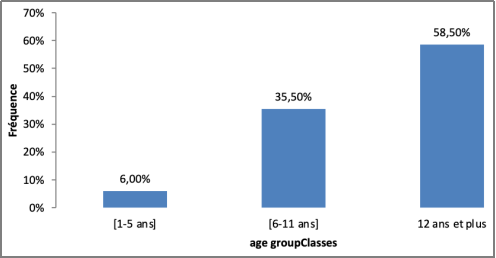
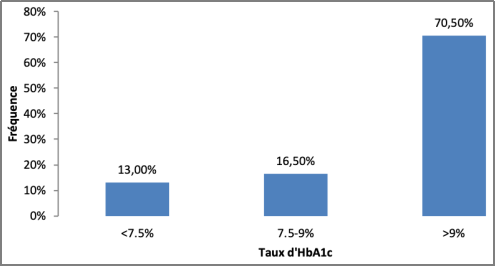
Introduction: Type 1 diabetes (T1D) accounts for more than 90% of all cases of diabetes in children and adolescents. The aim of this study is to determine the level of glycemic control and to analyze the factors of poor control. Methodology: This is a prospective study conducted in five (5) pediatric departments in Dakar over a period of 6 months and including all children aged 0 to 18 years with type 1 diabetes. Glycemic balance was assessed with glycated hemoglobin (HbA1c). Results: During the study, two hundred (200) patients were included. The mean age at diagnosis was 12.15 years ± 3.98 years [range 1.00 to 18.00 years]. Ketoacidosis was the main circumstance of discovery in 67.00% (134 individuals). The types of insulin used were human in 64% of cases. Among the patients who received therapeutic education (22), 39.33% were not educated by a qualified provider. There was a glycemic imbalance in 70.5% of patients. After an analytical study, there was no statistically significant difference between HbA1c and gender, geographical origin, socioeconomic and educational level of parents, duration of diabetes progression, physical activity and the therapeutic protocol used. However, therapeutic education had a positive influence on HbA1c. Conclusion: The glycemic control of diabetic patients in the Dakar region is very insufficient. This would be due to several factors including the insufficiency of therapeutic education. It is important to train providers in this fundamental aspect of diabetes management.
| Published in | American Journal of Pediatrics (Volume 10, Issue 4) |
| DOI | 10.11648/j.ajp.20251101.11 |
| Page(s) | 1-6 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Type 1 Diabetes, Glycemic Control, Therapeutic Education
Settings | HbA1c rate | Total | p-value | Odds [95% CI] | |||
|---|---|---|---|---|---|---|---|
< 9% | ≥ 9% | ||||||
N | % | N | % | ||||
Sex | |||||||
Female | 33 | 27.73 | 86 | 72.27 | 119 | 0.5 | |
Male | 14 | 73.7 | 5 | 26.3 | 19 | ||
Support Sites | 0.71 | ||||||
CHAN | 31 | 29.52 | 74 | 70.48 | 105 | ||
CHNEAR | 23 | 28.4 | 58 | 71.6 | 81 | ||
Diamniadio | 2 | 33.33 | 4 | 66.67 | 6 | ||
Philippe Senghor | 0 | 0 | 2 | 100 | 2 | ||
Pikine | 3 | 50 | 3 | 50 | 6 | ||
Socio-economic level | 0.06 | ||||||
Low | 26 | 33.33 | 52 | 66.67 | 78 | ||
Moderate | 15 | 18.29 | 67 | 81.71 | 82 | ||
High | 18 | 45 | 22 | 55 | 40 | ||
Parents' education level | 0.69 | ||||||
No educated | 21 | 33.33 | 42 | 66.67 | 63 | ||
Primary level | 11 | 23.4 | 36 | 76.6 | 47 | ||
High school | 13 | 28.26 | 33 | 71.74 | 46 | ||
University | 14 | 31.82 | 30 | 68.18 | 44 | ||
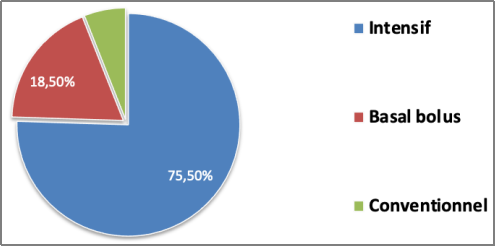
Insulin protocol | 0.22 | ||||||
Basal bolus | 12 | 32.43 | 25 | 67.57 | 37 | ||
Conventional | 6 | 50 | 6 | 50 | 12 | ||
Intensive | 41 | 27.15 | 110 | 72.85 | 151 | ||
Therapeutic Education | 0.02 | 4.7 [1.06-20.84] | |||||
Yes | 57 | 32.02 | 121 | 67.98 | 178 | ||
No | 2 | 9.09 | 22 | 90.91 | 24 | ||
Trained Educator | <0.001 | 35 [8, 22-151, 3] | |||||
Yes | 55 | 50.93 | 53 | 49.07 | 108 | ||
No | 2 | 2.86 | 68 | 97.14 | 70 | ||
Duration of diabetes development | 0.63 | ||||||
≥ 5 years | 8 | 24.24 | 25 | 75.76 | 33 | ||
< 5 years | 51 | 30.54 | 116 | 69.46 | 167 | ||
T1D | Type 1 Diabetes |
DCCT | The Diabetes Control and Complications Trial |
SD | Standard Deviation |
CDIC | Changing Diabetes in Children |
HBA1C | Glycated Hemoglobin |
ARHC | Albert Royer Hospital Center |
ANHC | Abass Ndao Hospital Center |
PHC | Pikine Hospital Center |
DCH | Diamniadio Children's Hospital DCH |
