Background: Systemic lupus erythematosus (SLE) is a chronic idiopathic autoimmune disease. Guillain-Barré syndrome (GBS) is an acute monophasic immune-mediated polyradiculoneuropathy. Case presentation: We report the case of a 16-year-old patient, who presented in November 2023 a flu-like syndrome with diarrhea and abdominal pain. Then he had visual hallucinations and psychosis, followed by generalized tonic-clonic seizures. Urine toxicology assay was positive, a syndrome of hepatic cytolysis and cholestasis were noted. Toxic encephalopathy and hepatopathy were mentioned and he was transferred to a psychiatric ward where he persisted with an infectious syndrome, hallucinations, delirium and then flaccid tetraplegia of ascending evolution with dyspnea and respiratory distress. In January 2024, there was tetraplegia, abolished deep tendon reflexes (DTR) in all 4 limbs, hypoesthesia in all 4 limbs. Cerebrospinal fluid examination found albumin -cytological dissociation. Magnetic resonance imaging of the spinal cord was normal. He received 500 mg of intravenous methylprednisolone for 3 days then a per os relay with prednisolone 50 mg in addition to azathioprine (Aza) 50 mg x2/day and functional rehabilitation. The electroencephalogram revealed signs of non-structural generalised epilepsy in March 2024. The electroneuromyogram found a neurophysiological pattern of acute polyradiculoneuropathy in the recovery phase. In the evolution, an antinuclear antibody assay (indirect immunofluorescence) came back positive at a titer of 1/160, with a speckled appearance. On the basis of the American College of Rhumatology (ACR) with a score of 19, the diagnosis of SLE was retained and background treatment with Aza 50 mg/day continued. At the end of May 2025, there persisted a predominantly distal tetraparesis, an abolition of DTR. Conclusion: Although rare, GBS can be the mode of revelation of SLE. This SLE-GBS association is often serious and can be life-threatening.
| Published in | American Journal of Psychiatry and Neuroscience (Volume 14, Issue 3) |
| DOI | 10.11648/j.ajpn.20261403.11 |
| Page(s) | 47-56 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Guillain-Barré Syndrome, Epilepsy, Systemic Lupus, Togo
07-Dec | December 16 | 26-Dec | 05-Jan | January 10 | January 18 | January 29 | 19- Feb | March 31 | 02 Sept | STANDARDS | |
|---|---|---|---|---|---|---|---|---|---|---|---|
AST | 2.3 N | 2.9 N | 4.1 N | 5.5 N | 4.1 N | 4 N | 2.4 N | 4 N | Less than 26, 38 or 37 IU/l | ||
ALT | 2.9 N | 1.6 N | 7.6 N | 7.7 N | 7.6 N | 8.8 N | 3.9 N | 4.6 N | Below 29, 40 or 41 | ||
GGT | 1.6 N | 3.5 N | 2.5 N | 3.5 N | 4 N | Normal | [10-50] | ||||
PAL | 1.4 N | 2.9 N | 1.0 N | 2.9 N | 1.7 N | Less than 280 | |||||
Urea | 0.28 | 0.40 | 0.3 | 0.22 | 0.36 | 0.28 | [0.15-0.45g/l] | ||||
Creatinine | 8.65 | 8 | 10 | 9 | 9 | 8 | 7 | [07-14mg/ml] | |||
D-dimers | 953.55 | N < 500 mg/ml | |||||||||
PBS | Negative | Negative | Negative | Negative | |||||||
