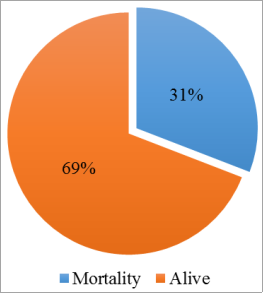
Background: Tuberculosis (TB) remains a significant public health concern globally, especially among HIV-positive individuals. The study aimed to investigate the factors associated with mortality among HIV/TB co-infected patients receiving antiretroviral therapy (ART) in Dire Dawa, Ethiopia. Methods: A retrospective follow-up study was conducted at Dilchora Referral Hospital among 434 HIV/TB co-infected patients enrolled in ART from January 2008 to January 2023. Standardized checklist was used for data collection and taken from patient’s medical cards and database system. Binary logistic regression was used to identify baseline factors associated with mortality. Results: The study found a mortality rate of 31% among HIV/TB co-infected patients. Factors such as WHO clinical stage III (AOR: 9.3, 95% CI: 3.03, 28.34) and WHO clinical stage IV (AOR: 11.3, 95% CI: 3.5, 36.34) and underweight and overweight body mass index were (AOR: 2.6, 95% CI: 1.35, 4.83) and (AOR: 21.4, 95% CI: 8.24, 55.5), poor ART adherence (AOR: 4.24, 95% CI: 2.25, 7.98), alcohol consumption (AOR: 3.15, 95%: 1.69, 5.87), and smoking (AOR: 4.12, 95% CI: 2.32, 7.29) were associated with increased odds of mortality. Conclusion: The study underscores the importance of identifying and addressing baseline factors that contribute to mortality in HIV/TB co-infected patients. Interventions targeting factors like clinical staging, adherence to ART, and lifestyle habits could help reduce mortality rates in this population.
| Published in | Science Journal of Clinical Medicine (Volume 13, Issue 3) |
| DOI | 10.11648/j.sjcm.20241303.11 |
| Page(s) | 38-46 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Mortality, HIV/TB Co-infection, Antiretroviral Therapy, Ethiopia
Variables | Categories | Frequency | Percentage (%) |
|---|---|---|---|
Sex | Male | 192 | 44.24 |
Female | 242 | 55.76 | |
Age | <15 | 22 | 5.07 |
15-24 | 45 | 10.37 | |
25-34 | 124 | 28.57 | |
35-44 | 148 | 34.10 | |
>44 | 95 | 21.89 | |
Residence | Urban | 386 | 88.94 |
Rural | 48 | 11.06 | |
Marital status | Never married | 140 | 32.26 |
Married | 154 | 35.48 | |
Divorced | 71 | 16.36 | |
Widowed | 43 | 9.91 | |
separated | 26 | 5.99 | |
Occupation status | Government Employed | 35 | 8.06 |
Private Employed | 14 | 3.23 | |
Student | 26 | 5.99 | |
Housewife | 52 | 11.98 | |
Merchant | 77 | 17.74 | |
Othersa | 128 | 29.49 | |
unknown | 102 | 23.50 | |
Educational status | No formal education | 108 | 24.88 |
Primary | 183 | 42.17 | |
Secondary | 121 | 27.88 | |
Tertiary | 22 | 5.07 | |
Religion | Muslim | 141 | 32.49 |
Orthodox | 254 | 58.53 | |
Othersb | 39 | 8.99 | |
HIV Disclosure | Yes | 302 | 69.59 |
No | 132 | 30.41 |
Variables | Categories | Frequency | Percentage (%) |
|---|---|---|---|
Clinical stages | Stage I | 67 | 15.44 |
Stage II | 102 | 23.50 | |
Stage III | 192 | 44.24 | |
Stage IV | 73 | 16.82 | |
BMI | Underweight | 231 | 53.23 |
Normal | 180 | 41.47 | |
Overweight | 23 | 5.3 | |
Functional status | Ambulatory | 144 | 33.18 |
Bedridden | 98 | 22.58 | |
Working | 192 | 44.24 | |
Site of TB infection | Pulmonary | 207 | 47.70 |
Extrapulomnary | 227 | 52.30 | |
