Secretary of the “Complementary Medicines and Integrated Therapies” Study Group of the Italian, Pediatric Society (SIP – Società Italiana di Pediatria), Parma, Italy
Contributor Roles: Sergio Bernasconi is the sole author. The author read and approved the final manuscript.
The introduction of the diagnostic-therapeutic approach based on Systems Medicine into the medical scenario has allowed us to deeper investigate into the concept of the human organism as a set of interconnected networks. This wide vision, in addition to shedding new light on the interpretation of pathological manifestations, allows us to set up new therapeutic strategies based on the management of alterations in the networks identified as involved in the onset and progression of the disease. The tool that, to date, can allow to set up network regulation treatments is Low Dose Medicine, a therapeutic approach based on low-dose pharmacology. The use of low doses signaling molecules is the physiologically most appropriate option for the management of network alterations. In the pediatric field, numerous experiences have confirmed the validity of this approach. A preclinical study and a Delphi Consensus have provided clear evidence on the action mechanism and clinical application of a low-dose medication (Citomix®) for the prevention and early treatment of Recurrent Respiratory Infections. The consensus was based on preclinical data and was aimed to collect clinical experiences with Citomix® about the biological capacity to modulate the immune response in the presence of infectious agents. The cornerstone of the consensus was the validation of the use of Citomix® as an option for the prevention and early add-on treatment of RRIs; the positive result which emerge from the vote of the statements constituting the consensus confirmed the validity of the investigated option.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
, such as genomics, metabolomics, transcriptomics, which allow for the acquisition of large amounts of information at the molecular level on the individual person and the individual pathology.
Given these premises, it is possible to define Systems Medicine as an interdisciplinary field of study in which human body systems (networks) are studied and considered as a part of an “integrated whole”, incorporating biochemical, physiological and environmental interactions
[3]
Conte F, Fiscon G, Licursi V. A paradigm shift in medicine: A comprehensive review of network-based approaches. Biochim Biophys Acta Gene Regul Mech. 2020; 1863(6): 194416.
In recent years, System Medicine has shown a notable development, both in terms of research and practical applications; among these, Low Dose Medicine (LDM) deserves particular attention.
LDM represent a successful example of integration between Molecular Biology and Psycho-Neuro-Endocrine- Immunology (PNEI)
[4]
Ader R, Cohen N, Felten DL. Brain, behavior, and immunity. Brain Behav Immun. 1987; 1(1): 1-6.
Haroon E, Raison CL, Miller AH. Psychoneuroimmunology meets neuropsychopharmacology: translational implications of the impact of inflammation on behavior. Neuropsychopharmacology. 2012; 37(1): 137-62.
, a key role is played by PNEI and its main unifying element: the crosstalk between the psycho-neuro-endocrine systems and the immune system, managed by signaling molecules such as neuropeptides, hormones, cytokines, growth factors that play a decisive role in determining the state of health or disease
Biancotto A, Wank A, Perl S. Baseline levels and temporal stability of 27 multiplexed serum cytokine concentrations in healthy subjects. PLoS One. 2013; 8(12): e76091.
Reeves R, Leonard WJ, Nissen MS. Binding of HMG-I(Y) imparts architectural specificity to a positioned nucleosome on the promoter of the human interleukin-2 receptor alpha gene. Mol Cell Biol. 2000; 20(13): 4666-79.
An altered crosstalk, caused by an imbalance in the concentration of specific signaling molecules, is crucial, for example, in the pathogenesis of inflammatory, allergic and autoimmune diseases.
Preserving or restoring the physiological concentration of messenger molecules is the key step for the maintenance or recovery of the physiological homeostatic balance which describes the healthy condition
[17]
Méndez-Samperio P, Badillo-Flores A, Nuñez-Vazquez A. Interleukin-4 inhibits secretion of interleukin-1beta in the response of human cells to mycobacterial heat shock proteins. Clin Diagn Lab Immunol. 1997; 4(6): 665-70.
In homeostatic conditions, the concentrations of signaling molecules are included in a specific physiological range (nanograms-picograms), above or below which a disease condition can occur. Given these theoretical premises, a substantial line of research has developed regarding the possibility of a therapeutic use of low doses biological molecules that, orally administered, can control and guide cellular functions to restore the original physiological conditions.
The mechanism of action of low dose signaling molecules consists in the modulation of the receptor’s response involved in the pathways that physiologically involve the signaling molecules themselves.
By virtue of their low concentration, the receptor activation which occurs in such a way does not trigger saturation mechanisms and consequent freezing of the receptor itself but, on the contrary, amplifies its physiological response. Furthermore, the use of physiological doses substantially reduces the risk of adverse events.
2. LDM and Scientific Research
Sixteen years of scientific research in the field of LDM
[20]
Gariboldi S, Palazzo M, Zanobbio L, Dusio GF, Mauro V, Solimene U, Cardani D, Mantovani M, Rumio C. Low dose oral administration of cytokines for treatment of allergic asthma. Pulm Pharmacol Ther. 2009; 22(6): 497-510.
D’Amico L, Ruffini E, Ferracini R. Low Dose of IL-12 stimulates T Cell response in cultures of PBMCs derived from Non Small Cell Lung Cancer Patients. Journal of Cancer Therapy 2012; 3: 337-342.
