Abstract
Introduction: According to world health organization each year, 3.6 million deaths in children under the age of five are attributable to neonatal mortality, accounting for 41% of all deaths in children under the age of five. Most of these deaths occur in low-income countries, and almost a million of these neonatal deaths either directly or indirectly related to neonatal sepsis. This study aimed to assess the time to death and its predictors among neonates admitted with neonatal sepsis at public comprehensive and general hospitals in the West Arsi zone of southern Ethiopia. Method: This multicenter institution-based retrospective follow-up study conducted from May 30 to June 30, 2023. Kobo toolbox was used for data collection. Checked for completeness, edited, and coded using Microsoft Excel. The data imported into STATA version 18 and cleaned before analysis. The incidence rate estimated for the entire study period and specified intervals of hospital stay. The Weibull regression model was selected using Akaike information criteria and Bayesian information criteria and used to analyze the relationship between the outcome and independent variables. Variables in the bi-variable analysis with p-value ≤ 0.25 were as candidates for multivariable analysis. In the multivariable analysis, statistical significance was set at p < 0.05. The association summarized using an adjusted hazard ratio (AHR) with a 95% confidence interval. Result: Of the 526 neonates with neonatal sepsis, 67 (12.7%) (95% confidence interval [CI]: 10–15.9) died. The overall incidence of neonatal mortality was 16.1 per 1000 neonatal days. The mean time to death among neonates died was 7.9 days (95% CI: 7.63, 8.19). Respiratory distress at admission (Adjusted Hazard Ratio (AHR): 0.37, 95% CI: 0.18, 0.77), breastfeeding within one hour (AHR: 3.15, 95% CI: 1.38, 7.18), gravidity (AHR: 0.37, 95% CI: 0.15, 0.88), and maternal health problems (AHR: 0.44, 95% CI: 0.25, 0.79) were found to be significant predictors of neonatal mortality. Conclusion: This study revealed that among neonates, 67 (12.7%) (95% CI: 10, 15.9) died during the follow-up period. Respiratory distress during admission, initiation of breastfeeding within one hour of birth, gravidity, and maternal health problems were predictors of mortality among neonates admitted with neonatal sepsis. Early initiation of breast feeding, monitoring of high-risk mothers, and strengthening NICU care are some of recommendations.
Keywords
Neonatal Sepsis, Mortality, Time to Death, Predictors, Ethiopia
1. Introduction
The first month of life is the most vulnerable period for neonates, among whom many face severe disease and the risk of death
| [1] | Degefa N, Diriba K, Girma T, Kebede A, Senbeto A, Eshetu E, et al. Knowledge about Neonatal Danger Signs and Associated Factors among Mothers Attending Immunization Clinic at Arba Minch General Hospital, Southern Ethiopia: A Cross-Sectional Study. Biomed Res Int. 2019; 2019: 1–8. |
| [2] | Geta T, Kassa T, Israel E. Magnitude of sepsis and its predictors among neonates admitted to neonatal intensive care unit at Hawassa University comprehensive specialized hospital in Southern Ethiopia 2022. 2022; 12(3). |
[1, 2]
. Sepsis, prematurity, and birth complications can lead to death and disease during the neonatal period
| [3] | Mengesha HG, Sahle BW. Cause of neonatal deaths in Northern Ethiopia: A prospective cohort study. BMC Public Health [Internet]. 2017; 17(1): 1–8. Available from:
http://dx.doi.org/10.1186/s12889-016-3979-8 |
| [4] | Getabelew A, Aman M, Fantaye E, Yeheyis T. Prevalence of Neonatal Sepsis and Associated Factors among Neonates in Neonatal Intensive Care Unit at Selected Governmental Hospitals in Shashemene Town, Oromia Regional State, Ethiopia, 2017. Int J Pediatr. 2018; 2018: 1–7. |
[3, 4]
. Sepsis is a life-threatening condition that results in organ dysfunction caused by an uncontrolled host response to infection, which can affect the health of neonates and is a serious worldwide health threat
| [5] | Lobo BBP, Marba STM, Machado HC, Caldas JPS. Neonatal Sequential Organ Failure Assessment as a late-onset sepsis mortality predictor in very low birth weight newborns: a Brazilian cohort study. Eur J Pediatr. 2022; 181(10): 3767–74. |
| [6] | Ahmed I, Ali SM, Amenga-Etego S, Ariff S, Bahl R, Baqui AH, et al. Population-based rates, timing, and causes of maternal deaths, stillbirths, and neonatal deaths in south Asia and sub-Saharan Africa: a multi-country prospective cohort study. Lancet Glob Heal. 2018; 6(12): e1297–308. |
[5, 6]
.
Neonatal sepsis (NS) is defined as any systemic manifestation such as abnormal body temperature, hypothermia, hyperthermia, respiratory problems such as fast breathing, hypoxia, respiratory distress, food intolerance, and the isolation of bacteria or other pathogens from the bloodstream
| [2] | Geta T, Kassa T, Israel E. Magnitude of sepsis and its predictors among neonates admitted to neonatal intensive care unit at Hawassa University comprehensive specialized hospital in Southern Ethiopia 2022. 2022; 12(3). |
| [7] | Tewabe T, Mohammed S, Tilahun Y, Melaku B, Fenta M, Dagnaw T, et al. Clinical outcome and risk factors of neonatal sepsis among neonates in Felege Hiwot referral Hospital, Bahir Dar, Amhara Regional State, North West Ethiopia 2016: A retrospective chart review. BMC Res Notes. 2017; 10(1): 1–7. |
[2, 7]
.
Neonatal sepsis is divided into two main groups: early onset neonatal sepsis (EONS) and late-onset neonatal sepsis (LONS)
| [2] | Geta T, Kassa T, Israel E. Magnitude of sepsis and its predictors among neonates admitted to neonatal intensive care unit at Hawassa University comprehensive specialized hospital in Southern Ethiopia 2022. 2022; 12(3). |
| [8] | Simonsen KA, Anderson-Berry AL, Delair SF, Dele Davies H. Early-onset neonatal sepsis. Clin Microbiol Rev. 2014; 27(1): 21–47. |
[2, 8]
. Early onset neonatal sepsis refers to newborn sepsis that manifests during the first seven days of life and is primarily caused by bacteria acquired before and after birth, with respiratory distress being the most frequent mode of presentation
| [2] | Geta T, Kassa T, Israel E. Magnitude of sepsis and its predictors among neonates admitted to neonatal intensive care unit at Hawassa University comprehensive specialized hospital in Southern Ethiopia 2022. 2022; 12(3). |
| [9] | Shehab El-Din EMR, El-Sokkary MMA, Bassiouny MR, Hassan R. Epidemiology of neonatal sepsis and implicated pathogens: A Study from Egypt. Biomed Res Int. 2015; 2015. |
[2, 9]
.
Appropriate antibiotic therapy and supportive care are crucial in the management of neonates with sepsis, and the choice of antibiotic therapy is best guided by the knowledge of the etiological agent
| [8] | Simonsen KA, Anderson-Berry AL, Delair SF, Dele Davies H. Early-onset neonatal sepsis. Clin Microbiol Rev. 2014; 27(1): 21–47. |
| [9] | Shehab El-Din EMR, El-Sokkary MMA, Bassiouny MR, Hassan R. Epidemiology of neonatal sepsis and implicated pathogens: A Study from Egypt. Biomed Res Int. 2015; 2015. |
[8, 9]
.
Despite substantial advances in neonatal sepsis diagnosis, prevention, care, and management strategies, the incidence of death among neonates with neonatal sepsis remains high
| [7] | Tewabe T, Mohammed S, Tilahun Y, Melaku B, Fenta M, Dagnaw T, et al. Clinical outcome and risk factors of neonatal sepsis among neonates in Felege Hiwot referral Hospital, Bahir Dar, Amhara Regional State, North West Ethiopia 2016: A retrospective chart review. BMC Res Notes. 2017; 10(1): 1–7. |
| [10] | Mustefa A, Abera A, Aseffa A, Abathun T, Degefa N, Tadesse H, et al. Prevalence of neonatal sepsis and associated factors amongst neonates admitted in arbaminch general hospital, arbaminch, southern Ethiopia, 2019. J Pediatr Neonatal Care. 2020; 10(1): 1–7. |
[7, 10]
. However, there are limited studies on the time to death and its predictors among neonates admitted with neonatal sepsis in the study area and Ethiopia.
Each year, 3.6 million deaths in children under the age of five are attributable to neonatal mortality, accounting for 41% of all deaths in children under the age of five
| [4] | Getabelew A, Aman M, Fantaye E, Yeheyis T. Prevalence of Neonatal Sepsis and Associated Factors among Neonates in Neonatal Intensive Care Unit at Selected Governmental Hospitals in Shashemene Town, Oromia Regional State, Ethiopia, 2017. Int J Pediatr. 2018; 2018: 1–7. |
| [9] | Shehab El-Din EMR, El-Sokkary MMA, Bassiouny MR, Hassan R. Epidemiology of neonatal sepsis and implicated pathogens: A Study from Egypt. Biomed Res Int. 2015; 2015. |
| [11] | Abebia MT. Time to Death and Its Predictors Among Neonates Admitted With Neonatal Sepsis at Public Referral Hospitals of Bahir Dar City, Northwest Ethiopia, 2021 : Retrospective Cohort Study. Res Sq. 2021; 1–24. |
[4, 9, 11]
. Neonatal sepsis (infections) (35%), preterm birth (28%), intrapartum related complications (24%), and asphyxia (23%) are the major causes of neonatal deaths globally, as estimated by the World Health Organization and United Nations Children’s Fund (UNICEF)
| [2] | Geta T, Kassa T, Israel E. Magnitude of sepsis and its predictors among neonates admitted to neonatal intensive care unit at Hawassa University comprehensive specialized hospital in Southern Ethiopia 2022. 2022; 12(3). |
| [5] | Lobo BBP, Marba STM, Machado HC, Caldas JPS. Neonatal Sequential Organ Failure Assessment as a late-onset sepsis mortality predictor in very low birth weight newborns: a Brazilian cohort study. Eur J Pediatr. 2022; 181(10): 3767–74. |
| [8] | Simonsen KA, Anderson-Berry AL, Delair SF, Dele Davies H. Early-onset neonatal sepsis. Clin Microbiol Rev. 2014; 27(1): 21–47. |
[2, 5, 8]
. As a result, neonatal sepsis is the most common cause of neonatal mortality and is probably responsible for 30-50% of total neonatal (infant) deaths each year in developing countries
| [6] | Ahmed I, Ali SM, Amenga-Etego S, Ariff S, Bahl R, Baqui AH, et al. Population-based rates, timing, and causes of maternal deaths, stillbirths, and neonatal deaths in south Asia and sub-Saharan Africa: a multi-country prospective cohort study. Lancet Glob Heal. 2018; 6(12): e1297–308. |
| [12] | Gudayu TW, Zeleke EG, Lakew AM. Time to Death and its Predictors among Neonates Admitted in the Intensive Care Unit of the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia . Res Reports Neonatol. 2020; Volume 10: 1–10. |
[6, 12]
.
