Drug-induced agranulocytosis (DIAG) is a rare but potentially fatal hematological complication. Thiopurines, such as mercaptopurine (6-MP), are widely used in the treatment of chronic inflammatory bowel diseases (IBD), but can cause myelotoxicity due to the accumulation of active metabolites. We report the case of a 48-year-old woman with ulcerative colitis who developed severe agranulocytosis following an accidental overdose of 6-MP. The patient presented with febrile pancytopenia with a neutrophil count of 0.04 G/L. Bone marrow examination revealed normal cellularity with an inversion of the maturation pyramid of the granulocyte lineage. A treatment combining growth factors (filgrastim) and antibiotics (tazobactam) was initiated, leading to progressive improvement over 5 weeks. The toxicity of 6-MP is mainly due to the accumulation of 6-thioguanine nucleotides (6-TGN). The polymorphism of the gene encoding the enzyme thiopurine S-methyltransferase (TPMT) can influence the risk of myelotoxicity. Two strategies are proposed to minimize this risk: evaluation of TPMT activity with dosage adjustment, or regular monitoring of blood counts with gradual dose increase. This case highlights the importance of rigorous biological monitoring when initiating 6-MP treatment, regardless of the TPMT test. Increased vigilance is necessary when using immunosuppressive drugs in the treatment of IBD to optimize efficacy and minimize toxicity.
| Published in | American Journal of Laboratory Medicine (Volume 9, Issue 3) |
| DOI | 10.11648/j.ajlm.20240903.11 |
| Page(s) | 23-28 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Iflammatory Bowel Disease, Myelotoxicity, Immunosuppressant, Mercaptopurine, Agranulocytosis
DRUG CLASSES | DRUGS |
|---|---|
ANTIBIOTIQUES | Cephalosporins, Chloramphenicol, Ciprofloxacin, Clindamycin, Cotrimoxazole, Tetracyclines, Ethambutol, Gentamicin, Isoniazid, Lincomycin, Metronidazole, Nitrofurantoin, Novobiocin, Penicillins, Rifampicin, Sulfamethoxazole, Sulfonamides, Streptomycin, Thiacetazone, Tinidazole, Vancomycin, Chloroquine, Flucytosine, Dapsone, Hydroxychloroquine, Levamisole, Mebendazole, Pyrimethamine, Quinine, Quinacrine, Acyclovir, Zidovudine, Terbinafine |
ANALGESICS AND NSAIDS | Acetylsalicylic acid, Diclofenac, Diflunisal, Tenoprofen, Flurbiprofen, Indomethacin, Ibuprofen, Noramidopyrine, Phenylbutazone, Piroxicam, Sulindac, Tenoxicam, Tolmetin |
ANTIPSYCHOTICS, SEDATIVES AND ANTIDEPRESSANTS | Amoxapine, Chlordiazepoxide, Clozapine, Diazepam, Haloperidol, Tricyclic antidepressants, Meprobamate, Mianserin, Phenothiazines, Risperidone, Tiapride |
ANTIEPILEPTIC | Carbamazepine, Ethosuximide, Phenytoins, Trimethadione, Valproic acid |
ANTITHYROID DRUGS | Carbimazole, Methimazole, Potassium perchlorate, Thiocyanate, Thiouracils |
CARDIAC MEDICATIONS | Acetylsalicylic acid, Aprindine, Captopril, Furosemide, Hydralazine, Lisinopril, Methyldopa, Nifedipine, Phenindione, Procainamide, Propafenone, Propranolol, Quinidine, Spironolactone, Thiazide Diuretics, Ticlopidine |
ANTIHISTAMINES | Brompheniramine, Chlorpheniramine, Cimetidine, Ranitidine, Tripelennamine |
HEAVY METALS | Arsenic derivatives, gold-containing compounds, and even mercury |
VARIOUS | Acetazolamide, Allopurinol, Aminoglutethimide, Bezafibrate, Colchicine, Dapsone, Deferiprone, Famotidine, Fluindione, Flutamide |
TOXIC | IMMUNO-ALLERGIC |
|---|---|
Direct cytotoxic effect of the drug on granulopoiesis | Indirect cytotoxicity through drug (antigen) binding to surface cell antibodies |
Dose-dependent effect No prior sensitization effcet | Non-dose dependent History of prior sensitization for more than 8 days |