CRP | 96 | < 5 | < 5 | < 5 | N < 5 mg/l | ||||||
ESR | 40 | 50 | 65 | 85 | 32 | 50 | < 20 mm | ||||
Blood sugar | 1.08 | 0.7-1.10g/l | |||||||||
CPK | 109 | [24-190] | |||||||||
ASLO | <200 | ||||||||||
CBC | |||||||||||
Hb | 15.0 | 14 | 10.2 | 10.2 | 11.3 | 14.4 | 12-16g/dl | ||||
MCV | 89.80 | 97.3 | 96 | 93 | 92.1 | 97.3 | 90-100 fl | ||||
MCHC | 31.70 | 33.2 | 33.1 | 32 | 31.6 | 31.2 | 27-32 pg | ||||
Platelets | 275000 | 264000 | 23100 | 98000 | 318000 | 264000 | [150-400,000/mm3] | ||||
Leukocytes | 5400 | 3700 | 7656 | 5500 | 7300 | 3700 | 4000-10000/mm 3 | ||||
Lymphocytes | 1697 | 1034 | 696 | 1870 | 949 | 1147 | 1500-4000/mm 3 | ||||
PNN | 1955 | 2445 | 2500 | 3410 | 4820 | 1700-7000/mm 3 | |||||
HIV serology, Hepatitis B, C | Negatives | Negatives | Negatives | ||||||||
Ionogram | Normal | ||||||||||
Blood cultures | Negatives | ||||||||||
Multi-drug test | Positives | ||||||||||
CSF: Proteins | 1.0 g/l | <0.5 g/l | |||||||||
Glucose | 0.45g/l | 0.50-0.70 g/l | |||||||||
Cytology | 0 cells | 0-5 cells | |||||||||
ANA (IFI) | 1/160 | < 1/160 |
Citation (Actor/Year) | Age/Sex | Demonstration of the LES | Antibody | Kind of SGB | Treatment | Evolution | Background treatment |
|---|---|---|---|---|---|---|---|
Uhunmwangho (2015) | 26/F | Polyarthralgia; high blood pressure, proteinuria, lupus nephritis, generalized myxedema | ANA, dsDNA | Not realized | Cs per os, IV | Complete (Time not defined) | AZA, HQC |
Boudanga (2023) | 41/F | Generalized Alopecia Myxedema | ANA 1/1280 dsANA 300 IU/ml | AMAN | IVIg, CP (IV) | Complete | CS, HQC |
Beshir (2021) | 14/F | No symptoms before GBS | ANA 1/1280 in ANA 12 UI | AMAN | EP, (8), IG, IV, CS, IV, Rituximab | Complete | CS Oral |
Yildiz (2015) | 47/F | Alopecia, oral ulcer, anemia, leukopenia, thrombocytopenia, | ANA | AMAN | Ig IV, CS | Complete (14 months) | RTX, HQC |
Wang (2024) | 62/M | Malar rash, protein | ANA 1/160 | MTX + intrathecal DXM | Not reported | Not reported | |
Fawzy (2022) | 39/M | Arthralgia Epilepsy PRES syndrome | ANA, dsDNA ANA, Smith, antiSSa, Low complements | IV Ig, EP | Death | ||
Chaudhuri (1989) | 40/M | Epilepsy, Leukopenia, Lupus nephritis | ANA in ANA | AIDP | EP, CS, CP | Partial (8 weeks) | |
He (2025) | 38/M | Malar rash, leukopenia, lupus pleurisy | ANA 1/1000 Rnp, Sm, Ro52, SSA, U1RNP, C3 low | AIDP | IVIg CS HCQ, MMF | Complete (18 months) | CS, HCQ, MMF |
Present case | 16/M | Psychosis, delirium, epilepsy, leukopenia psychosis | ANA | AIDP | CS, AZA | Partial (18 months) | AZA |
SLE | Systemic Lupus Erythematosus |
GBS | Guillain-Barré Syndrome |
CNS | Central Nervous System |
PNS | Peripheral Nervous System |
IV Ig | Intravenous Immunoglobulin |
PBS | Peripheral Blood Smear |
CT | Computed Tomography |
DTR | Deep Tendon Reflexes |
CRP | C reactive Protein |
HIV | Human Immunodeficiency Virus |
ENMG | Electroneuromyogram |
EEG | Electroencephalogram |
ESR | Erythrocyte Sedimentation Rate |
ANA | Antinuclear Antibodies |
DNA | Deoxyribonucleic Acid |
