 |
Sleep and Physical Symptoms | 2 | 7 | 4.39 ± 1.236 |
Total Burnout Score | 14 | 39 | 26.86 ± 5.283 |
Figure 3. Participation of Study Participants in Extracurricular Activities (n=105).
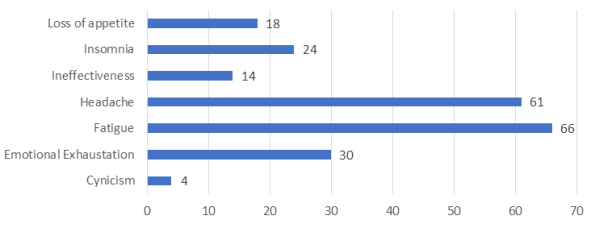
The symptoms of burnout among the surveyed doctors are detailed in
Figure 4. Fatigue (66, 62.9%) and headaches (61, 58.1%) were the most commonly reported physical symptoms. Emotional exhaustion (30, 28.6%) and insomnia (24, 22.9%) were also prevalent. A smaller but notable proportion of participants reported loss of appetite (18, 17.1%) and feelings of ineffectiveness (14, 13.3%). Cynicism was the least reported symptom (4, 3.8%), suggesting that the primary manifestation of burnout in this sample is physical exhaustion rather than emotional detachment.
Figure 4. Prevalence of Burnout Related Symptoms Among Study Participants (n=105).
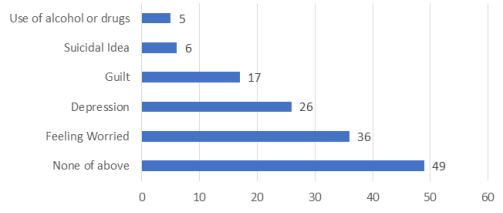
Regarding mental health, nearly half of the doctors (49, 46.7%) reported no symptoms. However, feeling worried was common (36, 34.3%), and a significant number reported symptoms of depression (26, 24.8%) and guilt (17, 16.2%). Suicidal ideation (6, 5.7%) and substance use (5, 4.8%) were also reported,
Figure 5.
Figure 5. Prevalence of Mental Health Symptoms Among Study Participants (n=105).
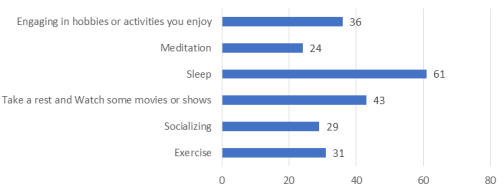
As shown in
Figure 6, the most common coping strategy was sleep (58.1%), followed by resting and watching movies or shows (41.0%). Other reported strategies included engaging in hobbies (34.3%), exercise (29.5%), and socializing (27.6%). Meditation was less common (22.9%) but remained a notable method. The mean self-reported efficacy score for these coping strategies was 3.64 (SD = 0.99), indicating that participants generally found them to be moderately effective.
Figure 6. Coping Strategies Used by Study Participants to Manage Burnout (n=105).
The assessment of burnout levels among the participating doctors yielded a clear and pressing finding: moderate burnout is the most prevalent experience, affecting (43.8%) of the sample. As detailed in
Table 3, when categorized by total score (range: 14-39), the majority of practitioners fell into this middle tier. While a third (33.3%) reported low burnout, it is alarming that nearly a quarter (22.9%) were identified as having high burnout. This distribution is crystallized in the sample's mean total score of 26.86 (SD = 5.28), which sits squarely within the moderate range. This data paints a picture of a workforce under significant strain, where a sizable majority is experiencing tangible levels of burnout.
Table 3. Burnout Levels Among Study Participants (n=105).
