Abstract
This study examines the determinants of health system performance in the countries of the Economic and Monetary Community of Central Africa (CEMAC) over the period 2007–2021. The analysis focuses on Cameroon, Chad, Gabon, Equatorial Guinea, the Central African Republic, and the Republic of Congo. Health systems in the region continue to face major structural constraints characterized by insufficient financing, weak governance, shortages of qualified health personnel, unequal access to healthcare services, and limited technological integration. In this context, identifying the main determinants of health system performance remains essential for improving healthcare delivery and achieving sustainable development objectives. The study adopts a multidimensional framework integrating economic, social, institutional, and technological determinants. Methodologically, the research relies on an unbalanced panel dataset and employs three complementary econometric approaches: Bayesian Model Averaging (BMA), Weighted Average Least Squares (WALS), and General-to-Specific Modelling (GenSpec). The Bayesian Model Averaging approach is particularly relevant because it explicitly addresses model uncertainty and simultaneously evaluates multiple competing explanatory variables, thereby reducing omitted variable bias and strengthening the robustness of the empirical analysis. The findings reveal that GDP per capita, financial development, life expectancy, government health expenditure, and final government consumption expenditure positively influence health system performance in the CEMAC region. These variables contribute to improving healthcare financing, infrastructure development, access to medical technologies, and the efficiency of healthcare delivery. In contrast, corruption negatively affects health system performance by weakening governance quality and generating inefficient allocation of public resources. The robustness analysis further identifies political stability, internet access, education, and trade openness as important complementary determinants supporting healthcare modernization and resilience. This study contributes to the literature by providing one of the few empirical analyses specifically focused on health system performance in the CEMAC region while combining Bayesian and classical model selection approaches to strengthen the reliability of the findings. The results suggest that strengthening governance, increasing public investment in health, promoting anti-corruption reforms, and accelerating digital transformation are essential policy priorities for improving health system performance and healthcare resilience in Central Africa. The study also emphasizes the importance of coordinated regional cooperation for achieving sustainable and equitable healthcare development objectives.
|
Published in
|
Central African Journal of Public Health (Volume 12, Issue 3)
|
|
DOI
|
10.11648/j.cajph.20261203.19
|
|
Page(s)
|
201-215 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Health System Performance, CEMAC, BMA, Governance, Public Health Expenditure, Determinants
1. Background
1.1. Context
During the 1990s, the member countries of the Economic and Monetary Community of Central Africa (CEMAC); Cameroon, Congo, Equatorial Guinea, Gabon, the Central African Republic, and Chad, faced significant health challenges. At that time, health systems were fragile, underfunded, and often inaccessible to a large share of the population. Limited health infrastructure and low levels of public investment in healthcare hindered the development of the sector
.
In response to international pressures and the recommendations of the World Health Organization (WHO), some countries attempted to increase their health budgets during the 2000s. For instance, Cameroon allocated 4.5% of its national budget to health in 2007, a commendable effort but still insufficient to meet growing needs
. In 2020, Chad devoted only 3.2% of its budget to health, thereby limiting the scope of its interventions and leaving a large proportion of the population without adequate access to care
.
Since 2018, a new momentum has emerged, marked by a shift towards universal health coverage (UHC) and improved access to care. Nevertheless, despite this renewed political commitment, health systems remain fragile, characterized by inadequate infrastructure, a shortage of qualified personnel, and precarious working conditions. Weak governance and inefficient resource management continue to hinder the performance of health systems, as illustrated by the situation in Gabon, which, despite allocating 6.3% of its GDP to health in 2021, still struggles to optimize the use of these funds
.
In the context of CEMAC countries, the performance of health systems cannot be analyzed in a unidimensional manner, as it is influenced by a wide range of interconnected factors. To better understand the drivers and constraints of this performance, it is useful to classify the determinants into three broad categories: social determinants, related to living conditions, education, demographics, and health behaviors; economic determinants, which refer to levels of funding, the efficiency of expenditure, the structure of public budgets, and economic growth; and institutional determinants, encompassing governance, political stability, the quality of public policies, and the capacity of institutions to organize and regulate the provision of healthcare. This classification allows for a more structured and operational understanding of the challenges faced by health systems in the sub-region.
1.2. Problem Statement
Theoretically, health system performance is a multidimensional construct encompassing efficiency, service quality, accessibility, equity and system resilience.
highlight the relevance of a systemic analytical framework that extends beyond input factors such as human, financial and physical capital, to include organizational processes as well as output and outcome performance. From this perspective, the determinants of performance can be grouped into internal factors, including governance structures, financing mechanisms and the organization and delivery of healthcare services, and external factors arising from the broader macroeconomic, political and socio institutional environment. However, these theoretical frameworks remain largely general and therefore require contextual adaptation in order to better reflect the structural constraints and institutional realities of health systems in developing economies, particularly in Central Africa.
Empirically, CEMAC countries exhibit a set of common structural characteristics that undermine the performance of their health systems, including low medical workforce density, chronic underfunding, dependence on external aid, and inefficient resource management. Despite the implementation of various strategies aimed at strengthening health systems, outcomes remain limited. For instance, the return on health investment remains low, inequalities in access to care persist, and crisis response mechanisms are still largely underdeveloped
| [5] | Mbau, R., Vassall, A., Gilson, L., &Barasa, E. (2023). Factors influencing the institutionalization of health technology assessment: a scoping literature review. Health Systems & Reform, 9(3), 2360315.
https://doi.org/10.1186/s12913-023-09673-4 |
[5]
. The COVID-19 pandemic further exposed systemic vulnerabilities, both in the management of the health emergency and in the continuity of essential care services
| [6] | Rowe, A. K., Rowe, S. Y., Peters, D. H., Holloway, K. A., Chalker, J., & Ross-Degnan, D. (2018). Effectiveness of strategies to improve health-care provider practices in low-income and middle-income countries: a systematic review. The Lancet Global Health, 6(11), e1163-e1175.
https://doi.org/10.1016/S2214-109X(18)30398-X |
[6]
. This empirical evidence highlights a persistent gap between the ambitions of public policies and their effective implementation on the ground.
From a factual standpoint, health indicators in the CEMAC region remain broadly below African averages, including high maternal and infant mortality rates, low vaccination coverage, and inadequate basic health infrastructure. This situation reflects a structural performance crisis, further exacerbated in some member countries by persistent political and economic instability. Against this backdrop, a central question arises: what are the determinants of health system performance in the CEMAC region?
1.3. Objective and Hypothesis
1.3.1. Objective
To address this question and deepen the understanding of health system performance in the CEMAC region, this study aims to assess the determinants of health system performance in CEMAC member countries.
1.3.2. Hypothesis
In line with this research question, the study is based on the following hypothesis: health system performance in the CEMAC region is determined by social, economic and institutional factors.
1.4. Literature Review
1.4.1. Theoretical Foundations of Health System Performance
The analysis of health system performance draws on several theoretical frameworks that help to capture its complexity. The Donabedian model (1988)
is a key reference in the assessment of healthcare quality. It is based on three interrelated dimensions: structure (resources, equipment and organizational arrangements), processes (clinical practices, coordination and interactions between patients and healthcare providers), and outcomes (patient health status, satisfaction and treatment effectiveness). This framework is particularly relevant for CEMAC countries, where weaknesses are often observed at the structural level, including inadequate infrastructure and shortages of qualified health personnel, which in turn negatively affect processes and ultimately outcomes. The strength of the Donabedian model lies in its ability to identify specific weak links within the system, thereby providing guidance for targeted policy reforms.
In addition,
proposes a more comprehensive and systemic perspective on the functioning of health systems. According to this approach, performance cannot be assessed in isolation, but must be understood through the entire set of system functions, namely governance, financing, service delivery, human resources, and knowledge generation. This framework places particular emphasis on equity and resilience, especially the ability of health systems to absorb shocks and maintain service provision during periods of crisis, as highlighted by the COVID-19 pandemic. For CEMAC countries, this model provides a relevant analytical framework given their exposure to recurrent crises, whether epidemiological, political or economic, as well as the frequent instability of governance structures.
Moreover, the economic literature offers a complementary perspective through the efficiency framework, as theorized by
. This approach is based on the notion of optimal resource allocation in order to maximize health outcomes, particularly in contexts of scarcity. Within this perspective, performance is assessed through the relationship between inputs mobilized (financing, personnel and equipment) and the outcomes achieved, such as improvements in population health, reductions in mortality and the extent of service coverage. This framework is especially relevant for CEMAC countries, where financial and human resources are both limited and unevenly distributed. The efficiency approach not only raises questions about the volume of resources mobilized, but more importantly about how they are utilized, while also highlighting the opportunity costs associated with weak governance and inefficient planning.