An increasing trend in the incidence of neonatal sepsis and decreasing trends in mortality from neonatal sepsis were observed worldwide from 1990 to 2019. The highest absolute burden in sub-Saharan Africa and Asia
| [3] | Mengesha HG, Sahle BW. Cause of neonatal deaths in Northern Ethiopia: A prospective cohort study. BMC Public Health [Internet]. 2017; 17(1): 1–8. Available from:
http://dx.doi.org/10.1186/s12889-016-3979-8 |
| [4] | Getabelew A, Aman M, Fantaye E, Yeheyis T. Prevalence of Neonatal Sepsis and Associated Factors among Neonates in Neonatal Intensive Care Unit at Selected Governmental Hospitals in Shashemene Town, Oromia Regional State, Ethiopia, 2017. Int J Pediatr. 2018; 2018: 1–7. |
[3, 4]
and the neonatal death rate decreased by 48% from the 1990 estimate to 28 per 1,000 live births in 2013, while the reduction rate of the under-five mortality rate was approximately 67%
| [6] | Ahmed I, Ali SM, Amenga-Etego S, Ariff S, Bahl R, Baqui AH, et al. Population-based rates, timing, and causes of maternal deaths, stillbirths, and neonatal deaths in south Asia and sub-Saharan Africa: a multi-country prospective cohort study. Lancet Glob Heal. 2018; 6(12): e1297–308. |
[6]
. More robust epidemiological research and effective health strategies are urgently required to reduce the disease burden of neonatal sepsis worldwide
| [6] | Ahmed I, Ali SM, Amenga-Etego S, Ariff S, Bahl R, Baqui AH, et al. Population-based rates, timing, and causes of maternal deaths, stillbirths, and neonatal deaths in south Asia and sub-Saharan Africa: a multi-country prospective cohort study. Lancet Glob Heal. 2018; 6(12): e1297–308. |
| [13] | Yamey G, Horváth H, Schmidt L, Myers J, Brindis CD. Reducing the global burden of Preterm Birth through knowledge transfer and exchange: A research agenda for engaging effectively with policymakers. Reprod Health [Internet]. 2016; 13(1): 1–9. Available from:
http://dx.doi.org/10.1186/s12978-016-0146-8 |
[6, 13]
.
Approximately 2.6 million children die in the first month of life and 7,000 newborns die each day
| [6] | Ahmed I, Ali SM, Amenga-Etego S, Ariff S, Bahl R, Baqui AH, et al. Population-based rates, timing, and causes of maternal deaths, stillbirths, and neonatal deaths in south Asia and sub-Saharan Africa: a multi-country prospective cohort study. Lancet Glob Heal. 2018; 6(12): e1297–308. |
| [11] | Abebia MT. Time to Death and Its Predictors Among Neonates Admitted With Neonatal Sepsis at Public Referral Hospitals of Bahir Dar City, Northwest Ethiopia, 2021 : Retrospective Cohort Study. Res Sq. 2021; 1–24. |
[6, 11]
. In 2018, neonatal sepsis accounted for 15% of the global neonatal mortality
| [6] | Ahmed I, Ali SM, Amenga-Etego S, Ariff S, Bahl R, Baqui AH, et al. Population-based rates, timing, and causes of maternal deaths, stillbirths, and neonatal deaths in south Asia and sub-Saharan Africa: a multi-country prospective cohort study. Lancet Glob Heal. 2018; 6(12): e1297–308. |
| [7] | Tewabe T, Mohammed S, Tilahun Y, Melaku B, Fenta M, Dagnaw T, et al. Clinical outcome and risk factors of neonatal sepsis among neonates in Felege Hiwot referral Hospital, Bahir Dar, Amhara Regional State, North West Ethiopia 2016: A retrospective chart review. BMC Res Notes. 2017; 10(1): 1–7. |
[6, 7]
. Early diagnosis and appropriate and timely clinical management of neonatal problems
| [5] | Lobo BBP, Marba STM, Machado HC, Caldas JPS. Neonatal Sequential Organ Failure Assessment as a late-onset sepsis mortality predictor in very low birth weight newborns: a Brazilian cohort study. Eur J Pediatr. 2022; 181(10): 3767–74. |
| [12] | Gudayu TW, Zeleke EG, Lakew AM. Time to Death and its Predictors among Neonates Admitted in the Intensive Care Unit of the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia . Res Reports Neonatol. 2020; Volume 10: 1–10. |
[5, 12]
can prevent around 84% of neonatal deaths. Compared to developed countries, low and middle-income countries have approximately forty times higher incidence rates of neonatal infection and double death rates
| [14] | Sisay EA, Mengistu BL, Taye WA, Fentie AM, Yabeyu AB. Length of Hospital Stay and Its Predictors Among Neonatal Sepsis Patients: A Retrospective Follow-Up Study. Int J Gen Med. 2022; 15(November): 8133–42. |
| [15] | Seyoum K, Sahiledengle B, Kene C, Geta G, Gomora D, Ejigu N, et al. Determinants of neonatal sepsis among neonates admitted to neonatal intensive care units in ethiopian hospitals: A systematic review and meta-analysis. Heliyon [Internet]. 2023; 9(9): e20336. Available from:
https://doi.org/10.1016/j.heliyon.2023.e20336 |
[14, 15]
. Neonatal infections account for 26% of annual neonatal deaths in sub-Saharan Africa
| [10] | Mustefa A, Abera A, Aseffa A, Abathun T, Degefa N, Tadesse H, et al. Prevalence of neonatal sepsis and associated factors amongst neonates admitted in arbaminch general hospital, arbaminch, southern Ethiopia, 2019. J Pediatr Neonatal Care. 2020; 10(1): 1–7. |
| [16] | SCHOOL OF GRADUAATE STUDIES SURVIVAL STATUS AND ITS PREDICTORS AMONG PRETERM NEONATES ADMITTED TO NEONATAL INTENSIVE CARE UNITS AT PUBLIC HOSPITALS IN WEST GUJI AND BORENA ZONES, SOUTHERN ETHIOPIA MPH THESIS ALO EDIN (BSC) COLLEGE : HEALTH AND MEDICAL. 2022. |
[10, 16]
. Ethiopia is among the highest neonatal death contributing countries placed at the 6th position globally, the second in sub-Saharan Africa next to Nigeria, and the leading country in East Africa
| [17] | Okube OT, Komen M. Prevalence and Predictors of Neonatal Sepsis among Neonates Admitted at the Newborn Unit of Kenyatta National Hospital, Nairobi, Kenya. Open J Obstet Gynecol. 2020; 10(09): 1216–32. |
| [18] | Agnche Z, Yeshita HY, Gonete KA. Neonatal sepsis and its associated factors among neonates admitted to neonatal intensive care units in primary hospitals in central gondar zone, northwest ethiopia, 2019. Infect Drug Resist. 2020; 13: 3957–67. |
[17, 18]
. In Ethiopia, neonatal mortality per 1,000 live births has been reported as 30.5 at the 1st day, 61.7 at the 1st week, and 22.7 at the 2nd week of life
| [3] | Mengesha HG, Sahle BW. Cause of neonatal deaths in Northern Ethiopia: A prospective cohort study. BMC Public Health [Internet]. 2017; 17(1): 1–8. Available from:
http://dx.doi.org/10.1186/s12889-016-3979-8 |
| [19] | Abiy SA, Animut Y, Ambaw WM, Aragaw GM, Rade BK. Incidence of death and its predictors among neonates admitted with sepsis in referral hospitals, northwest Ethiopia, a prospective cohort study. Front Pediatr. 2023; 11(April): 1–11. |
[3, 19]
. Different studies on neonatal mortality in Ethiopia have reported the Jimma Zone, the Tigray region, the Dabat Health and Demographic Surveillance site (found in the Amhara region), and the neonatal care unit of St. Paul’s Hospital, or 10 per 1000 live births
| [12] | Gudayu TW, Zeleke EG, Lakew AM. Time to Death and its Predictors among Neonates Admitted in the Intensive Care Unit of the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia . Res Reports Neonatol. 2020; Volume 10: 1–10. |
| [15] | Seyoum K, Sahiledengle B, Kene C, Geta G, Gomora D, Ejigu N, et al. Determinants of neonatal sepsis among neonates admitted to neonatal intensive care units in ethiopian hospitals: A systematic review and meta-analysis. Heliyon [Internet]. 2023; 9(9): e20336. Available from:
https://doi.org/10.1016/j.heliyon.2023.e20336 |
| [17] | Okube OT, Komen M. Prevalence and Predictors of Neonatal Sepsis among Neonates Admitted at the Newborn Unit of Kenyatta National Hospital, Nairobi, Kenya. Open J Obstet Gynecol. 2020; 10(09): 1216–32. |
[12, 15, 17]
.
The 2016 Ethiopian Demographic and Health Survey (EDHS) reported a neonatal mortality rate of 29 per 1,000 live births, which is a reduction from the 2005 EDHS report of 39 per 1,000 live births and the 2011 EDHS report of 37 per 1,000 live births
. The 2019 Mini EDHS reported a neonatal mortality rate of 33/1000 live births, showing an increase in neonatal mortality from the 2016 EDHS report
.
Various efforts have been made by the Ethiopian government as well as supporting non-governmental and international organizations to reduce neonatal mortality in the country. To reduce neonatal mortality, Ethiopia is working to increase skilled birth assistance through facility and healthcare provider expansion, family planning service utilization, antenatal care utilization, and postnatal care utilization. Despite efforts by governmental and non-governmental organizations, neonatal mortality continues to be a public health problem, with a significant rise in mortality rates in Ethiopia
| [21] | Bitew ZW, Alemu A, Ayele EG, Jember DA, Haile MT, Worku T. Incidence Density Rate of Neonatal Mortality and Predictors in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. Int J Pediatr (United Kingdom). 2020. |
[21]
.