NPLSE | Neuropsychological Manifestations of Systemic Lupus Erythematosus |
Aza | Azathioprine |
CSF | Cerebrospinal Fluid |
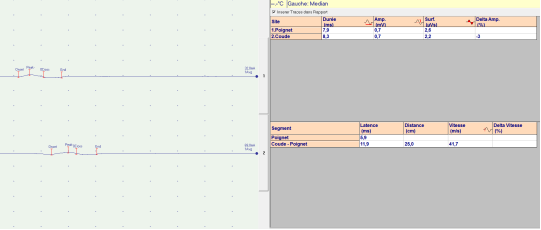
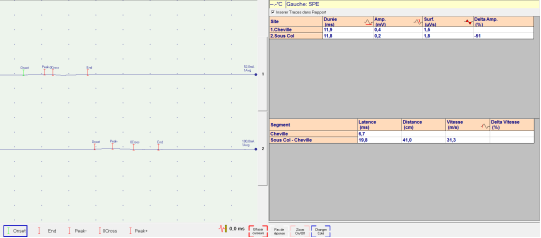
Motor nerve conduction | |||
|---|---|---|---|
Nerves | Distal latency (ms) | Amplitude (mV) | Speed (ms) |
Right median | 4.0 | 1.7 | 42.6 |
Left median | 5.9 | 0.7 | 41.7 |
Right ulnar | 3.3 | 1.2 | 43.8 |
Left ulnar | 3.9 | 2.8 | 46.0 |
Right common peroneal | 6.7 | 0.4 | 31.3 |
Left common peroneal | 8.8 | No potential | 28.6 |
Right tibial | 8.7 | 3.1 | 31.3 |
Left tibial | 3.8 | ||
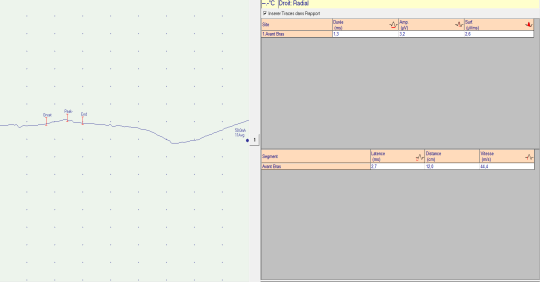
Sensory nerve conduction (orthodromic pathway) | |||
|---|---|---|---|
Nerves | Distal latency (ms) | Amplitude (mV) | Speed |
Right radial | 2.7 | 3.2 | 44.4 |
Left radial | 2.2 | 6.3 | 54.5 |
Right median | 24 | 16.2 | 50.0 |
Left median | 21 | 18.6 | 57.1 |
Right ulnar | 24 | 8.2 | 37.5 |
Left ulnar | 21 | 18.4 | 57.1 |
Right sural | 40 | 3.5 | 30.0 |
Left sural | No potential | ||
| [1] | Schwartz N., Stock AD, and C. Putterman. Neuropsychiatric lupus: new mechanistic insights and future treatment directions. Nat. Rev. Rheumatol. 2019; 15(3): 137‑152. |
| [2] | Bellanti R, Rinaldi S. Guillain-barre syndrome: A comprehensive review. Eur J Neurol. 2024; 31: e16365. |
| [3] | He L, Zhang Z, and Tan Y. Systemic lupus erythematosus complicated by severe Guillain-Barre syndrome: case report and literature review. Front. Immunol. 2025; 16: 1551448. |
| [4] | Bediri K, El Ouni A, Toujani S et al. Polyradiculonévrite aiguë avec atteinte diaphragmatique au cours d’un Lupus érythémateux systémique: à propos d’une revenante [Acute polyneuropathy with diaphragmatic involvement in systemic lupus erythematosus: a case report]. La Revue de medecine interne. 2021; 42: A103-A104. |
| [5] | Boudanga A, Chraa M, Rhazouani OC et al. Severe acute polyradiculoneuritis revealing systemic lupus erythematosus: a case report. Pan Afr Med J. 2023: 45(8). |
| [6] | Uhunmwangho CU, Abene EA, Gimba ZM, et al. Guillain barre syndrome as initial presentation of systemic lupus erythematosus. Highland Med Res J. 2015; 15(2): 96-98. |
| [7] | Apetse K, Dongmo Tajeuna JJ, Kumako VK et al. Guillain-Barre syndrome in hospitals in Togo. Médecine Tropicale Et Santé Internationale 2021. |
| [8] | Kumako VK, Apetse K, Dongmo Tajeuna JJ et al. Profils épidémiologiques, cliniques et évolutifs des syndromes de Guillain Barre selon le type électroneuromyographique au Togo [Epidemiological, clinical and clinical course profiles of Guillain-Barré syndrome according to electroneuromyographic type in Togo]. Revue neurologique 176(2020) S44–S86. |
| [9] | Sarwar S, Mohamed AS, Rogers S, et al. Neuropsychiatric Systemic Lupus Erythematosus: A 2021 Update on Diagnosis, Management, and Current Challenges. 2021; Cureus 13(9): e17969. |
| [10] |
ACR ad hoc committee on neuropsychiatric lupus nomenclature. The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes. Arthritis & Rheumatism. 1999; 42(4): 599-608.