Thus, the integration of these three frameworks, quality of care (Donabedian), the systems approach (Frenk), and economic efficiency (Culyer), provides a robust theoretical foundation for analyzing health system performance. It also enhances the understanding of the specific challenges faced by low resource settings such as CEMAC countries, while helping to identify potential levers for improvement at the intersection of structural, organizational and economic dimensions.
1.4.2. Empirical Literature on Health System Performance
Beyond theoretical approaches, a growing body of empirical literature has examined the determinants and efficiency of health systems in both developed and developing economies. Several studies emphasize the role of governance quality, public health expenditure, technological integration, and institutional stability in shaping healthcare outcomes. In African countries, empirical analyses frequently reveal that weak institutional capacity, corruption, and insufficient financing significantly constrain health system performance.
Recent studies using efficiency and panel data approaches have contributed to a better understanding of healthcare system performance across regions. For instance,
| [10] | Kirigia, J. M., Asbu, E. Z., Kirigia, D. G., Onwujekwe, O., Fonta, W. M., & Ichoku, H. E. (2011). Technical efficiency of human resources for health in Africa. European Journal of Business and Management, 3(4), 321-345.
https://www.researchgate.net/profile/Fonta-William-2/publication/52000114_Kirigia_JM_Asbu_ZE_Kirigia_GD_Onwujekwe_EO_Fonta_MW_HE_Ichoku_2011_ |
[10]
highlighted the importance of efficient human resource allocation in improving healthcare delivery in African countries. Similarly,
| [11] | Selamzade F. & Yeşilyurt Ö. (2023). Evaluation of Efficiency Status of Health Systems of African Countries by Data Envelopment and Tobit Analysis, Anemon Journal of Social Sciences of Mus Alparslan University, 11(Afrika), 204-224. http://dx.doi.org/10.18506/anemon.1290327 |
[11]
employed Data Envelopment Analysis (DEA) and Tobit estimation techniques to evaluate the efficiency of African health systems and demonstrated substantial disparities across countries. In the context of Sub-Saharan Africa,
| [12] | Şener, M. (2025), Can Access to Health Services and Universal Health Coverage Improve the Efficiency of Health Systems in Sub-Saharan African Countries? A Study Based on a Two-Stage Dynamic Data Envelopment Analysis (DEA) Model. World Medical & Health Policy, 17: 883-897.
https://doi.org/10.1002/wmh3.70047 |
[12]
showed that universal health coverage and access to healthcare services positively influence health system efficiency.
Other studies have explored the relationship between governance, health expenditure, and healthcare efficiency.
| [13] | Novignon, J., & Nonvignon, J. (2015). Fiscal space for health in sub-Saharan African countries: an efficiency approach. African Journal of Health Economics, 4, 1-11.
http://dx.doi.org/10.35202/ajhe.2015.4102 |
[13]
emphasized the importance of fiscal space and efficient allocation of public resources in strengthening African health systems. Likewise,
| [14] | Sosa-Rubí, S. G., Bautista-Arredondo, S., Chivardi-Moreno, C. et al.. (2021). Efficiency, quality, and management practices in health facilities providing outpatient HIV services in Kenya, Nigeria, Rwanda, South Africa and Zambia. Health Care Manag Sci 24, 41–54.
https://doi.org/10.1007/s10729-020-09541-1 |
[14]
demonstrated that management practices and institutional quality significantly influence the efficiency of healthcare facilities in several African countries.
Despite these important contributions, empirical evidence focusing specifically on CEMAC countries remains limited. Existing studies generally concentrate on broader Sub-Saharan African regions or OECD countries and rarely account for the institutional and structural specificities of Central African economies. Furthermore, few studies combine Bayesian approaches with robustness techniques such as WALS and GenSpec to address model uncertainty in the analysis of health system performance. This study 2.2.1. Presentation of the Results ///There should be at least two subheadings at the same level, while there is only one subheading 2.2.1 under the heading 2.2. Please check and revise (You are advised to add a heading 2.2.2 or delete the heading 2.2.1). therefore contributes to the literature by filling this empirical and methodological gap.
1.5. Significance: Understanding in Order to Act More Effectively: Social, Economic and Institutional Challenges
This study is more relevant as it focuses on the economic and social mechanisms that directly influence the performance of health systems within the CEMAC region.
1) On one hand, it analyses the economic management of resources, which is often characterized by inefficient allocation practices that undermine the quality of healthcare services
| [15] | Bloom, N., Genakos, C., Sadun, R., & Van Reenen, J. (2012). Management practices across firms and countries. Academy of management perspectives, 26(1), 12-33.
https://doi.org/10.5465/amp.2011.0077 |
[15]
.
2) On the other hand, it considers the impact of social inequalities associated with poverty, education and access to decent living conditions, all of which strongly determine populations’ ability to access healthcare services
.
Health institutions, which lie at the core of the management and governance of healthcare systems, are often fragile within the CEMAC region, facing issues related to corruption and poor resource management
| [18] | Harrison, T. M., &Sayogo, D. S. (2014). Transparency, participation, and accountability practices in open government: A comparative study. Government information quarterly, 31(4), 513-525. https://doi.org/10.1016/j.giq.2014.08.002 |
| [19] | Keenan, P. J. (2014). International institutions and the resource curse. Penn St. JL & Int'l Aff., 3, 216.
https://papers.ssrn.com/sol3/Delivery.cfm?abstractid=2350395 |
[18, 19]
. This study therefore seeks to highlight these institutional shortcomings and to identify reform pathways suited to local contexts.
1.6. Contribution: An Innovative Approach to an Overlooked Region
This research helps to fill several gaps in the scientific literature by focusing specifically on the CEMAC region, which has too often been overlooked in studies examining health system performance.
1) It adopts a multidimensional approach that incorporates economic, social and institutional dimensions, thereby providing a comprehensive and nuanced perspective.
2) The study also employs an advanced econometric methodology, particularly the Bayesian Model Averaging (BMA) approach, which makes it possible to model the complex interactions between explanatory variables and to address more effectively the uncertainty associated with model selection.
1.7. Shortcomings in the Existing Literature
The literature on health system performance in CEMAC countries remains limited and is characterized by significant gaps. The region is under-represented in scientific research, which tends to focus on other parts of Africa, particularly West and East Africa
| [20] | Sieleunou, I., Turcotte-Tremblay, A. M., Fotso, J. C. T., Tamga, D. M., Yumo, H. A., Kouokam, E., &Ridde, V. (2017). Setting performance-based financing in the health sector agenda: a case study in Cameroon. Globalization and health, 13(1), 52.
https://doi.org/10.1186/s12992-017-0278-9 |
| [21] | Ongolo-Zogo, P., Lavis, J. N., Tomson, G., &Sewankambo, N. K. (2014). Initiatives supporting evidence informed health system policymaking in Cameroon and Uganda: a comparative historical case study. BMC health services research, 14(1), 612. https://doi.org/10.1186/s12913-014-0612-3 |
[20, 21]
. Comparative regional studies are scarce, as are analyses on regional health system integration and public–private partnerships
| [22] | Closa, C., Casini, L., & Sender, O. (2016). Comparative regional integration: Governance and legal models (Vol. 10). Cambridge University Press. |
[22]
.
Moreover, the standard theoretical and methodological frameworks commonly used to assess health system performance do not always capture the complexity and specificities of the CEMAC context. Aggregate indicators such as life expectancy or vaccination coverage often conceal local realities related to governance, corruption, and socio-economic inequality
| [23] | Kruk, M. E., Gage, A. D., Arsenault, C., Jordan, K., Leslie, H. H., Roder-DeWan, S.,... & Pate, M. (2018). High-quality health systems in the Sustainable Development Goals era: time for a revolution. The Lancet global health, 6(11), e1196-e1252.
https://doi.org/10.1016/S2214-109X(18)30386-3 |
[23]
.
Finally, existing research is often disciplinary in nature and tends to focus on a single dimension, thereby overlooking the interactions between economic, social, and institutional factors. A more integrated approach, such as that proposed by
| [24] | Nundoochan, A. (2021). Improving equity in the distribution and financing of health services in Mauritius, a small island state with deeply rooted welfare state standards. BMJ Global Health, 6(12). https://doi.org/10.1136/bmjgh-2021-006757 |
[24]
, is therefore required in order to better understand the determinants of health system performance in these countries.
1.8. Definitions
The concept of Health System Performance (HSP) is multidimensional and encompasses the assessment of efficiency, quality, equity and governance within health systems. According to the World Health Organization
| [25] | World Health Organization. (2000). The world health report 2000: health systems: improving performance. World Health Organization. |
[25]
, performance is measured through four key criteria: service coverage, efficiency of care, system responsiveness, and equity. Similarly, WHO (2007)
| [26] | World Health Organization. (2007). Everybody's business: strengthening health systems to improve health outcomes: WHO's framework for action. |
[26]
defines a health system as the ensemble of institutions and resources whose primary purpose is to improve the health of populations.