Burnout Level | Score Range | Frequency | Percent | Cumulative Percent |
Low Burnout | 14-22 | 35 | 33.3% | 33.3% |
Moderate Burnout | 23-30 | 46 | 43.8% | 77.1% |
High Burnout | 31-39 | 24 | 22.9% | 100% |
Total | | 105 | 100% | |
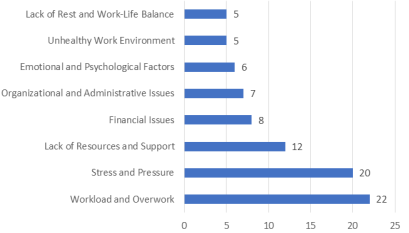
Data on the perceived causes of burnout are presented in
Figure 7. Workload and overwork were the most frequently cited causes of burnout (22, 21.0%), closely followed by stress and pressure (20, 19.0%). The third most significant factor was a lack of resources and support (12, 11.4%). Other notable causes included financial issues (7.6%), organizational and administrative problems (6.7%), and emotional and psychological factors (5.7%). Additionally, an unhealthy work environment and a lack of rest or work-life balance were each identified as contributing factors by (4.8%) of respondents.
Figure 7. Perceived Causes of Burnout Among Doctors (n=105).
An analysis was conducted to compare total burnout scores across key demographic and professional variables. The results indicated no statistically significant differences in burnout levels based on gender, specialization, engagement in continuing studies, or participation in work-related extracurricular activities (p > 0.05 for all comparisons). Specifically, while males reported a slightly lower mean burnout score than females, this difference was not statistically significant (t = -1.300, p = 0.196). Similarly, no significant difference was found between generalists (t = -1.194, p = 0.235).
The analysis also revealed non-significant trends in other areas: physicians continuing their studies showed marginally lower burnout scores (Mean = 26.40, SD = 5.143) than those who were not (Mean = 28.32, SD = 5.566) (t = -1.598, p = 0.113). Conversely, engagement in work-related extracurricular activities did not yield a significant protective effect (Engaged: Mean = 27.89, SD = 4.787 vs. Not Engaged: Mean = 26.48, SD = 5.433; t = 1.214, p = 0.227).
Therefore, it is concluded that these specific demographic and activity-related factors did not significantly influence burnout levels in the studied sample,
Table 4.
Table 4. Independent Samples T-Test Results for Total Burnout Score by Demographic and Activity-Related Factors (n=105).
Variable | Category | N | Mean | S. D | t-value | df | p-value | Mean Difference | Std. Error Difference |
Gender | Male | 26 | 25.69 | 5.85 | -1.30 | 103 | 0.196 | -1.55 | 1.19 |
| Female | 79 | 27.24 | 5.06 | | | | | |
Specialization | Generalist | 48 | 26.19 | 5.05 | -1.190 | 103 | 0.24 | -1.23 | 1.03 |
| Specialist | 57 | 27.42 | 5.454 | | | | | |
Continuing Studies | Yes | 80 | 26.40 | 5.143 | -1.60 | 103 | 0.11 | -1.92 | 1.20 |
| No | 25 | 28.32 | 5.57 | | | | | |
Extracurricular Activities | Yes | 28 | 27.90 | 4.79 | 1.21 | 103 | 0.23 | 1.41 | 1.16 |
| No | 77 | 26.48 | 5.43 | | | | | |
An Analysis of Variance (ANOVA) was conducted to determine if total burnout scores differed significantly based on work hours and the number of cases encountered. The results indicated no statistically significant differences across groups for either variable.
For work hours, the analysis compared three groups (less than 6 hours, 6-12 hours, and more than 12 hours) and found no significant effect on burnout scores (F = 0.399, p = 0.672). Post hoc tests confirmed that none of the pairwise comparisons between these groups were statistically significant.
Similarly, when comparing burnout scores across groups based on the number of cases encountered, the ANOVA result was not statistically significant (F = 2.071, p = 0.075). This suggests that, within this sample, neither work hours nor caseload were significant factors influencing burnout levels. The detailed ANOVA findings are presented in
Table 5.
Table 5. ANOVA for Total Burnout Score by Work Hours and Cases Encountered (n=105).