Radice E, Miranda V, Bellone G. Low-doses of sequential-kinetic-activated interferon-γ enhance the ex vivo cytotoxicity of peripheral blood natural killer cells from patients with early-stage colorectal cancer. A preliminary study. Int Immunopharmacol. 2014; 19(1): 66-73.
Roberti ML, Ricottini L, Capponi A. Immunomodulating treatment with low dose interleukin-4, interleukin-10 and interleukin-11 in psoriasis vulgaris. J Biol Regul Homeost Agents. 2014; 28(1): 133-9.
[25]
Luchetti P. Increasing of visual function in patients with retinal atrophy treated with drugs of Low Dose Medicine. Monocentric retrospective observational study. Minerva Oftalmologica 2014; 56(3-4): 53-61.
[26]
Barygina V, Becatti M, Lotti T. Treatment with low-dose cytokines reduces oxidative-mediated injury in perilesional keratinocytes from vitiligo skin. J Dermatol Sci. 2015; 79(2): 163-70.
Lotti T, Hercogova J, Wollina U. Vitiligo: successful combination treatment based on oral low dose cytokines and different topical treatments. J Biol Regul Homeost Agents. 2015; 29(1 Suppl): 53-8.
[28]
Radice E, Bellone G, Miranda V. Enhancement of the Immunostimulatory Functions of Ex Vivo-Generated Dendritic Cells from Early-Stage Colon Cancer Patients by Consecutive Exposure to Low Doses of Sequential-Kinetic-Activated IL-4 and IL-12. A Preliminary Study. Transl Oncol. 2015; 8(4): 327-38.
Lotti T. Successful combination treatment for psoriasis with phototherapy and low-dose cytokines: A spontaneous, retrospective observational clinical study. Hautarzt. 2015; 66(11): 849-54. German.
Tessaro I, Modina SC, Franciosi F. Effect of oral administration of low-dose follicle stimulating hormone on hyperandrogenized mice as a model of polycystic ovary syndrome. J Ovarian Res. 2015 Oct 6; 8: 64.
Genazzani AD, Despini G, Chierchia E, Benedetti C, Prati A. Pharmacological and Integrative Treatment of Stress-Induced Hypothalamic Amenorrhea. Chapter. Frontiers in Gynecological Endocrinology Part of the series ISGE Series pp 69-84.
[33]
Mancini F, Milardi D, Carfagna P. Low-dose SKA Progesterone and Interleukin-10 modulate the inflammatory pathway in endometriotic cell lines. Int Immunopharmacol. 2018; 55: 223-230.
Martin-Martin LS, Giovannangeli F, Bizzi E, An open randomized active-controlled clinical trial with low-dose SKA cytokines versus DMARDs evaluating low disease activity maintenance in patients with rheumatoid arthritis. Drug Des Devel Ther. 2017; 11: 985-994.
Carello R, Ricottini L, Miranda V. Long-term treatment with low-dose medicine in chronic childhood eczema: a double-blind two-stage randomized control trial. Ital J Pediatr. 2017; 43(1): 78.
Tagliacarne SC, Valsecchi C, Benazzo M. Low-dose multicomponent medication modulates humoral and cellular immune response in an ex-vivo study on children subjected to adenoid surgery. Immunol Lett. 2018; 203: 95-101.
have demonstrated the validity of the conceptual approach, and the efficacy and safety of pharmacological treatments based on the oral administration of low doses signaling molecules. Current scientific research highlights the high Immunostimulating and immunomodulating capacity of low-dose interleukins and interferons, hormones and neurotrophins. Evidence shows that orally (sublingually) administered signaling molecules can effectively modulate immune response. Due to its high accessibility, the oral mucosa is an elective gate for the administration of small active peptide molecules. The mechanism of action for orally administered peptides involves the uptake of the molecule by oral antigen-presenting cells (APCs) which present the signaling molecule itself to immunocompetent T cells within oropharyngeal lymph nodes, inducing a specific immune response.
Many experimental studies conducted so far have focused on pathologies characterized by an immune imbalance that is reflected mainly (although not exclusively) in an imbalance between the cytokines expressed by the two main lymphocyte subpopulations: Th1 and Th2. The LDM therapeutic rationale consists in the promotion of immune homeostasis by administering specific low dose cytokines.
For example, in a murine model of allergic asthma (20), the imbalance with increased production of IL-4 and IL-5 was found to be pivotal for the onset of the biological events that characterize the allergic pathology such as increased differentiation, maturation and migration of eosinophils at the medullary level.
The administration of IL-12 and IFN-gamma at low doses induces a significant reduction in the synthesis of IL-4 and IL-5 and a clear decrease in the number of eosinophils in the bronchoalveolar lavage fluid.
Some preclinical studies have shown that, using physiological sub-nanomolar doses of low dose hormones (FSH - follicle-stimulating hormone, Beta-estradiol, and Progesterone), it is possible to counteract certain imbalances of the PNEI axes involved in pathologies such as Polycystic Ovary Syndrome (PCOS)
[31]
Tessaro I, Modina SC, Franciosi F. Effect of oral administration of low-dose follicle stimulating hormone on hyperandrogenized mice as a model of polycystic ovary syndrome. J Ovarian Res. 2015 Oct 6; 8: 64.