A high-performing health system ensures universal access to healthcare services, maintains high standards of quality, and guarantees the responsible management of human, material and financial resources
| [27] | Evans, D. B., Tandon, A., Murray, C. J., & Lauer, J. A. (2000). The comparative efficiency of national health systems in producing health: an analysis of 191 countries. World Health Organization, 29(29), 1-36. |
| [28] | Yüksel, O. (2021). Comparison of healthcare system performances in OECD countries. International Journal of Health Services Research and Policy, 6(2), 251-261.
https://doi.org/10.33457/ijhsrp.935170 |
[27, 28]
. Health system performance must also take into account the socio-economic and political context in which the system operates
. In the CEMAC region, fragmented governance, geographical disparities and insufficient financing are key determinants. The shortage of skilled health personnel, exacerbated by the migration of professionals towards better-resourced areas, negatively affects performance
| [30] | Mills, E. J., Kanters, S., Hagopian, A., Bansback, N., Nachega, J., Alberton, M.,... & Ford, N. (2011). The financial cost of doctors emigrating from sub-Saharan Africa: human capital analysis. Bmj, 343. https://doi.org/10.1136/bmj.d7031 |
[30]
. Health infrastructure, often concentrated in urban areas, leaves rural populations in a critical situation
| [31] | Frenk, J. (1992). Primary care and reform of health systems: a framework for the analysis of Latin American experiences. Health Services Management Research, 5(1), 32-43.
https://doi.org/10.1177/095148489200500104 |
[31]
.
1.9. Systemic Determinants of Performance
Three main dimensions characterize health system performance in the CEMAC region: efficiency, cost-effectiveness (or value for money), and vulnerability.
Efficiency refers to the optimal use of available resources—human, financial and material—in order to achieve the best possible health outcomes. According to
, an efficient health system is one that maximizes health outcomes for each unit of resources spent. In the CEMAC context, where resources are often scarce, this dimension is particularly critical. However, in several countries in the region, efficiency is constrained by poor resource allocation, weak coordination among stakeholders, and limited integration of health services.
Cost-effectiveness, while closely related to efficiency, refers more specifically to the system’s ability to generate measurable gains relative to the investments made. In public health systems, this is reflected in tangible outcomes such as reduced mortality rates, improved access to healthcare, and increased user satisfaction. However, according to
| [5] | Mbau, R., Vassall, A., Gilson, L., &Barasa, E. (2023). Factors influencing the institutionalization of health technology assessment: a scoping literature review. Health Systems & Reform, 9(3), 2360315.
https://doi.org/10.1186/s12913-023-09673-4 |
[5]
, the cost-effectiveness of health systems in the region remains generally low. This is often attributed to inadequate public policies, poorly strategic budgetary choices, and weak governance characterized by limited accountability and insufficient monitoring and evaluation mechanisms.
Finally, vulnerability that is, the capacity of health systems to withstand shocks such as pandemics, natural disasters, or humanitarian crises constitutes a third essential dimension of performance.
| [6] | Rowe, A. K., Rowe, S. Y., Peters, D. H., Holloway, K. A., Chalker, J., & Ross-Degnan, D. (2018). Effectiveness of strategies to improve health-care provider practices in low-income and middle-income countries: a systematic review. The Lancet Global Health, 6(11), e1163-e1175.
https://doi.org/10.1016/S2214-109X(18)30398-X |
[6]
highlight that this vulnerability is particularly pronounced in low-income countries, where resilience capacities are constrained by external factors such as dependence on international aid, political instability, and unequal access to health infrastructure. In the CEMAC region, this structural fragility has been clearly exposed by recent health crises, particularly the COVID-19 pandemic, which placed already under-resourced systems under severe strain.
2. Methodology
The aim of this section is to assess the determinants of health system performance in CEMAC countries using a panel data econometric approach. This approach makes it possible to control for country-specific effects while accounting for temporal dynamics.
2.1. Data and Variables of the Study
2.1.1. Data
The study is based on an unbalanced panel of six CEMAC countries (Cameroon, the Central African Republic, Chad, the Republic of the Congo, Gabon and Equatorial Guinea), covering the period from 2007 to 2021. The restriction of the observation period is mainly due to data availability, particularly for the health system performance index provided by the Legatum Institute. The data are drawn from reliable secondary sources such as:
1) Legatum Prosperity Index: for the composite indicator of health system performance.
2) World Bank (World Development Indicators, WDI): for macroeconomic data.
3) Worldwide Governance Indicators (WGI): for institutional governance indicators.
2.1.2. Description of the Variables
1) Dependent Variable
Health System Performance Index
. This index reflects the overall quality of the health system through six sub-dimensions:
2) Explanatory variables (determinants)
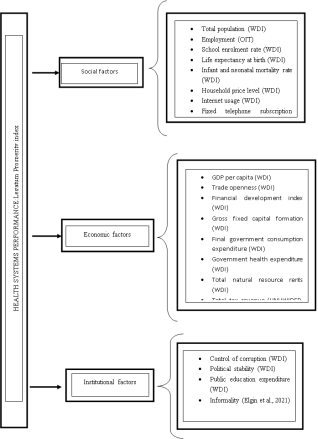
They are grouped into three main categories in line with the literature:
Figure 1. Conceptual Framework of the determinants of health performance.
2.1.3. Econometric Model Specification
To empirically analyze the determinants of health system performance (HS) in CEMAC countries, this study draws on the work of
| [33] | de Cos, P. H., & Moral-Benito, E. (2014). Determinants of health-system efficiency: evidence from OECD countries. International Journal of Health Care Finance and Economics, 14(1), 69-93. https://doi.org/10.1007/s10754-013-9140-7 |
[33]
, who employed the Bayesian Model Averaging (BMA) method to address model uncertainty arising from the selection of explanatory variables in the presence of multiple indicators. This approach is grounded in the seminal contributions of
| [34] | Raftery, A. E., Madigan, D., &Hoeting, J. A. (1997). Bayesian model averaging for linear regression models. Journal of the American Statistical Association, 92(437), 179-191.
https://doi.org/10.1080/01621459.1997.10473615 |
| [35] | Hoeting, J. A., Madigan, D., Raftery, A. E., &Volinsky, C. T. (1999). Bayesian model averaging: a tutorial (with comments by M. Clyde, David Draper and EI George, and a rejoinder by the authors. Statistical science, 14(4), 382-417.
https://doi.org/10.1002/jae.623 |
| [36] | Fernandez, C., Ley, E., & Steel, M. F. (2001). Model uncertainty in cross-country growth regressions. Journal of applied Econometrics, 16(5), 563-576. |
| [37] | Magnus, J. R., Powell, O., &Prüfer, P. (2010). A comparison of two model averaging techniques with an application to growth empirics. Journal of econometrics, 154(2), 139-153.
https://doi.org/10.1016/j.jeconom.2009.07.004 |
[34-37]
. The choice of the Bayesian Model Averaging (BMA) approach is motivated by the existence of significant model uncertainty regarding the determinants of health system performance in developing economies. Traditional panel data models, such as fixed effects or random effects estimations, generally require the researcher to select a single specification among numerous potential explanatory variables. Such an approach may generate omitted variable bias and unstable estimates, particularly when theoretical consensus regarding the relevant determinants remains limited. In contrast, BMA allows simultaneous evaluation of multiple competing models and computes posterior inclusion probabilities for each explanatory variable. This makes it possible to identify the most robust determinants while explicitly accounting for uncertainty associated with model selection. Given the multidimensional nature of health system performance and the relatively limited sample size of CEMAC countries, the BMA framework constitutes a more flexible and robust methodological approach. The baseline model is specified as a multiple linear regression as follows:
With , wheredenotes the level of health system performance in country i at time t, represents the matrix of social, economic, and institutional explanatory variables, and is the error term. Given that 21 indicators are retained as potential explanatory variables, the model can also be expressed as follows:
(2)
Estimating this equation directly using Ordinary Least Squares (OLS) would be problematic due to the large number of variables and the risk of multicollinearity. The BMA method therefore addresses this uncertainty by evaluating all possible combinations of variables, that is,= 2,097,152 potential models. For each model, the posterior probability is computed as follows:
(3)
Where is the sum of squared residuals of model i, is the number of parameters, and N is the number of observations? This makes it possible to compute the posterior inclusion probability (PIP) of a variable h:
(4)
A PIP greater than 0.5 indicates that the variable is considered a robust determinant of health system performance, in line with the criteria proposed by
| [33] | de Cos, P. H., & Moral-Benito, E. (2014). Determinants of health-system efficiency: evidence from OECD countries. International Journal of Health Care Finance and Economics, 14(1), 69-93. https://doi.org/10.1007/s10754-013-9140-7 |
[33]
.