Although neonatal sepsis remains, a major cause of neonatal mortality in both developed and developing countries, limited evidence exists on the time to death and predictors of this serious public health problem, especially in Ethiopia. Based on the available evidence, there is no previous study on the time to death and its predictors among neonates admitted with neonatal sepsis in a study setting (West Arsi zone). Thus, determining the time to death and identifying its predictors among neonates admitted with sepsis is important for optimizing neonatal care. Therefore, this study aimed to assess the time to death and identify the predictive factors for death among neonates admitted with neonatal sepsis at public comprehensive and general hospitals in the West Arsi zone.
2. Conceptual Framework
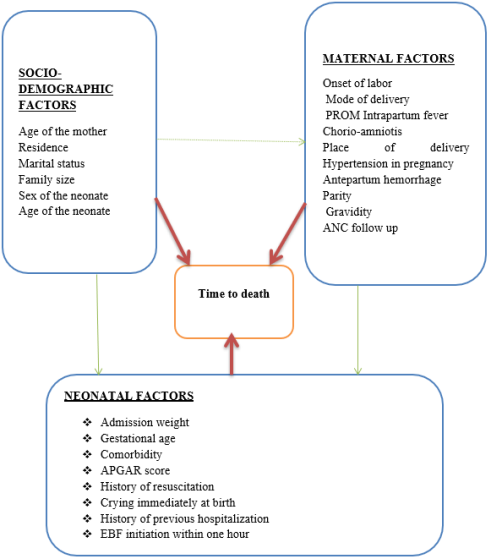
Conceptual framework for the time to death and its predictors among neonates admitted with neonatal sepsis at public comprehensive and general hospitals in the West Arsi zone, Southern Ethiopia (
Figure 1).
Figure 1. Conceptual framework for the time to death and its predictors among neonates admitted with neonatal sepsis at public comprehensive and general hospitals of West Arsi zone, Southern Ethiopia.
3. Methods and Materials
This study was conducted at public comprehensive and general hospitals in the West Arsi zone between May 30 and June 30, 2023. West Arsi zone officially estimated a population of 2,929,894 in mid-2022. The administrative center of this zone is Shashamane with an estimated 208,368 inhabitants by mid-2022. Other towns in this zone (with estimated populations in mid-2022) include Arsi Negele (98,114) in the Arsi Negele district, Dodola (43,186) in Dodola district, Asassa (42,867) in Gedeb Asasa district, Kofele (27,948) in Kofele district, and Adaba (25,098) in Adaba district
| [22] | Sên I, Øpuƒ SÍÑ. ¡õM-K eKQ´w. 1998. |
[22]
.
The zone has two general hospitals and one specialized comprehensive hospital. A Shashemene comprehensive specialized hospital is located in Shashemene town, which provides services to more than 2.1 million people from the catchment area. Melka Oda General Hospital is located in the town of Shashemene. The Dodola General Hospital has the same ward as the neonatal intensive care unit in the pediatric ward.
3.1. Study Design
An institution-based retrospective follow-up study was conducted.
3.2. Source Population
All neonates with neonatal sepsis were admitted to public comprehensive and general hospitals in the West Arsi zone from January 1, 2021 to December 31, 2022.
3.3. Study Population
All neonates admitted with neonatal sepsis to selected public comprehensive and general hospitals in the West Arsi zone from January 1, 2021 to December 31, 2022.
3.4. Eligibility Criteria
Inclusion criteria: All neonates admitted with neonatal sepsis and age less than or equal to 28 days at admission and were admitted during January 1, 2021 to December 31, 2022 was included in the study.
Exclusion criteria: Neonatal medical charts with incomplete records of major variables (admission date, survival status and discharge date) were excluded from the study. Neonates referred from the study hospitals were excluded.
3.5. Sample Size Determination
The sample size was determined using STATA version 18 by considering five variables from previous studies that are predictors of death in neonates with the assumption of a 5% significance level, a power of 80%, a 10% withdrawal rate and an equal proportion of subjects
| [11] | Abebia MT. Time to Death and Its Predictors Among Neonates Admitted With Neonatal Sepsis at Public Referral Hospitals of Bahir Dar City, Northwest Ethiopia, 2021 : Retrospective Cohort Study. Res Sq. 2021; 1–24. |
| [12] | Gudayu TW, Zeleke EG, Lakew AM. Time to Death and its Predictors among Neonates Admitted in the Intensive Care Unit of the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia . Res Reports Neonatol. 2020; Volume 10: 1–10. |
| [23] | Dessu S, Habte A, Melis T, Gebremedhin M. Survival Status and Predictors of Mortality among Newborns Admitted with Neonatal Sepsis at Public Hospitals in Ethiopia. Int J Pediatr (United Kingdom). 2020; 2020. |
[11, 12, 23]
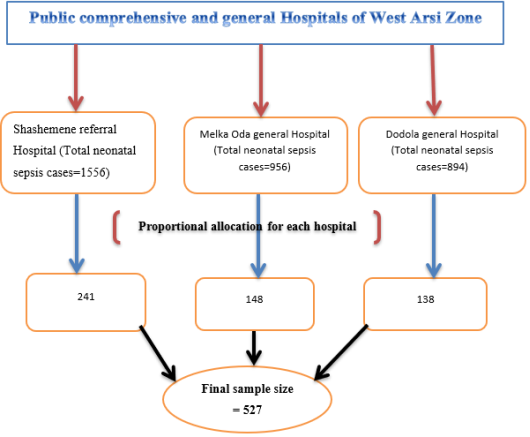
. The maximum sample size of was 527 taken as the final sample size (
Table 1).
Figure 2. Schematic representation of sampling procedure for time to death and its predictors among neonates admitted with neonatal sepsis at public comprehensive and general hospitals of West Arsi zone, Southern Ethiopia.
Table 1. Sample size calculation to determine time to death and its predictors among neonates admitted with neonatal sepsis at public comprehensive and general hospitals of West Arsi zone, Southern Ethiopia.
Variables | Power (%) | Hazard ratio | Probability of event | Sample size | |
Initiation of EBF (> one hour) | 80 | 3.4 | 0.0865 | 270 | (23) |
Onset of labor (induced) | 80 | 2.4 | 0.0865 | 527 | (23) |
Having comorbidity | 80 | 1.81 | 0.2816 | 352 | (11) |
PROM | 80 | 2.5 | 0.17 | 245 | (12) |
Preterm (earlier GA) | 80 | 2.9 | 0.17 | 182 | (12) |
Abbreviations: EBF; Exclusive Breast feeding, PROM; Premature Rupture of Membrane, GA; Gestational Age |
3.6. Sampling Technique
The medical record number (MRN) of all neonates with neonatal sepsis admitted for the last two years (January 1, 2021 to December 31, 2022) was obtained from the hospitals’ registration logbooks. A systematic random sampling technique was used to select neonatal charts after proportional allocation of the sample size to the hospitals according to their respective total neonatal sepsis cases (
Figure 2).
3.7. Data Collection Instruments and Procedure
A data collection tool was prepared as a checklist from the standardized Ethiopian National Neonatal and Delivery Registration Book to extract the required data from the selected charts. Data were collected using the Kobo toolbox from the first date of admission until death or censoring (lost to follow-up, improved, referred, or against medical treatment) or until the end of the follow-up period (28 days of age).
3.8. Dependent Variable: Time to Death
Independent variables: Socio demographic related factors included maternal age (years), maternal marital status, maternal occupation, residence, family size, neonatal age (days), and neonatal sex (male/female). Neonatal related factors included gestational age, comorbidity, admission weight, APGAR score (1st and 5th minutes), history of previous hospitalization, immediate crying at birth, history of resuscitation at birth, and exclusive breast feeding (EBF) initiation within one hour. Maternal medical and obstetric related factors included mode of onset of labor (spontaneous or induced), place of delivery, gravidity, parity, history of intrapartum fever, history of diagnosed chorioamniotis, mode of delivery, premature rupture of membrane (PROM), pregnancy-induced hypertension, history of urinary tract infection, and ANC follow-up.
3.9. Operational Definition
Neonate: a newborn from birth to 28 days old
| [12] | Gudayu TW, Zeleke EG, Lakew AM. Time to Death and its Predictors among Neonates Admitted in the Intensive Care Unit of the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia . Res Reports Neonatol. 2020; Volume 10: 1–10. |
[12]
.
Neonatal sepsis: Sepsis diagnosed and confirmed by physician among neonates
| [11] | Abebia MT. Time to Death and Its Predictors Among Neonates Admitted With Neonatal Sepsis at Public Referral Hospitals of Bahir Dar City, Northwest Ethiopia, 2021 : Retrospective Cohort Study. Res Sq. 2021; 1–24. |
[11]
.
Event: Death of neonate admitted with neonatal sepsis
| [11] | Abebia MT. Time to Death and Its Predictors Among Neonates Admitted With Neonatal Sepsis at Public Referral Hospitals of Bahir Dar City, Northwest Ethiopia, 2021 : Retrospective Cohort Study. Res Sq. 2021; 1–24. |
[11]
.
Censored: Neonates other than event/death (improved and discharged, referred to other health facilities, or against medical treatment)
| [12] | Gudayu TW, Zeleke EG, Lakew AM. Time to Death and its Predictors among Neonates Admitted in the Intensive Care Unit of the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia . Res Reports Neonatol. 2020; Volume 10: 1–10. |
[12]
.
Survival status: outcome of the neonate; death or censoring
| [12] | Gudayu TW, Zeleke EG, Lakew AM. Time to Death and its Predictors among Neonates Admitted in the Intensive Care Unit of the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia . Res Reports Neonatol. 2020; Volume 10: 1–10. |
[12]
.
Time to death: The time from admission to death in neonates with neonatal sepsis
| [11] | Abebia MT. Time to Death and Its Predictors Among Neonates Admitted With Neonatal Sepsis at Public Referral Hospitals of Bahir Dar City, Northwest Ethiopia, 2021 : Retrospective Cohort Study. Res Sq. 2021; 1–24. |
| [12] | Gudayu TW, Zeleke EG, Lakew AM. Time to Death and its Predictors among Neonates Admitted in the Intensive Care Unit of the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia . Res Reports Neonatol. 2020; Volume 10: 1–10. |
| [23] | Dessu S, Habte A, Melis T, Gebremedhin M. Survival Status and Predictors of Mortality among Newborns Admitted with Neonatal Sepsis at Public Hospitals in Ethiopia. Int J Pediatr (United Kingdom). 2020; 2020. |
[11, 12, 23]
.