Progressive agranulocytosis | Abrupt agranulocytosis |
Inhibition of granulopoiesis in vitro by the drug | Inhibition of granulopoiesis in vitro by the patient's serum |
Example: Cytotoxic chemotherapy, Carbamazepine, Quinine, Phenothiazines | Example: Synthetic antithyroid drugs, Antimalarials, Penicillins |
DIAG | Drug-Induced Agranulocytosis |
6-MP | Mercaptopurine |
IBD | Chronic Inflammatory Bowel Diseases |
6-TGN | 6-thioguanine Nucleotides |
TPMT | S-methyltransferase |
UC | Ulcerative Colitis |
ADCC | Antibody-dependent Cellular Cytotoxicity |
6-MMP | 6-Methylmercaptopurine |
CBC | Blood Cell Counts |
| [1] | E. Andrès a, F. Maloisel b, le groupe d’étude des agranulocytoses médicamenteuses des Hôpitaux universitaires de Strasbourg: Agranulocytoses médicamenteuses idiosyncrasiques [Idiosyncratic drug-induced agranulocytosis]. La Revue de Médecine Interne. 2006, 27(3): 209-214. |
| [2] | Andrès E, Kurtz JE, Maloisel F: Non-chemotherapy drug-induced agranulocytosis: experience of the Strasbourg teaching hospital (1985-2000) and review of the literature. Clin Lab Haematol. 2002, 24: 99-106. |
| [3] | Bénichou C, Solal-Celigny P: Standardization of definitions and criteria for causality assessment of adverse drug reactions. Drug-induced blood cytopenias: report of an international consensus meeting. Nouv Rev Fr Hematol. 1991, 33(3): 257-62. |
| [4] | David C. Pearson, Gary R. May, Gordon H. Fick, and Lloyd R. Sutherland: Azathioprine and 6- mercaptopurine in Crohn disease. A meta-analysis. Annals of Internal Medicine. 1995, 123(2): 132-142. |
| [5] | S Ardizzone, G Maconi, A Russo, V Imbesi, E Colombo, G Bianchi Porro: Randomised controlled trial of azathioprine and 5-aminosalicylic acid for treatment of steroid dependent ulcerative colitis. Gut. 2006, 55: 47-53. |
| [6] | Present DH, Meltzer SJ, Krumholz MP, et al.: 6-Mercaptopurine in the management of inflammatory bowel disease: short- and longterm toxicity. Ann Intern Med. 1989, 111: 641-649. |
| [7] | Gisbert JP, Gomollon F: Thiopurine-induced myelotoxicity in patients with inflammatory bowel disease: a review. American Journal of Gastroenterology. 2008, 103(7): 1783-1800. |
| [8] | Vovan AT, Ducroix JP, Barbuat C, Smail A, Terminassian L, Baillet J: Les agranulocytoses aiguës médicamenteuses immuno-allergiques [Acute Drug-Induced Immuno-Allergic Agranulocytosis]. La Revue de Médecine Interne. 1984, 5: 342-50. |
| [9] | Van der Klauw MM, Goudsmit R, Halie MR, et al.: A Population-Based Case-Cohort Study of Drug Associated Agranulocytosis. Archives of internal medicine. 1999, 159: 369-374. |
| [10] | Shapiro S, Issaragrisil S, Kaufman DW, Anderson T,: Agranulocytosis in Bangkok, Thailand: a predominantly drug-induced disease with an unusually low incidence. Aplastic Anemia Study Group.. American Journal of Tropical Medicine and Hygiene. 1999, 60(4): 573-577. |
| [11] | Mosyagin I, Dettling M, Roots I, Mueller Oerlinghausen B, Cascorbi I: Impact of Myeloperoxidase and NADPH-Oxidase Polymorphisms in Drug-Induced Agranulocytosis. Journal of Clinical Psychopharmacology. 2004, 24: 613-617. |
| [12] | W. Schultz: Über eigenartige Halserkrankungen [About peculiar throat diseases]. Dtsch Med Wochenschr. 1922, 48: 1495-6. |
| [13] | T Vial, C Pofilet, E Pham, C Payen, J C Evreux: Acute drug-induced agranulocytosis: experience of the Regional Center of Pharmacovigilance of Lyon over 7 years. Therapie. 1996, 51(5): 508-15. |
| [14] | Andrès E, Zimmer J, Affenberger S, Federici L, Alt M, Maloisel F: Idiosyncratic drug-induced agranulocytosis: Update of an old disorder. European Journal of Internal Medicine. 2006, 17: 529-535. |