CD4 cell count | < 200 | 223 | 51.38 |
>=200 | 211 | 48.62 | |
Hemoglobin level | <10 | 122 | 28.11 |
10 | 312 | 71.89 | |
Opportunistic infection | Yes | 297 | 68.43 |
No | 137 | 31.57 | |
Adherence status | Good | 244 | 56.22 |
Fair | 84 | 19.35 | |
Poor | 106 | 24.42 | |
CTP | Yes | 380 | 87.56 |
No | 54 | 12.44 | |
Drinking alcohol | Yes | 94 | 21.66 |
No | 340 | 78.34 | |
Smoking status | Yes | 121 | 27.88 |
No | 313 | 72.12 |
Variables | Categories | COR (95%CI) | AOR (95%CI) | P-value |
|---|---|---|---|---|
Age | <15 | 1 | 1 | |
15-24 | 2.6 (0.65, 10.20) | 2.0 (0.47, 8.52) | 0.351 | |
25-34 | 3.2 (0.91, 11.59) | 2.3 (0.69, 10.13) | 0.154 | |
35-44 | 3.4 (0.97, 12.14) | 2.3 (0.59, 8.75) | 0.232 | |
45 | 2.1 (0.58, 7.88) | 1.6 (0.38, 6.31) | 0.538 | |
Clinical stage | Stage I | 1 | 1 | |
stage II | 0.67 (0.22, 2.02) | 1.9 (0.49, 7.26) | 0.357 | |
Stage III | 4.6 (2.0, 10.68) | 9.3 (3.03, 28.34) | 0.0001* | |
stage IV | 7. 6 (3.11, 18.44) | 11.3 (3.5, 36.68) | 0.0001* | |
BMI | Normal | 1 | 1 | |
Underweight | 3.02 (1.82, 5.01) | 2.6 (1.35, 4.83) | 0.004* | |
Overweight | 10.5 (5.27, 20.76) | 21.4 (8.24, 55.5) | 0.0001* | |
Functional status | Ambulatory | 1.35 (0.82, 2.20) | 1.6 (0.93, 3.15) | 0.131 |
Bedridden | 3.0 (1.79, 5.05) | 2.8 (1.42, 5.38) | 0.112 | |
Working | 1 | |||
Site of TB infection | Pulmonary | 1.42 (0.94, 2.14) | 1.69 (0.97, 2.94) | 0.062 |
Extrapulomnary | 1 | 1 | ||
Hemoglobin | <10 | 2.1 (1.34, 3.23) | 1.66 (0.92, 2.99) | 0.091 |
10 | 1 | 1 | ||
Drug Adherence | Good | 1 | 1 | |
Fair | 2.1 (1.20, 3.74) | 1.9 (0.89, 3.99) | 0.110 | |
Poor | 4.2 (2.62, 6.84) | 4.24 (2.25, 7.98) | 0.0001* | |
Drinking alcohol | Yes | 3.17 (2.02, 4.99) | 3.15 (1.69, 5.87) | 0.0001* |
No | 1 | 1 | ||
Smoking status | Yes | 5.2 (3.36, 8.09) | 4.12 (2.32, 7.29) | 0.0001* |
No | 1 | 1 |
AIDS | Acquired Immunodeficiency Syndrome |
ART | Anti-Retroviral Treatment |
BMI | Body Mass Index |
CPT | Co-trimoxazole Preventive Treatment |
HIV | Human Immunodeficiency Virus |
PLHIV | People Living With HIV/AIDS |
TB | Tuberculosis |
WHO | World Health Organization |
| [1] | Masquelier B, Hug L, Sharrow D, You D, Mathers C, Gerland P, et al. Global, regional, and national mortality trends in youth aged 15–24 years between 1990 and 2019: a systematic analysis. The Lancet Global Health. 2021; 9(4): e409-e17. |
| [2] | Global tuberculosis report 2023. Geneva: World Health Organization, 2023. |
| [3] | Gatechompol S, Kawkitinarong K, Suwanpimolkul G, Kateruttanakul P, Manosuthi W, Sophonphan J, et al. Treatment outcomes and factors associated with mortality among individuals with both TB and HIV in the antiretroviral era in Thailand. Journal of Virus Eradication. 2019; 5(4): 225-30. |
| [4] | Fact Sheet World Tuberculosis Day 2022. UNAIDS, 2022. |
| [5] | Tuberculosis in the WHO African Region: 2023 progress update. Brazzaville: WHO African Region, 2023. |
| [6] | Global tuberculosis report 2022. Geneva: World Health Organization, 2022. |
| [7] | Seyoum E, Demissie M, Worku A, Mulu A, Berhane Y, Abdissa A. Increased Mortality in HIV Infected Individuals with Tuberculosis: A Retrospective Cohort Study, Addis Ababa, Ethiopia. HIV/AIDS - Research and Palliative Care. 2022; 14(null): 143-54. |
