Abstract
Objective: To analyze the current state of breastfeeding in Costa Rica by examining key indicators and identifying profiles of mothers at risk, to understand the factors influencing breastfeeding decisions and to propose evidence-based interventions in maternal and child health policies. Methodology: A qualitative study with an interpretative phenomenological approach was conducted. The lived experiences of 24 mothers from diverse regions across the country were explored and analyzed. Results: The findings reveal that, although both rural and urban mothers share a strong intention to breastfeed, they face different challenges. Perceptions of motherhood, insecurity regarding milk production, and employment-related obstacles significantly influence the time and exclusivity of breastfeeding. Urban mothers often encounter more pronounced work-related barriers, while rural mothers report limited access to professional support. Maternal education and the availability of postnatal support emerged as critical factors in sustaining breastfeeding practices. Conclusions: Strengthening postnatal support systems, enhancing maternal education, and developing strategies to reconcile breastfeeding with employment demands are essential. These measures could improve national breastfeeding indicators and help close socioeconomic gaps among mothers in different contexts.
|
Published in
|
Science Journal of Public Health (Volume 13, Issue 5)
|
|
DOI
|
10.11648/j.sjph.20251305.13
|
|
Page(s)
|
269-282 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Breastfeeding, Socioeconomic Factors, Maternal Education, Postnatal Support, Phenomenology, Costa Rica
1. Introduction
Breastfeeding (BF) is a fundamental strategy for both infant and maternal health, promoted by the World Health Organization (WHO) as the optimal standard of nutrition during the first six months of life. Its benefits have been extensively documented in scientific literature, including the reduction of infectious diseases, the strengthening of the infant's immune system, and the decreased risk of metabolic disorders in adulthood
| [1] | Victora CG, Bahl R, Barros AJ, França GV, Horton S, Krasevec J, Murch S, Sankar MJ, Walker N, Rollins NC; Lancet Breastfeeding Series Group. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016; 387(10017): 475-90. https://doi.org/10.1016/S0140-6736(15)01024-7 |
| [2] | Horta B, Victora C, World Health Organization. (2013). Long-term effects of breastfeeding: a systematic review. World Health Organization. https://iris.who.int/handle/10665/79198 |
[1, 2]
.
BF not only provides essential nutrients but also serves as a protective factor against various pathologies, making it a crucial practice in public health
| [3] | Alotiby AA. The role of breastfeeding as a protective factor against the development of the immune-mediated diseases: A systematic review. Front Pediatr. 2023 Feb 16; 11: 1086999. https://doi.org/10.3389/fped.2023.1086999 |
[3]
. It is one of the most powerful practices for promoting child survival and well-being, as it protects against chronic and potentially life-threatening diseases and fosters healthy child development. BF has been shown to support brain development and is associated with higher intelligence levels
| [4] | Grantham-McGregor S, Cheung YB, Cueto S, Glewwe P, Richter L, Strupp B; International Child Development Steering Group. Developmental potential in the first 5 years for children in developing countries. Lancet. 2007 Jan 6; 369(9555): 60-70. https://doi.org/10.1016/S0140-6736(07)60032-4 |
[4]
.
These benefits have been observed in both developing and developed countries, highlighting the universality of its positive effects
. Moreover, BF should not be viewed only as a biological act but also as a social, cultural, and political phenomenon, shaped by gender dynamics, power relations, and inequalities
. Decisions regarding BF are influenced by multiple factors, including age, ethnicity, sexual orientation, socioeconomic status, education, migration status, and the presence of disabilities, among others. Therefore, it is essential to adopt an intersectional approach
that facilitates the understanding of how these dimensions intersect and shape differentiated experiences among women.
From feminist theoretical perspectives, the medicalization and standardization of BF have been critically examined, as these processes may exert pressure and induce guilty feelings in women who are unable or unwilling to breastfeed
. It is important to promote a perspective on BF that respects women’s autonomy and informed decision-making, without imposing a singular model of the “good mother.”
The promotion of BF is also intrinsically linked to the defense of human rights for women and children
| [9] | Van T, Varadi D, Adams AC, Feldman-Winter L. Promotion, Protection, and Support of Breastfeeding as a Human Right: A Narrative Review. Breastfeed Med. 2023 Aug; 18(8): 561-570. https://doi.org/10.1089/bfm.2023.0061 |
[9]
. Access to accurate information and appropriate support for BF is essential to ensure that women can exercise their rights to sexual and reproductive health, and that children’s rights to adequate nutrition are protected.
In 2020, the rate of exclusive BF (EBF) during the first six months of life in Latin America and the Caribbean was 37.3%, below the global average of 43.8%. Mesoamerica has made significant progress, increasing from 21.6% in 2012 to 31.9% in 2020. Although this represents an improvement, it remains below both the global average and the targets set by the Global Breastfeeding Collective (50%) and the Sustainable Development Goals (SDGs) (70%)
. In contrast, EBF in the Caribbean declined between 2012 and 2020 to 27.3%, while in South America, the rate reached 42%, approaching the global average
.
Notably, Bolivia, Guatemala, and Peru were the only countries in the region with EBF rates above 50% in 2020. Some countries in Latin America and the Caribbean reported significant increases between 2012 and 2020; for example, Belize showed the highest increase (24 percentage points), followed by El Salvador (22.7 percentage points) and Trinidad and Tobago (almost 20 percentage points). Bolivia and Haiti also reported increases of 15 percentage points. Conversely, EBF rates declined by nearly seven percentage points in Dominican Republic (between 2011 and 2018) and in Costa Rica
.
Although BF is a socially accepted practice in Costa Rica and supported by legal frameworks and public health programs, data from the Women, Children, and Adolescents Survey (EMNA, 2018) highlight persistent challenges in terms of exclusivity and duration among Costa Rican mothers. Significant disparities are observed based on geographic origin (urban vs. rural), educational level, and income quintiles
.
Based on the analysis of these indicators, published since 1966 through various national surveys and literature sources
| [13] | Ministerio de Salud, Instituto Nacional de Estadística y Censos (INEC) y Fondo de las Naciones Unidas para la Infancia (UNICEF). (2018). Encuesta de Mujeres, Niñez y Adolescencia (EMNA): Informe de resultados de la encuesta. San José, Costa Rica. [accessed Wednesday, May 21, 2025]. Available from: Available from: https://www.unicef.org/costarica/media/436/file/Encuesta-de-mujeres-ninez-y-adolescencia-2018.pdf |
| [14] | Ministerio de Salud, INCIENSA. Caja Costarricense de Seguro Social. Encuesta basal comunidades centinela en alimentación y nutrición 1999-2000. San José, Costa Rica: Ministerio de Salud; 2002. [accessed Wednesday, May 21, 2025]. Available from: https://www.binasss.sa.cr/Cendamas.pdf |
| [15] | Morice AC. Lactancia natural en Costa Rica: tendencias y factores de riesgo, período 1975 a 1990. Comisión Nacional de Lactancia Materna, INCAP/OPS. Publicación INCAP ME/027. Centro de Desarrollo Social; 1992. [accessed Wednesday, May 21, 2025]. Available from: Available from: https://bvssan.incap.int/local/M/ME-027.pdf |
| [16] | Machado Cruz V, Chaves Quirós S, Pérez Gutiérrez E. Lactancia Materna en Costa Rica, Tendencias y Desafíos Período 1990-1998. Departamento de Medicina Preventiva, Sección Salud del Niño, Caja Costarricense de Seguro Social, San José, Costa Rica. Revista Costarricense de Epidemiología. 2005 [accessed Wednesday, May 21, 2025]. Available from: https://www.binasss.sa.cr/revistas/epidemiologia/v1n2/art3.pdf |
[13-16]
, this study is focused on a qualitative perspective with the aim of deeply examine the lived experiences of BF and complementary feeding among 24 mothers from all seven provinces of Costa Rica.
Justification
In Costa Rica, the early initiation of BF (< 1 hour) has declined over time, from 95% in 1940 to 52.9% in 2018. While this percentage is higher than the global average of 46%, it remains below the SDG target of 70%. Similarly, the indicator for EBF in infants under six months of age has fluctuated from 11.2% in 1975 to 27.5% in 2018. Like the previous indicator, it also falls short of both the SDG target (60%) and the global average (48%).
Regarding the indicator “women aged 15-49 with a live birth in the last two years whose child was placed skin-to-skin,” statistically significant differences (p < 0.005) were found among rural women, women with only primary education, those with lower income, and those who gave birth in public hospitals, compared to urban women, those with higher education, and those who delivered their babies in private hospitals. Conversely, the percentage of children aged 0-23 months who were bottle-fed on the previous day (according to the 2018 EMNA survey) was significantly higher among children of mothers from urban areas (78.1%), with higher education (78.6%), and higher income (79.8%), compared to children of mothers from rural areas (68.2%), with lower education (68.7%), and lower income (72.8%)
.