Genazzani AD, Despini G, Chierchia E, Benedetti C, Prati A. Pharmacological and Integrative Treatment of Stress-Induced Hypothalamic Amenorrhea. Chapter. Frontiers in Gynecological Endocrinology Part of the series ISGE Series pp 69-84.
[32]
and Endometriosis
[33]
Mancini F, Milardi D, Carfagna P. Low-dose SKA Progesterone and Interleukin-10 modulate the inflammatory pathway in endometriotic cell lines. Int Immunopharmacol. 2018; 55: 223-230.
The use of pharmacological aids such as low-dose hormones with bioregulatory capacity appear to be therapeutic tools of great interest alone (in conditions of preserved capacity for self-regulation) or in overlapping with hormone replacement therapy (in conditions of advanced state of endocrine dysregulation) to reduce – if possible – the dosage of the replacement hormone and, consequently, the possible onset of dose-related side effects.
Biological activity is also described for low dose neurotrophins: in vitro and in vivo studies
[36]
Tagliacarne SC, Valsecchi C, Benazzo M. Low-dose multicomponent medication modulates humoral and cellular immune response in an ex-vivo study on children subjected to adenoid surgery. Immunol Lett. 2018; 203: 95-101.
demonstrated the efficacy of low dose BDNF (Brain-Derived Neurotrophic Factor) in supporting neuroprotection mechanisms and in particular a positive effect has been highlighted control of ROS expression, vitality of cortical neurons and astrocytes, and proliferation of astrocytes.
3. LDM Clinical Applications in the Pediatric Field
All the studies conducted so far show the ability of signaling molecules to modulate the cellular response in a highly selective way.
Basic and clinical research conducted to date in the field of LDM shows encouraging signs in terms of efficacy, compliance and safety which are of particular interest in the pediatric field.
An example of pediatric clinical application of LDM is in Atopic Dermatitis management
[35]
Carello R, Ricottini L, Miranda V. Long-term treatment with low-dose medicine in chronic childhood eczema: a double-blind two-stage randomized control trial. Ital J Pediatr. 2017; 43(1): 78.
. Treatment with low dose cytokines (IL-12 and IFN-γ) was evaluated in a pediatric population affected by chronic atopic dermatitis. The results show that low dose cytokines treatment reduced the severity of the disease and contributed to maintaining a Low Disease Activity (LDA) in the treatment-free at the follow-up period. These results were transduced in a progressive improvement in the quality of life of subjects treated with low dose throughout the investigation period.
The LDM approach has also proven effective in the management of stress-induced hypothalamic amenorrhea
[32]
Genazzani AD, Despini G, Chierchia E, Benedetti C, Prati A. Pharmacological and Integrative Treatment of Stress-Induced Hypothalamic Amenorrhea. Chapter. Frontiers in Gynecological Endocrinology Part of the series ISGE Series pp 69-84.
[32]
, a condition in which the absence of the menstrual cycle is determined by an imbalance in the neuroendocrine response to stress with overexpression of opioid peptides and blockade of the pulsatility of hypothalamic GnRH (Gonadotropin Releasing Hormone) and pituitary LH (Luteinizing Hormone) hormones release. The use of weak estrogens in low doses such as epimestrol and estriol has proven capable of rebalancing the GnRH-LH axis by increasing the release of the latter. The use of low-dose estradiol has proven equally effective by increasing the sensitivity of the GnRH receptors at the hypothalamic and pituitary levels, supporting the synthesis of LH and FSH. Clinical data demonstrate that low-dose estradiol can restore the normal connectivity of the HPG axis compromised by stress and, because of that, responsible for the onset of stress-induced hypothalamic amenorrhea.
4. Highlight: LDM for Recurring Respiratory Infections (RRIs) Management
Respiratory infections are a demanding challenge for physicians. Commonly, a relative immune defect sustains their recurrence. At present, there is no standardized treatment for their prevention acting on the immune system
[36]
Tagliacarne SC, Valsecchi C, Benazzo M. Low-dose multicomponent medication modulates humoral and cellular immune response in an ex-vivo study on children subjected to adenoid surgery. Immunol Lett. 2018; 203: 95-101.
Recurrent Respiratory infections (RRIs) are a very common clinical condition in childhood, with an important social and economic impact. It is estimated that about 25% of children under 1 year old and 6% of children during the first 6 years of life have RRIs, making them one of the most common reasons for pediatric medical visits in the early years of life
[38]
Chiappini E, Santamaria F, Marseglia GL. Prevention of recurrent respiratory infections: Inter-society Consensus. Ital J Pediatr. 2021; 47(1): 211.
RI treatment is generally based on symptomatic drugs (e.g. acetaminophen) and antibiotics administration, but frequently without precise indication. Therefore, prevention of RRI is at present a goal in clinical practice. Bacterial lysates are also used with mild results in reducing respiratory morbidity in clinical practice. Thus, there is a high interest in preventive and alternative treatment by doctors. In this regard, immunomodulants are widely used in common practice
[36]
Tagliacarne SC, Valsecchi C, Benazzo M. Low-dose multicomponent medication modulates humoral and cellular immune response in an ex-vivo study on children subjected to adenoid surgery. Immunol Lett. 2018; 203: 95-101.