Follow up time: Neonatal age (neonates with neonatal sepsis from admission until either event or censorship occurs)
| [11] | Abebia MT. Time to Death and Its Predictors Among Neonates Admitted With Neonatal Sepsis at Public Referral Hospitals of Bahir Dar City, Northwest Ethiopia, 2021 : Retrospective Cohort Study. Res Sq. 2021; 1–24. |
| [23] | Dessu S, Habte A, Melis T, Gebremedhin M. Survival Status and Predictors of Mortality among Newborns Admitted with Neonatal Sepsis at Public Hospitals in Ethiopia. Int J Pediatr (United Kingdom). 2020; 2020. |
[11, 23]
.
3.10. Data Quality Assurance
The data extraction tool (checklist) in the kobo toolbox was pretested among 5% of the study participants to ensure the quality of the data. The necessary modifications and corrections were made to standardize and ensure validity. The data collectors were experienced BSc nurses working in the NICU. Training was provided for two days on the purpose of the study, the data collection tool (checklist), the use of the kobo toolbox, how to send the data to the server, editing the finalized data, and ethical concerns during data collection. The supervisor monitored the data collection process of the data collectors.
3.11. Data Processing and Analysis
Data were collected using the kobo toolbox, checked for completeness, and edited, coded, and consistence checked using Microsoft Excel. The data were then imported into STATA version 18 and cleaned before analysis. Data presented as means, standard deviations, frequencies, and percentages, depending on the variable type. The incidence rate was estimated for the entire study period and specified intervals of hospital stay. Consequently, the neonatal mortality rate (NMR) within the study period was divided by the total number of neonatal days at hazard on follow-up and was reported per 1000 neonate days. The Kaplan-Meier survival curve with log-rank test was used to compare survival time between categories of different predictors and survival curve equality among strata, and a significant difference was determined using the log-rank test. Cumulative survival probability at certain time intervals was estimated using a life table. The Cox proportional hazard model and three parametric models (Weibull, Exponential & Gompertz) were fitted to identify predictors. The Weibull regression model was selected as the best model with the lowest Akaike information criteria (AIC) and Bayesian information criteria (BIC) (
Table 2). The goodness of fit was checked using the Cox-Snell residual. The Weibull regression model was used to analyze the relationship between the outcome and independent variables. Bi-variable analysis was performed for all variables, and variables in the bi-variable analysis of p-value ≤ 0.25 were as candidates for multivariable analysis. In the multivariable analysis, statistical significance was set at p < 0.05. Multi-collinearity was checked by the variance inflation factor (VIF), which was less than 10, indicating that there was no significant multi-collinearity among the variables. Associations were summarized using an adjusted hazard ratio (HR) with a 95%CI. Finally, the results were presented using statements, tables, and graphs.
Table 2. Models comparison for identifying predictors among neonates admitted with neonatal sepsis at public comprehensive and general hospitals of West Arsi zone, Southern Ethiopia.
Model | Null (11) | Model (11) | Df | AIC | BIC |
Weibull | -200.81 | -128.83 | 36 | 329.6652 | 483.2161 |
Gompertz | -208.2275 | -132.6934 | 36 | 337.3867 | 490.9376 |
Exponential | -220.9213 | -156.8553 | 35 | 383.7106 | 532.9962 |
Cox PH | -368.7674 | -300.1745 | 34 | 668.3489 | 813.3692 |
Abbreviations: AIC; Akaike information criteria, BIC; Bayesian information criteria, Cox PH; Cox proportional hazard |
4. Results
4.1. Socio-Demographic Characteristics
In total, 526 neonatal charts were reviewed, including 148 from Melka Oda General Hospital, 242 from Shashemene Referral Hospital, and 136 from Dodola General Hospital. Approximately half of the 258 neonates (49.05%) were male. Approximately 460 (87.45%) neonates were aged less than seven days. Among the neonates who died, 56 (83.6%) died within the first seven days of life. The mean (±SD) age of the mothers was 28.3±4.58 years and more than three-fourths of the 435 (82.70%) mothers were 20 to 34 years old, and more than half 293 (55.7%) were urban residents (
Table 3).
Table 3. Socio-demographic characteristics of neonates admitted with neonatal sepsis at public comprehensive and general hospitals of West Arsi zone, Southern Ethiopia (N=526).
Variables | Category | Status of the neonates | Total (%) |
Death (%) | Censored (%) |
Hospital | Melka Oda | 21 (14.2) | 127 (85.8) | 148 (28.1) |
Shashemene | 31 (12.8) | 211 (87.2) | 242 (46.0) |
Dodola | 15 (11.0) | 121 (89) | 136 (25.9) |
Neonatal age (day) | <7 | 56 (12.2) | 404 (87.8) | 460 (87.5) |
7-28 | 11 (16.7) | 55 (83.3) | 66 (12.5) |
Maternal age (year) | <=19 | 5 (20.8) | 19 (79.2) | 24 (4.6) |
20-34 | 57 (12.9) | 382 (87.1) | 439 (82.7) |
≥35 | 5 (7.9) | 58 (92.1) | 63 (12.7) |
Neonatal sex | Male | 42 (16.3) | 216 (83.7) | 258 (49.1) |
Female | 25 (9.3) | 243 (92.7) | 268 (50.9) |
Residence | Urban | 43 (14.7) | 250 (85.3) | 293 (55.7) |
Rural | 24 (10.3) | 209 (89.7) | 233 (44.3) |
4.2. Neonatal Related Characteristics
The mean (±SD) weight of neonates at admission was 2716.96 ± 657.42 grams, and the majority 363 (69.01%) of the neonates had an admission weight greater than 2500 grams. Regarding gestational age, the mean (±SD) gestational age was 36.84±1.35 weeks, with a minimum of 29 and a maximum of 41 weeks. Among the neonates who died, 48 (71.6%) had respiratory distress during hospital admission, and more than half (56.7%) of the dead neonates did not initiate breastfeeding within one hour of birth (
Table 4).
Table 4. Neonatal characteristics of neonates admitted with neonatal sepsis at public comprehensive and general hospitals of West Arsi zone, Southern Ethiopia (N=526).
Characteristics | Category | Status of the neonates | Total (%) |
Death (%) | Censored (%) |
Gestational age (weeks) | <37 | 26 (31.7) | 56 (68.3) | 82 (15.6) |
≥37 | 41 (9.2) | 403 (90.8) | 444 (84.4) |
Weight at admission (gram) | <2500 | 36 (22.1) | 127 (77.9) | 163 (30.9) |
≥2500 | 31 (8.5) | 332 (91.5) | 363 (69.1) |
Respiratory distress during admission | Yes | 48 (28.7) | 119 (71.3) | 167 (31.7) |
No | 19 (5.3) | 340 (94.7) | 359 (68.3) |
BF initiated within one hour | Yes | 29 (6.6) | 410 (93.4) | 439 (83.5) |
No | 38 (43.7) | 49 (56.3) | 87 (16.5) |
History of previous hospitalization | Yes | 23 (18.7) | 100 (81.3) | 123 (23.4) |
No | 44 (10.9) | 359 (89.1) | 403 (76.6) |
Comorbidity | Yes | 41 (23.7) | 132 (76.3) | 173 (32.9) |
No | 26 (7.4) | 327 (92.6) | 353 (67.1) |
Abbreviations: BF; Breast feeding |
4.3. Obstetrics Characteristics and Medical Conditions Among Mothers
Almost all the mothers had at least one antenatal care visit. The majority 45 (86.9%) of dead neonates were born to multi gravida mothers. Pregnancy complications were reported in 117 (22.2%) mothers, and nearly three-fourths of the 25 (71.4%) neonates who died were born to mothers with preeclampsia. Four hundred and eight mothers had a spontaneous onset of labor (
Table 5).
Table 5. Obstetrics characteristics and medical conditions among mothers at public comprehensive and general hospitals of West Arsi zone, Southern Ethiopia (N=526).