In terms of dietary diversity (defined as children who appropriately received liquids and solids or soft foods the minimum number of times or more during the previous day) findings from 2018 showed that the diets of children whose mothers had higher educational achievement and belonged to the upper income quintiles were significantly more nutritionally adequate than those of children whose mothers had lower levels of education and income.
These data justify the need for this study, which adopts a qualitative approach to explore in depth the lived experiences of BF and complementary feeding among mothers from Costa Rica. The findings aim to support the development of differentiated and effective strategies directed at mothers based on place of residence (urban vs. rural), educational level, and income quintile, to strengthen BF practices across the country, reduce early dropout rates, and promote environments conducive to continued BF.
This study is further justified by the consideration of social and economic inequalities that influence BF practices. Women living in poverty, migrants with disabilities, and those belonging to ethnic minorities may face additional barriers in accessing quality BF information, support, and services
| [17] | Chiang KV, Li R, Anstey EH, Perrine CG. Racial and Ethnic Disparities in Breastfeeding Initiation ─ United States, 2019. MMWR Morb Mortal Wkly Rep 2021; 70: 769-774. https://doi.org/10.15585/mmwr.mm7021a1 |
[17]
. These barriers may include limited financial resources, discrimination, lack of access to culturally competent healthcare services, and insufficient familial or community support.
Intersectionality provides a critical analytical framework for understanding how these inequities manifest and are perpetuated in the context of BF. By analyzing women's experiences through an intersectional lens, it is possible to identify specific barriers and design more effective interventions that promote equality in access to BF support.
Moreover, gender rules and cultural expectations significantly influence women's decisions about BF. In many societies, BF is considered a “natural” responsibility of women, which can lead to pressure and guilty feelings among those who are unable or unwilling to breastfeed
. It is essential to challenge these gender stereotypes and promote a more equitative view of parenting in which both men and women share responsibilities for childcare.
The research question focused on "How do mothers experience and make sense of the particular social phenomenon of breastfeeding?" This inquiry specifically delved into "how" workplace pressure, misinformation, and lack of support contribute to mothers in Costa Rica discontinuing breastfeeding before the recommended period. Finally, this study is justified by its potential to inform public policies and health programs that promote BF through a gender-sensitive, human rights-based, and socially inclusive lens. By gaining a deeper understanding of women’s experiences and needs, more effective interventions can be designed to reduce disparities and ensure that all women can exercise their right to breastfeed and to benefit from the associated health outcomes for themselves and their children.
2. Methodology
The Interpretative Phenomenological Analysis (IPA) method was employed, which integrates phenomenology, hermeneutics, and ideography
| [19] | Duque H, Aristizábal Díaz Granados E. T. Análisis fenomenológico interpretativo: Una guía metodológica para su uso en la investigación cualitativa en psicología. Pensando Psicología. 2019; 15(25): 1-24. https://doi.org/10.16925/2382-3984.2019.01.03 |
[19]
. Phenomenology was reflected in the full respect given to the narratives shared by the mothers regarding their lived experiences with BF and complementary feeding. The focus was placed on studying lived realities-experiences that are often difficult to articulate. Hermeneutics was applied throughout the research process, as the researchers immersed themselves in the content and dynamics of each participating mother’s account, exploring the implications for their lives and efforts to construct a coherent and meaningful interpretation of the whole. Ideography guided this qualitative inquiry based on the premise that each mother is unique, and her experiences, emotions, and behaviors must be studied and understood within her specific context. This approach sought a deeper understanding of the mothers by considering their personal history, cultural background, values, and circumstances related to breastfeeding and complementary feeding practices.
2.1. Introduction to Interpretative Phenomenological Analysis (IPA) Method
The following steps were followed for the application of the Interpretative Phenomenological Analysis (IPA) method:
1. Research Question and Participant Selection
1) Formulation of the Research Question: the research question focused on "How do mothers experience and make sense of the particular social phenomenon of breastfeeding?" This inquiry specifically delved into "how" workplace pressure, misinformation, and lack of support contribute to mothers in Costa Rica discontinuing breastfeeding before the recommended period. The question was open-ended, allowing for a deep exploration of subjective perceptions.
2) Purposive Sampling: a group of participants from both urban and rural areas who had experienced the phenomenon of interest (breastfeeding) were selected. The aim was to obtain rich and detailed accounts of their experiences, as statistical generalizability was not the objective.
2. Data Collection
1) Semi-structured Interviews: semi-structured interviews were employed for data collection, serving as the quintessential technique for the Interpretative Phenomenological Analysis method. The interviews were flexible, allowing participants to freely explore their experiences, while the researchers guided the conversation with open-ended and exploratory questions. The researchers also utilized diaries and/or field notes.
2) Recording and Transcription: interviews were recorded and transcribed verbatim to ensure data fidelity.
3. Data Analysis (Iterative and Detailed Process for Each Case)
1) Reading and Rereading of Transcripts: the researchers deeply familiarized themselves with the data from each individual transcript. A complete immersion in the experience of each participating mother was sought.
2) Initial Annotation (Free Notes): while reading, annotations were made in the margins of the transcripts. These notes were of different types:
(a) Descriptive: summarizing or paraphrasing what the participant stated.
(b) Linguistic: observations regarding language use, pauses, emphasis, etc.
(c) Conceptual/Interpretative: preliminary ideas about meaning, potential emergent themes, connections to the literature or the researchers' reflections.
3) Transformation of Notes into Emergent Themes: free notes were reviewed, and those that appeared to capture the same meaning or experience were grouped. Concise and meaningful names were assigned to these "emergent themes" (or "sub-themes"). This constituted a process of abstraction.
4) Connecting Themes and Seeking Superordinate Themes: patterns and relationships among the emergent themes were sought. Related themes were grouped under broader "superordinate themes," creating a hierarchical structure of meanings.
5) Moving to Interpretation: at this stage, the researchers delved into the "why" behind the experiences and meanings. The concept of double hermeneutics was pursued: the researchers interpreted the interpretations that the participating mothers made of their own breastfeeding experiences. The psychological and emotional significance of the discoveries was explored. A constant connection with the raw data was maintained to ensure that the interpretation was well-founded.
4. Inter-Case Analysis (Synthesis and Comparison)
1) Once the detailed analysis of each individual case was completed, a comparison of the superordinate and emergent themes among the participating mothers was undertaken.
2) Convergences (similarities) and divergences (differences) in experiences and meanings were sought, always preserving the particularity of each case. The objective was not to generalize, but to comprehend the variability and richness of experiences within the two groups of participating mothers (from urban and rural areas).
5. Reporting Findings
1) This article presents a rich and detailed account of the participants' experiences, using significant extracts from the transcripts to illustrate the themes.
2) The narrative in this article was organized around the superordinate themes and their sub-themes, highlighting both similarities and differences between cases.
3) The writing of the findings is compelling, allowing readers to conceive the experience from the perspective of the participating mothers, supported by the researchers' interpretation. The researchers' reflexivity was important, acknowledging their role in the interpretive process.
It is important to note that the Interpretative Phenomenological Analysis method is flexible. This implied moving back and forth between stages (e.g., rereading transcripts while developing themes). The key is a deep immersion in the data, a systematic yet interpretive analysis, and a rich presentation of findings that honors the lived experience of the participating mothers.
2.2. Study Population
The mothers were intentionally selected from a sample involved in a research project on health and nutrition habits within educational communities located across the seven provinces of Costa Rica. This project was conducted by the authors and concluded in 2018.
2.3. Selection Criteria
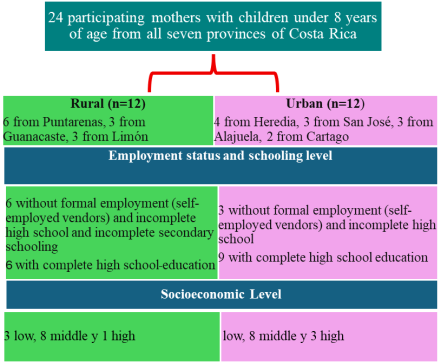
Mothers were included based on the following criteria: (1) having at least one child aged 8 years or younger; and (2) living for over 20 years in either rural or peri-urban areas of Puntarenas, Guanacaste, and Limón, or in urban areas of Heredia, San José, Alajuela, and Cartago.