The Bayesian estimation framework relies on prior assumptions regarding model probabilities and parameter distributions. In this study, non-informative priors are adopted in order to minimize subjective influence on the estimation process and allow the data to primarily drive posterior inference. Equal prior probabilities are assigned to competing models, while posterior inclusion probabilities are computed based on the likelihood contribution of each specification. The BMA approach is implemented to identify robust determinants under conditions of model uncertainty.
To enhance the robustness of the analysis, two complementary methods are employed. First, the Weighted Average Least Squares (WALS) method is used to estimate coefficients by weighting different model specifications according to their relevance
| [37] | Magnus, J. R., Powell, O., &Prüfer, P. (2010). A comparison of two model averaging techniques with an application to growth empirics. Journal of econometrics, 154(2), 139-153.
https://doi.org/10.1016/j.jeconom.2009.07.004 |
[37]
. WALS combines the advantages of ordinary least squares and Bayesian inference by adjusting estimated coefficients using Bayesian weights assigned to each model. This reduces estimation bias and improves the reliability of the results.
Second, the Generalized Specificity (GenSpec) method, as proposed by
, is used to correct biases related to model specification, particularly when certain variables, such as political turnover, are binary. GenSpec therefore helps to better control for selection effects and improves the precision of inference, especially in ANCOVA-type models.
2.2. Presentation of the Results and Robustness Analysis
This section presents and analyses the results of our estimations. First, we present the analysis of the main results, while in a second step we discuss the results of the robustness tests.
2.2.1. Base Results
The results obtained using the Bayesian Model Averaging (BMA) method, presented in
Table 1, identify seven (07) variables with a posterior inclusion probability (PIP) greater than 0.5, making them significant determinants of health system performance (HS) in the CEMAC region. Among these variables, five have a positive effect on health system performance, while two exhibit a negative effect.
Among the variables with a positive effect, GDP per capita stands out as an indicator of economic development. According to
| [39] | Swift, R. (2011). The relationship between health and GDP in OECD countries in the very long run. Health economics, 20(3), 306-322. https://doi.org/10.1002/hec.1590 |
[39]
, a higher GDP per capita strengthens healthcare financing through both public and private investment, particularly in infrastructure, medical technologies, and human resource training. The main channel of influence is financial, as it facilitates resource allocation and improves the quality of services delivered. Beyond this financial dimension, increases in GDP per capita also enhance the internal circulation dynamics of the health system. Indeed, a more prosperous economy promotes a better flow of resources, including financial flows, medical equipment, and health personnel, thereby reducing bottlenecks in service delivery. This improved circulation enhances coordination across different levels of care (primary, secondary, and tertiary) and enables faster and more efficient patient management. In addition, higher income levels stimulate demand for quality healthcare services, encouraging both public authorities and private actors to continuously improve service provision. Thus, GDP per capita is not merely an indicator of wealth but a structuring lever of overall health system performance, strengthening its financing capacity, organizational fluidity, and operational efficiency.
Financial development also emerges as a positive determinant.
| [40] | Liu, H., Saleem, M. M., Al-Faryan, M. A. S., Khan, I., & Zafar, M. W. (2022). Impact of governance and globalization on natural resources volatility: The role of financial development in the Middle East North Africa countries. Resources Policy, 78, 102881. https://doi.org/10.1016/j.resourpol.2022.102881 |
[40]
show that a strong banking system and efficient capital markets facilitate access to credit for households and health institutions, thereby promoting investment in medical equipment, research, and staff training. The channel of influence here is financial intermediation. Third, total population acts as a dual determinant.
argue that a larger population increases demand for healthcare services, which may place pressure on health facilities but can also generate economies of scale, particularly in logistics, vaccination campaigns, and drug distribution, thereby improving overall efficiency.
Fourth, life expectancy at birth is often viewed as an outcome of health system performance; however, it can also be used as a relevant determinant within a dynamic framework.
explain that it reflects the cumulative effects of preventive policies, access to healthcare, and treatment effectiveness. A higher life expectancy, in turn, influences the health system by shaping its structure, priorities, and efficiency. Indeed, longer life expectancy generally indicates better control of health risks, wider diffusion of healthy behaviors, and greater trust in health institutions, which encourages earlier and more regular use of healthcare services. The case of Japan is particularly illustrative: with one of the highest life expectancies globally, the country has developed a health system strongly oriented towards prevention, continuous care, and efficiency, thereby reinforcing a virtuous cycle between longevity and health system performance
| [43] | Hashimoto, H., Ikegami, N., Shibuya, K., Izumida, N., Noguchi, H., Yasunaga, H.,... & Reich, M. R. (2011). Cost containment and quality of care in Japan: is there a trade-off? The Lancet, 378(9797), 1174-1182.
https://doi.org/10.1016/S0140-6736(11)60987-2 |
[43]
. Hence, rather than being solely an outcome, life expectancy becomes a structuring signal that guides public policy, improves health information flows, and fosters more efficient system organization. It can therefore be considered an indirect but significant determinant of health system performance.
Finally, government health expenditure positively influences performance. According
| [44] | Onofrei, M., Vatamanu, A. F., Vintilă, G., &Cigu, E. (2021). Government health expenditure and public health outcomes: a comparative study among EU developing countries. International Journal of Environmental Research and Public Health, 18(20), 10725.
https://doi.org/10.3390/ijerph182010725 |
[44]
, increases in public health budgets improve system capacity through the acquisition of medical equipment, the construction of health facilities, and the remuneration of healthcare personnel. This channel operates through direct public investment in health infrastructure.
In contrast, two variables show a negative effect on health system performance in the CEMAC region. First, the tax level is negatively correlated with performance. This relationship suggests that high taxation may reduce households’ disposable income and limit consumption, including health-related spending. However,
| [45] | Reeves, A., Gourtsoyannis, Y., Basu, S., McCoy, D., McKee, M., &Stuckler, D. (2015). Financing universal health coverage—effects of alternative tax structures on public health systems: cross-national modelling in 89 low-income and middle-income countries. The Lancet, 386(9990), 274-280.
https://doi.org/10.1016/S0140-6736(15)60574-8 |
[45]
nuance this interpretation by noting that well-designed taxation systems can increase public revenues allocated to the health sector. Thus, the negative effect observed in the CEMAC context may be explained by inefficient tax management, poor allocation of fiscal revenues, or weak redistribution mechanisms. Second, government final consumption expenditure, when poorly allocated (for example towards recurrent or non-productive spending), may fail to contribute to improvements in health services, which explains its observed negative effect.
Table 1. BMA and WALS Results for the Determinants of Health System Performance in CEMAC.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 |
HS Performance | BMA | | | | WALS | | |
| Coef. | Std.Error | T | PIP | T | Coef. | Std.Error |
GDP per capita | 0.032 | 0.009 | 3.490 | 0.980 | 1.940 | 0.034 | 0.018 |
Trade openness | 0.000 | 0.003 | 0.120 | 0.070 | 1.290 | 0.017 | 0.013 |
Financial development | 0.709 | 0.143 | 4.970 | 1.000 | 4.250 | 0.599 | 0.141 |
GFCF2 | -0.000 | 0.001 | -0.060 | 0.060 | -0.520 | -0.004 | 0.007 |
Total population | 0.028 | 0.006 | 4.850 | 0.980 | 1.230 | 0.019 | 0.016 |
Employment | -0.000 | 0.008 | 0.000 | 0.060 | 0.460 | 0.026 | 0.057 |
Informality | 0.000 | 0.006 | 0.020 | 0.060 | 0.560 | 0.029 | 0.051 |
Inflation | -0.000 | 0.004 | -0.050 | 0.050 | -0.390 | -0.007 | 0.018 |
Corruption | -0.004 | 0.011 | -0.390 | 0.190 | -1.230 | -0.021 | 0.017 |
Political stability | 0.000 | 0.002 | 0.080 | 0.050 | 1.200 | 0.011 | 0.010 |
Internet access | 0.000 | 0.002 | 0.170 | 0.080 | 2.080 | 0.010 | 0.005 |
Fixed telephone lines | 0.000 | 0.001 | 0.120 | 0.070 | 1.540 | 0.003 | 0.002 |
Total natural resources revenue | -0.000 | 0.001 | -0.050 | 0.060 | -0.810 | -0.008 | 0.009 |
Education | 0.002 | 0.009 | 0.270 | 0.120 | 1.540 | 0.027 | 0.017 |
Infant mortality at birth | -0.005 | 0.022 | -0.230 | 0.150 | 0.100 | 0.012 | 0.123 |
Infant mortality (-52 years) | -0.015 | 0.031 | -0.470 | 0.270 | -0.570 | -0.063 | 0.110 |
Life expectancy at birth | 0.474 | 0.157 | 3.010 | 0.970 | 1.090 | 0.161 | 0.147 |
Taxes | -0.118 | 0.106 | -1.110 | 0.630 | -0.500 | -0.056 | 0.113 |
Household consumption expenditure | 0.000 | 0.003 | 0.090 | 0.060 | -0.590 | -0.011 | 0.019 |
Final Government consumption expenditure | 0.021 | 0.006 | 3.260 | 0.970 | 3.100 | 0.023 | 0.007 |
Government health expenditure | 0.010 | 0.007 | 1.380 | 0.720 | 1.020 | 0.005 | 0.005 |
Constant term | -2.199 | 0.654 | -3.360 | 1.000 | -1.530 | -1.040 | 0.596 |
Source: Authors calculations.