https://doi.org/10.1002/1529-0131(199904)42:4<599::AID-ANR2>3.0.CO;2-F |
| [11] | Yacouba MN et al. Mapoure Njankouo Yacouba et al. Manifestations neuropsychiatriques au cours du lupus érythémateux systémique: à propos de 108 cas au Cameroun [Neuropsychiatric manifestations in patients with systemic lupus erythematosus: about 108 cases in Cameroon]. Pan African Medical Journal. 2022: 42(241). |
| [12] | Martin-Blondel G, Alric L. Atteinte hépatique dans les maladies de système [Liver damage in systemic diseases. EMC – Hepatology]. 2009; 4(4): 1-9. |
| [13] | Algren DA, Christian MR. Buyer Beware: Pitfalls in Toxicology Laboratory Testing. Emergency Medicine 2015. |
| [14] | Melanson SEF, Lee-Lewandrowski E, Griggs DA et al. Reduced Interference by Phenothiazines in Amphetamine Drug of Abuse Immunoassays. Archives of Pathology & Laboratory Medicine. 2006; 130(12): 1834‑1838. |
| [15] | Fokke C, van den Berg B, Drenthen J, Walgaard C, van Doorn PA, Jacobs BC. Diagnosis of Guillain-Barré syndrome and validation of Brighton criteria. Brain. 2014; 137: 33–43. |
| [16] | Coomes EA, Haghbayan H, Spring J, and al. Fulminant Guillain-Barré syndrome in a patient with systemic lupus erythematosus. BMJ Case Rep. 2019; 12(1) 2018-226634. |
| [17] | Chaudhuri KR, Taylor IK, Niven RM. A case of systemic lupus erythematosus presenting as Guillain-Barre syndrome. British Journal of Rheumatology. 1989; 28: 440-442. |
| [18] | Uluta ÅŸ F. Systemic Lupus Erythematosus Presenting With Two Different Neurologic Entities, Guillain Barre Syndrome And Posterior Reversible Encephalopathy Syndrome: Case Report. Int. J. Clin. Rheumatol. (2022) 17(3), 058-061. |
| [19] | Wang J, Zhe Z, Junyan Q et al. Clinical features of Guillain-Barré Syndrome and chronic inflammatory demyelinating polyradiculoneuritis associated with SLE. Lupus Sci Med. (2024) 11(20). |
| [20] | Yıldız ÖK, Balaban H, Senel S, et al. Acute lumbosacral polyradiculoneuropathy heralding transformation to systemic lupus erythematosus in a patient with discoid lupus. Lupus (2011) 20, 972–974. |
| [21] | Bertsias GK, Ioannidis JPA, Aringer M, et al. EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs. Annals of the Rheumatic Diseases 2010; 69(12): 2074‑2082. |
| [22] | Beshir E, Belt E, Chencheri Net al. Case Report: Guillain-Barré Syndrome as Primary Presentation of Systemic Lupus Erythematosus (SLE-GBS) in a Teenage Girl. Front. Pediatr. 2022; 10: 838927. |
APA Style
Ephoevi-ga, A. M., Guinhouya, K. M., Agba, L., Anayo, K. N., Kabassem, B., et al. (2026). Seizures and Guillain-Barré Syndrome Leading to the Discovery of Systemic Lupus: Case of an Adolescent in Lomé and Review of the Literature. American Journal of Psychiatry and Neuroscience, 14(3), 47-56. https://doi.org/10.11648/j.ajpn.20261403.11
ACS Style
Ephoevi-ga, A. M.; Guinhouya, K. M.; Agba, L.; Anayo, K. N.; Kabassem, B., et al. Seizures and Guillain-Barré Syndrome Leading to the Discovery of Systemic Lupus: Case of an Adolescent in Lomé and Review of the Literature. Am. J. Psychiatry Neurosci. 2026, 14(3), 47-56. doi: 10.11648/j.ajpn.20261403.11
AMA Style
Ephoevi-ga AM, Guinhouya KM, Agba L, Anayo KN, Kabassem B, et al. Seizures and Guillain-Barré Syndrome Leading to the Discovery of Systemic Lupus: Case of an Adolescent in Lomé and Review of the Literature. Am J Psychiatry Neurosci. 2026;14(3):47-56. doi: 10.11648/j.ajpn.20261403.11
@article{10.11648/j.ajpn.20261403.11,
author = {Adama Mawulikplimi Ephoevi-ga and Kokou Mensah Guinhouya and Lehleng Agba and Komla Nyinevi Anayo and Bitankade Kabassem and Kossivi Apetse and Komi Assogba and Vinyo Kumako and Mofou Belo and Agnon Koffi Balogou},