PMS | Philippe Maguillène Senghor Health Center |
BMI | Body Mass Index |
| [1] | Boiro D. Diabetic ketoacidosis in children: Epidemiological, diagnostic and evolutionary aspects: About 74 cases in the pediatric department of the hospital center, Medical thesis, Dakar, 2013, No. 101. |
| [2] | Hanaire H. Lessons from DCCT and EDIC: Glycemic control and insulin protocols, Research Group; 2015: 3-6. |
| [3] | Wine cellar ITS, Irwin ML, Editor NS, Gray Metal. Correlates of overweight and obesity in 5529 adolescents with type 1 diabetes: The T1D Exchange Clinic Registry; 2017; 126, 68-78 |
| [4] | Niang B, Faye PM, Dème/Ly I, Ba A, Thiam L, Thiongane A et al. Epidemiological and clinical profile in type 1 diabetic children in a Dakar hospital setting. Reverend CAMES. 2015; 3(2): 89-92 |
| [5] | Ngwiri T, Were F, Predieri B, Ngugi P, and Lughetti L. Glycemic control in Kenyan children and adolescents with type 1 diabetes mellitus; IJOE; 2015 |
| [6] | Ghannem H, Harrabi I, Gaha R, Trabelsi L, Chouchen I, Essoussi AS et al. Epidemiology of diabetes in children in schools in Sousse, Tunisia. Methab for Diabetes. 2001; 27(5): 613-617. |
| [7] | Yatsuya H, Kwaguchi L, Hatego E, Aoyama A. Sex differences in diabetes mellitus, WHO Bulletin, 2013; 91(9): 621-715. |
| [8] | Togo AD Epidemiological, clinical and therapeutic aspects Medical thesis Bamako, University of Bamako 2010. |
| [9] | Wildi S, Geiser C, Perrenoud L, Perolini M, Lazarevic C et al. Welcoming young diabetics at school, Continuing education: Pediatric endocrinology 2016; 27 (1). |
| [10] | Rosenbloom AL, Silverstein JH, Amemiya S, ZeitlerP, Klingensmith G. Type 2 diabetes in children and adolescents. Pediatric Diabetes 2009: 10 (Suppl. 12): 17–32. |
| [11] | Philips JC. Type 1 diabetes: from genetic predisposition to a hypothetical environmental context, Rev Med Liège 2012; 67: 5-6: 319-325. |
| [12] | West NA, Lawrence J M., Maahs DM and Mayer-Davis E. Epidemiology of type 1 diabetes, Endocrinol Metab Clin North Am. 2010; 39(3): 481–497. |
| [13] | Messaaoui A, Dorchy H. Growth of diabetic children. Rev Med Brux 2010; 31 (Supplement): S 77-80. |
| [14] | Jaffiol C. Diabetes mellitus in Africa. Taurus. Acad. Natl Med. 2011, 195(6), 1239-1250. |
| [15] | MN Elbagir, MA Eltom, EO Mahadi and C. Berne. “Pattern of long-term complications in Sudanese diabetics treated with insulin patients”, Diabetes Research and Clinical Practice, vol. 30, no. 1, pp. 59–67, 1995. |
| [16] | MN Elbagir, MA Eltom, H. Rosling, and C. Berne. “Glycemic control of insulin-dependent diabetes mellitus in Sudan: influence of insulin shortage,” Diabetes Research and Clinical Practice, vol. 30, no. 1, pp. 43–52, 1995. |
| [17] | GC Onyemelukwe, HS Isah and EC Mba. “Glycosylated haemoglobin (HbA1) for the control of diabetes in Africans; preliminary results of the microcolumn technique,” Tropical and Geographical Medicine, vol. 35, no. 4, pp. 347–351, 1983. |
| [18] | A. Gebre-Yohannes and SI Rahlenbeck, “Glycemic control and its determinants in diabetic patients in Ethiopia,” Diabetes Research and Clinical Practice, vol. 35, no. 2-3, pp. 129-134, 1997. |
| [19] | ES Majaliwa, E. Munubhi, K. Ramaiya et al. “A survey of acute and chronic complications in children and adolescents with type 1 diabetes at Muhimbili National Hospital, Dar es Salaam, Tanzania,” Diabetes Care, vol. 30, no. 9, pp. 2187–2192, 2007. |
| [20] |
HB Mortensen, KJ Robertson, HJ. Aanstoot et al. “Insulin management and metabolic control of type 1 diabetes mellitus in children and adolescents in 18 countries,” Diabetic Medicine, vol. 15, no. 9, pp. 752–759, 1998.