The administration of cytokines modulates the immune response in a complex manner, as demonstrated in a study by Tagliacarne et al
[36]
Tagliacarne SC, Valsecchi C, Benazzo M. Low-dose multicomponent medication modulates humoral and cellular immune response in an ex-vivo study on children subjected to adenoid surgery. Immunol Lett. 2018; 203: 95-101.
conducted at the Laboratory of Clinical Immunology of the Pediatric Clinic of the University of Pavia on adenoid tissue taken from children with recurrent inflammation of the airways in whom adenoidectomy had been indicated. Adding known concentrations of LDM multicomponent drug Citomix® (Guna S.p.a. Milan, Italy) to the cell culture of the adenoid tissue demonstrated an immune modulatory action characterized by:
a) increase in Interleukin 6 and Interferon-gamma with a reduction in the initial phases of Interleukin 10 useful for enhancing the anti-viral response.
b) increased production of IgA and IgM;
c) proliferation of B lymphocyte subpopulations.
These results are in line with the data of the first clinical experiences on children with recurrent upper respiratory tract infections who, following cycles of therapy and prophylaxis according to the following protocol, significantly decreased the days of fever and absence from school and were treated much less frequently with antibiotics, therefore in line with the most current recommendations for less use of these drugs, especially in the early ages of life, motivated above all by the increase in bacterial resistance phenomena worldwide.
Based on this background and on the real-life experience with Citomix® in the management of RRI
[39]
Arrighi A. CITOMIX vs IMMUCYTAL® nella prevenzione e terapia delle Infezioni Respiratorie Acute in età pediatrica – Studio prospettico controllato. La Med Biol 2009; 3: 3-11.
[40]
Lombardi Mistura E. – Lymphomyosot ®, Citomix e Omeogriphi ® nella prevenzione delle Infezioni Respiratorie Ricorrenti in Pediatria. La Med. Biol 2015; 1: 15-24.
[39, 40]
, a Delphi Consensus on the management of RRIs using Citomix® was designed involving a large group of Italian primary care, private practice, and hospital/university pediatricians
[41]
Agosti M, Arrighi A, Bernasconi S. A low-dose multicomponent medication as a new approach in prevention and early add-on treatment of recurrent respiratory infections in children: a Delphi Consensus. Eur Rev Med Pharmacol Sci. 2024; 28(16): 4156-4169.
A modified Delphi process was used to reach consensus within a panel of Italian specialists (112 Pediatricians) on the preventive and overlapping approach with Citomix® as a new intervention model for the management of IRRs. The voting panel was composed of general practitioners (64%), free choice (27%) and hospital/university pediatricians (9%).
A scientific committee analyzed the literature, determined the areas requiring investigation (in accordance with the results of the multiple-choice questionnaire) and identified two macro-topics of interest:
a) IRRs as disease (definition and diagnosis)
b) treatment and prophylaxis of IRRs.
Statements for each of these topics were then formulated and validated. The Delphi method involves rounds of questions submitted to the panel experts using an online platform. In the first round of voting, consensus was reached for all the statements.
In accordance with their usual methods of managing IRRs and with current clinical evidence, the panel members provided their feedback on their agreement with each statement of the questionnaire.
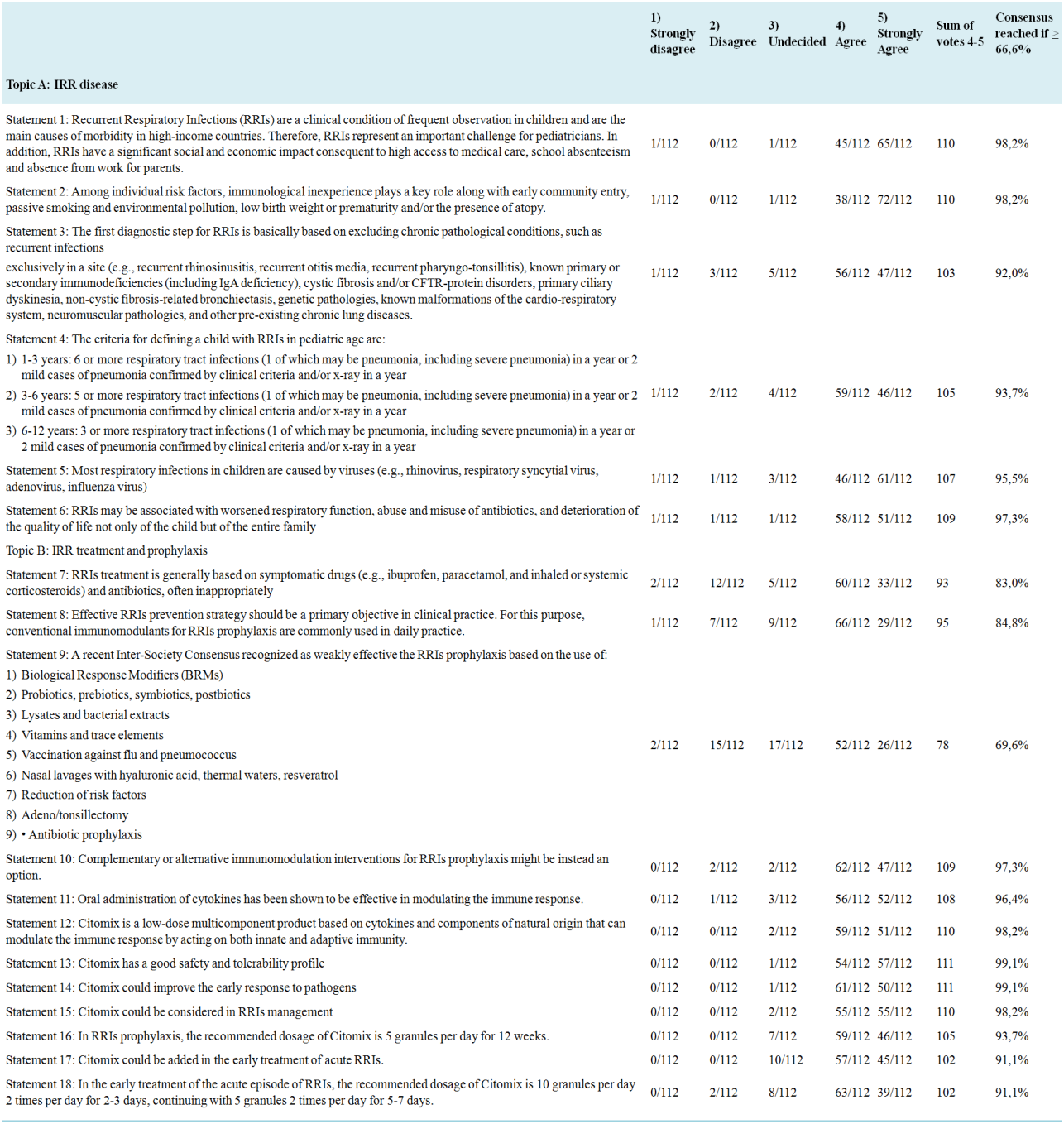