| [8] | Gemechu J, Gebremichael B, Tesfaye T, Seyum A, Erkalo D. Predictors of mortality among TB-HIV co-infected children attending anti-retroviral therapy clinics of selected public hospitals in southern, Ethiopia: retrospective cohort study. Archives of Public Health. 2022; 80(1): 1-13. |
| [9] | Lelisho ME, Wotale TW, Tareke SA, Alemu BD, Hassen SS, Yemane DM, et al. Survival rate and predictors of mortality among TB/HIV co-infected adult patients: retrospective cohort study. Scientific Reports. 2022; 12(1): 18360. |
| [10] | Getaneh T, Negesse A, Dessie G, Desta M. The impact of tuberculosis co-infection on virological failure among adults living with HIV in Ethiopia: A systematic review and meta-analysis. Journal of Clinical Tuberculosis and Other Mycobacterial Diseases. 2022; 27: 100310. |
| [11] | The CDC Division of Global HIV & TB Country profile. CDC, 2022 September. Report No. |
| [12] | HIV/AIDS National Strategic Plan (NSP) for Ethiopia 2021-2025. Federal HIV/AIDS Prevention and Control Office (FHAPCO), 2021. |
| [13] | Kefyalew Addis A, Ahmed E, Dylan DB, Susan FR, Punam A, Daniel JW, et al. Spatial codistribution of HIV, tuberculosis and malaria in Ethiopia. BMJ Global Health. 2022; 7(2): e007599. |
| [14] | Belay GM, Wubneh CA. Childhood tuberculosis treatment outcome and its association with HIV co-infection in Ethiopia: a systematic review and meta-analysis. Tropical Medicine and Health. 2020; 48(1): 7. |
| [15] | Lelisho ME, Teshale BM, Tareke SA, Hassen SS, Andargie SA, Merera AM, et al. Modeling Survival Time to Death Among TB and HIV Co-infected Adult Patients: an Institution-Based Retrospective Cohort Study. Journal of Racial and Ethnic Health Disparities. 2023; 10(4): 1616-28. |
| [16] | Fenta A, Demeke G, Bitew A, Kebede D, Hailu T. Prevalence and Associated Factors of TB Co-Morbidity Among HIV Sero-Positive Individuals in Shegaw Motta District Hospital, Ethiopia. International Journal of General Medicine. 2020; 13(null): 1529-36. |
| [17] | Birhan H, Derebe K, Muche S, Melese B. Statistical Analysis on Determinant Factors Associated with Time to Death of HIV/TB Co-Infected Patients Under HAART at Debre Tabor Referral Hospital: An Application of Accelerated Failure Time-Shared Frailty Models. HIV/AIDS - Research and Palliative Care. 2021; 13(null): 775-87. |
| [18] | Podlekareva DN, Efsen AM, Schultze A, Post FA, Skrahina AM, Panteleev A, et al. Tuberculosis-related mortality in people living with HIV in Europe and Latin America: an international cohort study. The lancet HIV. 2016; 3(3): e120-31. |
| [19] | Zeru MA. Prevalence and associated factors of HIV-TB co-infection among HIV patients: a retrospective Study. African health sciences. 2021; 21(3): 1003-9. |
| [20] | Birara Aychiluhm S, Mohammed E, Altaye H, Urgessa K, Mare KU, Tadesse AW, et al. Tuberculosis Co-infection and Associated Factors among People Living with HIV /AIDS Who are on Antiretroviral Therapy in Pastoral Community, Northeast Ethiopia. A Bayesian Analysis Approach. Cogent Public Health. 2022; 9(1): 2145700. |