2.2.2. Robustness Analysis of the Results
The robustness analysis conducted using the WALS approach (columns 5 to 7 of
Table 1) complements the results obtained through the BMA method by identifying four additional significant determinants of health system performance (HS) in the CEMAC region: corruption, political stability, internet use, and fixed telephone usage.
Corruption has a negative effect on health system performance.
| [46] | Tormusa, D. O., &Idom, A. M. (2016). The impediments of corruption on the efficiency of healthcare service delivery in Nigeria. Online Journal of Health Ethics, 12(1), 3.
https://doi.org/10.18785/ojhe.1201.03 |
[46]
argue that it leads to the misallocation of resources, unequal access to healthcare, and undermines trust in health institutions. The main transmission channel is institutional, as corruption weakens governance structures and reduces the efficiency of resource allocation.
In contrast, political stability exerts a positive effect, as it promotes more effective governance and better planning of health expenditures
| [47] | Tibrewal, K., & Chaudhuri, S. (2022). Institutional quality and public healthcare. Theoretical & Applied Economics, 29(1). |
[47]
. The channel of influence operates through improved governance quality and policy continuity.
Furthermore, increased use of the internet and fixed telephone lines enhances health system performance by facilitating communication, medical data management, and telemedicine services, as demonstrated by
| [48] | Kvedar, J., Coye, M. J., & Everett, W. (2014). Connected health: a review of technologies and strategies to improve patient care with telemedicine and telehealth. Health affairs, 33(2), 194-199. https://doi.org/10.1377/hlthaff.2013.0992 |
[48]
and
, respectively. These results highlight the importance of ICT development in modernizing the health sector.
The results obtained from the GenSpec approach (
Table 2), which is based on a general-to-specific estimation strategy, broadly confirm the robustness of the model, as indicated by a Chi-square statistic that is significant at the 1% level and an R² value close to 1. Out of the 21 initial indicators, only 8 are retained as significant determinants.
Among these, corruption once again confirms its negative effect, highlighting its recurrent role in undermining health system performance. In contrast, two new factors emerge with a positive influence: the level of education and trade openness. A higher level of education enhances understanding of health-related issues, improves adherence to health policies, and contributes to better hygiene practices and disease prevention. Trade openness, in turn, facilitates the importation of medical technologies, pharmaceuticals, and healthcare equipment, while also promoting the exchange of skills and best practices (through the channel of economic integration).
Taken together, these results show that beyond traditional economic factors, health system performance in the CEMAC region is strongly influenced by institutional quality, political stability, technological diffusion, as well as the integration of human capital and international trade into health strategies.
Table 2. Determinants of Health System Performance (General-to-Specific Approach).
VARIABLES | HS performance |
GDP per capita | 0.0526*** |
(0.00301) |
Trade openness | 0.0188** |
(0.00868) |
Financial development | 0.628*** |
(0.115) |
Total population | 0.0277*** |
(0.00450) |
Internet access | 0.00911*** |
0.00270 |
Education | 0.0550*** |
0.0121 |
Final gov. consum. Exp | 0.0274*** |
(0.00475) |
Corruption | -0.0237 |
(0.0138) |
Constant term | -0.503*** |
(0.0947) |
Observations | 90 |
Number of countries | 6 |
Chi 2 | 5748*** |
R2 between | 1.000 |
R2 within | 0.861 |
Source: Authors calculations.
In summary, although the different estimation methods (BMA, WALS, and GenSpec) produced partially divergent results, they nevertheless converge towards a limited set of key and robust variables. To reliably identify these determinants, the authors synthesized the results in
Table 3 by assigning a score of 1 to each variable selected by a given method, and 0 otherwise. Consequently, only variables selected by at least two of the three approaches are considered robust determinants of health system performance. This procedure helps to reduce interpretation bias and avoid unfounded economic policy recommendations. Ultimately, 8 out of the 21 initial indicators emerge as truly determinant variables and are highlighted in
Table 3.
Table 3. Summary of the Selected Indicators.
Variables | BMA | WAL | GenSpec | Score |
GDP per capita | 1 | 1 | 1 | 3 |
Trade openness | 0 | 0 | 1 | 1 |
Financial development | 1 | 1 | 1 | 3 |
GFCF | 0 | 0 | 0 | 0 |
Total population | 1 | 1 | 1 | 3 |
Employment | 0 | 0 | 0 | 0 |
Informality | 0 | 0 | 0 | 0 |
Inflation | 0 | 0 | 0 | 0 |
Corruption | 0 | 1 | 1 | 2 |
Political stability | 0 | 1 | 0 | 1 |
Internet access | 0 | 1 | 1 | 2 |
Fixed telephone | 0 | 1 | 0 | 1 |
Total natural resources | 0 | 0 | 0 | 0 |
Education | 0 | 0 | 1 | 1 |
Infant mortality | 0 | 0 | 0 | 0 |
Under-five mortality | 0 | 0 | 0 | 0 |
Life expectancy | 1 | 1 | 0 | 2 |
Taxes | 1 | 0 | 0 | 1 |
Household consumption | 0 | 0 | 0 | 0 |
Fin. Gov. Consum. Exp. | 1 | 1 | 1 | 3 |
Gov. health exp. | 1 | 1 | 0 | 2 |
Source: Authors calculations
3. Limitations of the Study
Despite its contributions, this study presents several limitations. First, the analysis is restricted to six CEMAC countries over the period 2007–2021 due to data availability constraints, particularly regarding the social, economic and institutional factors provided by the WDI. Second, the study relies on an unbalanced panel dataset, which may limit the generalizability of certain findings. Third, although the selected variables capture major economic, social, and institutional dimensions, other potentially relevant determinants such as healthcare workforce quality, regional inequalities, and health infrastructure indicators could not be fully incorporated because of missing data. Finally, while the Bayesian framework reduces model uncertainty, the results remain sensitive to the quality and availability of secondary data sources. Future research could therefore extend the analysis by incorporating additional countries, longer time periods, and more disaggregated indicators of healthcare system performance.
4. Conclusion
This article aimed to identify the main determinants of health system performance in the CEMAC countries through a rigorous empirical analysis employing three advanced econometric methods: Bayesian Model Averaging (BMA), Weighted Average Least Squares (WALS), and General-to-Specific Modelling (GenSpec). Each of these approaches presents specific methodological advantages. BMA formally addresses the uncertainty surrounding the selection of explanatory variables by simultaneously testing multiple models; WALS assigns weights to variables according to their statistical relevance and reduces omission bias; while GenSpec progressively refines the model by eliminating non-significant variables. By combining these three complementary approaches, the study ensures the robustness of the results obtained and avoids interpretation errors that could arise from relying on a single and potentially biased model.
The empirical findings consistently show that certain economic, institutional, and technological factors play a central role in the performance of health systems within the CEMAC region. From an economic perspective, three variables emerge as major determinants: GDP per capita, financial development, and public health expenditure. A higher level of GDP per capita enhances the capacity to finance health infrastructure, reflecting the direct relationship between economic development and the quality of healthcare services. The development of the financial sector, by facilitating access to credit and investment, enables households and medical institutions to better cope with health-related expenditures. Finally, government expenditure on health reflects the State’s commitment to the sector, and its positive impact highlights the importance of sustained budgetary support to ensure the acquisition of medical equipment, the construction of infrastructure, and adequate remuneration for healthcare personnel.