title = {Seizures and Guillain-Barré Syndrome Leading to the Discovery of Systemic Lupus: Case of an Adolescent in Lomé and Review of the Literature},
journal = {American Journal of Psychiatry and Neuroscience},
volume = {14},
number = {3},
pages = {47-56},
doi = {10.11648/j.ajpn.20261403.11},
url = {https://doi.org/10.11648/j.ajpn.20261403.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajpn.20261403.11},
abstract = {Background: Systemic lupus erythematosus (SLE) is a chronic idiopathic autoimmune disease. Guillain-Barré syndrome (GBS) is an acute monophasic immune-mediated polyradiculoneuropathy. Case presentation: We report the case of a 16-year-old patient, who presented in November 2023 a flu-like syndrome with diarrhea and abdominal pain. Then he had visual hallucinations and psychosis, followed by generalized tonic-clonic seizures. Urine toxicology assay was positive, a syndrome of hepatic cytolysis and cholestasis were noted. Toxic encephalopathy and hepatopathy were mentioned and he was transferred to a psychiatric ward where he persisted with an infectious syndrome, hallucinations, delirium and then flaccid tetraplegia of ascending evolution with dyspnea and respiratory distress. In January 2024, there was tetraplegia, abolished deep tendon reflexes (DTR) in all 4 limbs, hypoesthesia in all 4 limbs. Cerebrospinal fluid examination found albumin -cytological dissociation. Magnetic resonance imaging of the spinal cord was normal. He received 500 mg of intravenous methylprednisolone for 3 days then a per os relay with prednisolone 50 mg in addition to azathioprine (Aza) 50 mg x2/day and functional rehabilitation. The electroencephalogram revealed signs of non-structural generalised epilepsy in March 2024. The electroneuromyogram found a neurophysiological pattern of acute polyradiculoneuropathy in the recovery phase. In the evolution, an antinuclear antibody assay (indirect immunofluorescence) came back positive at a titer of 1/160, with a speckled appearance. On the basis of the American College of Rhumatology (ACR) with a score of 19, the diagnosis of SLE was retained and background treatment with Aza 50 mg/day continued. At the end of May 2025, there persisted a predominantly distal tetraparesis, an abolition of DTR. Conclusion: Although rare, GBS can be the mode of revelation of SLE. This SLE-GBS association is often serious and can be life-threatening.},
year = {2026}
}
TY - JOUR T1 - Seizures and Guillain-Barré Syndrome Leading to the Discovery of Systemic Lupus: Case of an Adolescent in Lomé and Review of the Literature AU - Adama Mawulikplimi Ephoevi-ga AU - Kokou Mensah Guinhouya AU - Lehleng Agba AU - Komla Nyinevi Anayo AU - Bitankade Kabassem AU - Kossivi Apetse AU - Komi Assogba AU - Vinyo Kumako AU - Mofou Belo AU - Agnon Koffi Balogou Y1 - 2026/07/17 PY - 2026 N1 - https://doi.org/10.11648/j.ajpn.20261403.11 DO - 10.11648/j.ajpn.20261403.11 T2 - American Journal of Psychiatry and Neuroscience JF - American Journal of Psychiatry and Neuroscience JO - American Journal of Psychiatry and Neuroscience SP - 47 EP - 56 PB - Science Publishing Group SN - 2330-426X UR - https://doi.org/10.11648/j.ajpn.20261403.11 AB - Background: Systemic lupus erythematosus (SLE) is a chronic idiopathic autoimmune disease. Guillain-Barré syndrome (GBS) is an acute monophasic immune-mediated polyradiculoneuropathy. Case presentation: We report the case of a 16-year-old patient, who presented in November 2023 a flu-like syndrome with diarrhea and abdominal pain. Then he had visual hallucinations and psychosis, followed by generalized tonic-clonic seizures. Urine toxicology assay was