The experts evaluated and voted on 18 statements and reached a consensus on all 18; the first 6 statements were related to the pathology itself (Topic A) and the following 12 (Topic B) related to the current methods of treating IRRs and the options offered by Citomix®. For each statement, consensus was considered to have been reached with the achievement of agreement by at least 66.6% of the expert group and the acceptance of the scientific committee.
To calculate the consensus, the sum of the votes expressed with the values of 4 and 5 on the Likert scale corresponding to: “in agreement” and “in strong agreement” was considered (Table 1).
Table 1. Statements summary and voting results for each statement
[41]
Agosti M, Arrighi A, Bernasconi S. A low-dose multicomponent medication as a new approach in prevention and early add-on treatment of recurrent respiratory infections in children: a Delphi Consensus. Eur Rev Med Pharmacol Sci. 2024; 28(16): 4156-4169.
a) The statements relating to the IRR pathology showed high levels of agreement, with a consensus ranging from 92% to 98.2%.
b) The statements regarding the treatment and prophylaxis of IRR also showed very high levels of agreement, with a consensus ranging from 69.6% to 99.1%.
Through the Delphi Method it was possible to reach consensus among doctors on the most significant aspects of the current management of IRR management and the possibility of a new approach towards pediatric patients subject to IRR both in terms of prevention and overlapping with current therapies based on the use of Citomix®.
The consensus was unanimous, among Pediatricians, in identifying the prevention and overlapping approach based on Citomix® for the management of RRIs. This Consensus collected the level of agreement expressed by a large panel of pediatricians who have developed a solid experience in the use of Citomix® to manage children with RRIs. The high level of agreement reached in a single voting round allows to endorse the use of Citomix® in clinical practice for the prevention and early treatment in overlapping of RRIs. It is important to underline that the opinions of the panel members, expressed in the form of voting, derive both from their experience, acquired from daily practice, and from the evidence derived from preclinical and clinical studies. In conclusion, Citomix® represents, for a significant sample of pediatricians, a valid tool for both prevention and overlapping treatment of RRIs.
5. Conclusions
Starting from a series of basic evidence proven with scientifically correct methodologies, LDM has increasingly carved out a specific role in the field of clinical medicine. Its applications and boundaries are still largely to be studied and controlled but current evidence already allows us to consider it, in some specific pathologies, as an important complementary therapy that, in connection with the "classic" one, can be useful to improve the quality of life of patients, reduce the risk of unwanted side events and adverse reactions, reduce the use of drugs that are certainly useful but potentially harmful, maintain the patient in LDA (Low Disease Activity) after reaching the remission of symptomatology (such as, for instance in Rheumatoid Arthritis patients who had undergone remission after biological drugs or conventional therapy)
[34]
Martin-Martin LS, Giovannangeli F, Bizzi E, An open randomized active-controlled clinical trial with low-dose SKA cytokines versus DMARDs evaluating low disease activity maintenance in patients with rheumatoid arthritis. Drug Des Devel Ther. 2017; 11: 985-994.
, and contribute to reduce the costs of therapies, especially chronic ones. Regarding the specific topic of RRIs, the Delphi consensus results have verified the initial hypothesis: it is therefore possible to include Citomix® among the drugs that can be used for prevention or combined with other interventions (overlapping) to enhance their efficacy (add-on treatment) in the early treatment of RRIs.