2.4. Multiple Perspectives
To enhance the depth of the qualitative inquiry, three additional perspectives were incorporated
:
1. Mothers who exclusively breastfed their youngest child for at least four months.
2. Mothers who introduced infant formula feeding to their youngest child within the first three months after birth.
3. Mothers who were willing to share their experiences regarding when, why, and with what types of liquids or solid foods they fed their youngest child.
2.5. Participant Recruitment
A total of 52 mothers who met the inclusion criteria were invited to participate. From these, 24 agreed to take part in the study. Statistical analyses (chi-square test) revealed no significant differences in sociodemographic characteristics between those who participated and those who declined.
2.6. Sample Size
In accordance with IPA, the aim was to obtain a reasonably homogeneous group of 8 to 12 participants per geographic area to allow for an in-depth analysis of the complexity of each individual experience. The final number of participants was determined based on practical considerations related to the period of the study and an interpretative judgment that a “reasonably homogeneous” sample had been achieved
| [21] | Tindall L, Smith J. A, Flowers P, Larkin M. Interpretative Phenomenological Analysis: Theory, Method and Research.: London: Sage. Qualitative Research in Psychology. 2009; 6(4): 346-347. https://doi.org/10.1080/14780880903340091 |
[21]
.
2.7. Variation Within Homogeneity
It is acknowledged that some degree of variation within a homogeneous sample can be useful for comparative purposes and can enhance understanding of how differences contribute to the experiences under study. Considering this, eight participants were initially contacted from each geographic area by intentional selection. If a participant declined or did not answer, others with similar sociodemographic characteristics were invited until 12 participants per area were recruited. While all participants shared common experiences, they differed slightly in terms of educational achievement, employment status, and socioeconomic level. The characteristics of the participating mothers are presented in
Figure 1.
2.8. Data Collection
Face-to-face, semi-structured interviews were conducted at a location selected by each participating mother. All interviews were audio recorded and transcribed (word for word). The researchers-professionals in nutrition, microbiology, education, and psychology, with experience in BF kept reflective journals throughout the study to document their thoughts on each interview, thereby identifying potential biases. The combination of insider and outsider perspectives on BF allowed for the consideration of underlying assumptions in the interpretative process, resulting in a richer analysis
.
2.9. Interview Focus
In alignment with the IPA method, the interviews centered on two principal questions: “How was your BF experience?” and “What were you thinking and how did you feel?”
Follow-up questions were used to explore specific details, emotions, and meanings, such as: “Can you tell me more about (a specific detail)?”, “How did you feel when (a key moment) happened?”, and “What did you mean when you said (a key phrase)?”
2.10. Data Analysis
According to IPA guidelines
| [19] | Duque H, Aristizábal Díaz Granados E. T. Análisis fenomenológico interpretativo: Una guía metodológica para su uso en la investigación cualitativa en psicología. Pensando Psicología. 2019; 15(25): 1-24. https://doi.org/10.16925/2382-3984.2019.01.03 |
[19]
, data analysis was conducted through the following steps:
1. Transcripts were read and re-read to enable deep immersion in the participants’ narratives, while initial reflections were noted.
2. A detailed line-by-line coding process was carried out, classifying text segments into descriptive, emotional, or evaluative codes (e.g., attitudes, beliefs, values).
3. Codes were reviewed and refined until consensus was reached among the researchers. Similar codes were grouped into categories.
4. ATLAS. ti version 23.3.4 was used to facilitate the coding process and the comparison of qualitative data across the two groups of mothers from the analyzed regions.
2.11. Data Interpretation
Following IPA
| [19] | Duque H, Aristizábal Díaz Granados E. T. Análisis fenomenológico interpretativo: Una guía metodológica para su uso en la investigación cualitativa en psicología. Pensando Psicología. 2019; 15(25): 1-24. https://doi.org/10.16925/2382-3984.2019.01.03 |
[19]
, the data were interpreted using the following procedures:
1. During interviews, prior interpretations were “bracketed” to respect the individuality of each case (mother).
2. Themes were compared within and across the regional groups (rural and peri-urban vs. urban) to identify higher-order patterns or themes, which constituted the findings section.
3. Three global connections across categories were identified to construct unifying themes and interpret the mothers’ narratives in both regional groups.
3. Results
The findings revealed three main themes, considering the participants’ geographic area of origin (urban or rural) (
Tables 1-3).
Theme 1. Identified pattern. All mothers expressed a strong desire to breastfeed. However, urban mothers perceived BF as a task that competed with their autonomy and professional roles, whereas rural mothers considered it as an essential part of motherhood. Differences in the perception of the maternal role influenced the decision to continue EBF (
Table 1).
The analysis of events and experiences from the two groups of mothers revealed a striking pattern: both shared a deep belief in BF as the optimal choice for their children. Prior to birth, mothers from both urban and rural/peri-urban areas expressed a strong desire to provide the best for their babies, identifying BF as the ideal path.
Although the intention to breastfeed was common across both groups, the interpretation of BF in the context of motherhood revealed significant differences. Urban mothers viewed BF as a pragmatic choice, focused in scientific evidence positioning it as the optimal nourishment for child development. This decision often became a moral obligation, further influenced by prevailing social expectations.
However, this choice was conflictive with their autonomy and identity as women. BF was often perceived as a barrier for leading an active and fulfilling life. Despite receiving support with domestic tasks and infant care, BF became a source of exhaustion, hindering adequate rest and negatively impacting their mental health.
In contrast, mothers from rural and peri-urban areas associate BF with the fulfillment of motherhood. The act of BF was experienced as personally rewarding-a path for feeling whole and capable. Internal motivation, free from external pressures, enabled them to develop creative strategies to overcome BF challenges. This autonomy allowed them to enjoy the experience and to achieve greater success in EBF.
Therefore, although BF intentions were similar in both groups, the lived experience and interpretation of BF differed significantly, shaped by social context and cultural expectations.
Theme 2. Identified pattern. Many mothers, especially those living in urban areas, reported insecurity feelings regarding their ability to produce enough breast milk. The influence of family members, persistent BF myths, and work-related demands emerged as decisive factors contributing to the early introduction of infant formula (
Table 2).
Both groups of mothers discontinued breastfeeding due to insecurity about their breast milk's quality and quantity, believing it unsatisfied or harmed their children.
In both groups, the introduction of infant formula feeding through bottles emerged as a solution to the exhaustion and distress caused by their infants’ crying. The need to return to work and the influence of the work environment also played a crucial role in the adoption of infant formula feeding. However, the way in which these factors were manifested differed between the two groups.
For mothers from urban areas, external validation as mothers-particularly from their own mothers, partners, and society at large-became significantly important. The perception of social stigma associated with BF in public and advice from their mothers incited them to introduce infant formula, which helped relieve the guilt they felt about this change.
The perceived incompatibility between the demands of BF and their roles as women led many of them to prefer infant formula. The father's role in bottle-feeding became essential to compensate for their inability to breastfeed.
Conversely, while some mothers from rural and peri-urban areas did not maintain exclusive breastfeeding (EBF) for up to six months and chose to use infant formula, they did not completely abandon breastfeeding. Numerous individuals reported that BF was a personally gratifying experience, despite facing challenges and a shortage of external support.
BF was understood not only as nourishment but also as an expression of commitment and love toward the baby-a way of connecting physically and emotionally. It became a form of demonstrating their worth as complete mothers, regardless of external validation.
Therefore, the decision to discontinue BF was influenced by insecurity, the search for practical solutions, and social pressures. However, the interpretation of BF and the value attributed to it varied significantly between the two groups, reflecting the cultural differences and social expectations each group faced.
Theme 3. Identified pattern. Mothers introduced complementary feeding early due to concerns about digestive issues and to facilitate the transition upon returning to work (
Table 3).
The introduction of complementary foods-alongside breast milk or infant formula-revealed a shared pattern among both groups of mothers, marked by the desire to prepare the infant early in anticipation of the mother’s return to work.
The inclusion of “baby cereals,” culturally foreign and non-native products, alongside mashed foods, soups, and drinks-mainly fruit juices and natural beverages-responded to the need to transition the infant toward a more diverse diet, easing the shift to solid foods.
Nevertheless, a latent fear among both urban and rural mothers was that solid foods could cause gastrointestinal issues in their infants. The introduction of teas, such as chamomile, and fruit juices was perceived as a preventive measure to mitigate such risks and protect the infant’s health.
Therefore, the introduction of complementary feeding was characterized by a pursuit of practicality and safety, driven by the need to prepare the infant for the mother’s absence and to prevent potential gastrointestinal problems.
4. Tables
Figure 1. Selection of study participants by geographic area, educational achievement, employment status, and socioeconomic level.
Table 1. Breastfeeding intentions and motherhood experience according to geographic origin.