Variable | Sum of Squares | df | Mean Square | F | Sig. |
Work Hours | | | | | |
Between Groups | 22.540 | 2 | 11.270 | 0.399 | 0.672 |
Within Groups | 2880.318 | 102 | 28.238 | | |
Total | 2902.857 | 104 | | | |
Cases Encountered | | | | | |
Between Groups | 277.333 | 5 | 55.467 | 2.071 | 0.075 |
Within Groups | 2624.782 | 98 | 26.783 | | |
Total | 2902.115 | 103 | | | |
Following the t-test and ANOVA results that indicated burnout levels were not significantly influenced by demographic or simple professional groupings, the analysis proceeded to a more robust, multivariate approach. A multiple regression analysis was therefore conducted to determine if more substantive variables—namely, Sleep and Physical Symptoms and Workload & Job Demands—could predict burnout, while also re-evaluating the role of Gender in the context of these stronger predictors.
The model was statistically significant (F = 22.576, p < 0.001) and explained approximately (40.1%) of the variance in burnout scores (R² = 0.401, Adjusted R² = 0.384). It revealed that while demographic factors were not significant, perceived Workload and Sleep/Physical Symptoms were strong, unique predictors of burnout.
Analysis of the predictors revealed that both Workload & Job Demands (β = 0.377, p < 0.001) and Sleep & Physical Symptoms (β = 0.449, p < 0.001) were significant positive predictors of burnout. This indicates that higher levels of workload and more severe sleep and physical symptoms are associated with increased burnout scores. In contrast, Gender was not a significant predictor in the model (β = 0.028, p = 0.727). These findings are presented in detail in
Table 6.
Table 6. Regression Analysis for Predictors of Total Burnout Score (n=105).
Variable | Unstandardized Coefficients (B) | Standardized Coefficients (β) | t | Sig. |
Constant | 8.344 | - | 3.486 | 0.001 |
Gender | 0.336 | 0.028 | 0.350 | 0.727 |
Workload & Job Demands | 0.953 | 0.377 | 4.842 | 0.000 |
Sleep & Physical Symptoms | 1.918 | 0.449 | 5.623 | 0.000 |
Model Summary | | | | |
R | 0.634 | | | |
R Square | 0.401 | | | |
Adjusted R Square | 0.384 | | | |
Std. Error of the Estimate | 4.148 | | | |
6. Discussion
This study provides a critical snapshot of the mental health and well-being of medical doctors in Sudan, a country grappling with a severely compromised healthcare system due to ongoing conflict. It has severely disrupted the country's healthcare infrastructure, resulting in the closure of approximately (70%) of hospitals in affected regions. This has led to critical shortages of medical supplies and personnel, further exacerbating the challenges faced by healthcare providers
.
Our findings reveal a moderate prevalence of burnout among Sudanese physicians, with (22.9%) experiencing high levels. This prevalence, while significant, is notably lower than pre-conflict data from Khartoum, which reported (77%) of physicians with high emotional exhaustion, (54%) experienced high depersonalization, and (14%) felt a low sense of personal
| [9] | Elsadig SA, Eisawi AO, Ahmed ZE, Ali HA, Ali AM, Hammad AY. The prevalence of Physicians’ burnout syndrome in Ibrahim Malik teaching hospital, Khartoum, Sudan, 2020. J Educ Soc Behav Sci [Internet]. 2023; 36(9): 1–7. Available from: http://dx.doi.org/10.9734/jesbs/2023/v36i91252 |
[9]
. This discrepancy may be attributed to the different methodologies or sampling frames used, or it could reflect a shifting manifestation of distress in a post-collapse environment where the concept of "work-related" stress has been subsumed by survival-related stress.
The symptomatology observed in our sample—primarily fatigue, headaches, emotional exhaustion, and insomnia—aligns with established burnout profiles. These findings are consistent with other regional studies, such as one which reported (21.6%) for high emotional exhaustion and (30.7%) for low personal accomplishment
| [10] | Salihu, Mumeen O. Salihu, et al. Predictors of burnout among resident doctors in a Nigerian teaching hospital. South African Journal of Psychiatry, 2023, 29.1. |
[10]
. Furthermore, the significant mental health burden, with high rates of worry, depression, and guilt, corroborates existing literature on the high prevalence of anxiety and depression among physicians in high-stress environments
| [11] | Obeng nkrumaho, Samuel, et al. Prevalence and correlates of depression, anxiety, and burnout among physicians and postgraduate medical trainees: a scoping review of recent literature. Frontiers in Public Health, 2025, 13: 1537108. |
[11]
.