Furthermore, the study highlights the crucial role of institutional and technological factors in health system performance. Corruption, for example, constitutes a significant obstacle: weak governance leads to poor resource allocation, limits the efficiency of health expenditure, and undermines public confidence in healthcare services. This finding is consistent with the work of
| [50] | Ndulu, B. J. (2007). Challenges of African growth: Opportunities, constraints, and strategic directions. World Bank Publications. https://hdl.handle.net/10986/6656 |
[50]
, who emphasized the detrimental impact of corruption on the performance of public services. Conversely, political stability fosters an environment conducive to the effective implementation of health policies. From a technological perspective, the use of the internet and even traditional telecommunications (fixed-line telephones) appear to be important facilitators, enabling improved circulation of medical information, supporting telemedicine, and optimizing the management of health data. These technological tools contribute to the modernization of health systems, particularly in contexts where physical access to healthcare services remains limited.
Ultimately, the performance of health systems in the CEMAC region depends on a multidimensional set of factors related to the level of economic development, institutional strength, public governance, and the degree of technological integration. To sustainably improve the quality, accessibility, and efficiency of healthcare services in the region, public policies must therefore adopt an integrated approach combining economic reforms, institutional strengthening, anti-corruption measures, investment in ICTs, and continuous increases in public health expenditure. Only through such a comprehensive and coordinated vision will the health systems of CEMAC countries be able to meet the growing needs of their populations and fully contribute to the region’s human and sustainable development objectives.
This study contributes to the existing literature in several important ways. From a methodological perspective, it combines Bayesian Model Averaging, WALS, and GenSpec approaches in order to address model uncertainty and strengthen the robustness of empirical findings. From an empirical perspective, it provides one of the few comprehensive analyses specifically dedicated to the determinants of health system performance in CEMAC countries. The study also highlights the central role of governance quality, technological integration, and macroeconomic stability in improving healthcare outcomes in developing economies. These contributions provide useful evidence for policymakers seeking to strengthen healthcare resilience and accelerate progress toward universal health coverage in Central Africa.
5. Recommendations
In light of the robust empirical results obtained through the BMA, WALS, and GenSpec methods, several priority areas for intervention emerge to improve the performance of health systems in CEMAC countries. These recommendations are based on the factors identified as significantly associated with health system performance and aim to strengthen efficiency, equity, and resilience within the region’s health systems.
5.1. Strengthening Inclusive Economic Growth
3) Increase GDP per capita through policies that promote economic growth, diversification, and the creation of decent employment opportunities.
4) Promote investment in productive and socially beneficial sectors (agriculture, light industry, education, and health) in order to improve population welfare while strengthening the fiscal base of States.
5) Ensure that the benefits of growth are equitably distributed in order to reduce social inequalities, which in turn influence access to healthcare services.
5.2. Developing the Financial Sector in Support of Health
1) Strengthen financial inclusion, particularly for rural populations and private healthcare providers, by improving access to credit, microfinance, and appropriate health insurance products.
2) Promote financial inclusion and the digitalization of payment systems in order to improve transparency and the efficient allocation of resources within the health sector.
3) Develop innovative financing instruments (health funds, social bonds, public–private partnerships) to broaden the funding base of the health sector.
5.3. Improving Governance and Combating Corruption in the Health Sector
1) Strengthen transparency and accountability mechanisms, particularly through regular audits, participatory budget monitoring platforms, and effective sanctions in cases of misappropriation of funds.
2) Implement electronic resource and procurement management systems (e-health, e-procurement) to reduce losses and improve expenditure efficiency.
3) Raise awareness among health sector stakeholders on professional ethics and anti-corruption practices through targeted training and campaigns.
5.4. Increasing Public Health Expenditure and Improving Its Efficiency
1) Gradually and sustainably increase the health budget in line with the Abuja Declaration commitment (at least 15% of the national budget).
2) Reallocate public expenditure towards essential primary healthcare services, particularly in underserved areas.
3) Improve planning of investments in health infrastructure (health centers, hospitals, laboratories) as well as recruitment and training of healthcare personnel.
5.5. Fully Integrating Information and Communication Technologies (ICTs)
1) Promote the adoption of ICTs in the health sector, including telemedicine, electronic medical records, inter-institutional communication platforms, and epidemiological alert systems.
2) Reduce the digital divide by investing in internet infrastructure and training healthcare professionals in the use of digital tools.
3) Establish a legal and regulatory framework to govern the development of e-health and ensure the protection of personal data.
5.6. Emphasizing Education and Trade Openness
1) Invest in education, particularly in health and hygiene, in order to improve prevention, encourage healthy behaviors, and promote the rational use of healthcare services.
2) Encourage controlled trade openness to facilitate access to high-quality medical equipment, essential medicines, and medical innovations.
Abbreviations
ANCOVA | Analysis of Covariance |
BMA | Bayesian Model Averaging |
CEMAC | Economic and Monetary Community of Central Africa |
COVID-19 | Coronavirus Disease 2019 |
GenSpec | General-to-Specific Modelling |
GDP | Gross Domestic Product |
GFCF | Gross Fixed Capital Formation |
HS | Health System |
HSP | Health System Performance |
ICTs | Information and Communication Technologies |
OLS | Ordinary Least Squares |
PIP | Posterior Inclusion Probability |
UHC | Universal Health Coverage |
WALS | Weighted Average Least Squares |
WDI | World Development Indicators |
WGI | Worldwide Governance Indicators |
WHO | World Health Organization |
Author Contributions
Fleurine Paola Njanga Tsele: Conceptualization, Investigation, Data curation, Resources, Methodology, Writing – original draft, Software
Albert Ze: Supervision, Validation, Data curation, Writing – review & editing, Formal analysis, Software
Jean Tchitchoua: Methodology, Supervision, Validation, Writing – review & editing
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix
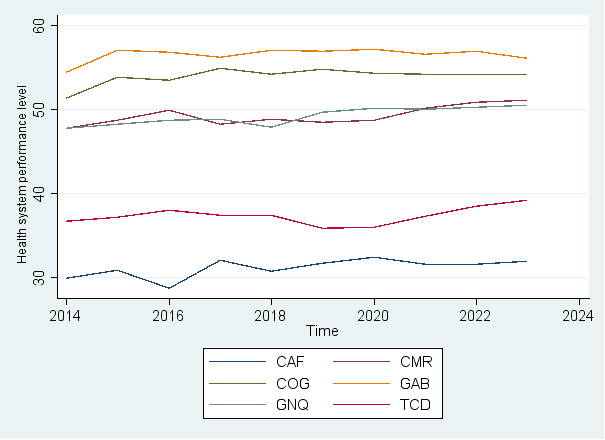
Appendix I: Comparative Evolution of Health System Performance Levels Among CEMAC Countries (2007–2022)
Figure 2. Trends in Health System Performance in CEMAC Countries (2014–2023).
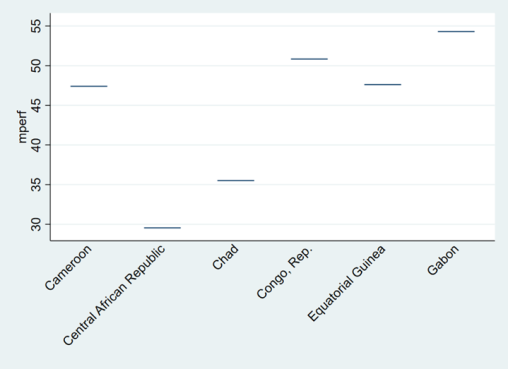
Appendix II: Comparative Health System Performance Across CEMAC Countries
Figure 3. Average Health System Performance Across CEMAC Countries.
Key: mperf = mean health system performance
Source: Authors construction
References
| [1] |
Mondiale, B. (2020). Evaluation of the Economic Impact of COVID-19 and Policy Responses in Sub-Saharan Africa. Report of the Office of the Chief Economist for the Africa Region, Africa’s Pulse, 21.
https://www.atibt.org/wp-content/uploads/2020/04/AFRIQUE-Africas-Pulse-Analyse-de-lImpact-Economique-vFR-202004.pdf
|
| [2] |
World Health Organization. (2022). Atlas of African health statistics 2022: health situation analysis of the WHO African Region—country profiles.
https://iris.who.int/bitstream/handle/10665/364837/9789290234852-eng.pdf
|
| [3] |
National Institute of Statistics. (2021). Statistical Report 2021.
https://ins-cameroun.cm/2021/
|
| [4] |
McPake, B., & Hanson, K. (2016). Managing the public–private mix to achieve universal health coverage. The lancet, 388(10044), 622-630.
https://doi.org/10.1016/S0140-6736(16)00344-5
|
| [5] |
Mbau, R., Vassall, A., Gilson, L., &Barasa, E. (2023). Factors influencing the institutionalization of health technology assessment: a scoping literature review. Health Systems & Reform, 9(3), 2360315.
https://doi.org/10.1186/s12913-023-09673-4
|
| [6] |
Rowe, A. K., Rowe, S. Y., Peters, D. H., Holloway, K. A., Chalker, J., & Ross-Degnan, D. (2018). Effectiveness of strategies to improve health-care provider practices in low-income and middle-income countries: a systematic review. The Lancet Global Health, 6(11), e1163-e1175.