Abbreviations
APCs
Antigen-Presenting Cells
BDNF
Brain-Derived Neurotrophic Factor
FSH
Follicle-Stimulating Hormone
GnRH
Gonadotropin Releasing Hormone
LDA
Low Disease Activity
LDM
Low Dose Medicine
LH
Luteinizing Hormone
PCOS
Polycystic Ovary Syndrome
RRIs
Recurrent Respiratory Infections
Author Contributions
Sergio Bernasconi is the sole author. The author read and approved the final manuscript.
Funding
This work is not supported by any external funding.
Conflicts of Interest
Prof. Sergio Bernasconi carries out consultancy activities for Guna S.p.a.
References
[1]
Barabási AL, Gulbahce N, Loscalzo J. Network medicine: a network-based approach to human disease. Nat Rev Genet. 2011; 12(1): 56-68.
Haroon E, Raison CL, Miller AH. Psychoneuroimmunology meets neuropsychopharmacology: translational implications of the impact of inflammation on behavior. Neuropsychopharmacology. 2012; 37(1): 137-62.
Biancotto A, Wank A, Perl S. Baseline levels and temporal stability of 27 multiplexed serum cytokine concentrations in healthy subjects. PLoS One. 2013; 8(12): e76091.
Reeves R, Leonard WJ, Nissen MS. Binding of HMG-I(Y) imparts architectural specificity to a positioned nucleosome on the promoter of the human interleukin-2 receptor alpha gene. Mol Cell Biol. 2000; 20(13): 4666-79.
Méndez-Samperio P, Badillo-Flores A, Nuñez-Vazquez A. Interleukin-4 inhibits secretion of interleukin-1beta in the response of human cells to mycobacterial heat shock proteins. Clin Diagn Lab Immunol. 1997; 4(6): 665-70.
Gariboldi S, Palazzo M, Zanobbio L, Dusio GF, Mauro V, Solimene U, Cardani D, Mantovani M, Rumio C. Low dose oral administration of cytokines for treatment of allergic asthma. Pulm Pharmacol Ther. 2009; 22(6): 497-510.
D’Amico L, Ruffini E, Ferracini R. Low Dose of IL-12 stimulates T Cell response in cultures of PBMCs derived from Non Small Cell Lung Cancer Patients. Journal of Cancer Therapy 2012; 3: 337-342.
Radice E, Miranda V, Bellone G. Low-doses of sequential-kinetic-activated interferon-γ enhance the ex vivo cytotoxicity of peripheral blood natural killer cells from patients with early-stage colorectal cancer. A preliminary study. Int Immunopharmacol. 2014; 19(1): 66-73.
Roberti ML, Ricottini L, Capponi A. Immunomodulating treatment with low dose interleukin-4, interleukin-10 and interleukin-11 in psoriasis vulgaris. J Biol Regul Homeost Agents. 2014; 28(1): 133-9.
[25]
Luchetti P. Increasing of visual function in patients with retinal atrophy treated with drugs of Low Dose Medicine. Monocentric retrospective observational study. Minerva Oftalmologica 2014; 56(3-4): 53-61.
[26]
Barygina V, Becatti M, Lotti T. Treatment with low-dose cytokines reduces oxidative-mediated injury in perilesional keratinocytes from vitiligo skin. J Dermatol Sci. 2015; 79(2): 163-70.
Lotti T, Hercogova J, Wollina U. Vitiligo: successful combination treatment based on oral low dose cytokines and different topical treatments. J Biol Regul Homeost Agents. 2015; 29(1 Suppl): 53-8.
[28]
Radice E, Bellone G, Miranda V. Enhancement of the Immunostimulatory Functions of Ex Vivo-Generated Dendritic Cells from Early-Stage Colon Cancer Patients by Consecutive Exposure to Low Doses of Sequential-Kinetic-Activated IL-4 and IL-12. A Preliminary Study. Transl Oncol. 2015; 8(4): 327-38.
Lotti T. Successful combination treatment for psoriasis with phototherapy and low-dose cytokines: A spontaneous, retrospective observational clinical study. Hautarzt. 2015; 66(11): 849-54. German.
Tessaro I, Modina SC, Franciosi F. Effect of oral administration of low-dose follicle stimulating hormone on hyperandrogenized mice as a model of polycystic ovary syndrome. J Ovarian Res. 2015 Oct 6; 8: 64.
Genazzani AD, Despini G, Chierchia E, Benedetti C, Prati A. Pharmacological and Integrative Treatment of Stress-Induced Hypothalamic Amenorrhea. Chapter. Frontiers in Gynecological Endocrinology Part of the series ISGE Series pp 69-84.
[33]
Mancini F, Milardi D, Carfagna P. Low-dose SKA Progesterone and Interleukin-10 modulate the inflammatory pathway in endometriotic cell lines. Int Immunopharmacol. 2018; 55: 223-230.
Martin-Martin LS, Giovannangeli F, Bizzi E, An open randomized active-controlled clinical trial with low-dose SKA cytokines versus DMARDs evaluating low disease activity maintenance in patients with rheumatoid arthritis. Drug Des Devel Ther. 2017; 11: 985-994.