A key driver identified in our study is the moderate to high level of perceived workload and job demands. This aligns with research from other low-resource settings, such as Tanzania, where inadequate staffing, long working hours, and administrative burdens were major contributors to burnout
.
A meta-analysis included 109 studies from diverse global locations reported that key factors influencing burnout included workplace bullying, job stress, and poor communication, with protective factors such as supportive work environments, adequate staffing, and individual resilience
| [14] | Amiri S, Mahmood N, Mustafa H, Javaid SF, Khan MA. Occupational risk factors for burnout syndrome among healthcare professionals: A global systematic review and meta-analysis. International journal of environmental research and public health. 2024 Nov 27; 21(12): 1583. |
[14]
. In the Sudanese context, these factors are severely exacerbated by the conflict, which has led to increased patient loads and critical resource constraints, intensifying the pressure on remaining healthcare workers.
Further statistical analysis clarifies the drivers of this occupational health problem. Our regression model identified perceived workload and job demands and, even more strongly, Sleep & Physical Symptoms as the only significant predictors of burnout. This finding is critical, as it indicates that the subjective feeling of being overwhelmed and its physical toll are more decisive than objective factors like specific work hours or caseload, which showed no significant association in our ANOVA and t-test analyses. This suggests burnout in Sudan is a universal syndrome, driven less by individual circumstances than by the pervasive pressures of a collapsed system.
Interestingly, our study found low scores for work engagement and attendance issues, contrasting with findings from regions like Saudi Arabia, where burnout is strongly linked to disengagement and absenteeism
| [15] | Aldrees TM, Aleissa S, Zamakhshary M, Badri M, Sadat-Ali M. Physician well-being: prevalence of burnout and associated risk factors in a tertiary hospital, Riyadh, Saudi Arabia. Ann Saudi Med [Internet]. 2013; 33(5): 451–6. Available from: http://dx.doi.org/10.5144/0256-4947.2013.451 |
[15]
. This suggests that Sudanese physicians, despite experiencing burnout, may remain present and engaged in their roles. This resilience could be driven by a profound sense of professional duty and the acute awareness of being one of the few remaining pillars of the healthcare system during a national crisis. However, this sustained engagement likely comes at a great personal cost, as evidenced by the reported work-life imbalance, physical symptoms, and mental health concerns. The presence of suicidal ideation in a small but alarming proportion of respondents underscores the severity of this problem.
7. Conclusion
This study provides critical insights into the prevalence and drivers of burnout among physicians in Sudan, highlighting the severe challenges inherent in their work environment. The findings confirm that high workloads, chronic stress, resource scarcity, and work-life imbalance are significant contributors to burnout, aligning with trends observed in other low-resource and conflict-affected settings.
Despite these immense pressures, a strong sense of professional duty appears to sustain work engagement among Sudanese doctors, even under extreme duress. While personal coping strategies provide some relief, this resilience should not be mistaken for a sustainable solution. The findings underscore an urgent need for systemic interventions to address this occupational health crisis. Ultimately, safeguarding the well-being of healthcare workers is not merely an ethical imperative but a fundamental necessity for preserving Sudan's fragile health system.
8. Recommendations
To address physician burnout in Sudan, a multi-level, collaborative approach is essential. Key recommendations include instituting reasonable working hours, improving workplace conditions, and establishing accessible psychological support systems.
Healthcare institutions must take the lead by improving working conditions through adequate staffing, flexible scheduling, and ensuring the availability of essential resources. Concurrently, they should implement structured mental health support programs, guarantee regular breaks, and foster a supportive work environment. Government and policy makers play a crucial role in establishing and enforcing policies that regulate work hours, enhance job security, and increase funding for healthcare infrastructure. Public health initiatives should also be strengthened to raise awareness about physician well-being. Medical associations are vital for advocating for fair working conditions, providing stress management training, and facilitating peer support networks for their members. Furthermore, these associations should champion ongoing research to monitor burnout trends and guide evidence-based policy. Finally, medical education institutions have a responsibility to integrate burnout prevention and stress management directly into their curricula, emphasizing the importance of work-life balance and equipping future physicians with robust coping strategies from the outset of their careers.