https://doi.org/10.1016/S2214-109X(18)30398-X
|
| [7] |
Donabedian, A. (1988). The quality of care: how can it be assessed? Jama, 260(12), 1743-1748.
https://doi.org/10.1001/jama.1988.03410120089033
|
| [8] |
Frenk, J. (2010). The global health system: strengthening national health systems as the next step for global progress. PLoS medicine, 7(1), e1000089.
https://doi.org/10.1371/journal.pmed.1000089
|
| [9] |
Culyer, A. J. (2001). Equity-some theory and its policy implications. Journal of medical ethics, 27(4), 275-283.
https://doi.org/10.1136/jme.27.4.275
|
| [10] |
Kirigia, J. M., Asbu, E. Z., Kirigia, D. G., Onwujekwe, O., Fonta, W. M., & Ichoku, H. E. (2011). Technical efficiency of human resources for health in Africa. European Journal of Business and Management, 3(4), 321-345.
https://www.researchgate.net/profile/Fonta-William-2/publication/52000114_Kirigia_JM_Asbu_ZE_Kirigia_GD_Onwujekwe_EO_Fonta_MW_HE_Ichoku_2011_
|
| [11] |
Selamzade F. & Yeşilyurt Ö. (2023). Evaluation of Efficiency Status of Health Systems of African Countries by Data Envelopment and Tobit Analysis, Anemon Journal of Social Sciences of Mus Alparslan University, 11(Afrika), 204-224.
http://dx.doi.org/10.18506/anemon.1290327
|
| [12] |
Şener, M. (2025), Can Access to Health Services and Universal Health Coverage Improve the Efficiency of Health Systems in Sub-Saharan African Countries? A Study Based on a Two-Stage Dynamic Data Envelopment Analysis (DEA) Model. World Medical & Health Policy, 17: 883-897.
https://doi.org/10.1002/wmh3.70047
|
| [13] |
Novignon, J., & Nonvignon, J. (2015). Fiscal space for health in sub-Saharan African countries: an efficiency approach. African Journal of Health Economics, 4, 1-11.
http://dx.doi.org/10.35202/ajhe.2015.4102
|
| [14] |
Sosa-Rubí, S. G., Bautista-Arredondo, S., Chivardi-Moreno, C. et al.. (2021). Efficiency, quality, and management practices in health facilities providing outpatient HIV services in Kenya, Nigeria, Rwanda, South Africa and Zambia. Health Care Manag Sci 24, 41–54.
https://doi.org/10.1007/s10729-020-09541-1
|
| [15] |
Bloom, N., Genakos, C., Sadun, R., & Van Reenen, J. (2012). Management practices across firms and countries. Academy of management perspectives, 26(1), 12-33.
https://doi.org/10.5465/amp.2011.0077
|
| [16] |
Marmot, M. (2005). Social determinants of health inequalities. The lancet, 365(9464), 1099-1104.
https://doi.org/10.1016/S0140-6736(05)71146-6
|
| [17] |
Sen, A. (1999). Freedom. Development, Oxford University Press, Oxford.
https://www.academia.edu/download/62207935/10._Sen_1999120200226-89537-10i3ce1.pdf
|
| [18] |
Harrison, T. M., &Sayogo, D. S. (2014). Transparency, participation, and accountability practices in open government: A comparative study. Government information quarterly, 31(4), 513-525.
https://doi.org/10.1016/j.giq.2014.08.002
|
| [19] |
Keenan, P. J. (2014). International institutions and the resource curse. Penn St. JL & Int'l Aff., 3, 216.
https://papers.ssrn.com/sol3/Delivery.cfm?abstractid=2350395
|
| [20] |
Sieleunou, I., Turcotte-Tremblay, A. M., Fotso, J. C. T., Tamga, D. M., Yumo, H. A., Kouokam, E., &Ridde, V. (2017). Setting performance-based financing in the health sector agenda: a case study in Cameroon. Globalization and health, 13(1), 52.
https://doi.org/10.1186/s12992-017-0278-9
|
| [21] |
Ongolo-Zogo, P., Lavis, J. N., Tomson, G., &Sewankambo, N. K. (2014). Initiatives supporting evidence informed health system policymaking in Cameroon and Uganda: a comparative historical case study. BMC health services research, 14(1), 612.
https://doi.org/10.1186/s12913-014-0612-3
|
| [22] |
Closa, C., Casini, L., & Sender, O. (2016). Comparative regional integration: Governance and legal models (Vol. 10). Cambridge University Press.
|
| [23] |
Kruk, M. E., Gage, A. D., Arsenault, C., Jordan, K., Leslie, H. H., Roder-DeWan, S.,... & Pate, M. (2018). High-quality health systems in the Sustainable Development Goals era: time for a revolution. The Lancet global health, 6(11), e1196-e1252.
https://doi.org/10.1016/S2214-109X(18)30386-3
|
| [24] |
Nundoochan, A. (2021). Improving equity in the distribution and financing of health services in Mauritius, a small island state with deeply rooted welfare state standards. BMJ Global Health, 6(12).
https://doi.org/10.1136/bmjgh-2021-006757
|
| [25] |
World Health Organization. (2000). The world health report 2000: health systems: improving performance. World Health Organization.
|
| [26] |
World Health Organization. (2007). Everybody's business: strengthening health systems to improve health outcomes: WHO's framework for action.
|
| [27] |
Evans, D. B., Tandon, A., Murray, C. J., & Lauer, J. A. (2000). The comparative efficiency of national health systems in producing health: an analysis of 191 countries. World Health Organization, 29(29), 1-36.
|
| [28] |
Yüksel, O. (2021). Comparison of healthcare system performances in OECD countries. International Journal of Health Services Research and Policy, 6(2), 251-261.
https://doi.org/10.33457/ijhsrp.935170
|
| [29] |
McCartney, G., Popham, F., McMaster, R., & Cumbers, A. (2019). Defining health and health inequalities. Public health, 172, 22-30.
https://doi.org/10.1016/j.puhe.2019.03.023
|
| [30] |
Mills, E. J., Kanters, S., Hagopian, A., Bansback, N., Nachega, J., Alberton, M.,... & Ford, N. (2011). The financial cost of doctors emigrating from sub-Saharan Africa: human capital analysis. Bmj, 343.
https://doi.org/10.1136/bmj.d7031
|
| [31] |
Frenk, J. (1992). Primary care and reform of health systems: a framework for the analysis of Latin American experiences. Health Services Management Research, 5(1), 32-43.
https://doi.org/10.1177/095148489200500104
|
| [32] |
Legatum institute, Prosperity index
https://www.prosperity.com
|
| [33] |
de Cos, P. H., & Moral-Benito, E. (2014). Determinants of health-system efficiency: evidence from OECD countries. International Journal of Health Care Finance and Economics, 14(1), 69-93.
https://doi.org/10.1007/s10754-013-9140-7
|
| [34] |
Raftery, A. E., Madigan, D., &Hoeting, J. A. (1997). Bayesian model averaging for linear regression models. Journal of the American Statistical Association, 92(437), 179-191.
https://doi.org/10.1080/01621459.1997.10473615
|
| [35] |
Hoeting, J. A., Madigan, D., Raftery, A. E., &Volinsky, C. T. (1999). Bayesian model averaging: a tutorial (with comments by M. Clyde, David Draper and EI George, and a rejoinder by the authors. Statistical science, 14(4), 382-417.
https://doi.org/10.1002/jae.623
|
| [36] |
Fernandez, C., Ley, E., & Steel, M. F. (2001). Model uncertainty in cross-country growth regressions. Journal of applied Econometrics, 16(5), 563-576.
|
| [37] |
Magnus, J. R., Powell, O., &Prüfer, P. (2010). A comparison of two model averaging techniques with an application to growth empirics. Journal of econometrics, 154(2), 139-153.
https://doi.org/10.1016/j.jeconom.2009.07.004
|
| [38] |
Magnus, J. R., & De Luca, G. (2016). Weighted average least squares (WALS): a survey. Journal of Economic Surveys, 30(1), 117-148.
https://doi.org/10.1111/joes.12094
|
| [39] |
Swift, R. (2011). The relationship between health and GDP in OECD countries in the very long run. Health economics, 20(3), 306-322.
https://doi.org/10.1002/hec.1590
|
| [40] |
Liu, H., Saleem, M. M., Al-Faryan, M. A. S., Khan, I., & Zafar, M. W. (2022). Impact of governance and globalization on natural resources volatility: The role of financial development in the Middle East North Africa countries. Resources Policy, 78, 102881.