Carello R, Ricottini L, Miranda V. Long-term treatment with low-dose medicine in chronic childhood eczema: a double-blind two-stage randomized control trial. Ital J Pediatr. 2017; 43(1): 78.
Tagliacarne SC, Valsecchi C, Benazzo M. Low-dose multicomponent medication modulates humoral and cellular immune response in an ex-vivo study on children subjected to adenoid surgery. Immunol Lett. 2018; 203: 95-101.
Arrighi A. CITOMIX vs IMMUCYTAL® nella prevenzione e terapia delle Infezioni Respiratorie Acute in età pediatrica – Studio prospettico controllato. La Med Biol 2009; 3: 3-11.
[40]
Lombardi Mistura E. – Lymphomyosot ®, Citomix e Omeogriphi ® nella prevenzione delle Infezioni Respiratorie Ricorrenti in Pediatria. La Med. Biol 2015; 1: 15-24.
[41]
Agosti M, Arrighi A, Bernasconi S. A low-dose multicomponent medication as a new approach in prevention and early add-on treatment of recurrent respiratory infections in children: a Delphi Consensus. Eur Rev Med Pharmacol Sci. 2024; 28(16): 4156-4169.
Bernasconi, S. (2024). Systems Medicine and the Contribution of Low Dose Pharmacology in Paediatrics. American Journal of Pediatrics, 10(4), 244-251. https://doi.org/10.11648/j.ajp.20241004.24
Bernasconi, S. Systems Medicine and the Contribution of Low Dose Pharmacology in Paediatrics. Am. J. Pediatr.2024, 10(4), 244-251. doi: 10.11648/j.ajp.20241004.24
Bernasconi S. Systems Medicine and the Contribution of Low Dose Pharmacology in Paediatrics. Am J Pediatr. 2024;10(4):244-251. doi: 10.11648/j.ajp.20241004.24
@article{10.11648/j.ajp.20241004.24,
author = {Sergio Bernasconi},
title = {Systems Medicine and the Contribution of Low Dose Pharmacology in Paediatrics
},
journal = {American Journal of Pediatrics},
volume = {10},
number = {4},
pages = {244-251},
doi = {10.11648/j.ajp.20241004.24},
url = {https://doi.org/10.11648/j.ajp.20241004.24},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20241004.24},
abstract = {The introduction of the diagnostic-therapeutic approach based on Systems Medicine into the medical scenario has allowed us to deeper investigate into the concept of the human organism as a set of interconnected networks. This wide vision, in addition to shedding new light on the interpretation of pathological manifestations, allows us to set up new therapeutic strategies based on the management of alterations in the networks identified as involved in the onset and progression of the disease. The tool that, to date, can allow to set up network regulation treatments is Low Dose Medicine, a therapeutic approach based on low-dose pharmacology. The use of low doses signaling molecules is the physiologically most appropriate option for the management of network alterations. In the pediatric field, numerous experiences have confirmed the validity of this approach. A preclinical study and a Delphi Consensus have provided clear evidence on the action mechanism and clinical application of a low-dose medication (Citomix®) for the prevention and early treatment of Recurrent Respiratory Infections. The consensus was based on preclinical data and was aimed to collect clinical experiences with Citomix® about the biological capacity to modulate the immune response in the presence of infectious agents. The cornerstone of the consensus was the validation of the use of Citomix® as an option for the prevention and early add-on treatment of RRIs; the positive result which emerge from the vote of the statements constituting the consensus confirmed the validity of the investigated option.
},
year = {2024}
}
TY - JOUR
T1 - Systems Medicine and the Contribution of Low Dose Pharmacology in Paediatrics
AU - Sergio Bernasconi
Y1 - 2024/12/31
PY - 2024
N1 - https://doi.org/10.11648/j.ajp.20241004.24
DO - 10.11648/j.ajp.20241004.24
T2 - American Journal of Pediatrics
JF - American Journal of Pediatrics
JO - American Journal of Pediatrics
SP - 244
EP - 251
PB - Science Publishing Group
SN - 2472-0909
UR - https://doi.org/10.11648/j.ajp.20241004.24
AB - The introduction of the diagnostic-therapeutic approach based on Systems Medicine into the medical scenario has allowed us to deeper investigate into the concept of the human organism as a set of interconnected networks. This wide vision, in addition to shedding new light on the interpretation of pathological manifestations, allows us to set up new therapeutic strategies based on the management of alterations in the networks identified as involved in the onset and progression of the disease. The tool that, to date, can allow to set up network regulation treatments is Low Dose Medicine, a therapeutic approach based on low-dose pharmacology. The use of low doses signaling molecules is the physiologically most appropriate option for the management of network alterations. In the pediatric field, numerous experiences have confirmed the validity of this approach. A preclinical study and a Delphi Consensus have provided clear evidence on the action mechanism and clinical application of a low-dose medication (Citomix®) for the prevention and early treatment of Recurrent Respiratory Infections. The consensus was based on preclinical data and was aimed to collect clinical experiences with Citomix® about the biological capacity to modulate the immune response in the presence of infectious agents. The cornerstone of the consensus was the validation of the use of Citomix® as an option for the prevention and early add-on treatment of RRIs; the positive result which emerge from the vote of the statements constituting the consensus confirmed the validity of the investigated option.