Characteristics | Category | Status of the neonates | Total (%) |
Death (%) | Censored (%) |
Gravidity | Prim gravid a | 15 (21.7) | 54 (78.3) | 69 (13.1) |
Multi gravid a | 52 (11.4) | 405 (88.6) | 457 (86.9) |
ANC follow up | Yes | 60 (11.8) | 447 (88.2) | 507 (96.4) |
No | 7 (36.8) | 12 (63.2) | 19 (3.6) |
Number of ANC visit | Once | 0 (0.0) | 4 (100) | 4 (0.8) |
Twice | 3 (15.8) | 16 (84.2) | 19 (3.6) |
Three times | 10 (10.3) | 87 (89.7) | 97 (18.4) |
Four times | 47 (12.1) | 340 (87.9) | 387 (73.6) |
Onset of labor | Spontaneous | 59 (12.2) | 424 (87.8) | 483 (91.8) |
Induced | 8 (18.6) | 35 (81.4) | 43 (8.2) |
History of PROM | Yes | 48 (20.2) | 190 (79.8) | 238 (45.2) |
No | 19 (6.6) | 269 (93.4) | 288 (54.8) |
Place of delivery | Health institution | 63 (12.6) | 437 (87.4) | 500 (95.1) |
Home | 4 (15.4) | 22 (84.6) | 26 (4.9) |
Mode of delivery | SVD | 55 (11.5) | 422 (88.5) | 477 (90.7) |
Instrumental | 3 (14.3) | 18 (85.7) | 21 (3.9) |
CS | 9 (32.1) | 19 (67.9) | 28 (5.3) |
Type of pregnancy | Singleton | 66 (12.9) | 446 (87.1) | 512 (97.3) |
Multiple | 1 (7.1) | 13 (92.9) | 14 (2.7) |
History of intra partum fever | Yes | 52 (14.4) | 308 (85.6) | 360 (68.4) |
No | 15 (9.0) | 151 (91.0) | 166 (31.6) |
Maternal health problem | Yes | 34 (29.1) | 83 (70.1) | 117 (22.2) |
No | 33 (8.1) | 376 (91.9) | 409 (77.8) |
Type of health problem | Preeclampsia | 25 (42.4) | 34 (57.6) | 59 (50.0) |
UTI | 1 (5.3) | 18 (94.7) | 19 (16.1) |
APH | 7 (20.6) | 27 (79.4) | 34 (28.8) |
Other | 2 (33.3) | 4 (66.7) | 6 (5.1) |
Abbreviations: ANC; Antenatal Care, APH; Antepartum Hemorrhage, CS; Cesarean Section, PROM; Premature Rupture of Membrane, SVD; Spontaneous Vaginal Delivery, UTI; Urinary Tract Infection |
4.4. Status of Neonates with Neonatal Sepsis
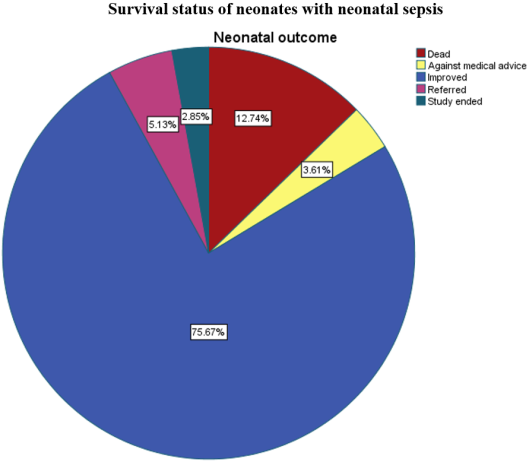
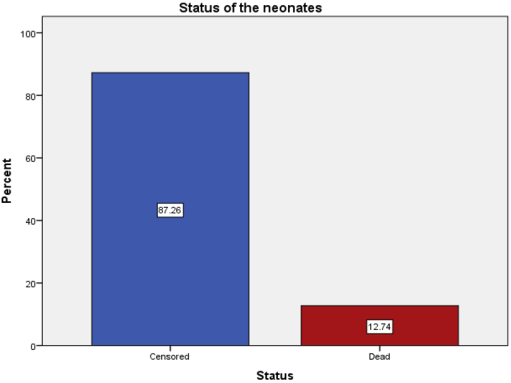
During the follow-up period, 67 (12.7%) (95% CI: 10–15.9) neonates died, 398 (75.67%) improved and were discharged, 27 (5.13%) were referred to other hospitals, 19 (3.61%) left the hospital against medical advice, and 15 (2.85%) ended the study without the development of events (
Figures 3 & 4).
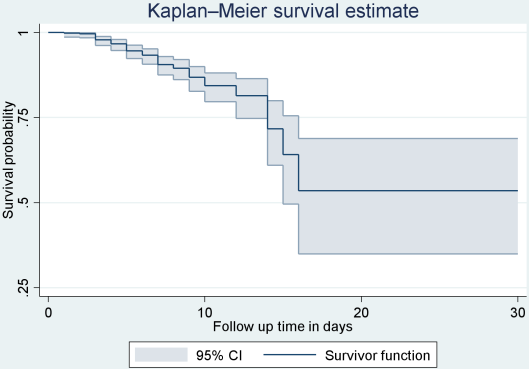
The overall incidence of neonatal mortality was 16.1 per 1000 neonatal days, and the neonatal mortality rate (NMR) was 128 per 1000 neonates admitted with sepsis. Neonates were followed for different periods: a minimum of 1 day and a maximum of 28 days, with a mean follow-up period of 7.9 (95% CI: 7.63, 8.19) days. The total time at risk for the 526 neonates was 4161 neonatal days. The cumulative probabilities of survival at the fourth, 8th, and 28th days was 97.8% (95%CI: 96.2–98.8), 89.4% (95%CI: 85.9–92.1), and 48.2% (95%CI: 27.5–66.2), respectively (
Table 6).
Figure 3. Proportion of neonatal outcome among neonates admitted with neonatal sepsis at public comprehensive and general hospitals of West Arsi zone, Southern Ethiopia.
Figure 4. Status of the neonates among neonates admitted with neonatal sepsis at public comprehensive and general hospitals of West Arsi zone, Southern Ethiopia.
Table 6. Survival probability of neonates admitted with neonatal sepsis at public comprehensive and general hospitals of West Arsi zone, Southern Ethiopia (N=526).
Interval in days | Total at the beginning | Death | Lost to follow up | Survival probability % | 95% CI for Survival probability % |
0 | 4 | 526 | 11 | 19 | 97.8 | 96.2 | 98.8 |
5 | 8 | 496 | 33 | 229 | 89.4 | 85.9 | 92.1 |
9 | 12 | 234 | 12 | 166 | 82.3 | 76.9 | 86.5 |
13 | 16 | 56 | 9 | 35 | 63.1 | 50.3 | 73.4 |
17 | 20 | 12 | 2 | 7 | 48.2 | 27.5 | 66.2 |
21 | 24 | 3 | 0 | 1 | 48.2 | 27.5 | 66.2 |
25 | 28 | 2 | 0 | 2 | 48.2 | 27.5 | 66.2 |
Abbreviations: CI; Confidence Interval |
In this study, because the maximum observation time was censored, the mean time to death was an appropriate measure of the central tendency. Accordingly, the mean time to death among neonates was 7.9 days (95% CI: 7.63, 8.19).
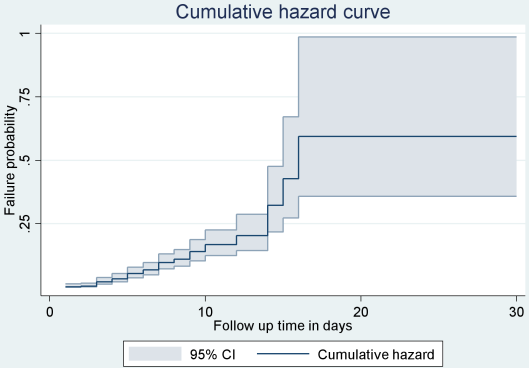
The probability of survival and death in neonates with neonatal sepsis during the follow-up period is also presented using survival and failure curves. Accordingly, during the first 15 days there is higher probability of death, between days 10 and 15 the probability of death continued and the graph moved upward. On the remaining days of the follow-up period, especially starting from day 16, the graph became straight, indicating that the likelihood of death in neonates with neonatal sepsis remained stable, with almost no deaths occurring after day 20 (
Figures 5 & 6).
Figure 5. Overall Kaplan-Meir survival estimate of neonates admitted with neonatal sepsis at public comprehensive and general hospitals of West Arsi zone, Southern Ethiopia.
Figure 6. Overall Cumulative hazard estimate of neonates admitted with neonatal sepsis at public comprehensive and general hospitals of West Arsi zone, Southern Ethiopia.
4.5. Log-rank Estimate of Mortality Across Predictors
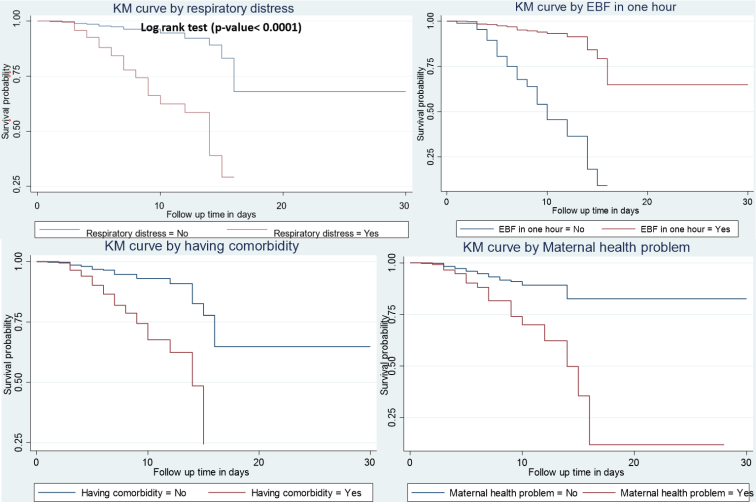
The log-rank test estimates between the categories of different predictor variables revealed that the survival patterns among neonates were significantly different. The Kaplan-Meier method, together with the log-rank test, shows the effect of each predictor on neonatal mortality. (
Table 7 &
Figure 7)
Table 7. Log-rank test for equality of different categorical predictors of neonates admitted with neonatal sepsis at public comprehensive and general hospitals of West Arsi zone, Southern Ethiopia (N=526).
Variables | Category | X2 | P-value |
ANC follow up | Yes | 7.57 | 0.0059 |
No |
Gravidity | Primi gravida | 5.63 | <0.0001 |
Multi gravida |
Gestational age (weeks) | <37 | 27.95 | <0.0001 |
≥37 |
Respiratory distress during admission | Yes | 65.56 | <0.0001 |
No |
BF initiated within one hour | Yes | 104.5 | <0.0001 |
No |
History of previous hospitalization | Yes | 8.45 | 0.0036 |
No |
Having comorbidity | Yes | 36.54 | <0.0001 |
No |
History of PROM | Yes | 21.05 | <0.0001 |
No |
Mode of delivery | SVD | 10.46 | 0.0046 |
Instrumental |
Cesarean section |
Maternal health problem | Yes | 26.88 | <0.0001 |
No |
Abbreviations: ANC; Antenatal Care, BF; Breast feeding, PROM; Premature Rupture of Membrane, SVD; Spontaneous Vaginal Delivery NB: X2 = Chi-square |
Figure 7. Kaplan-Meir curve test for equality of different categorical predictors of neonates admitted with neonatal sepsis at public comprehensive and general hospitals of West Arsi zone, Southern Ethiopia.
4.6. Model Comparison and Model Fitness
The Cox proportional hazard model and three parametric models (Weibull, Exponential & Gompertz) were fitted to identify predictors. The Weibull regression model was selected as the best model with the lowest Akaike information criteria (AIC) and Bayesian information criteria (BIC) (
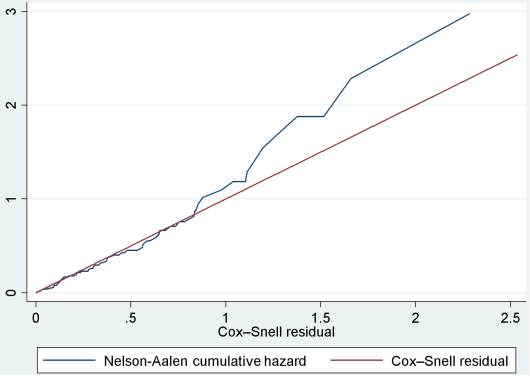
Table 2). The Weibull regression model was used to analyze the relationship between the outcome and independent variables. Goodness of fit was checked using the Cox–Snell residual (
Figure 8).