Urban area | Rural area |
“(...) I didn’t hesitate; I breastfed my children because I wanted to see them beautiful and healthy. Also, I’ve always had a lot of milk, like a good cow, like my sisters-yes, indeed, a lot of milk. So, when they handed her to me, I immediately sticks her on, and I gave her milk, milk, and more milk” (Mother 16, urban area, 2 children, 43 years old, technical education, Office worker (Bank), middle socioeconomic level, married). | “(...) I couldn’t wait to breastfeed again, to feel that again, to protect such a defenseless little creature” (Mother 1, rural or peri-urban area, 2 children, 37 years old, incomplete primary education, Merchant, low socioeconomic level, cohabiting). |
“(...) I never thought about not BF. As he grew up, I noticed the changes and thought now he has the antibodies that will protect him against diseases. We have a nephew who wasn’t breastfed, and he is very, very different from mine-as I said, that cousin is very weak” (Mother 21, urban area, 2 children, 51 years old, university degree, Psychologist, middle socioeconomic level, married)”. | “(...) We want the best for our children; so we expect that (to breastfeed). From what I understand, breast milk is better than powdered milk (infant formula). The nutrition (in BF) is better than that of infant formulas. We don’t know where infant formulas come from, but in the case of breast milk, we know it naturally comes from our own body” (Mother 3, rural or peri-urban area, 1 child, 45 years old, incomplete high school education, Merchant, middle socioeconomic level, married). |
Table 2. Insecurity and perceived convenience as reasons for discontinuing breastfeeding.
Urban area | Rural area |
“(...) I exclusively breastfed for four months, with a few small amounts of infant formula during the first month, and continued BF until almost nine months. That worked well for me and everyone at home, but it was extremely exhausting and emotionally difficult. You don’t feel like you’re living-you’re just surviving, pushing through each day. It felt impossible to feed a baby exclusively for six months. I had to give him infant formula; he cried a lot, and everyone was staring at me, expecting me to fix it” (Mother 17, urban area, 2 children, 41 years old, university degree, Dentist, high socioeconomic status, married). | “(...) I think the first three months were the hardest for me. My nipples are extremely sensitive, and it hurt so much-I couldn’t even touch them. I went to the clinic, and the doctor told me there was nothing he could do and offered me the infant formula option. But I still wanted to continue BF my daughter, and I said: I will not give up and switch to infant formula. So, I kept going until she was six months old, only with my milk, even though it was very painful. I did it, and it brought me and my daughter great happiness. That gave me a deep sense of fulfillment” (Mother 11, rural or peri-urban area, 1 daughter, 38 years old, high school education, Restaurant owner, middle socioeconomic status, married). |
“(...) If you breastfeed, you can't even read a book. You always must be with your baby. There’s no time to relax alone, no personal space-you must constantly be with the baby, and everything hurts! They should remove that from the leaflets-it really does hurt, in any position! I thought, yes, the baby needs to eat, but not only from the breast; so, I also gave him an infant formula and continued like that until four months. My friends have combined infant formula and BF for over a year, which I can’t even imagine BF for that long…” (Mother 24, urban area, 1 child, 38 years old, technical degree, Office worker (Bank), high socioeconomic status, married). | “(...) I love it-I enjoy BF. It makes me feel very maternal (laughs). I find it truly amazing how our bodies produce-what power! And I look at her (my daughter), and I think… my baby is amazing because she was raised with my milk. She was so small, and now she is so big. That makes me feel like the good life lies within us, women. It’s something fathers won’t understand-they’re intolerant and think BF isn’t enjoyable. I say it’s a shame that it lasts so little; I breastfed exclusively for about five months, and now she’s two years old and still sticks onto my breasts (laughs)” (Mother 12, rural or peri-urban area, 2 children, 36 years old, high school education, Waitress, middle socioeconomic status, cohabiting). |
Table 3. Infant preparation and digestive care.
Urban area | Rural area |
“(...) Everyone kept telling me, try this, try that, and it really upset me because I had already tried everything. So, no advice worked for me. Nobody could give me a confident answer as to whether my milk was enough for my baby, until a doctor recommended supplementing with infant formula to correct my baby’s weight loss and jaundice. That’s when I realized my milk wasn’t doing him any good” (Mother 18, from an urban area, 1 daughter, 44 years old, university degree, Teacher, middle socioeconomic status, married). | “(...) I tried to finish quickly (the paperwork from Ministry of Public Education), but he couldn’t stand the hunger. I pumped milk from both breasts, but not much came out. It was terrible for me; I wasn’t a good milk producer. I never hesitated to continue BF, but I also gave him infant formula” (Mother 9, 1 son, 45 years old, university degree, Teacher, middle socioeconomic status, married). |
“(...) I think it would be best if they showed you the worst-case scenario, but all they show you with BF is the ideal, like your milk is amazing. Of course, it would be great because of all the health benefits, but honestly, I wish we were all prepared for BF from a young age. My husband and I hated sitting there like fools thinking, well, there’s nothing to be done if my milk doesn’t satisfy him. We had to switch to infant formula” (Mother 23, from an urban area, 2 children, 36 years old, university degree, Accountant, high socioeconomic status, married). | “(...) I had to pump because I have inverted nipples. It’s very uncomfortable-my nipples would come out for a moment and then go back in. I couldn’t keep it up for months, just about 4, so I also gave him an infant formula. I pumped from both breasts, whatever came out-not much-and it was almost transparent, just to quench his thirst! I wanted to exclusively breastfeed, but I was going to starve him” (Mother 6, from a rural or peri-urban area, 1 son, 45 years old, incomplete high school education, Merchant, middle socioeconomic status, married). |
“(...) I’ve always worked independently, with clients. You see mothers using blankets, completely covering their babies. I thought, what if I bring mine and breastfeed here? Will I lose clients? I’ll look like a desperate mom who will do anything to make money. My husband said, 'You only need to breastfeed in front of X' (his best friend). I don’t know, I don’t think BF is sexy; it’s not sexualized-it's just a baby nursing from its mother. But I don't recall seeing it here or abroad. So, to avoid issues with my clients, husband, I gave him infant formula with a bottle for two months old” (Mother 19, from an urban area, 1 son, 43 years old, high school education, Liquor store owner, middle socioeconomic status, married). | “(...) I felt a lot of pain down there, almost to cry. Using the bathroom was terrible, and BF hurt a lot. I thought, am I the only woman going through this? My mother comforted me and said: ‘It’s okay, look at your younger brother-he was fed both BF and infant formula and grew up just fine; he was always the tallest in class.’ So, I talked to my baby, saying, let's do this, help me out (laughs). I didn’t stop BF, but yes, I also gave infant formula” (Mother 4, from a rural or peri-urban area, 3 children, 49 years old, incomplete high school education, Merchant, middle socioeconomic status, married). |
“(...) My mom told me, BF is the best vitamin for babies, they don’t even need water when nursing, and my partner (my companion and friend), he had to be aware of what was happening. So, the three of us decided to give the baby a bottle with infant formula or natural juices at night and some of my milk during the day. I started to sleep well, and eventually, the baby only wanted the bottle” (Mother 22, from an urban area, 1 son, 41 years old, technical level education, Optometrist, middle socioeconomic status, cohabiting). | “(...) The nurses gave us BF advice and helped us nurse the babies; before that, they trained us and explained how to breastfeed right after delivery. But once you’re discharged, doubts flood and, of course, the nurse isn’t there anymore. I thought, I’m not going to let him cry from hunger, so I gave him some infant formula, but also my milk, after four months. I know it’s not ideal, but infant formula is a relieving option” (Mother 2, from a rural or peri-urban area, 2 children, 44 years old, primary education, Merchant, low socioeconomic status, cohabiting). |
5. Discussion
The findings of this study demonstrate that BF is a complex practice that transcends biological processes, being deeply intertwined with culture, social structures, and women’s subjective experiences. In this regard, BF can be interpreted as an act of female empowerment, reaffirming women’s ability to nourish and care for their children. However, it may also be perceived as an imposition that limits autonomy and reinforces traditional gender roles
| [24] | Augusto A, Neves DM, Henriques V. Breastfeeding experiences and women's self-concept: Negotiations and dilemmas in the transition to motherhood. Front Sociol. 2023 Apr 5; 8: 1130808. https://doi.org/10.3389/fsoc.2023.1130808 |
[24]
. This ambivalence reflects the inherent tensions within the social constructions of motherhood and femininity.