Ultimately, safeguarding the well-being of healthcare workers is not merely an ethical imperative but a fundamental necessity for preserving Sudan's fragile health system.
9. Strengths and Limitations
This study offers valuable insights into the drivers of burnout among physicians in Sudan and suggests potential mitigation strategies. A key strength is its identification of critical, well-established factors such as excessive workload, resource scarcity, and work-life imbalance, which aligns the findings with the global literature on physician burnout and confirms their relevance to similar low-resource settings. Furthermore, the study grounds its recommendations in the practical and actionable changes suggested by the physicians themselves, including reduced working hours, an improved work environment, and accessible psychological support. This provides a crucial foundation for developing targeted, context-specific interventions.
However, several limitations must be considered. The cross-sectional design precludes the establishment of causal relationships between the identified factors and burnout. The reliance on self-reported data introduces the potential for response bias, and the use of a convenience sample, combined with a relatively small sample size, may limit the generalizability of the findings to the broader population of Sudanese physicians. The study's focus may also overlook broader, systemic issues within the national healthcare system that contribute to burnout. Despite these limitations, this research provides an important preliminary understanding of physician burnout in Sudan and effectively highlights critical areas requiring urgent intervention.
Abbreviations
WHO | World Health Organization |
IRB | Institutional Review Board |
Acknowledgments
We would like to thank the respondents for agreeing to participate in this study. We express our deep gratitude to Dr. Salah Abdelgadir Abdelmagid, and Ms. Samia Mohammed Eltayeb for their help and support.
Author Contributions
Afkar Awad Morgan Mohamad: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing
Hiba Salah Abdelgadir: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing.
Naela Hamed Albala Hamed: Investigation, Writing– original draft
Mohammed Yousif Mohammed Elhaj: Investigation, Writing– original draft
Mohammed Abdulwahab Mohammed Sadiq: Investigation, Writing– original draft
Funding
The research was fully funded by the authors.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
Authors declare that there is no competing of interest.
References
| [1] |
Burnout - Mental Health UK (mentalhealth-uk.org) © Mental Health UK, 28 AlbertEmbankment, London, SE1 7GR. Registered Charity no. 1170815.
|
| [2] |
Gonzales Y, Guevara-Delgado N, Alcahuaman J, Jiménez V, Osorio P. Burnout syndrome and intention to leave: An analysis of its impact through a systematic review 2015–2025. Journal of Ecohumanism. 2025; 4(1): 4370-82.
|
| [3] |
Treml MF, Sarubbi AV, Madeira ME, Rasoto AW, Schwarzer N. Burnout syndrome in Brazil (2014–2024): regional variations and temporal trends in an epidemiological study. Revista Brasileira de Medicina do Trabalho. 2025 Sep 14; 23(3): e220251479.
|
| [4] |
Symptoms of Burnout Syndrome among Physicians during the Outbreak of COVID-19 Pandemic—A Systematic Literature Review - PMC (nih.gov).
|
| [5] |
Mental_Distress_among_Medical_Students_in_Khartoum_Sudan_2022Copyright © 2022 by author(s) and Scientific Research Publishing Inc.
https://www.researchgate.net/publication/364704966_
|
| [6] |
Owuoro, Rosebenter Awuor, et al. Prevalence of burnout among nurses in sub-Saharan Africa: a systematic review. JBI Evidence Synthesis, 2020, 18.6: 1189-1207.
|
| [7] |
Dubaled, Benyam W., et al. Systematic review of burnout among healthcare providers in sub-Saharan Africa. BMC public health, 2019, 19.1: 1247.