Figure 8. Cox-Snell residual Nelson -Aalen cumulative hazard graph on neonates admitted with neonatal sepsis at public comprehensive and general hospitals of West Arsi zone, Southern Ethiopia.
4.7. Predictors of Neonatal Mortality
Bivariate analysis showed that neonatal sex, residence, maternal age, admission weight, respiratory distress during admission, initiation of breastfeeding within one hour, history of previous hospitalization, comorbidity, gravidity, history of premature rupture of membrane, place of delivery, mode of delivery, and maternal health problems during pregnancy were predictor variables with a p-value < 0.25 and were significantly associated with neonatal death.
Multivariable regression results revealed that respiratory distress during admission, initiation of breastfeeding within one hour of birth, gravidity, and maternal health problems during pregnancy were significant predictors of neonatal death.
Neonates without respiratory distress during admission had a 63% reduced risk of death compared to those with respiratory distress at admission (Adjusted Hazard Ratio (AHR): 0.37; 95% CI: 0.18, 0.77). Neonates who did not initiate breastfeed within one hour of birth were three times more likely to die than their counterparts were (AHR: 3.15; 95% CI: 1.38, 7.18). The hazard of death in neonates born from multi gravida mothers was 63% lower than that in neonates born from gravida mothers (AHR: 0.37; 95% CI: 0.15, 0.88). Neonates born from mothers without maternal health problems had a 56% decreased hazard of death compared to neonates born from mothers with maternal health problems (AHR: 0.44, 95% CI: 0.25, 0.79) (
Table 8).
Table 8. Predictors of neonatal mortality among neonates admitted with neonatal sepsis at public comprehensive and general hospitals of West Arsi zone, Southern Ethiopia (N=526).
Variable | Category | Survival status | AHR 95% CI | P-value |
Death (%) | Censored (%) |
Neonatal sex | Male | 42 (16.3) | 216 (83.7) | 1 | 0.115 |
Female | 25 (9.3) | 243 (92.7) | 0.61 (0.33, 1.13) |
Maternal age (year) | <20 | 5 (20.8) | 19 (79.2) | 1 | |
20-34 | 53 (12.2) | 382 (87.8) | 2.64 (0.56, 12.43) | 0.218 |
≥35 | 9 (13.4) | 58 (86.6) | 8.93 (1.39, 57.42) | 0.021 |
Residence | Urban | 43 (14.7) | 250 (85.3) | 1 | |
Rural | 24 (10.3) | 209 (89.7) | 0.69 (0.38, 1.28) | 0.242 |
Weight at admission (grams) | <2500 | 36 (22.1) | 127 (77.9) | 1 | |
≥2500 | 31 (8.5) | 332 (91.5) | 0.56 (0.28, 1.13) | 0.108 |
Gestational age (week) | <37 | 26 (31.7) | 56 (68.3) | 1 | |
≥37 | 41 (9.2) | 403 (90.8) | 1.12 (0.44, 2.86) | 0.807 |
Respiratory distress during admission | Yes | 48 (28.7) | 119 (71.3) | 1 | |
No | 19 (5.3) | 340 (94.7) | 0.37 (0.18, 0.77) | 0.008 |
Initiation of breast feeding within one hour | Yes | 29 (6.6) | 410 (93.4) | 1 | |
No | 38 (43.7) | 49 (56.3) | 3.15 (1.38, 7.18) | 0.006 |
History of previous hospitalization | Yes | 23 (18.7) | 100 (81.3) | 1 | |
No | 44 (10.9) | 359 (89.1) | 0.59 (0.31, 1.12) | 0.108 |
Comorbidity | Yes | 41 (23.7) | 132 (76.3) | 1 | |
No | 26 (7.4) | 327 (92.6) | 0.58 (0.30, 1.11) | 0.100 |
Gravidity | Primi gravida | 15 (21.7) | 54 (78.3) | 1 | |
Multi gravida | 52 (11.4) | 405 (88.6) | 0.37 (0.15, 0.88) | 0.025 |
Parity | Prim para | 42 (13.9) | 259 (86.1) | 1 | |
Multi para | 25 (11.1) | 200 (88.9) | 1.06 (0.52, 2.17) | 0.862 |
ANC follow up | Yes | 60 (11.8) | 447 (88.2) | 1 | |
No | 7 (36.8) | 12 (63.2) | 1.17 (0.32, 4.24) | 0.814 |
Maternal health problem during pregnancy | Yes | 34 (29.1) | 83 (70.1) | 1 | |
No | 33 (8.1) | 376 (91.9) | 0.44 (0.25, 0.79) | 0.006 |
Abbreviations: AHR; Adjusted Hazard Ratio, ANC; Antenatal Care, CI; Confidence Interval |
5. Discussion
In this study, out of 526 neonates with neonatal sepsis 67 (12.7%) (95% CI: 10, 15.9) neonates were died. This is consistent with the findings from studies conducted in Bahir Dar city, with 58 (11.6%) (95% CI: 9.07, 14.73) neonates died during the follow-up period
| [11] | Abebia MT. Time to Death and Its Predictors Among Neonates Admitted With Neonatal Sepsis at Public Referral Hospitals of Bahir Dar City, Northwest Ethiopia, 2021 : Retrospective Cohort Study. Res Sq. 2021; 1–24. |
[11]
. This might be due to the related socioeconomic status of the two study populations and the same person-time measurements of the two studies.
The overall incidence of neonatal mortality was 16.1 per 1000 neonatal days, and the neonatal mortality rate (NMR) was 128 per 1000 neonates admitted with sepsis. This is lower than the results of studies conducted in Gondar
| [12] | Gudayu TW, Zeleke EG, Lakew AM. Time to Death and its Predictors among Neonates Admitted in the Intensive Care Unit of the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia . Res Reports Neonatol. 2020; Volume 10: 1–10. |
[12]
and study conducted at Eastern Ethiopia
| [24] | Jibro U, Desalew A, Ayana GM, Tura AK. Time to Death and Its Predictors among Neonates Hospitalized with Sepsis in Eastern Ethiopia. Biomed Res Int. 2024; 2024. |
[24]
. This could be explained by the difference in the source population, as the current study used neonates with sepsis instead of all neonates
| [12] | Gudayu TW, Zeleke EG, Lakew AM. Time to Death and its Predictors among Neonates Admitted in the Intensive Care Unit of the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia . Res Reports Neonatol. 2020; Volume 10: 1–10. |
[12]
.
The cumulative probabilities of survival at the fourth, 8th and 28th days was 97.8% (95%CI: 96.2–98.8), 89.4% (95%CI: 85.9–92.1) and 48.2% (95%CI: 27.5–66.2) respectively. This is in line with a study conducted in southern Ethiopia, where the cumulative proportion of survivors at the end of the fourth day was 99.5% and 98.2% at the end of the fifth day
| [23] | Dessu S, Habte A, Melis T, Gebremedhin M. Survival Status and Predictors of Mortality among Newborns Admitted with Neonatal Sepsis at Public Hospitals in Ethiopia. Int J Pediatr (United Kingdom). 2020; 2020. |
[23]
. A possible explanation for this finding could be related to socioeconomic status and use of the same methods.
In this study, the overall incidence of neonatal mortality was 16.1 per 1000 neonatal days. This was slightly higher than that in a study conducted in southern Ethiopia (Arbaminch, Sawla, and Chencha), with an incidence rate of mortality among neonates admitted with neonatal sepsis of 14.57 per 1000 neonate days
| [23] | Dessu S, Habte A, Melis T, Gebremedhin M. Survival Status and Predictors of Mortality among Newborns Admitted with Neonatal Sepsis at Public Hospitals in Ethiopia. Int J Pediatr (United Kingdom). 2020; 2020. |
[23]
, and a study conducted at Boru Meda General Hospital
| [25] | Awoke AB, Tilahun F, Hassen S, Bialfew F, Molla A, Yimam AM. Time to death and its predictors among neonates admitted to the neonatal intensive care unit at Boru Meda General Hospital, Northeast Ethiopia. Sci Rep. 2025; 15(1): 1–13. |
[25]
. A possible explanation for this difference might be the difference in sample size, as the current study used a large sample size.
Also lower than the study done at Gondar University Specialized Hospital indicates that the neonatal mortality rate was 173 per 1000 live births, and the overall incidence rate in this study was 26.56 per 1000 neonatal days for birth to death and 34.69 per 1000 neonatal admission days for admission to death
| [12] | Gudayu TW, Zeleke EG, Lakew AM. Time to Death and its Predictors among Neonates Admitted in the Intensive Care Unit of the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia . Res Reports Neonatol. 2020; Volume 10: 1–10. |
[12]
. This might be due to differences in the follow-up time and study period.
According to this study, respiratory distress was a significant predictor of neonatal mortality. Neonates without respiratory distress during admission had a 63% reduced risk of death compared with those with respiratory distress at admission. This finding is supported by studies conducted in Bahir Dar
| [7] | Tewabe T, Mohammed S, Tilahun Y, Melaku B, Fenta M, Dagnaw T, et al. Clinical outcome and risk factors of neonatal sepsis among neonates in Felege Hiwot referral Hospital, Bahir Dar, Amhara Regional State, North West Ethiopia 2016: A retrospective chart review. BMC Res Notes. 2017; 10(1): 1–7. |
[7]
, northwest Ethiopia
| [19] | Abiy SA, Animut Y, Ambaw WM, Aragaw GM, Rade BK. Incidence of death and its predictors among neonates admitted with sepsis in referral hospitals, northwest Ethiopia, a prospective cohort study. Front Pediatr. 2023; 11(April): 1–11. |
[19]
, and Northeast Ethiopia
| [26] | Wudu MA, Bekalu YE, Wondifraw EB, Birhanu TA, Hailu MK, Belete MA, et al. Time to death and its predictors among neonates admitted with sepsis in neonatal intensive care unit at comprehensive specialized hospitals in Northeast Ethiopia. Front Pediatr. 2024; 12(April). |
[26]
. This might be explained by the fact that respiratory distress is a sign of severe neonatal sepsis. This indicates a higher probability of death.