The dominant discourse surrounding BF, often centered solely on the benefits of breast milk for the infant, tends to darken the individual and social contexts in which BF takes place
. The mothers’ narratives in this study reveal that while the intention to breastfeed is common, there are structural and sociocultural factors that shape the practice. Among these, the perception of breast milk sufficiency stands out, as it can trigger anxiety and lead to the premature introduction of infant formula
| [26] | Bürger B, Schindler K, Tripolt T, Griesbacher A, Stüger HP, Wagner KH, Weber A, Wolf-Spitzer A. Factors Associated with (Exclusive) Breastfeeding Duration-Results of the SUKIE-Study. Nutrients. 2022 Apr 20; 14(9): 1704. https://doi.org/10.3390/nu14091704 |
[26]
. This perception-often fueled by myths and misinformation-may be exacerbated by the lack of support and guidance from health professionals, many of whom are not adequately trained to address the emotional and social dimensions of BF
| [27] | Ojantausta O, Pöyhönen N, Ikonen R, Kaukonen M. Health professionals’ competencies regarding breastfeeding beyond 12 months: A systematic review. International Breastfeeding Journal. 2023; 18(1): 55. https://doi.org/10.1186/s13006-023-00591-z |
[27]
.
From a gender perspective, it is essential to acknowledge that BF is not a universal or homogeneous experience. Socioeconomic, ethnic, cultural, and generational differences influence how women perceive and experience BF. In this sense, intersectionality provides a critical analytical lens to understand how these intersecting dimensions shape differentiated experiences
. For instance, migrant women may face additional barriers in accessing BF support and information, due to language, cultural differences, and discrimination. Self-Determination Theory offers a useful framework to understand how autonomy, competence, and relatedness are fundamental to maternal intrinsic motivation and well-being
. Supporting maternal autonomy in BF decisions, providing accurate information and emotional support, and promoting the development of social support networks are key strategies to promote successful BF.
It has been demonstrated that autonomous motivation during pregnancy predicts higher rates of EBF at six weeks postpartum, as well as improved maternal well-being and self-efficacy. Support should include both BF and infant care skills, as well as emotional preparation for parenting. Maternal confidence during the early postpartum period is particularly vulnerable to the perception of insufficient milk supply, a concern that is prevalent among mothers worldwide
.
Furthermore, BF difficulties can lead to significant maternal distress, including anxiety and postpartum depression
| [31] | Modak A, Ronghe V, Gomase KP, Mahakalkar MG, Taksande V. A Comprehensive Review of Motherhood and Mental Health: Postpartum Mood Disorders in Focus. Cureus. 2023 Sep 29; 15(9): e46209. https://doi.org/10.7759/cureus.46209 |
[31]
. Positive support experiences have been shown to modulate maternal stress and improve BF outcomes
| [32] | Chaput KH, Nettel-Aguirre A, Musto R, Adair CE, Tough SC. Breastfeeding difficulties and supports and risk of postpartum depression in a cohort of womenwho have given birth in Calgary: a prospective cohort study. CMAJ Open. 2016 Mar 21; 4(1): E103-9. https://doi.org/10.9778/cmajo.20150009 |
[32]
. Therefore, it is crucial for mothers to have access to BF and mental health support services, such as the Breastfeeding and Child Development Clinics of the Costa Rican Social Security (Caja Costarricense de Seguro Social).
The workplace represents another major challenge for BF mothers. Urban mothers face greater difficulty reconciling BF with professional responsibilities. The implementation of supportive workplace policies-such as lactation rooms, flexible schedules, and extended maternity leave-is essential to ensure women’s right to breastfeed without having to forgo their professional development
| [33] | UNICEF. (2019). Lactancia materna y políticas orientadas a la familia: Un informe de evidencias. Fondo de las Naciones Unidas para la Infancia. Available from: Lactancia Materna y Politicas Orientadas a la Familia (pdf, 703 KB). |
[33]
. Some mothers in this study believed it was better to introduce a combination of BF and infant formula feeding early on to train their infants to accept bottles in preparation for returning to work. This practice was partially driven by the perception among participating mothers that exclusively breastfed infants may become “dependent on breast milk,” making weaning more difficult. Faced with the risk of losing job security and while reaffirming their identities as working women, these mothers found it imperative to negotiate ways to accommodate both employment and BF.
For most women in this study, combining BF with infant formula feeding-or offering expressed breast milk primarily through bottles-was viewed as the most viable alternative to EBF. This approach provided some relief from the demands of BF, allowing the mother to pursue other priorities while ensuring the infant still received “some” breast milk. By examining the experiences of rural and peri-urban mothers who breastfed exclusively and those who did not, this study shows that reconciling other identities with BF and motherhood is essential to encouraging persistence with BF and promoting maternal confidence and enjoyment-both of which are crucial for sustaining the practice.
From a cultural standpoint, significant differences were observed in how BF is perceived across socioeconomic sectors. In rural and peri-urban areas, BF remains a main component of motherhood, whereas in urban areas, pressures to meet expectations of independence and productivity may undermine sustained BF practices. It is vital to recognize and respect these cultural differences, avoiding the imposition of a single model of motherhood or BF
| [34] | Romero Morales, P. P., Zúñiga Torres, M., & Sánchez Delgado, M. (2023). Factores socioculturales que influyen en la práctica de la lactancia y la alimentación de la madre en una comunidad semiurbana de México. Población y Salud en Mesoamérica, 21(1). https://doi.org/10.15517/psm.v21i1.52851 |
[34]
. Maternal identity is closely tied to socially constructed ideals of good parenting. The dominant parenting discourse in many Western societies, including Costa Rica, defines “good” or “ideal” motherhood as a role in which women are primarily responsible for child-care, guided by healthcare personnel who focus predominantly on the child’s health
. BF, promoted as the best way to nourish an infant, has become a measure for many women of how well they perform as mothers, making it a critical aspect of their maternal identity.
The experiences of women in this study, as well as those reported elsewhere, highlight deeper conflicts regarding the construction of motherhood. Some mothers found breastfeeding challenging and therefore opted to use infant formulas. Participants expressed mixed views on how BF breastfeeding aligns with motherhood. Some maintained a pragmatic approach to infant feeding, viewing BF as just one way to nourish a child, and appeared largely unaffected by societal pressure to be the “ideal mother.” Others internalized the notion that “breast is best” and experienced BF as meaningful and deeply fulfilling. Nevertheless, most urban mothers remained in conflict about how to integrate BF with the realities of women’s social and professional lives. This tension shows the competing demands of the maternal ideal, which requires mothers to successfully breastfeed while also fulfilling multiple roles at home, in society, and in the workplace. The “good mother” ideology implicitly expects women to sacrifice their individual ambitions for the benefit of their child
.
Studies have shown that mothers experience significant social pressure to breastfeed, and deviating from this standard often requires a redefinition of maternal identity
. The influence of cultural standards on BF is complex and requires a deep understanding of the values and beliefs within different communities
| [38] | EjieI. L, ElejeG. U, Chibuzor M. T, Anetoh M. U, Nduka I. J, Umeh I. B, Ogbonna B. O, Ekwunife O. I. A systematic review of qualitative research on barriers and facilitators to exclusive breastfeeding practice in sub-Saharan African countries. International Breastfeeding Journal. 2021; 16: 44. https://doi.org/10.1186/s13006-021-00380-6 |
[38]
.
The dialogue between health services and maternal demand must focus on understanding how Costa Rican women assign diverse meanings to BF. Such understanding can assist healthcare professionals in interpreting early infant feeding behaviors and providing custom made support strategies. Maternal self-doubt regarding milk production may be exacerbated by the lack of professional support and guidance
| [27] | Ojantausta O, Pöyhönen N, Ikonen R, Kaukonen M. Health professionals’ competencies regarding breastfeeding beyond 12 months: A systematic review. International Breastfeeding Journal. 2023; 18(1): 55. https://doi.org/10.1186/s13006-023-00591-z |
[27]
. This perception-often driven by myths and misinformation-could be mitigated through educational programs and ongoing support during the lactation period, as evidenced by recent studies that underscore the importance of maternal-child health education
| [39] | Ramos-Pla A, Fornons Casol L. Health Education in Early Childhood Education: A Systematic Review of Literature. Societies. 2025; 15(4): 106. https://doi.org/10.3390/soc15040106 |
[39]
.