|
| [8] |
Taha AE. The state of health and health services in Sudan as a result of the war. Afr J Prim Health Care Fam Med [Internet]. 2023; 15(1): 4260. Available from:
http://dx.doi.org/10.4102/phcfm.v15i1.4260
|
| [9] |
Elsadig SA, Eisawi AO, Ahmed ZE, Ali HA, Ali AM, Hammad AY. The prevalence of Physicians’ burnout syndrome in Ibrahim Malik teaching hospital, Khartoum, Sudan, 2020. J Educ Soc Behav Sci [Internet]. 2023; 36(9): 1–7. Available from:
http://dx.doi.org/10.9734/jesbs/2023/v36i91252
|
| [10] |
Salihu, Mumeen O. Salihu, et al. Predictors of burnout among resident doctors in a Nigerian teaching hospital. South African Journal of Psychiatry, 2023, 29.1.
|
| [11] |
Obeng nkrumaho, Samuel, et al. Prevalence and correlates of depression, anxiety, and burnout among physicians and postgraduate medical trainees: a scoping review of recent literature. Frontiers in Public Health, 2025, 13: 1537108.
|
| [12] |
Iyer S, Suleman S, Qiu Y, Platt S. Risk factors for physician burnout: a perspective from Tanzania. Pan Afr Med J [Internet]. 2022; 41: 298. Available from:
http://dx.doi.org/10.11604/pamj.2022.41.298.31055
|
| [13] |
Doctor on the frontlines: Saving Sudan’s most vulnerable in the midst of war [Internet]. Angels in Medicine. 2025 [cited 2025 Mar 21]. Available from:
https://www.medangel.org/doctor-on-the-frontlines-saving-sudans-most-vulnerable-in-the-midst-of-war
|
| [14] |
Amiri S, Mahmood N, Mustafa H, Javaid SF, Khan MA. Occupational risk factors for burnout syndrome among healthcare professionals: A global systematic review and meta-analysis. International journal of environmental research and public health. 2024 Nov 27; 21(12): 1583.
|
| [15] |
Aldrees TM, Aleissa S, Zamakhshary M, Badri M, Sadat-Ali M. Physician well-being: prevalence of burnout and associated risk factors in a tertiary hospital, Riyadh, Saudi Arabia. Ann Saudi Med [Internet]. 2013; 33(5): 451–6. Available from:
http://dx.doi.org/10.5144/0256-4947.2013.451
|
Cite This Article
-
APA Style
Mohamad, A. A. M., Abdelgadir, H. S., Hamed, N. H. A., Elha, M. Y. M., Sadiq, M. A. M. (2026). Prevalence of Burnout Syndrome Among Medical Doctors in Sudan 2025. Innovation, 7(1), 1-10. https://doi.org/10.11648/j.innov.20260701.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Mohamad, A. A. M.; Abdelgadir, H. S.; Hamed, N. H. A.; Elha, M. Y. M.; Sadiq, M. A. M. Prevalence of Burnout Syndrome Among Medical Doctors in Sudan 2025. Innovation. 2026, 7(1), 1-10. doi: 10.11648/j.innov.20260701.11
Copy
|
Download
-
@article{10.11648/j.innov.20260701.11,
author = {Afkar Awad Morgan Mohamad and Hiba Salah Abdelgadir and Naela Hamed Albala Hamed and Mohammed Yousif Mohammed Elha and Mohammed Abdulwahab Mohammed Sadiq},
title = {Prevalence of Burnout Syndrome Among Medical Doctors in Sudan 2025},
journal = {Innovation},
volume = {7},
number = {1},
pages = {1-10},
doi = {10.11648/j.innov.20260701.11},
url = {https://doi.org/10.11648/j.innov.20260701.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.innov.20260701.11},
abstract = {Burnout syndrome is a state of emotional, mental, and physical exhaustion resulting from prolonged occupational stress, which is highly prevalent among healthcare professionals. It adversely affects clinical performance, decision-making, and personal well-being. In Sudan, medical doctors face unique stressors, including political instability and extended working hours; however, burnout remains an under-investigated area. This study aims to determine the prevalence of burnout among Sudanese medical doctors, identify its contributing factors, assess its impact on well-being, and explore effective coping mechanisms. A cross-sectional study was conducted using a convenience sample of Sudanese medical doctors. Data collected electronically via standardized questionnaires, capturing demographic information, work-related variables, and burnout symptoms. Data analysis was performed using SPSS to determine burnout prevalence and associated factors. Ethical approval was obtained from Alzaiem Alazhari University. Among the 105 participating doctors, the mean age was 28 years; the majority were female (75.2%) and single (74.3%). Specialists constituted (54.3%) of the sample. Most participants worked 