| [21] | Chanie ES, Gelaye GA, Tadesse TY, Feleke DG, Admas WT, Molla Alemu E, et al. Estimation of lifetime survival and predictors of mortality among TB with HIV co-infected children after test and treat strategies launched in Northwest, Ethiopia, 2021; a multicentre historical follow-up study. 2021; 16(12): e0258964. |
| [22] | Rossetto M, Brand ÉM, Rodrigues RM, Serrant L, Teixeira LB. Factors associated with hospitalization and death among TB/HIV co-infected persons in Porto Alegre, Brazil. PLoS One. 2019; 14(1): e0209174. |
| [23] | World Health O. Global tuberculosis report 2013: World Health Organization; 2013. |
| [24] | Dawit Z, Abebe S, Dessu S, Mesele M, Sahile S, Ajema D. Incidence and predictors of mortality among children co-infected with tuberculosis and human immunodeficiency virus at public hospitals in Southern Ethiopia. Plos one. 2021; 16(6): e0253449. |
| [25] | Tola A, Mishore KM, Ayele Y, Mekuria AN, Legese N. Treatment Outcome of Tuberculosis and Associated Factors among TB-HIV Co-Infected Patients at Public Hospitals of Harar Town, Eastern Ethiopia. A five-year retrospective study. BMC Public Health. 2019; 19(1): 1658. |
| [26] | Wondimu W, Dube L, Kabeta T. Factors Affecting Survival Rates Among Adult TB/HIV Co-Infected Patients in Mizan Tepi University Teaching Hospital, South West Ethiopia. HIV/AIDS - Research and Palliative Care. 2020; 12(null): 157-64. |
| [27] | Gezae KE, Abebe HT, Gebretsadik LG, Gebremeskel AK. Predictors of time to death among TB/HIV co-infected adults on ART at two governmental hospitals in Mekelle, Ethiopia, 2009–2016: A retrospective cohort study. Ann Infect Dis Epidemiol 2020; 5(1). 2020; 1049. |
| [28] | Acharya S, Karanjkar V, Bhamre SP, Palkar A, Rathod D, Setia MS. Factors associated with mortality in HIV‐TB co‐infected patients during and after the course of TB treatment in high‐burden settings, Mumbai, India: A cohort analysis. Tropical Medicine & International Health. 2024; 29(1): 23-32. |
| [29] | Qi TK, Chen J, Zhang RF, Liu L, Shen YZ, Wang ZY, et al. A retrospective cohort study of early mortality among patients with HIV/TB co‐infection in Shanghai municipality. HIV medicine. 2020; 21(11): 739-46. |
| [30] | Pacheco AG, Veloso VG, Nunes EP, Ribeiro S, Guimarães MR, Lourenço MC, et al. Tuberculosis is associated with non-tuberculosis-related deaths among HIV/AIDS patients in Rio de Janeiro. The international journal of tuberculosis and lung disease: the official journal of the International Union against Tuberculosis and Lung Disease. 2014; 18(12): 1473-8. |
| [31] | Oshi DC, Oshi SN, Alobu I, Ukwaja KN. Profile, outcomes, and determinants of unsuccessful tuberculosis treatment outcomes among HIV-infected tuberculosis patients in a Nigerian state. Tuberculosis research and treatment. 2014; 2014. |
| [32] | Fiseha T, Gebru T, Gutema H, Debela Y. Tuberculosis treatment outcome among HIV co-infected patients at Mizan-Aman general hospital, Southwest Ethiopia: a retrospective study. J Bioeng Biomed Sci. 2015; 5(1): 139. |
| [33] | Kiros T, Dejen E, Tiruneh M, Tiruneh T, Eyayu T, Damtie S, et al. Magnitude and associated factors of pulmonary tuberculosis among HIV/AIDS patients attending antiretroviral therapy clinic at Debre tabor specialized hospital, Northwest Ethiopia, 2019. HIV/AIDS-Research and Palliative Care. 2020: 849-58. |