The initiation of breastfeeding within one hour of birth is a significant predictor of neonatal mortality. Neonates who did not initiate breastfeed within one hour of birth were three times more likely to die than their counterparts were. This finding is consistent with those of studies conducted in Bahir Dar
| [11] | Abebia MT. Time to Death and Its Predictors Among Neonates Admitted With Neonatal Sepsis at Public Referral Hospitals of Bahir Dar City, Northwest Ethiopia, 2021 : Retrospective Cohort Study. Res Sq. 2021; 1–24. |
[11]
, Southern Ethiopia
| [23] | Dessu S, Habte A, Melis T, Gebremedhin M. Survival Status and Predictors of Mortality among Newborns Admitted with Neonatal Sepsis at Public Hospitals in Ethiopia. Int J Pediatr (United Kingdom). 2020; 2020. |
[23]
, and Eastern Ethiopia
| [24] | Jibro U, Desalew A, Ayana GM, Tura AK. Time to Death and Its Predictors among Neonates Hospitalized with Sepsis in Eastern Ethiopia. Biomed Res Int. 2024; 2024. |
[24]
. This result may be explained by the fact that many defense factors in the mother's milk include large amounts of secretory Immunoglobulin A antibodies produced by lymphocytes that migrate from the mother's gut to the mammary glands. Thus, breastfeeding modulates early exposure of the neonate's intestinal mucosa to microbes and limits bacterial translocation through the gut mucosa; neonates who did not receive feeding within one hour did not benefit from the mother’s milk. Therefore, early breastfeeding initiation provides adequate nutrition at an appropriate time and immunological value from the first milk (colostrum), which prevents hypothermia and hypoglycemia.
Gravidity is another predictor of neonatal mortality due to sepsis. Neonates born to multi-gravid mothers had a 63% lower risk of death than neonates born to prim-gravid mothers. This finding is supported by studies conducted at Bashir Dar Public Hospitals and Iraq
| [11] | Abebia MT. Time to Death and Its Predictors Among Neonates Admitted With Neonatal Sepsis at Public Referral Hospitals of Bahir Dar City, Northwest Ethiopia, 2021 : Retrospective Cohort Study. Res Sq. 2021; 1–24. |
| [13] | Yamey G, Horváth H, Schmidt L, Myers J, Brindis CD. Reducing the global burden of Preterm Birth through knowledge transfer and exchange: A research agenda for engaging effectively with policymakers. Reprod Health [Internet]. 2016; 13(1): 1–9. Available from:
http://dx.doi.org/10.1186/s12978-016-0146-8 |
[11, 13]
. This might be because prim gravid mothers are more prone to maternal complication than multi gravid mothers.
This study identified maternal health problems as significant predictors of neonatal mortality. Neonates born to mothers without maternal health problems had a 56% lower risk of death than those born to mothers with health problems. This finding is consistent with that of a study conducted in Central India
| [7] | Tewabe T, Mohammed S, Tilahun Y, Melaku B, Fenta M, Dagnaw T, et al. Clinical outcome and risk factors of neonatal sepsis among neonates in Felege Hiwot referral Hospital, Bahir Dar, Amhara Regional State, North West Ethiopia 2016: A retrospective chart review. BMC Res Notes. 2017; 10(1): 1–7. |
| [10] | Mustefa A, Abera A, Aseffa A, Abathun T, Degefa N, Tadesse H, et al. Prevalence of neonatal sepsis and associated factors amongst neonates admitted in arbaminch general hospital, arbaminch, southern Ethiopia, 2019. J Pediatr Neonatal Care. 2020; 10(1): 1–7. |
[7, 10]
. This finding may be attributable to the well-established relationship between maternal health complications and adverse neonatal outcomes.
6. Limitations of the Study
Because the study reviewed secondary data, important socio-demographic predictors, such as maternal educational status, income, maternal occupation, and family size were excluded from the study. Event documentation may differ depending on the service provider's documentation practice and data utilization culture, leading to an underestimation of problems. A lack of literature on similar studies, both nationally and internationally, for discussion and selection bias might have been present during chart selection, because charts with incomplete data were excluded from the study.
7. Strengths of the Study
Parametric survival model, health professionals working in the same unit for data collection, the neonatal intensive care unit and the latest version of the Stata version 18 are considered as the strength of the study.
8. Conclusion and Recommendation
This study revealed that among neonates, 67 (12.7%) (95% CI: 10–15.9) died during the follow-up period.
Respiratory distress during admission, initiation of breastfeeding within one hour of birth, gravidity, and maternal health problems during pregnancy were predictors of mortality among neonates admitted with neonatal sepsis.
The Federal Ministry of Health of Ethiopia should pay more attention to the prevention, early diagnosis, and management of sepsis and maternal health problems.
Hospitals’ administrative staff and health bureaus should encourage healthcare providers working in the NICU to pay special attention to neonates with neonatal sepsis during their first seven days of life.
Initiation of breastfeeding within one hour, proper management of neonates with respiratory distress, and early identification and management of maternal health problems should be the focus of healthcare providers and we recommend that future researchers use prospective cohort study design to overcome the limitations of retrospective cohort study design.
Abbreviations
ANC | Antenatal Care |
AHR | Adjusted Hazard Ratio |
APGAR | Appearance Pulse Grimace, Activity Respiration |
CI | Confidence Interval |
CHR | Crude Hazard Ratio |
EBF | Exclusive Breast Feeding |
EDHS | Ethiopian Demographic and Health Survey |
EONS | Early Onset Neonatal Sepsis |
ERB | Ethical Review Board |
IDR | Incidence Density Rate |
LONS | Late-onset Neonatal Sepsis |
NICU | Neonatal Intensive Care Unit |
PROM | Premature Rupture of Membrane |
SSA | sub-Saharan Africa |
UTI | Urinary Tract Infection |
WHO | World Health Organization |
Acknowledgments
First, we would like to express our gratitude to the College of Medicine and Health Science of Arba Minch University. We also thank the hospital staff, data collectors, and the participants for their cooperation.
Author Contributions
Mamud Umer Wakeyo: Conceptualization, Data curation, Formal Analysis, Supervison, Visualization
Mesfin Kote: Conceptualization, Data curation, Resources, Supervision
Zeleke Girma: Conceptualization, Data curation, Formal Analysis, Supervision, Visualization
Funding
The authors received no specific funding for this work.
Data Availability Statement
Data will be made available upon request from the corresponding authors.
Conflicts of Interest
The authors declare that they have no competing interests.
References
| [1] |
Degefa N, Diriba K, Girma T, Kebede A, Senbeto A, Eshetu E, et al. Knowledge about Neonatal Danger Signs and Associated Factors among Mothers Attending Immunization Clinic at Arba Minch General Hospital, Southern Ethiopia: A Cross-Sectional Study. Biomed Res Int. 2019; 2019: 1–8.
|
| [2] |
Geta T, Kassa T, Israel E. Magnitude of sepsis and its predictors among neonates admitted to neonatal intensive care unit at Hawassa University comprehensive specialized hospital in Southern Ethiopia 2022. 2022; 12(3).
|
| [3] |
Mengesha HG, Sahle BW. Cause of neonatal deaths in Northern Ethiopia: A prospective cohort study. BMC Public Health [Internet]. 2017; 17(1): 1–8. Available from:
http://dx.doi.org/10.1186/s12889-016-3979-8
|
| [4] |
Getabelew A, Aman M, Fantaye E, Yeheyis T. Prevalence of Neonatal Sepsis and Associated Factors among Neonates in Neonatal Intensive Care Unit at Selected Governmental Hospitals in Shashemene Town, Oromia Regional State, Ethiopia, 2017. Int J Pediatr. 2018; 2018: 1–7.
|
| [5] |
Lobo BBP, Marba STM, Machado HC, Caldas JPS. Neonatal Sequential Organ Failure Assessment as a late-onset sepsis mortality predictor in very low birth weight newborns: a Brazilian cohort study. Eur J Pediatr. 2022; 181(10): 3767–74.
|
| [6] |
Ahmed I, Ali SM, Amenga-Etego S, Ariff S, Bahl R, Baqui AH, et al. Population-based rates, timing, and causes of maternal deaths, stillbirths, and neonatal deaths in south Asia and sub-Saharan Africa: a multi-country prospective cohort study. Lancet Glob Heal. 2018; 6(12): e1297–308.
|
| [7] |
Tewabe T, Mohammed S, Tilahun Y, Melaku B, Fenta M, Dagnaw T, et al. Clinical outcome and risk factors of neonatal sepsis among neonates in Felege Hiwot referral Hospital, Bahir Dar, Amhara Regional State, North West Ethiopia 2016: A retrospective chart review. BMC Res Notes. 2017; 10(1): 1–7.
|
| [8] |
Simonsen KA, Anderson-Berry AL, Delair SF, Dele Davies H. Early-onset neonatal sepsis. Clin Microbiol Rev. 2014; 27(1): 21–47.
|
| [9] |
Shehab El-Din EMR, El-Sokkary MMA, Bassiouny MR, Hassan R. Epidemiology of neonatal sepsis and implicated pathogens: A Study from Egypt. Biomed Res Int. 2015; 2015.
|
| [10] |
Mustefa A, Abera A, Aseffa A, Abathun T, Degefa N, Tadesse H, et al. Prevalence of neonatal sepsis and associated factors amongst neonates admitted in arbaminch general hospital, arbaminch, southern Ethiopia, 2019. J Pediatr Neonatal Care. 2020; 10(1): 1–7.
|
| [11] |
Abebia MT. Time to Death and Its Predictors Among Neonates Admitted With Neonatal Sepsis at Public Referral Hospitals of Bahir Dar City, Northwest Ethiopia, 2021 : Retrospective Cohort Study. Res Sq. 2021; 1–24.
|
| [12] |
Gudayu TW, Zeleke EG, Lakew AM. Time to Death and its Predictors among Neonates Admitted in the Intensive Care Unit of the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia . Res Reports Neonatol. 2020; Volume 10: 1–10.
|
| [13] |
Yamey G, Horváth H, Schmidt L, Myers J, Brindis CD. Reducing the global burden of Preterm Birth through knowledge transfer and exchange: A research agenda for engaging effectively with policymakers. Reprod Health [Internet]. 2016; 13(1): 1–9. Available from:
http://dx.doi.org/10.1186/s12978-016-0146-8
|
| [14] |
Sisay EA, Mengistu BL, Taye WA, Fentie AM, Yabeyu AB. Length of Hospital Stay and Its Predictors Among Neonatal Sepsis Patients: A Retrospective Follow-Up Study. Int J Gen Med. 2022; 15(November): 8133–42.