6–12 hours daily, with a significant proportion exceeding 12 hours. While the majority handled fewer than 20 cases per day, a minority reported a high patient load. Key burnout indicators revealed a moderate to high perceived workload (Mean = 10.32, SD = 2.092), low work engagement (Mean = 1.27, SD = 1.085), and a compromised work-life balance (Mean = 5.40, SD = 2.737). The most common physical symptoms were fatigue (62.9%) and headaches (58.1%). Emotional exhaustion (28.6%) and insomnia (22.9%) were also prevalent, while loss of appetite (17.1%), feelings of ineffectiveness (13.3%), and cynicism (3.8%) were reported by smaller but notable proportions. The findings indicate a moderate prevalence of burnout among Sudanese medical doctors, primarily driven by long working hours, high patient loads, and limited engagement in restorative activities. The concurrent pursuit of academic advancement amidst these stressors likely exacerbates emotional exhaustion. This study underscores the urgent need for institutional mental health support, increased awareness, and the implementation of structured coping strategies to mitigate burnout and enhance the overall well-being and professional performance of doctors in Sudan.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Prevalence of Burnout Syndrome Among Medical Doctors in Sudan 2025
AU - Afkar Awad Morgan Mohamad
AU - Hiba Salah Abdelgadir
AU - Naela Hamed Albala Hamed
AU - Mohammed Yousif Mohammed Elha
AU - Mohammed Abdulwahab Mohammed Sadiq
Y1 - 2026/02/02
PY - 2026
N1 - https://doi.org/10.11648/j.innov.20260701.11
DO - 10.11648/j.innov.20260701.11
T2 - Innovation
JF - Innovation
JO - Innovation
SP - 1
EP - 10
PB - Science Publishing Group
SN - 2994-7138
UR - https://doi.org/10.11648/j.innov.20260701.11
AB - Burnout syndrome is a state of emotional, mental, and physical exhaustion resulting from prolonged occupational stress, which is highly prevalent among healthcare professionals. It adversely affects clinical performance, decision-making, and personal well-being. In Sudan, medical doctors face unique stressors, including political instability and extended working hours; however, burnout remains an under-investigated area. This study aims to determine the prevalence of burnout among Sudanese medical doctors, identify its contributing factors, assess its impact on well-being, and explore effective coping mechanisms. A cross-sectional study was conducted using a convenience sample of Sudanese medical doctors. Data collected electronically via standardized questionnaires, capturing demographic information, work-related variables, and burnout symptoms. Data analysis was performed using SPSS to determine burnout prevalence and associated factors. Ethical approval was obtained from Alzaiem Alazhari University. Among the 105 participating doctors, the mean age was 28 years; the majority were female (75.2%) and single (74.3%). Specialists constituted (54.3%) of the sample. Most participants worked 6–12 hours daily, with a significant proportion exceeding 12 hours. While the majority handled fewer than 20 cases per day, a minority reported a high patient load. Key burnout indicators revealed a moderate to high perceived workload (Mean = 10.32, SD = 2.092), low work engagement (Mean = 1.27, SD = 1.085), and a compromised work-life balance (Mean = 5.40, SD = 2.737). The most common physical symptoms were fatigue (62.9%) and headaches (58.1%). Emotional exhaustion (28.6%) and insomnia (22.9%) were also prevalent, while loss of appetite (17.1%), feelings of ineffectiveness (13.3%), and cynicism (3.8%) were reported by smaller but notable proportions. The findings indicate a moderate prevalence of burnout among Sudanese medical doctors, primarily driven by long working hours, high patient loads, and limited engagement in restorative activities. The concurrent pursuit of academic advancement amidst these stressors likely exacerbates emotional exhaustion. This study underscores the urgent need for institutional mental health support, increased awareness, and the implementation of structured coping strategies to mitigate burnout and enhance the overall well-being and professional performance of doctors in Sudan.
VL - 7
IS - 1
ER -
Copy
|
Download