| [15] | Gianluigi Zazaa, Meyling Cheokb, Natalia Krynetskaiae, et al.: Thiopurine pathway. Pharmacogenetics and Genomics. 2010, 20: 573-574. |
| [16] | Emmanuel Andre`s, Frederic Maloisel and Jacques Zimmer: The role of haematopoietic growth factors granulocyte colony-stimulating factor and granulocyte-macrophage colony-stimulating factor in the management of drug-induced agranulocytosis. British Journal of Haematology. 2010, 150: 3-8. |
| [17] | R van Egmond, P Chin, M Zhang, C W Sies, M L Barclay: High TPMT enzyme activity does not explain drug resistance due to preferential 6-methylmercaptopurine production in patients on thiopurine treatment. Alimentary Pharmacology and Therapeutics. 2012, 5(10): 1181-9. |
| [18] |
Monographie de produit, Comprimés de mercaptopurine. [Product Monograph, Mercaptopurine Tablets]. Sterimax Inc.2735 Matheson Boulevard East, Suite 1. (2024). Accessed: 06/05:
https://sterimaxinc.com/wp-cotent/uploads/2014/12/mercaptopurine.pdf |
| [19] |
Faustine Lhomme, Dr Marlène Ochmann, Pr Thierry Lamy: AGRANULOCYTOSE MÉDICAMENTEUSE: Conduite à tenir [DRUG-INDUCED AGRANULOCYTOSIS: Management Guidelines]. LA REVUE DU PRATICIEN. 2015, 65(5): 697-700.
https://www.chem-sante.fr/elearning/parcours_33/biblio_1/agranulocytose_medicamenteuse.pdf |
APA Style
Bardi, T. E., Ouarradi, A. E., Rouhi, S., Quiddi, W., Sayagh, S. (2024). Agranulocytosis Induced by Overdosage of Mercaptopurine: A Case Report. American Journal of Laboratory Medicine, 9(3), 23-28. https://doi.org/10.11648/j.ajlm.20240903.11
ACS Style
Bardi, T. E.; Ouarradi, A. E.; Rouhi, S.; Quiddi, W.; Sayagh, S. Agranulocytosis Induced by Overdosage of Mercaptopurine: A Case Report. Am. J. Lab. Med. 2024, 9(3), 23-28. doi: 10.11648/j.ajlm.20240903.11
@article{10.11648/j.ajlm.20240903.11,
author = {Touria El Bardi and Assia El Ouarradi and Salma Rouhi and Wafae Quiddi and Sanae Sayagh},
title = {Agranulocytosis Induced by Overdosage of Mercaptopurine: A Case Report
},
journal = {American Journal of Laboratory Medicine},
volume = {9},
number = {3},
pages = {23-28},
doi = {10.11648/j.ajlm.20240903.11},
url = {https://doi.org/10.11648/j.ajlm.20240903.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajlm.20240903.11},
abstract = {Drug-induced agranulocytosis (DIAG) is a rare but potentially fatal hematological complication. Thiopurines, such as mercaptopurine (6-MP), are widely used in the treatment of chronic inflammatory bowel diseases (IBD), but can cause myelotoxicity due to the accumulation of active metabolites. We report the case of a 48-year-old woman with ulcerative colitis who developed severe agranulocytosis following an accidental overdose of 6-MP. The patient presented with febrile pancytopenia with a neutrophil count of 0.04 G/L. Bone marrow examination revealed normal cellularity with an inversion of the maturation pyramid of the granulocyte lineage. A treatment combining growth factors (filgrastim) and antibiotics (tazobactam) was initiated, leading to progressive improvement over 5 weeks. The toxicity of 6-MP is mainly due to the accumulation of 6-thioguanine nucleotides (6-TGN). The polymorphism of the gene encoding the enzyme thiopurine S-methyltransferase (TPMT) can influence the risk of myelotoxicity. Two strategies are proposed to minimize this risk: evaluation of TPMT activity with dosage adjustment, or regular monitoring of blood counts with gradual dose increase. This case highlights the importance of rigorous biological monitoring when initiating 6-MP treatment, regardless of the TPMT test. Increased vigilance is necessary when using immunosuppressive drugs in the treatment of IBD to optimize efficacy and minimize toxicity.