https://doi.org/10.1016/j.resourpol.2022.102881
|
| [41] |
Mendelson, D. N., & Schwartz, W. B. (1993). The effects of aging and population growth on health care costs. Health affairs, 12(1), 119-125.
https://doi.org/10.1377/hlthaff.12.1.119
|
| [42] |
Zarulli, V., Sopina, E., Toffolutti, V., &Lenart, A. (2021). Health care system efficiency and life expectancy: A 140-country study. PLoS One, 16(7), e0253450.
https://doi.org/10.1371/journal.pone.0253450
|
| [43] |
Hashimoto, H., Ikegami, N., Shibuya, K., Izumida, N., Noguchi, H., Yasunaga, H.,... & Reich, M. R. (2011). Cost containment and quality of care in Japan: is there a trade-off? The Lancet, 378(9797), 1174-1182.
https://doi.org/10.1016/S0140-6736(11)60987-2
|
| [44] |
Onofrei, M., Vatamanu, A. F., Vintilă, G., &Cigu, E. (2021). Government health expenditure and public health outcomes: a comparative study among EU developing countries. International Journal of Environmental Research and Public Health, 18(20), 10725.
https://doi.org/10.3390/ijerph182010725
|
| [45] |
Reeves, A., Gourtsoyannis, Y., Basu, S., McCoy, D., McKee, M., &Stuckler, D. (2015). Financing universal health coverage—effects of alternative tax structures on public health systems: cross-national modelling in 89 low-income and middle-income countries. The Lancet, 386(9990), 274-280.
https://doi.org/10.1016/S0140-6736(15)60574-8
|
| [46] |
Tormusa, D. O., &Idom, A. M. (2016). The impediments of corruption on the efficiency of healthcare service delivery in Nigeria. Online Journal of Health Ethics, 12(1), 3.
https://doi.org/10.18785/ojhe.1201.03
|
| [47] |
Tibrewal, K., & Chaudhuri, S. (2022). Institutional quality and public healthcare. Theoretical & Applied Economics, 29(1).
|
| [48] |
Kvedar, J., Coye, M. J., & Everett, W. (2014). Connected health: a review of technologies and strategies to improve patient care with telemedicine and telehealth. Health affairs, 33(2), 194-199.
https://doi.org/10.1377/hlthaff.2013.0992
|
| [49] |
Blaya, J. A., Fraser, H. S., & Holt, B. (2010). E-health technologies show promise in developing countries. Health affairs, 29(2), 244-251.
https://doi.org/10.1377/hlthaff.2009.0894
|
| [50] |
Ndulu, B. J. (2007). Challenges of African growth: Opportunities, constraints, and strategic directions. World Bank Publications.
https://hdl.handle.net/10986/6656
|
Cite This Article
-
APA Style
Tsele, F. P. N., Ze, A., Tchitchoua, J. (2026). Health System Performance in CEMAC: A Bayesian Analysis of Key Determinants. Central African Journal of Public Health, 12(3), 201-215. https://doi.org/10.11648/j.cajph.20261203.19
 Copy
|
Copy
|
 Download
Download
ACS Style
Tsele, F. P. N.; Ze, A.; Tchitchoua, J. Health System Performance in CEMAC: A Bayesian Analysis of Key Determinants. Cent. Afr. J. Public Health 2026, 12(3), 201-215. doi: 10.11648/j.cajph.20261203.19
Copy
|
Download
AMA Style
Tsele FPN, Ze A, Tchitchoua J. Health System Performance in CEMAC: A Bayesian Analysis of Key Determinants. Cent Afr J Public Health. 2026;12(3):201-215. doi: 10.11648/j.cajph.20261203.19
Copy
|
Download
-
@article{10.11648/j.cajph.20261203.19,
author = {Fleurine Paola Njanga Tsele and Albert Ze and Jean Tchitchoua},
title = {Health System Performance in CEMAC: A Bayesian Analysis of Key Determinants},
journal = {Central African Journal of Public Health},
volume = {12},
number = {3},
pages = {201-215},
doi = {10.11648/j.cajph.20261203.19},
url = {https://doi.org/10.11648/j.cajph.20261203.19},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cajph.20261203.19},
abstract = {This study examines the determinants of health system performance in the countries of the Economic and Monetary Community of Central Africa (CEMAC) over the period 2007–2021. The analysis focuses on Cameroon, Chad, Gabon, Equatorial Guinea, the Central African Republic, and the Republic of Congo. Health systems in the region continue to face major structural constraints characterized by insufficient financing, weak governance, shortages of qualified health personnel, unequal access to healthcare services, and limited technological integration. In this context, identifying the main determinants of health system performance remains essential for improving healthcare delivery and achieving sustainable development objectives. The study adopts a multidimensional framework integrating economic, social, institutional, and technological determinants. Methodologically, the research relies on an unbalanced panel dataset and employs three complementary econometric approaches: Bayesian Model Averaging (BMA), Weighted Average Least Squares (WALS), and General-to-Specific Modelling (GenSpec). The Bayesian Model Averaging approach is particularly relevant because it explicitly addresses model uncertainty and simultaneously evaluates multiple competing explanatory variables, thereby reducing omitted variable bias and strengthening the robustness of the empirical analysis. The findings reveal that GDP per capita, financial development, life expectancy, government health expenditure, and final government consumption expenditure positively influence health system performance in the CEMAC region. These variables contribute to improving healthcare financing, infrastructure development, access to medical technologies, and the efficiency of healthcare delivery. In contrast, corruption negatively affects health system performance by weakening governance quality and generating inefficient allocation of public resources. The robustness analysis further identifies political stability, internet access, education, and trade openness as important complementary determinants supporting healthcare modernization and resilience. This study contributes to the literature by providing one of the few empirical analyses specifically focused on health system performance in the CEMAC region while combining Bayesian and classical model selection approaches to strengthen the reliability of the findings. The results suggest that strengthening governance, increasing public investment in health, promoting anti-corruption reforms, and accelerating digital transformation are essential policy priorities for improving health system performance and healthcare resilience in Central Africa. The study also emphasizes the importance of coordinated regional cooperation for achieving sustainable and equitable healthcare development objectives.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Health System Performance in CEMAC: A Bayesian Analysis of Key Determinants
AU - Fleurine Paola Njanga Tsele
AU - Albert Ze
AU - Jean Tchitchoua
Y1 - 2026/06/10
PY - 2026
N1 - https://doi.org/10.11648/j.cajph.20261203.19
DO - 10.11648/j.cajph.20261203.19
T2 - Central African Journal of Public Health
JF - Central African Journal of Public Health
JO - Central African Journal of Public Health
SP - 201
EP - 215
PB - Science Publishing Group
SN - 2575-5781
UR - https://doi.org/10.11648/j.cajph.20261203.19
AB - This study examines the determinants of health system performance in the countries of the Economic and Monetary Community of Central Africa (CEMAC) over the period 2007–2021. The analysis focuses on Cameroon, Chad, Gabon, Equatorial Guinea, the Central African Republic, and the Republic of Congo. Health systems in the region continue to face major structural constraints characterized by insufficient financing, weak governance, shortages of qualified health personnel, unequal access to healthcare services, and limited technological integration. In this context, identifying the main determinants of health system performance remains essential for improving healthcare delivery and achieving sustainable development objectives. The study adopts a multidimensional framework integrating economic, social, institutional, and technological determinants. Methodologically, the research relies on an unbalanced panel dataset and employs three complementary econometric approaches: Bayesian Model Averaging (BMA), Weighted Average Least Squares (WALS), and General-to-Specific Modelling (GenSpec). The Bayesian Model Averaging approach is particularly relevant because it explicitly addresses model uncertainty and simultaneously evaluates multiple competing explanatory variables, thereby reducing omitted variable bias and strengthening the robustness of the empirical analysis. The findings reveal that GDP per capita, financial development, life expectancy, government health expenditure, and final government consumption expenditure positively influence health system performance in the CEMAC region. These variables contribute to improving healthcare financing, infrastructure development, access to medical technologies, and the efficiency of healthcare delivery. In contrast, corruption negatively affects health system performance by weakening governance quality and generating inefficient allocation of public resources. The robustness analysis further identifies political stability, internet access, education, and trade openness as important complementary determinants supporting healthcare modernization and resilience. This study contributes to the literature by providing one of the few empirical analyses specifically focused on health system performance in the CEMAC region while combining Bayesian and classical model selection approaches to strengthen the reliability of the findings. The results suggest that strengthening governance, increasing public investment in health, promoting anti-corruption reforms, and accelerating digital transformation are essential policy priorities for improving health system performance and healthcare resilience in Central Africa. The study also emphasizes the importance of coordinated regional cooperation for achieving sustainable and equitable healthcare development objectives.
VL - 12
IS - 3
ER -
Copy
|
Download