VL - 10
IS - 4
ER -
Secretary of the “Complementary Medicines and Integrated Therapies” Study Group of the Italian, Pediatric Society (SIP – Società Italiana di Pediatria), Parma, Italy
Biography:
Sergio Bernasconi is retired full Professor of Pediatrics He has been President of the Italian Society for Pediatric Endocrinology and Diabetology (ISPED), Member of the Council and of the DTC Committee of the European Society for Pediatric Endocrinology (ESPE), Editor in chief of the Italian Journal of Pediatrics (currently Editor Emeritus), Chairman of The Department of Pediatrics of the Universities of Modena and Parma (Italy). He is honorary member of the University of Chieti (Italy) and he received the “Outstanding Clinician Award” from ESPE. He is author and/or co-author of about 500 scientific papers published on international journals and he is member of Editorial Boards of national and international journals. He has been Chair and Invited Speaker in national and international Conferences and Congresses.
Research Fields:
Pediatric Endocrinology, Auxology, Clinical Genetics, Complementary Medicine
Bernasconi, S. (2024). Systems Medicine and the Contribution of Low Dose Pharmacology in Paediatrics. American Journal of Pediatrics, 10(4), 244-251. https://doi.org/10.11648/j.ajp.20241004.24
Bernasconi, S. Systems Medicine and the Contribution of Low Dose Pharmacology in Paediatrics. Am. J. Pediatr.2024, 10(4), 244-251. doi: 10.11648/j.ajp.20241004.24
Bernasconi S. Systems Medicine and the Contribution of Low Dose Pharmacology in Paediatrics. Am J Pediatr. 2024;10(4):244-251. doi: 10.11648/j.ajp.20241004.24
@article{10.11648/j.ajp.20241004.24,
author = {Sergio Bernasconi},
title = {Systems Medicine and the Contribution of Low Dose Pharmacology in Paediatrics
},
journal = {American Journal of Pediatrics},
volume = {10},
number = {4},
pages = {244-251},
doi = {10.11648/j.ajp.20241004.24},
url = {https://doi.org/10.11648/j.ajp.20241004.24},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20241004.24},
abstract = {The introduction of the diagnostic-therapeutic approach based on Systems Medicine into the medical scenario has allowed us to deeper investigate into the concept of the human organism as a set of interconnected networks. This wide vision, in addition to shedding new light on the interpretation of pathological manifestations, allows us to set up new therapeutic strategies based on the management of alterations in the networks identified as involved in the onset and progression of the disease. The tool that, to date, can allow to set up network regulation treatments is Low Dose Medicine, a therapeutic approach based on low-dose pharmacology. The use of low doses signaling molecules is the physiologically most appropriate option for the management of network alterations. In the pediatric field, numerous experiences have confirmed the validity of this approach. A preclinical study and a Delphi Consensus have provided clear evidence on the action mechanism and clinical application of a low-dose medication (Citomix®) for the prevention and early treatment of Recurrent Respiratory Infections. The consensus was based on preclinical data and was aimed to collect clinical experiences with Citomix® about the biological capacity to modulate the immune response in the presence of infectious agents. The cornerstone of the consensus was the validation of the use of Citomix® as an option for the prevention and early add-on treatment of RRIs; the positive result which emerge from the vote of the statements constituting the consensus confirmed the validity of the investigated option.
},
year = {2024}
}
TY - JOUR
T1 - Systems Medicine and the Contribution of Low Dose Pharmacology in Paediatrics
AU - Sergio Bernasconi
Y1 - 2024/12/31
PY - 2024
N1 - https://doi.org/10.11648/j.ajp.20241004.24
DO - 10.11648/j.ajp.20241004.24
T2 - American Journal of Pediatrics
JF - American Journal of Pediatrics
JO - American Journal of Pediatrics
SP - 244
EP - 251
PB - Science Publishing Group
SN - 2472-0909
UR - https://doi.org/10.11648/j.ajp.20241004.24
AB - The introduction of the diagnostic-therapeutic approach based on Systems Medicine into the medical scenario has allowed us to deeper investigate into the concept of the human organism as a set of interconnected networks. This wide vision, in addition to shedding new light on the interpretation of pathological manifestations, allows us to set up new therapeutic strategies based on the management of alterations in the networks identified as involved in the onset and progression of the disease. The tool that, to date, can allow to set up network regulation treatments is Low Dose Medicine, a therapeutic approach based on low-dose pharmacology. The use of low doses signaling molecules is the physiologically most appropriate option for the management of network alterations. In the pediatric field, numerous experiences have confirmed the validity of this approach. A preclinical study and a Delphi Consensus have provided clear evidence on the action mechanism and clinical application of a low-dose medication (Citomix®) for the prevention and early treatment of Recurrent Respiratory Infections. The consensus was based on preclinical data and was aimed to collect clinical experiences with Citomix® about the biological capacity to modulate the immune response in the presence of infectious agents. The cornerstone of the consensus was the validation of the use of Citomix® as an option for the prevention and early add-on treatment of RRIs; the positive result which emerge from the vote of the statements constituting the consensus confirmed the validity of the investigated option.
VL - 10
IS - 4
ER -