},
year = {2024}
}
TY - JOUR T1 - Agranulocytosis Induced by Overdosage of Mercaptopurine: A Case Report AU - Touria El Bardi AU - Assia El Ouarradi AU - Salma Rouhi AU - Wafae Quiddi AU - Sanae Sayagh Y1 - 2024/08/30 PY - 2024 N1 - https://doi.org/10.11648/j.ajlm.20240903.11 DO - 10.11648/j.ajlm.20240903.11 T2 - American Journal of Laboratory Medicine JF - American Journal of Laboratory Medicine JO - American Journal of Laboratory Medicine SP - 23 EP - 28 PB - Science Publishing Group SN - 2575-386X UR - https://doi.org/10.11648/j.ajlm.20240903.11 AB - Drug-induced agranulocytosis (DIAG) is a rare but potentially fatal hematological complication. Thiopurines, such as mercaptopurine (6-MP), are widely used in the treatment of chronic inflammatory bowel diseases (IBD), but can cause myelotoxicity due to the accumulation of active metabolites. We report the case of a 48-year-old woman with ulcerative colitis who developed severe agranulocytosis following an accidental overdose of 6-MP. The patient presented with febrile pancytopenia with a neutrophil count of 0.04 G/L. Bone marrow examination revealed normal cellularity with an inversion of the maturation pyramid of the granulocyte lineage. A treatment combining growth factors (filgrastim) and antibiotics (tazobactam) was initiated, leading to progressive improvement over 5 weeks. The toxicity of 6-MP is mainly due to the accumulation of 6-thioguanine nucleotides (6-TGN). The polymorphism of the gene encoding the enzyme thiopurine S-methyltransferase (TPMT) can influence the risk of myelotoxicity. Two strategies are proposed to minimize this risk: evaluation of TPMT activity with dosage adjustment, or regular monitoring of blood counts with gradual dose increase. This case highlights the importance of rigorous biological monitoring when initiating 6-MP treatment, regardless of the TPMT test. Increased vigilance is necessary when using immunosuppressive drugs in the treatment of IBD to optimize efficacy and minimize toxicity. VL - 9 IS - 3 ER -
Hematology Laboratory, Mohammed VI University Hospital, Marrakech, Morocco; Faculty of Medicine and Pharmacy of Marrakech, Cadi Ayyad University, Marrakech, Morocco
Hematology Laboratory, Mohammed VI University Hospital, Marrakech, Morocco; Faculty of Medicine and Pharmacy of Marrakech, Cadi Ayyad University, Marrakech, Morocco
Hematology Laboratory, Mohammed VI University Hospital, Marrakech, Morocco; Faculty of Medicine and Pharmacy of Marrakech, Cadi Ayyad University, Marrakech, Morocco
Hematology Laboratory, Mohammed VI University Hospital, Marrakech, Morocco; Faculty of Medicine and Pharmacy of Marrakech, Cadi Ayyad University, Marrakech, Morocco
Hematology Laboratory, Mohammed VI University Hospital, Marrakech, Morocco; Faculty of Medicine and Pharmacy of Marrakech, Cadi Ayyad University, Marrakech, Morocco
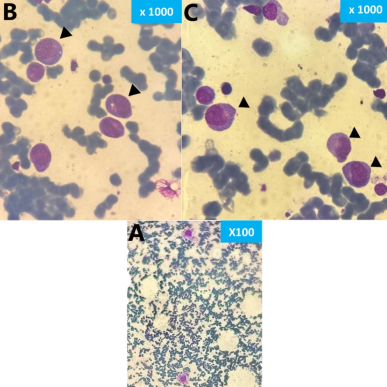
Figure 1. Appearance of promyelocytic blockage in the bone marrow (MGG stain): A: Low magnification, Bone marrow of normal cellularity, with megakaryocytes present. B and C: High magnifications, Blockage of granular differentiation with an excess of normal-appearing promyelocytes (black arrows): large cells, highly granular basophilic cytoplasm, and well-visible archoplasm.
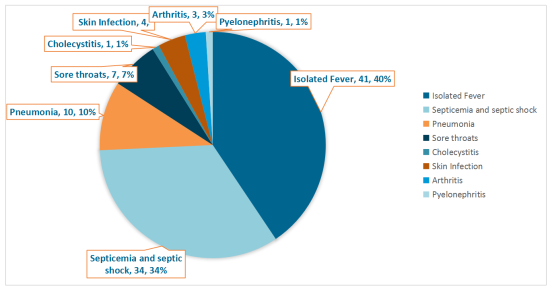
Figure 2. Main clinical manifestations reported in the series of drug-induced agranulocytosis at the University Hospitals of Strasbourg (n = 91) [1].
Information

