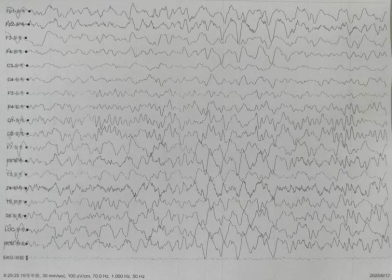
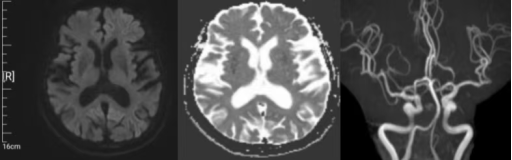
Background: RT-QuIC (Real-Time QuIC) is a clinical diagnostic method that detects trace proteins in samples through protein amplification. According to the international CJD diagnostic criteria, RT-QuIC provides diagnostic evidence that is second only to that of pathology. Presently, this approach remains underutilized in China. Case Report: A 76-year-old female patient was admitted to the hospital for a period of two weeks, characterized by a general slowing of her cognitive responses. A physical examination revealed elevated levels of cognitive impairment, as indicated by a Mini-Mental State Examination (MMSE) score of 12 and a Montreal Cognitive Assessment (MoCA) score of 8. An electroencephalogram (EEG) revealed moderate abnormalities, characterized by intermittent high-amplitude delta waves (frequency 3–3.5 Hz) across multiple leads and short-range rhythmic discharges in several leads. A magnetic resonance imaging (MRI) scan revealed the presence of ribbon-like changes in the parietal and temporal cortical regions on diffusion-weighted imaging (DWI) sequences. CSF testing for 14-3-3 protein yielded a negative result, while RT-QuIC testing produced a positive result. Treatment: The primary management strategy encompassed the provision of supportive care and the management of symptoms. The clinical outcome is as follows: The treatment response was unsatisfactory, with a rapid disease progression over a 52-day period. The patient exhibited a progressive deterioration in visuospatial function, accompanied by the emergence of myoclonus, tremor, urinary and fecal incontinence, and motor mutism. Conclusion: RT-QuIC testing has the potential to enhance diagnostic specificity and sensitivity in patients suspected of having Creutzfeldt-Jakob disease (CJD).
| Published in | Science Discovery (Volume 13, Issue 6) |
| DOI | 10.11648/j.sd.20251306.16 |
| Page(s) | 139-142 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Creutzfeldt-Jakob Disease, 14-3-3 Protein, RT-QuIC, Cortical Ribbon Sign

| [1] | 鄢琳琳, 杨羽芳, 罗忠. 散发型克-雅病一例 [J]. 海南医学, 2025, 36(09): 1329-1332. |
| [2] | Narula R, Tinaz S. Creutzfeldt-Jakob Disease[J]. New England Journal of Medicine, 2018, 378(4): e7. |
| [3] | 葛天翔, 荚杨洋, 李春辉, 等. 克-雅病医疗机构感染防控专家共识 [J]. 中国感染控制杂志, 2025, 24(04): 437-450. |
| [4] | Kong Y, Chen Z, Shi Q, et al. Clinical correlates of cerebrospinal fluid 14-3-3 protein in non-prion rapid progressive dementia[J]. Journal of Alzheimer’s Disease, 2023, 91(1): 263-272. |
| [5] | Humpel C, Benke T. Cerebrospinal fluid levels of 14-3-3 gamma: what does it tell us about sporadic Creutzfeldt-Jakob disease?[J]. Pharmacology, 2017, 100(5-6): 243-245. |
| [6] | Fayolle M, Lehmann S, Delaby C. Comparison of cerebrospinal fluid tau, ptau (181), synuclein, and 14-3-3 for the detection of Creutzfeldt–Jakob disease in clinical practice[J]. Journal of Neural Transmission, 2022, 129(2): 133-139. |
| [7] | Atarashi R. RT-QuIC as ultrasensitive method for prion detection[J]. Cell and Tissue Research, 2023, 392(1): 295-300. |
| [8] | Green A J E. RT-QuIC: a new test for sporadic CJD[J]. Practical neurology, 2019, 19(1): 49-55. |
| [9] | Orrú C D, Groveman B R, Foutz A, et al. Ring trial of 2nd generation RT‐QuIC diagnostic tests for sporadic CJD[J]. Annals of Clinical and Translational Neurology, 2020, 7(11): 2262-2271. |
| [10] | Fan T H, Kharal G A, Biedny J, et al. Callosal Diffusion-Restriction in Patients with Intracranial Hemorrhage[J]. Journal of Stroke and Cerebrovascular Diseases, 2021, 30(9): 105951. |
| [11] | Haq I, Sohail A A, Rasheed M. Role of MRI in Diagnosis of Rapidly Progressive Cognitive Impairment-A Case Of Sporadic Creutzfeldt Jakob Disease (sCJD)[J]. Age and Ageing, 2024, 53(Supplement_4): afae178. 072. |
| [12] | Fiorini M, Iselle G, Perra D, et al. High diagnostic accuracy of RT-QuIC assay in a prospective study of patients with suspected sCJD[J]. International journal of molecular sciences, 2020, 21(3): 880. |
| [13] | 陈帅, 贺爽, 张杰文. 散发型克-雅病头颅磁共振影像异常分析 [J]. 中国实用神经疾病杂志, 2020, 23(05): 401-405. |
| [14] | Matsubayashi T, Akaza M, Hayashi Y, et al. Specific electroencephalogram features in the very early phases of sporadic Creutzfeldt–Jakob disease[J]. Journal of the neurological sciences, 2022, 437: 120265. |
| [15] | Mousailidis G, Lazzari C, Bhan‐Kotwal S, et al. Rapidly progressive dementia with psychosis caused by CJD[J]. Progress in Neurology and Psychiatry, 2018, 22(4): 19-22. |
APA Style
Jia, Z., Geng, J. (2025). A Case of Sporadic Creutzfeldt-Jakob Disease (sCJD) with Lightning-like Progression. Science Discovery, 13(6), 139-142. https://doi.org/10.11648/j.sd.20251306.16