https://doi.org/10.1002/(sici)1096-9136(199809)15:9%3C752::aid-dia678%3E3.0.co;2-w |
APA Style
Babacar, N., Aminata, M., Djibril, B., Amadou, S., Oulimata, N., et al. (2025). Glycemic Assessment of Type I Diabetic Children in the Dakar Region, Senegal. American Journal of Pediatrics, 10(4), 1-6. https://doi.org/10.11648/j.ajp.20251101.11
ACS Style
Babacar, N.; Aminata, M.; Djibril, B.; Amadou, S.; Oulimata, N., et al. Glycemic Assessment of Type I Diabetic Children in the Dakar Region, Senegal. Am. J. Pediatr. 2025, 10(4), 1-6. doi: 10.11648/j.ajp.20251101.11
@article{10.11648/j.ajp.20251101.11,
author = {Niang Babacar and Mbaye Aminata and Boiro Djibril and Sow Amadou and Ndiaye Oulimata and Dina Obambi and Ly Fatou and Sy Khady and Mbaye Maimouna Ndour and Ndiaye Ousmane},
title = {Glycemic Assessment of Type I Diabetic Children in the Dakar Region, Senegal
},
journal = {American Journal of Pediatrics},
volume = {10},
number = {4},
pages = {1-6},
doi = {10.11648/j.ajp.20251101.11},
url = {https://doi.org/10.11648/j.ajp.20251101.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20251101.11},
abstract = {Introduction: Type 1 diabetes (T1D) accounts for more than 90% of all cases of diabetes in children and adolescents. The aim of this study is to determine the level of glycemic control and to analyze the factors of poor control. Methodology: This is a prospective study conducted in five (5) pediatric departments in Dakar over a period of 6 months and including all children aged 0 to 18 years with type 1 diabetes. Glycemic balance was assessed with glycated hemoglobin (HbA1c). Results: During the study, two hundred (200) patients were included. The mean age at diagnosis was 12.15 years ± 3.98 years [range 1.00 to 18.00 years]. Ketoacidosis was the main circumstance of discovery in 67.00% (134 individuals). The types of insulin used were human in 64% of cases. Among the patients who received therapeutic education (22), 39.33% were not educated by a qualified provider. There was a glycemic imbalance in 70.5% of patients. After an analytical study, there was no statistically significant difference between HbA1c and gender, geographical origin, socioeconomic and educational level of parents, duration of diabetes progression, physical activity and the therapeutic protocol used. However, therapeutic education had a positive influence on HbA1c. Conclusion: The glycemic control of diabetic patients in the Dakar region is very insufficient. This would be due to several factors including the insufficiency of therapeutic education. It is important to train providers in this fundamental aspect of diabetes management.
},
year = {2025}
}
TY - JOUR T1 - Glycemic Assessment of Type I Diabetic Children in the Dakar Region, Senegal AU - Niang Babacar AU - Mbaye Aminata AU - Boiro Djibril AU - Sow Amadou AU - Ndiaye Oulimata AU - Dina Obambi AU - Ly Fatou AU - Sy Khady AU - Mbaye Maimouna Ndour AU - Ndiaye Ousmane Y1 - 2025/01/16 PY - 2025 N1 - https://doi.org/10.11648/j.ajp.20251101.11 DO - 10.11648/j.ajp.20251101.11 T2 - American Journal of Pediatrics JF - American Journal of Pediatrics JO - American Journal of Pediatrics SP - 1 EP - 6 PB - Science Publishing Group SN - 2472-0909 UR - https://doi.org/10.11648/j.ajp.20251101.11 AB - Introduction: Type 1 diabetes (T1D) accounts for more than 90% of all cases of diabetes in children and adolescents. The aim of this study is to determine the level of glycemic control and to analyze the factors of poor control. Methodology: This is a prospective study conducted in five (5) pediatric departments in Dakar over a period of 6 months and including all children aged 0 to 18 years with type 1 diabetes. Glycemic balance was assessed with glycated hemoglobin (HbA1c). Results: During the study, two hundred (200) patients were included. The mean age at diagnosis was 12.15 years ± 3.98 years [range 1.00 to 18.00 years]. Ketoacidosis was the main circumstance of discovery in 67.00% (134 individuals). The types of insulin used were human in 64% of cases. Among the patients who received therapeutic education (22), 39.33% were not educated by a qualified provider. There was a glycemic imbalance in 70.5% of patients. After an analytical study, there was no statistically significant difference between HbA1c and gender, geographical origin, socioeconomic and educational level of parents, duration of diabetes progression, physical activity and the therapeutic protocol used. However, therapeutic education had a positive influence on HbA1c. Conclusion: The glycemic control of diabetic patients in the Dakar region is very insufficient. This would be due to several factors including the insufficiency of therapeutic education. It is important to train providers in this fundamental aspect of diabetes management. VL - 10 IS - 4 ER -
Centre Hospitalier National d’Enfants Albert Royer, Dakar, Senegal
Centre Hospitalier National d’Enfants Albert Royer, Dakar, Senegal
Information