| [34] | Gupta P, Tomar A, Bansal M, Gupta RK. Clinico-epidemiological Determinants of Tuberculosis Co-infection among Adults Attending an Antiretroviral Centre at a Tertiary Care Hospital in Madhya Pradesh. Journal of Medical Evidence. 2023; 4(3): 220-4. |
| [35] | Mollel EW, Todd J, Mahande MJ, Msuya SE. Effect of tuberculosis infection on mortality of HIV-infected patients in Northern Tanzania. Tropical Medicine and Health. 2020; 48(1): 1-10. |
| [36] | Birhan H, Seyoum A, Derebe K, Muche S, Wale M, Sisay S. Joint clinical and socio-demographic determinants of CD4 cell count and body weight in HIV/TB co-infected adult patients on HAART. Scientific African. 2022; 18: e01396. |
| [37] | Zerdali E, Nakir IY, Surme S, Sayili U, Yildirim M. Predictors for tuberculosis co-infection in people living with HIV/AIDs. African health sciences. 2021; 21(3): 995-1002. |
| [38] | Obeagu EI, Onuoha EC. Tuberculosis among HIV Patients: A review of Prevalence and Associated Factors. Int J Adv Res Biol Sci. 2023; 10(9): 128-34. |
| [39] | Van Rie A, Westreich D, Sanne I. Tuberculosis in patients receiving antiretroviral treatment: incidence, risk factors and prevention strategies. Journal of acquired immune deficiency syndromes (1999). 2011; 56(4): 349. |
APA Style
Bayisa, F. S., Nimani, T. D. (2024). Mortality and Associated Factors Among HIV/TB Co-infected Patients Under ART Clinic in Dire Dawa, Ethiopia, 2023. Science Journal of Clinical Medicine, 13(3), 38-46. https://doi.org/10.11648/j.sjcm.20241303.11
ACS Style
Bayisa, F. S.; Nimani, T. D. Mortality and Associated Factors Among HIV/TB Co-infected Patients Under ART Clinic in Dire Dawa, Ethiopia, 2023. Sci. J. Clin. Med. 2024, 13(3), 38-46. doi: 10.11648/j.sjcm.20241303.11
AMA Style
Bayisa FS, Nimani TD. Mortality and Associated Factors Among HIV/TB Co-infected Patients Under ART Clinic in Dire Dawa, Ethiopia, 2023. Sci J Clin Med. 2024;13(3):38-46. doi: 10.11648/j.sjcm.20241303.11
@article{10.11648/j.sjcm.20241303.11,
author = {Feyisa Shasho Bayisa and Teshome Demis Nimani},
title = {Mortality and Associated Factors Among HIV/TB Co-infected Patients Under ART Clinic in Dire Dawa, Ethiopia, 2023
},
journal = {Science Journal of Clinical Medicine},
volume = {13},
number = {3},
pages = {38-46},
doi = {10.11648/j.sjcm.20241303.11},
url = {https://doi.org/10.11648/j.sjcm.20241303.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjcm.20241303.11},
abstract = {Background: Tuberculosis (TB) remains a significant public health concern globally, especially among HIV-positive individuals. The study aimed to investigate the factors associated with mortality among HIV/TB co-infected patients receiving antiretroviral therapy (ART) in Dire Dawa, Ethiopia. Methods: A retrospective follow-up study was conducted at Dilchora Referral Hospital among 434 HIV/TB co-infected patients enrolled in ART from January 2008 to January 2023. Standardized checklist was used for data collection and taken from patient’s medical cards and database system. Binary logistic regression was used to identify baseline factors associated with mortality. Results: The study