ACS Style
Jia, Z.; Geng, J. A Case of Sporadic Creutzfeldt-Jakob Disease (sCJD) with Lightning-like Progression. Sci. Discov. 2025, 13(6), 139-142. doi: 10.11648/j.sd.20251306.16
@article{10.11648/j.sd.20251306.16,
author = {Zhengchang Jia and Jinfeng Geng},
title = {A Case of Sporadic Creutzfeldt-Jakob Disease (sCJD) with Lightning-like Progression
},
journal = {Science Discovery},
volume = {13},
number = {6},
pages = {139-142},
doi = {10.11648/j.sd.20251306.16},
url = {https://doi.org/10.11648/j.sd.20251306.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sd.20251306.16},
abstract = {Background: RT-QuIC (Real-Time QuIC) is a clinical diagnostic method that detects trace proteins in samples through protein amplification. According to the international CJD diagnostic criteria, RT-QuIC provides diagnostic evidence that is second only to that of pathology. Presently, this approach remains underutilized in China. Case Report: A 76-year-old female patient was admitted to the hospital for a period of two weeks, characterized by a general slowing of her cognitive responses. A physical examination revealed elevated levels of cognitive impairment, as indicated by a Mini-Mental State Examination (MMSE) score of 12 and a Montreal Cognitive Assessment (MoCA) score of 8. An electroencephalogram (EEG) revealed moderate abnormalities, characterized by intermittent high-amplitude delta waves (frequency 3–3.5 Hz) across multiple leads and short-range rhythmic discharges in several leads. A magnetic resonance imaging (MRI) scan revealed the presence of ribbon-like changes in the parietal and temporal cortical regions on diffusion-weighted imaging (DWI) sequences. CSF testing for 14-3-3 protein yielded a negative result, while RT-QuIC testing produced a positive result. Treatment: The primary management strategy encompassed the provision of supportive care and the management of symptoms. The clinical outcome is as follows: The treatment response was unsatisfactory, with a rapid disease progression over a 52-day period. The patient exhibited a progressive deterioration in visuospatial function, accompanied by the emergence of myoclonus, tremor, urinary and fecal incontinence, and motor mutism. Conclusion: RT-QuIC testing has the potential to enhance diagnostic specificity and sensitivity in patients suspected of having Creutzfeldt-Jakob disease (CJD).
},
year = {2025}
}
TY - JOUR T1 - A Case of Sporadic Creutzfeldt-Jakob Disease (sCJD) with Lightning-like Progression AU - Zhengchang Jia AU - Jinfeng Geng Y1 - 2025/12/24 PY - 2025 N1 - https://doi.org/10.11648/j.sd.20251306.16 DO - 10.11648/j.sd.20251306.16 T2 - Science Discovery JF - Science Discovery JO - Science Discovery SP - 139 EP - 142 PB - Science Publishing Group SN - 2331-0650 UR - https://doi.org/10.11648/j.sd.20251306.16 AB - Background: RT-QuIC (Real-Time QuIC) is a clinical diagnostic method that detects trace proteins in samples through protein amplification. According to the international CJD diagnostic criteria, RT-QuIC provides diagnostic evidence that is second only to that of pathology. Presently, this approach remains underutilized in China. Case Report: A 76-year-old female patient was admitted to the hospital for a period of two weeks, characterized by a general slowing of her cognitive responses. A physical examination revealed elevated levels of cognitive impairment, as indicated by a Mini-Mental State Examination (MMSE) score of 12 and a Montreal Cognitive Assessment (MoCA) score of 8. An electroencephalogram (EEG) revealed moderate abnormalities, characterized by intermittent high-amplitude delta waves (frequency 3–3.5 Hz) across multiple leads and short-range rhythmic discharges in several leads. A magnetic resonance imaging (MRI) scan revealed the presence of ribbon-like changes in the parietal and temporal cortical regions on diffusion-weighted imaging (DWI) sequences. CSF testing for 14-3-3 protein yielded a negative result, while RT-QuIC testing produced a positive result. Treatment: The primary management strategy encompassed the provision of supportive care and the management of symptoms. The clinical outcome is as follows: The treatment response was unsatisfactory, with a rapid disease progression over a 52-day period. The patient exhibited a progressive deterioration in visuospatial function, accompanied by the emergence of myoclonus, tremor, urinary and fecal incontinence, and motor mutism. Conclusion: RT-QuIC testing has the potential to enhance diagnostic specificity and sensitivity in patients suspected of having Creutzfeldt-Jakob disease (CJD). VL - 13 IS - 6 ER -
Department of Neurology, Jinzhong Second People's Hospital, Jinzhong, China
Information