|
| [15] |
Seyoum K, Sahiledengle B, Kene C, Geta G, Gomora D, Ejigu N, et al. Determinants of neonatal sepsis among neonates admitted to neonatal intensive care units in ethiopian hospitals: A systematic review and meta-analysis. Heliyon [Internet]. 2023; 9(9): e20336. Available from:
https://doi.org/10.1016/j.heliyon.2023.e20336
|
| [16] |
SCHOOL OF GRADUAATE STUDIES SURVIVAL STATUS AND ITS PREDICTORS AMONG PRETERM NEONATES ADMITTED TO NEONATAL INTENSIVE CARE UNITS AT PUBLIC HOSPITALS IN WEST GUJI AND BORENA ZONES, SOUTHERN ETHIOPIA MPH THESIS ALO EDIN (BSC) COLLEGE : HEALTH AND MEDICAL. 2022.
|
| [17] |
Okube OT, Komen M. Prevalence and Predictors of Neonatal Sepsis among Neonates Admitted at the Newborn Unit of Kenyatta National Hospital, Nairobi, Kenya. Open J Obstet Gynecol. 2020; 10(09): 1216–32.
|
| [18] |
Agnche Z, Yeshita HY, Gonete KA. Neonatal sepsis and its associated factors among neonates admitted to neonatal intensive care units in primary hospitals in central gondar zone, northwest ethiopia, 2019. Infect Drug Resist. 2020; 13: 3957–67.
|
| [19] |
Abiy SA, Animut Y, Ambaw WM, Aragaw GM, Rade BK. Incidence of death and its predictors among neonates admitted with sepsis in referral hospitals, northwest Ethiopia, a prospective cohort study. Front Pediatr. 2023; 11(April): 1–11.
|
| [20] |
Ethiopian Public Health Institute (EPHI), ICF. Ethiopia Mini Demographic and Health Survey 2019: Final Report [Internet]. 2021. 1–207 p. Available from:
https://dhsprogram.com/pubs/pdf/FR363/FR363.pdf
|
| [21] |
Bitew ZW, Alemu A, Ayele EG, Jember DA, Haile MT, Worku T. Incidence Density Rate of Neonatal Mortality and Predictors in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. Int J Pediatr (United Kingdom). 2020.
|
| [22] |
Sên I, Øpuƒ SÍÑ. ¡õM-K eKQ´w. 1998.
|
| [23] |
Dessu S, Habte A, Melis T, Gebremedhin M. Survival Status and Predictors of Mortality among Newborns Admitted with Neonatal Sepsis at Public Hospitals in Ethiopia. Int J Pediatr (United Kingdom). 2020; 2020.
|
| [24] |
Jibro U, Desalew A, Ayana GM, Tura AK. Time to Death and Its Predictors among Neonates Hospitalized with Sepsis in Eastern Ethiopia. Biomed Res Int. 2024; 2024.
|
| [25] |
Awoke AB, Tilahun F, Hassen S, Bialfew F, Molla A, Yimam AM. Time to death and its predictors among neonates admitted to the neonatal intensive care unit at Boru Meda General Hospital, Northeast Ethiopia. Sci Rep. 2025; 15(1): 1–13.
|
| [26] |
Wudu MA, Bekalu YE, Wondifraw EB, Birhanu TA, Hailu MK, Belete MA, et al. Time to death and its predictors among neonates admitted with sepsis in neonatal intensive care unit at comprehensive specialized hospitals in Northeast Ethiopia. Front Pediatr. 2024; 12(April).
|
Cite This Article
-
APA Style
Wakeyo, M. U., Kote, M., Girma, Z. (2026). Time to Death and Its Predictors Among Neonates Admitted with Neonatal Sepsis at Public Hospitals of West Arsi Zone, Southern Ethiopia. Science Discovery Public Health, 1(1), 32-49. https://doi.org/10.11648/j.sdph.20260101.15
 Copy
|
Copy
|
 Download
Download
ACS Style
Wakeyo, M. U.; Kote, M.; Girma, Z. Time to Death and Its Predictors Among Neonates Admitted with Neonatal Sepsis at Public Hospitals of West Arsi Zone, Southern Ethiopia. Sci. Discov. Public Health 2026, 1(1), 32-49. doi: 10.11648/j.sdph.20260101.15
Copy
|
Download
AMA Style
Wakeyo MU, Kote M, Girma Z. Time to Death and Its Predictors Among Neonates Admitted with Neonatal Sepsis at Public Hospitals of West Arsi Zone, Southern Ethiopia. Sci Discov Public Health. 2026;1(1):32-49. doi: 10.11648/j.sdph.20260101.15
Copy
|
Download
-
@article{10.11648/j.sdph.20260101.15,
author = {Mamud Umer Wakeyo and Mesfin Kote and Zeleke Girma},
title = {Time to Death and Its Predictors Among Neonates Admitted with Neonatal Sepsis at Public Hospitals of West Arsi Zone, Southern Ethiopia},
journal = {Science Discovery Public Health},
volume = {1},
number = {1},
pages = {32-49},
doi = {10.11648/j.sdph.20260101.15},
url = {https://doi.org/10.11648/j.sdph.20260101.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sdph.20260101.15},
abstract = {Introduction: According to world health organization each year, 3.6 million deaths in children under the age of five are attributable to neonatal mortality, accounting for 41% of all deaths in children under the age of five. Most of these deaths occur in low-income countries, and almost a million of these neonatal deaths either directly or indirectly related to neonatal sepsis. This study aimed to assess the time to death and its predictors among neonates admitted with neonatal sepsis at public comprehensive and general hospitals in the West Arsi zone of southern Ethiopia. Method: This multicenter institution-based retrospective follow-up study conducted from May 30 to June 30, 2023. Kobo toolbox was used for data collection. Checked for completeness, edited, and coded using Microsoft Excel. The data imported into STATA version 18 and cleaned before analysis. The incidence rate estimated for the entire study period and specified intervals of hospital stay. The Weibull regression model was selected using Akaike information criteria and Bayesian information criteria and used to analyze the relationship between the outcome and independent variables. Variables in the bi-variable analysis with p-value ≤ 0.25 were as candidates for multivariable analysis. In the multivariable analysis, statistical significance was set at p < 0.05. The association summarized using an adjusted hazard ratio (AHR) with a 95% confidence interval. Result: Of the 526 neonates with neonatal sepsis, 67 (12.7%) (95% confidence interval [CI]: 10–15.9) died. The overall incidence of neonatal mortality was 16.1 per 1000 neonatal days. The mean time to death among neonates died was 7.9 days (95% CI: 7.63, 8.19). Respiratory distress at admission (Adjusted Hazard Ratio (AHR): 0.37, 95% CI: 0.18, 0.77), breastfeeding within one hour (AHR: 3.15, 95% CI: 1.38, 7.18), gravidity (AHR: 0.37, 95% CI: 0.15, 0.88), and maternal health problems (AHR: 0.44, 95% CI: 0.25, 0.79) were found to be significant predictors of neonatal mortality. Conclusion: This study revealed that among neonates, 67 (12.7%) (95% CI: 10, 15.9) died during the follow-up period. Respiratory distress during admission, initiation of breastfeeding within one hour of birth, gravidity, and maternal health problems were predictors of mortality among neonates admitted with neonatal sepsis. Early initiation of breast feeding, monitoring of high-risk mothers, and strengthening NICU care are some of recommendations.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Time to Death and Its Predictors Among Neonates Admitted with Neonatal Sepsis at Public Hospitals of West Arsi Zone, Southern Ethiopia
AU - Mamud Umer Wakeyo
AU - Mesfin Kote
AU - Zeleke Girma
Y1 - 2026/04/24
PY - 2026
N1 - https://doi.org/10.11648/j.sdph.20260101.15
DO - 10.11648/j.sdph.20260101.15
T2 - Science Discovery Public Health
JF - Science Discovery Public Health
JO - Science Discovery Public Health
SP - 32
EP - 49
PB - Science Publishing Group
UR - https://doi.org/10.11648/j.sdph.20260101.15
AB - Introduction: According to world health organization each year, 3.6 million deaths in children under the age of five are attributable to neonatal mortality, accounting for 41% of all deaths in children under the age of five. Most of these deaths occur in low-income countries, and almost a million of these neonatal deaths either directly or indirectly related to neonatal sepsis. This study aimed to assess the time to death and its predictors among neonates admitted with neonatal sepsis at public comprehensive and general hospitals in the West Arsi zone of southern Ethiopia. Method: This multicenter institution-based retrospective follow-up study conducted from May 30 to June 30, 2023. Kobo toolbox was used for data collection. Checked for completeness, edited, and coded using Microsoft Excel. The data imported into STATA version 18 and cleaned before analysis. The incidence rate estimated for the entire study period and specified intervals of hospital stay. The Weibull regression model was selected using Akaike information criteria and Bayesian information criteria and used to analyze the relationship between the outcome and independent variables. Variables in the bi-variable analysis with p-value ≤ 0.25 were as candidates for multivariable analysis. In the multivariable analysis, statistical significance was set at p < 0.05. The association summarized using an adjusted hazard ratio (AHR) with a 95% confidence interval. Result: Of the 526 neonates with neonatal sepsis, 67 (12.7%) (95% confidence interval [CI]: 10–15.9) died. The overall incidence of neonatal mortality was 16.1 per 1000 neonatal days. The mean time to death among neonates died was 7.9 days (95% CI: 7.63, 8.19). Respiratory distress at admission (Adjusted Hazard Ratio (AHR): 0.37, 95% CI: 0.18, 0.77), breastfeeding within one hour (AHR: 3.15, 95% CI: 1.38, 7.18), gravidity (AHR: 0.37, 95% CI: 0.15, 0.88), and maternal health problems (AHR: 0.44, 95% CI: 0.25, 0.79) were found to be significant predictors of neonatal mortality. Conclusion: This study revealed that among neonates, 67 (12.7%) (95% CI: 10, 15.9) died during the follow-up period. Respiratory distress during admission, initiation of breastfeeding within one hour of birth, gravidity, and maternal health problems were predictors of mortality among neonates admitted with neonatal sepsis. Early initiation of breast feeding, monitoring of high-risk mothers, and strengthening NICU care are some of recommendations.
VL - 1
IS - 1
ER -
Copy
|
Download