positive, a syndrome of hepatic cytolysis and cholestasis were noted. Toxic encephalopathy and hepatopathy were mentioned and he was transferred to a psychiatric ward where he persisted with an infectious syndrome, hallucinations, delirium and then flaccid tetraplegia of ascending evolution with dyspnea and respiratory distress. In January 2024, there was tetraplegia, abolished deep tendon reflexes (DTR) in all 4 limbs, hypoesthesia in all 4 limbs. Cerebrospinal fluid examination found albumin -cytological dissociation. Magnetic resonance imaging of the spinal cord was normal. He received 500 mg of intravenous methylprednisolone for 3 days then a per os relay with prednisolone 50 mg in addition to azathioprine (Aza) 50 mg x2/day and functional rehabilitation. The electroencephalogram revealed signs of non-structural generalised epilepsy in March 2024. The electroneuromyogram found a neurophysiological pattern of acute polyradiculoneuropathy in the recovery phase. In the evolution, an antinuclear antibody assay (indirect immunofluorescence) came back positive at a titer of 1/160, with a speckled appearance. On the basis of the American College of Rhumatology (ACR) with a score of 19, the diagnosis of SLE was retained and background treatment with Aza 50 mg/day continued. At the end of May 2025, there persisted a predominantly distal tetraparesis, an abolition of DTR. Conclusion: Although rare, GBS can be the mode of revelation of SLE. This SLE-GBS association is often serious and can be life-threatening. VL - 14 IS - 3 ER -
Neurology Department, Campus Teaching Hospital, Lome, Togo
Research Fields: General Neurology, Cerebrovascular diseases, neuroinflammatory diseases, Peripheral neurological disorders and muscle pathologies
Neurology Department, Sylvanus Olympio Teaching Hospital, Lome, Togo
Research Fields: General Neurology, Epileptology, Peripheral neurological disorders and muscle pathologies, Neurodegenerative diseases
Neurology Department, Kara Teaching Hospital, Kara, Togo
Research Fields: General Neurology, Epileptology, Peripheral neurological disorders and muscle pathologies, Neurodegenerative diseases
Neurology Department, Campus Teaching Hospital, Lome, Togo
Research Fields: General Neurology, Epileptology, Peripheral neurological disorders and muscle pathologies, Neurodegenerative diseases
Neurology Department, Campus Teaching Hospital, Lome, Togo
Research Fields: General Neurology, Epileptology, Peripheral neurological disorders and muscle pathologies, Neurodegenerative diseases
Neurology Department, Atakpame Regional Hospital, Atakpame, Togo
Research Fields: Epileptology, Peripheral neurological disorders and muscle pathologies, Neurophysiology, movement disorders, neuroinflammatory diseases, Neurodegenerative diseases
Neurology Department, Sylvanus Olympio Teaching Hospital, Lome, Togo
Research Fields: Epileptology, Peripheral neurological disorders and muscle pathologies, Neurophysiology, movement disorders, neuroinflammatory diseases, Neurodegenerative diseases
Neurology Department, Kara Teaching Hospital, Kara, Togo
Research Fields: Epileptology, Peripheral neurological disorders, Neurophysiology, movement disorders, Neurodegenerative diseases
Neurology Department, University of Lome, Lome, Togo
Research Fields: Epileptology, Peripheral neurological disorders and muscle pathologies, Neurophysiology, movement disorders, neuroinflammatory diseases, Neurodegenerative diseases
Neurology Department, Campus Teaching Hospital, Lome, Togo
Research Fields: Epileptology, Peripheral neurological disorders, Neurophysiology, movement disorders, Neurodegenerative diseases
Information