BF education-including information about milk production, proper techniques, and management of common issues-has proven to be a critical factor in extending BF duration
| [40] | Araya P, López-Alegría F. Intervenciones efectivas para aumentar la duración y la exclusividad de la lactancia materna: una revisión sistemática. Revista Chilena de Obstetricia y Ginecología. 2022; 87(1): 26-35. https://doi.org/10.24875/RECHOG.21000001 |
[40]
. However, professional education alone may not be sufficient to alleviate maternal anxiety about milk sufficiency. Previous studies have shown that peer support plays an important role in BF duration
| [41] | Cameron AJ, Hesketh K, Ball K, Crawford D, Campbell KJ. Influence of peers on breastfeeding discontinuation among new parents: the Melbourne InFANT Program. Pediatrics. 2010 Sep; 126(3): e601-7. https://doi.org/10.1542/peds.2010-0771 |
| [42] | Sudfeld CR, Fawzi WW, Lahariya C. Peer support and exclusive breastfeeding duration in low and middle-income countries: a systematic review and meta-analysis. PLoS One. 2012; 7(9): e45143. https://doi.org/10.1371/journal.pone.0045143 |
[41, 42]
. Additionally, education on how to objectively assess milk adequacy and infant development could help reduce maternal concerns.
Ongoing follow-up is necessary to support mothers in resuming EBF, as neglecting this may reinforce the belief of milk insufficiency. Strengthening family relationships is another vital strategy to promote maternal identification with BF, even beginning during pregnancy
| [43] | Ramos IF, Campos B, Schetter CD. Pregnancy Anxiety and Beliefs Surrounding Motherhood in Latinas: A Qualitative Study. J Lat Psychol. 2022 Nov; 10(4): 277-290. https://doi.org/10.1037/lat0000208 |
[43]
. This study found that mothers often experience low emotional support during the early postpartum period due to family conflict and/or lack of partner involvement. Healthcare professionals can help strengthen family ties by including partners and grandmothers in BF education and support during the perinatal period. Involving key family members may reduce disagreements about what, when, why, and how to breastfeed. Furthermore, BF education should emphasize the unique benefits of this practice for fostering the mother-infant bond.
Literature recognizes that BF goes beyond the transfer of nutrients from mother to child; it embodies deeper values and identities embedded within a woman’s specific social and cultural context
. Maternal identity is closely tied to socially constructed ideals of good parenting. The dominant discourse on parenting in many Western cultures, including Costa Rica, defines ideal motherhood as a role where women are primarily responsible for child-care, guided by health personnel who focus predominantly on the child’s health
.
Critics have noted that these ideals of good motherhood conflict with cultural expectations that women should also succeed professionally
. Maternal identity conflict refers to the tension involved in meeting the demands of BF while simultaneously maintaining other social roles as wives, workers, and independent individuals
. Addressing these challenges requires a comprehensive approach that incorporates education, institutional and cultural support to promote sustained BF in Costa Rica. A multisectoral approach-engaging healthcare professionals, partners, communities, and cultural leaders-is essential for creating an environment that supports and encourages BF
.
Strengths and limitations
The use of IPA to examine the BF experiences of a sample of 24 mothers enabled a deeper understanding of the phenomenon within its context. Moreover, the inclusion of perspectives from both EBF and non-EBF practices, as well as complementary feeding, highlighted key areas to support Costa Rican mothers.
One limitation was the potential for recall bias due to differences in the time elapsed since the BF experience. Longer recall periods may reduce the vividness and detail of memories and reflections.
6. Conclusions
This study explored BF experiences among Costa Rican mothers, with a particular focus on how these experiences related to their maternal identity. The integration of BF into their maternal identity emerged as an important motivator and a factor contributing to self-efficacy, enabling some mothers to overcome initial BF challenges and derive satisfaction from the practice. However, the tensions between BF demands and identities outside of motherhood were prevalent and contributed to significant maternal stress.
The findings underscore the importance of adopting a gender-sensitive and human rights-based approach to BF promotion. It is essential to recognize that BF is a personal and autonomous decision for each woman, and that this choice should be respected and supported regardless of socioeconomic, cultural, or occupational context.
Based on the findings, the promotion of BF in Costa Rica requires a multidimensional approach that addresses individual, social, and structural factors. Therefore, it is necessary to:
1. Implement workplace-friendly strategies, such as extended maternity license and appropriate facilities for breast milk expression and storage.
2. Strengthen prenatal and postnatal education programs by incorporating a gender and human rights perspective, to empower mothers and reduce anxiety about milk sufficiency.
3. Involve partners and support networks in the BF process, acknowledging their role in sustaining BF and promoting shared responsibility in childcare.
4. Promote awareness campaigns in the business sector and in society to present BF as a right rather than merely an option, and to challenge gender stereotypes that restrict women’s autonomy.
5. Ensure access to comprehensive and high-quality healthcare services that include BF support and maternal mental health care.
6. Promote BF research from a gender and human rights perspective, for a better understanding of women's experiences and needs, and to generate evidence for the development of more effective public policies.
The findings and recommendations of this study may contribute to the formulation of more effective public policies that support maternal child health and advance BF goals at both national and international levels. A gender-sensitive and human rights-based approach helps ensure that all women can breastfeed, benefiting their health and their children's.
Abbreviations
BF | Breastfeeding |
EBF | Exclusive BF |
IPA | Interpretative Phenomenological Analysis |
SDG | Sustainable Development Goals |
WHO | World Health Organization |
Acknowledgments
We are deeply grateful to all the participating mothers, who generously and candidly shared their reflections and lived experiences of breastfeeding in Costa Rica, making this phenomenological analysis possible.
Ethical Responsibilities
The authors declare that all procedures performed in this study complied with the ethical standards of the Responsible Human Experimentation Committee, the principles of the World Medical Association and the Helsinki Declaration. Likewise, the authors declare that they followed the institutional protocols regarding the publication of participant data and that they obtained informed consent from the mothers referenced in this article.
Author Contributions
Hilda Patricia Núñez-Rivas: made substantial contributions to the conception and design of the study; to the acquisition, analysis, and interpretation of data; to the drafting of the manuscript; and to the critical revision of its significant intellectual content. She provided final approval for the version to be published and agrees to be accountable for all aspects of the work, ensuring that any questions related to the accuracy or integrity of any part of the manuscript are appropriately investigated and resolved.
Marlene Roselló-Araya: contributed to the analysis and interpretation of the data; to the drafting of the manuscript; and to the critical revision of its significant intellectual content. They provided final approval for the version to be published and agree to be accountable for all aspects of the work, ensuring that any questions related to the accuracy or integrity of any part of the manuscript are appropriately investigated and resolved.
Ileana Holst-Schumacher: contributed to the analysis and interpretation of the data; to the drafting of the manuscript; and to the critical revision of its significant intellectual content. They provided final approval for the version to be published and agree to be accountable for all aspects of the work, ensuring that any questions related to the accuracy or integrity of any part of the manuscript are appropriately investigated and resolved.
Natalia Campos-Saborío: contributed to the analysis and interpretation of the data; to the drafting of the manuscript; and to the critical revision of its significant intellectual content. They provided final approval for the version to be published and agree to be accountable for all aspects of the work, ensuring that any questions related to the accuracy or integrity of any part of the manuscript are appropriately investigated and resolved.
Funding
This work was supported by the Costa Rican Institute for Nutrition and Health Research and Teaching (INCIENSA; IC-2010-05), the University of Costa Rica (UCR; 430-B1-343), and the State University of Costa Rica (UNED; V-INVES/2010-012). No external funding was received from any agency, commercial sector, or non-governmental organization.
Data Availability Statement
The data supporting the findings of this research are included in this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Victora CG, Bahl R, Barros AJ, França GV, Horton S, Krasevec J, Murch S, Sankar MJ, Walker N, Rollins NC; Lancet Breastfeeding Series Group. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016; 387(10017): 475-90.
https://doi.org/10.1016/S0140-6736(15)01024-7
|
| [2] |
Horta B, Victora C, World Health Organization. (2013). Long-term effects of breastfeeding: a systematic review. World Health Organization.
https://iris.who.int/handle/10665/79198
|
| [3] |
Alotiby AA. The role of breastfeeding as a protective factor against the development of the immune-mediated diseases: A systematic review. Front Pediatr. 2023 Feb 16; 11: 1086999.
https://doi.org/10.3389/fped.2023.1086999
|
| [4] |
Grantham-McGregor S, Cheung YB, Cueto S, Glewwe P, Richter L, Strupp B; International Child Development Steering Group. Developmental potential in the first 5 years for children in developing countries. Lancet. 2007 Jan 6; 369(9555): 60-70.
https://doi.org/10.1016/S0140-6736(07)60032-4
|
| [5] |
World Health Organization (WHO) & United Nations Children’s Fund (UNICEF). (2017). Global Breastfeeding Scorecard, 2017: Tracking Progress for Breastfeeding Policies and Programmes. Geneva: WHO. Available from:
https://www.who.int/publications/m/item/global-breastfeeding-scorecard-2017-tracking-progress-for-breastfeeding-policies-and-programmes
|
| [6] |
Fraile Isart A, Cao Torija M. J. Lactancia materna con perspectiva de género. Revista De Lactancia Materna. 2023; 1(1): e31040.