found a mortality rate of 31% among HIV/TB co-infected patients. Factors such as WHO clinical stage III (AOR: 9.3, 95% CI: 3.03, 28.34) and WHO clinical stage IV (AOR: 11.3, 95% CI: 3.5, 36.34) and underweight and overweight body mass index were (AOR: 2.6, 95% CI: 1.35, 4.83) and (AOR: 21.4, 95% CI: 8.24, 55.5), poor ART adherence (AOR: 4.24, 95% CI: 2.25, 7.98), alcohol consumption (AOR: 3.15, 95%: 1.69, 5.87), and smoking (AOR: 4.12, 95% CI: 2.32, 7.29) were associated with increased odds of mortality. Conclusion: The study underscores the importance of identifying and addressing baseline factors that contribute to mortality in HIV/TB co-infected patients. Interventions targeting factors like clinical staging, adherence to ART, and lifestyle habits could help reduce mortality rates in this population.
},
year = {2024}
}
TY - JOUR T1 - Mortality and Associated Factors Among HIV/TB Co-infected Patients Under ART Clinic in Dire Dawa, Ethiopia, 2023 AU - Feyisa Shasho Bayisa AU - Teshome Demis Nimani Y1 - 2024/08/15 PY - 2024 N1 - https://doi.org/10.11648/j.sjcm.20241303.11 DO - 10.11648/j.sjcm.20241303.11 T2 - Science Journal of Clinical Medicine JF - Science Journal of Clinical Medicine JO - Science Journal of Clinical Medicine SP - 38 EP - 46 PB - Science Publishing Group SN - 2327-2732 UR - https://doi.org/10.11648/j.sjcm.20241303.11 AB - Background: Tuberculosis (TB) remains a significant public health concern globally, especially among HIV-positive individuals. The study aimed to investigate the factors associated with mortality among HIV/TB co-infected patients receiving antiretroviral therapy (ART) in Dire Dawa, Ethiopia. Methods: A retrospective follow-up study was conducted at Dilchora Referral Hospital among 434 HIV/TB co-infected patients enrolled in ART from January 2008 to January 2023. Standardized checklist was used for data collection and taken from patient’s medical cards and database system. Binary logistic regression was used to identify baseline factors associated with mortality. Results: The study found a mortality rate of 31% among HIV/TB co-infected patients. Factors such as WHO clinical stage III (AOR: 9.3, 95% CI: 3.03, 28.34) and WHO clinical stage IV (AOR: 11.3, 95% CI: 3.5, 36.34) and underweight and overweight body mass index were (AOR: 2.6, 95% CI: 1.35, 4.83) and (AOR: 21.4, 95% CI: 8.24, 55.5), poor ART adherence (AOR: 4.24, 95% CI: 2.25, 7.98), alcohol consumption (AOR: 3.15, 95%: 1.69, 5.87), and smoking (AOR: 4.12, 95% CI: 2.32, 7.29) were associated with increased odds of mortality. Conclusion: The study underscores the importance of identifying and addressing baseline factors that contribute to mortality in HIV/TB co-infected patients. Interventions targeting factors like clinical staging, adherence to ART, and lifestyle habits could help reduce mortality rates in this population. VL - 13 IS - 3 ER -
Department of Epidemiology and Biostatistics, School of Public Health, College of Health and Medical Science, Haramaya University, Harar, Ethiopia
Department of Epidemiology and Biostatistics, School of Public Health, College of Health and Medical Science, Haramaya University, Harar, Ethiopia
Information