https://doi.org10.14201/rlm.31040
|
| [7] |
Cunill-Grau N. La intersectorialidad en las nuevas políticas sociales: Un acercamiento analítico-conceptual. Gestión y política pública. 2014; 23(1): 5-46. [accessed Wednesday, May 21, 2025]. Available from:
http://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S1405-10792014000100001&lng=es&tlng=es
|
| [8] |
Gitz E. Lactancia materna: debates teóricos sobre su presencia en la identidad femenina y en las representaciones de la buena maternidad. Revista Científica de UCES. 2020; 25(2): 87-105. [accessed Wednesday, May 21, 2025]. Available from
https://publicacionescientificas.uces.edu.ar/index.php/cientifica/article/view/848
|
| [9] |
Van T, Varadi D, Adams AC, Feldman-Winter L. Promotion, Protection, and Support of Breastfeeding as a Human Right: A Narrative Review. Breastfeed Med. 2023 Aug; 18(8): 561-570.
https://doi.org/10.1089/bfm.2023.0061
|
| [10] |
UNICEF. (2020). UNICEF. (2020, agosto). World Breastfeeding Week 2020: Breastfeeding practices worldwide. United Nations Children’s Fund.
https://data.unicef.org/resources/world-breastfeeding-week-2020/
|
| [11] |
World Health Organization. (2021). World Health Organization. (2021). Global breastfeeding scorecard, 2021: Protecting breastfeeding through bold national actions during the COVID-19 pandemic and beyond (WHO/HEP/NFS/21.45).
https://www.who.int/publications/i/item/WHO-HEP-NFS-21.45
|
| [12] |
Organización de las Naciones Unidas para la Alimentación y la Agricultura (FAO). (2022). Indicadores nutricionales adicionales de la Asamblea Mundial de la Salud: Prevalencia de la lactancia materna exclusiva durante los primeros seis meses de vida. En Estadísticas regionales de seguridad alimentaria y nutrición 2022 - América Latina y el Caribe (Sección 3.2). FAO.
https://openknowledge.fao.org/server/api/core/bitstreams/efefa9bb-2deb-4f04-944b-f805532d4aee/content/sofi-statistics-rlc-2022/breastfeeding-first-six-months.html
|
| [13] |
Ministerio de Salud, Instituto Nacional de Estadística y Censos (INEC) y Fondo de las Naciones Unidas para la Infancia (UNICEF). (2018). Encuesta de Mujeres, Niñez y Adolescencia (EMNA): Informe de resultados de la encuesta. San José, Costa Rica. [accessed Wednesday, May 21, 2025]. Available from: Available from:
https://www.unicef.org/costarica/media/436/file/Encuesta-de-mujeres-ninez-y-adolescencia-2018.pdf
|
| [14] |
Ministerio de Salud, INCIENSA. Caja Costarricense de Seguro Social. Encuesta basal comunidades centinela en alimentación y nutrición 1999-2000. San José, Costa Rica: Ministerio de Salud; 2002. [accessed Wednesday, May 21, 2025]. Available from:
https://www.binasss.sa.cr/Cendamas.pdf
|
| [15] |
Morice AC. Lactancia natural en Costa Rica: tendencias y factores de riesgo, período 1975 a 1990. Comisión Nacional de Lactancia Materna, INCAP/OPS. Publicación INCAP ME/027. Centro de Desarrollo Social; 1992. [accessed Wednesday, May 21, 2025]. Available from: Available from:
https://bvssan.incap.int/local/M/ME-027.pdf
|
| [16] |
Machado Cruz V, Chaves Quirós S, Pérez Gutiérrez E. Lactancia Materna en Costa Rica, Tendencias y Desafíos Período 1990-1998. Departamento de Medicina Preventiva, Sección Salud del Niño, Caja Costarricense de Seguro Social, San José, Costa Rica. Revista Costarricense de Epidemiología. 2005 [accessed Wednesday, May 21, 2025]. Available from:
https://www.binasss.sa.cr/revistas/epidemiologia/v1n2/art3.pdf
|
| [17] |
Chiang KV, Li R, Anstey EH, Perrine CG. Racial and Ethnic Disparities in Breastfeeding Initiation ─ United States, 2019. MMWR Morb Mortal Wkly Rep 2021; 70: 769-774.
https://doi.org/10.15585/mmwr.mm7021a1
|
| [18] |
Subramani S. Beyond Public Health and Private Choice: Breastfeeding, Embodiment and Public Health Ethics. Asian Bioeth Rev. 2024 Oct 26; 16(2): 249-266.
https://doi.org/10.1007/s41649-023-00259-0
|
| [19] |
Duque H, Aristizábal Díaz Granados E. T. Análisis fenomenológico interpretativo: Una guía metodológica para su uso en la investigación cualitativa en psicología. Pensando Psicología. 2019; 15(25): 1-24.
https://doi.org/10.16925/2382-3984.2019.01.03
|
| [20] |
Larkin M, Shaw R, Flowers P. Multiperspectival designs and processes in interpretative phenomenological analysis research. Qual. Res. Psychol 2018; 16(2): 182-198.
https://doi.org/10.1080/14780887.2018.1540655
|
| [21] |
Tindall L, Smith J. A, Flowers P, Larkin M. Interpretative Phenomenological Analysis: Theory, Method and Research.: London: Sage. Qualitative Research in Psychology. 2009; 6(4): 346-347.
https://doi.org/10.1080/14780880903340091
|
| [22] |
Clancy M. Is reflexivity the key to minimising problems of interpretation in phenomenological research? Nurse Res. 2013 Jul; 20(6): 12-6.
https://doi.org/10.7748/nr2013.07.20.6.12.e1209
|
| [23] |
Berger R. Now I see it, now I don’t: researcher’s position and reflexivity in qualitative research. Qual. Res. 2015; 15(2): 219-234.
https://doi.org/10.1177/1468794112468475
|
| [24] |
Augusto A, Neves DM, Henriques V. Breastfeeding experiences and women's self-concept: Negotiations and dilemmas in the transition to motherhood. Front Sociol. 2023 Apr 5; 8: 1130808.
https://doi.org/10.3389/fsoc.2023.1130808
|
| [25] |
Turco F. To be Mother or not? Cultural Models of Motherhood and Their Meaning Effects on Gendered Representations. Int J Semiot Law. 2022; 35(4): 1393-1406.
https://doi.org/10.1007/s11196-021-09831-z
|
| [26] |
Bürger B, Schindler K, Tripolt T, Griesbacher A, Stüger HP, Wagner KH, Weber A, Wolf-Spitzer A. Factors Associated with (Exclusive) Breastfeeding Duration-Results of the SUKIE-Study. Nutrients. 2022 Apr 20; 14(9): 1704.
https://doi.org/10.3390/nu14091704
|
| [27] |
Ojantausta O, Pöyhönen N, Ikonen R, Kaukonen M. Health professionals’ competencies regarding breastfeeding beyond 12 months: A systematic review. International Breastfeeding Journal. 2023; 18(1): 55.
https://doi.org/10.1186/s13006-023-00591-z
|
| [28] |
Collins, P. H. (2019). Intersectionality as critical social theory. Duke University Press.
https://doi.org/10.1057/s41296-021-00490-0
|
| [29] |
Kestler-Peleg M, Shamir-Dardikman M, Hermoni D, Ginzburg K. Breastfeeding motivation and Self-Determination Theory. Soc Sci Med. 2015 Nov; 144: 19-27.
https://doi.org/10.1016/j.socscimed.2015.09.006
|
| [30] |
Gatti L. Maternal perceptions of insufficient milk supply in breastfeeding. J Nurs Scholarsh. 2008; 40(4): 355-63.
https://doi.org/10.1111/j.1547-5069.2008.00234.x
|
| [31] |
Modak A, Ronghe V, Gomase KP, Mahakalkar MG, Taksande V. A Comprehensive Review of Motherhood and Mental Health: Postpartum Mood Disorders in Focus. Cureus. 2023 Sep 29; 15(9): e46209.
https://doi.org/10.7759/cureus.46209
|
| [32] |
Chaput KH, Nettel-Aguirre A, Musto R, Adair CE, Tough SC. Breastfeeding difficulties and supports and risk of postpartum depression in a cohort of womenwho have given birth in Calgary: a prospective cohort study. CMAJ Open. 2016 Mar 21; 4(1): E103-9.
https://doi.org/10.9778/cmajo.20150009
|
| [33] |
UNICEF. (2019). Lactancia materna y políticas orientadas a la familia: Un informe de evidencias. Fondo de las Naciones Unidas para la Infancia. Available from: Lactancia Materna y Politicas Orientadas a la Familia (pdf, 703 KB).
|
| [34] |
Romero Morales, P. P., Zúñiga Torres, M., & Sánchez Delgado, M. (2023). Factores socioculturales que influyen en la práctica de la lactancia y la alimentación de la madre en una comunidad semiurbana de México. Población y Salud en Mesoamérica, 21(1).
https://doi.org/10.15517/psm.v21i1.52851
|
| [35] |
Donath O, Berkovitch N, Segal-Engelchin D. “I Kind of Want to Want”: Women Who Are Undecided About Becoming Mothers. Front Psychol. 2022 Apr 7; 13: 848384.
https://doi.org/10.3389/fpsyg.2022.848384
|
| [36] |
Marshall JL, Godfrey M, Renfrew MJ. Being a 'good mother': managing breastfeeding and merging identities. Soc Sci Med. 2007 Nov; 65(10): 2147-59.
https://doi.org/10.1016/j.socscimed.2007.06.015
|
| [37] |
Lee E. Health, morality, and infant feeding: British mothers' experiences of formula milk use in the early weeks. Sociol Health Illn. 2007 Nov; 29(7): 1075-90.
https://doi.org/10.1111/j.1467-9566.2007.01020.x
|
| [38] |
EjieI. L, ElejeG. U, Chibuzor M. T, Anetoh M. U, Nduka I. J, Umeh I. B, Ogbonna B. O, Ekwunife O. I. A systematic review of qualitative research on barriers and facilitators to exclusive breastfeeding practice in sub-Saharan African countries. International Breastfeeding Journal. 2021; 16: 44.
https://doi.org/10.1186/s13006-021-00380-6
|
| [39] |
Ramos-Pla A, Fornons Casol L. Health Education in Early Childhood Education: A Systematic Review of Literature. Societies. 2025; 15(4): 106.
https://doi.org/10.3390/soc15040106
|
| [40] |
Araya P, López-Alegría F. Intervenciones efectivas para aumentar la duración y la exclusividad de la lactancia materna: una revisión sistemática. Revista Chilena de Obstetricia y Ginecología. 2022; 87(1): 26-35.
https://doi.org/10.24875/RECHOG.21000001
|
| [41] |
Cameron AJ, Hesketh K, Ball K, Crawford D, Campbell KJ. Influence of peers on breastfeeding discontinuation among new parents: the Melbourne InFANT Program. Pediatrics. 2010 Sep; 126(3): e601-7.
https://doi.org/10.1542/peds.2010-0771
|
| [42] |
Sudfeld CR, Fawzi WW, Lahariya C. Peer support and exclusive breastfeeding duration in low and middle-income countries: a systematic review and meta-analysis. PLoS One. 2012; 7(9): e45143.
https://doi.org/10.1371/journal.pone.0045143
|
| [43] |
Ramos IF, Campos B, Schetter CD. Pregnancy Anxiety and Beliefs Surrounding Motherhood in Latinas: A Qualitative Study. J Lat Psychol. 2022 Nov; 10(4): 277-290.
https://doi.org/10.1037/lat0000208
|
| [44] |
Crossley ML. Breastfeeding as a moral imperative: an autoethnographic study, Fem. Psychol. 2009; 19(1): 71-87.
https://doi.org/10.1177/0959353508098620
|
| [45] |
Franco, S. The Cultural Contradictions of Motherhood. The Journal of Clinical Psychiatry. 2000; 61(7): 530-531. [accessed Wednesday, May 21, 2025]. Available from:
https://scispace.com/pdf/the-cultural-contradictions-of-motherhood-1n44qy3dkv.pdf/
|
| [46] |
UNICEF. (2023). Early Childhood Development: UNICEF Vision for Every Child. Nueva York: Fondo de las Naciones Unidas para la Infancia (UNICEF). Available from:
https://www.unicef.org/reports/early-childhood-development-unicef-vision-every-child
|
Cite This Article
-
APA Style
Núñez-Rivas, H. P., Holst-Schumacher, I., Roselló-Araya, M., Campos-Saborío, N. (2025). Challenges and Key Factors of Breastfeeding in Costa Rica Listening to Mothers' Voices: A Phenomenological Analysis. Science Journal of Public Health, 13(5), 269-282. https://doi.org/10.11648/j.sjph.20251305.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Núñez-Rivas, H. P.; Holst-Schumacher, I.; Roselló-Araya, M.; Campos-Saborío, N. Challenges and Key Factors of Breastfeeding in Costa Rica Listening to Mothers' Voices: A Phenomenological Analysis. Sci. J. Public Health 2025, 13(5), 269-282. doi: 10.11648/j.sjph.20251305.13
Copy
|
Download
AMA Style
Núñez-Rivas HP, Holst-Schumacher I, Roselló-Araya M, Campos-Saborío N. Challenges and Key Factors of Breastfeeding in Costa Rica Listening to Mothers' Voices: A Phenomenological Analysis. Sci J Public Health. 2025;13(5):269-282. doi: 10.11648/j.sjph.20251305.13
Copy
|
Download
-
@article{10.11648/j.sjph.20251305.13,
author = {Hilda Patricia Núñez-Rivas and Ileana Holst-Schumacher and Marlene Roselló-Araya and Natalia Campos-Saborío},
title = {Challenges and Key Factors of Breastfeeding in Costa Rica Listening to Mothers' Voices: A Phenomenological Analysis
},
journal = {Science Journal of Public Health},
volume = {13},
number = {5},
pages = {269-282},
doi = {10.11648/j.sjph.20251305.13},
url = {https://doi.org/10.11648/j.sjph.20251305.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjph.20251305.13},
abstract = {Objective: To analyze the current state of breastfeeding in Costa Rica by examining key indicators and identifying profiles of mothers at risk, to understand the factors influencing breastfeeding decisions and to propose evidence-based interventions in maternal and child health policies. Methodology: A qualitative study with an interpretative phenomenological approach was conducted. The lived experiences of 24 mothers from diverse regions across the country were explored and analyzed. Results: The findings reveal that, although both rural and urban mothers share a strong intention to breastfeed, they face different challenges. Perceptions of motherhood, insecurity regarding milk production, and employment-related obstacles significantly influence the time and exclusivity of breastfeeding. Urban mothers often encounter more pronounced work-related barriers, while rural mothers report limited access to professional support. Maternal education and the availability of postnatal support emerged as critical factors in sustaining breastfeeding practices. Conclusions: Strengthening postnatal support systems, enhancing maternal education, and developing strategies to reconcile breastfeeding with employment demands are essential. These measures could improve national breastfeeding indicators and help close socioeconomic gaps among mothers in different contexts.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Challenges and Key Factors of Breastfeeding in Costa Rica Listening to Mothers' Voices: A Phenomenological Analysis
AU - Hilda Patricia Núñez-Rivas
AU - Ileana Holst-Schumacher
AU - Marlene Roselló-Araya
AU - Natalia Campos-Saborío
Y1 - 2025/09/23
PY - 2025
N1 - https://doi.org/10.11648/j.sjph.20251305.13
DO - 10.11648/j.sjph.20251305.13
T2 - Science Journal of Public Health
JF - Science Journal of Public Health
JO - Science Journal of Public Health
SP - 269
EP - 282
PB - Science Publishing Group
SN - 2328-7950
UR - https://doi.org/10.11648/j.sjph.20251305.13
AB - Objective: To analyze the current state of breastfeeding in Costa Rica by examining key indicators and identifying profiles of mothers at risk, to understand the factors influencing breastfeeding decisions and to propose evidence-based interventions in maternal and child health policies. Methodology: A qualitative study with an interpretative phenomenological approach was conducted. The lived experiences of 24 mothers from diverse regions across the country were explored and analyzed. Results: The findings reveal that, although both rural and urban mothers share a strong intention to breastfeed, they face different challenges. Perceptions of motherhood, insecurity regarding milk production, and employment-related obstacles significantly influence the time and exclusivity of breastfeeding. Urban mothers often encounter more pronounced work-related barriers, while rural mothers report limited access to professional support. Maternal education and the availability of postnatal support emerged as critical factors in sustaining breastfeeding practices. Conclusions: Strengthening postnatal support systems, enhancing maternal education, and developing strategies to reconcile breastfeeding with employment demands are essential. These measures could improve national breastfeeding indicators and help close socioeconomic gaps among mothers in different contexts.
VL - 13
IS - 5
ER -
Copy
|
Download