Intraoperative transesophageal echocardiography is used to more accurately assess a patient's cardiac condition and is important for the guidance of cardiac surgery. This case reports a pediatric cardiac surgery performed under TEE guidance in a patient with multiple complications. A 5-year-old child presented with diarrhea as the first symptom. At the age of 2 years, she was admitted to the hospital with ptosis of the right upper eyelid, morning lightness and evening heaviness, hand tremor, and the presence of a murmur in the mid to late stages of cardiac systole on auscultation. She was diagnosed with mitral valve prolapse and myasthenia gravis, which resolved with treatment. Subsequently, she was diagnosed with hyperthyroidism due to obvious protrusion of the eyeballs, and was admitted to the hospital for heart valve surgery after her thyroid function was controlled. Intraoperative TEE suggested mitral valve prolapse combined with embolization of the P2 region. In the complex case of this child, the suture points during mitral valvuloplasty and the scar tissue caused by the mitral valvuloplasty annulus may limit the growth of the annulus as well as the leaflet motion. Therefore, it was recommended that the surgeon perform mitral valve extension to maximize the prognosis. TEE herein guided the cardiac surgical decision making to maximize the prognosis of the child.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Mitral valve prolapse (MVP) is one of the most common cardiac valve diseases in pediatric patients, manifested mainly by prolapse of the mitral valve leaflet into the left atrium during ventricular systole. Hyperthyroidism is closely related to MVP, mainly in terms of immune and genetic susceptibility
[1]
Zhao CZ, Yan Y, et al. Sequential multidisciplinary minimally invasive therapeutic strategy for heart failure caused by four diseases: A case report. World J Clin Cases. 2022 Aug 16; 10(23): 8255-8261.
Antonelli A, Fallahi P, Elia G, et al. Graves' disease: Clinical manifestations, immune pathogenesis (cytokines and chemokines) and therapy. Best Pract Res Clin Endocrinol Metab. 2020; 34(1): 101388.
. In addition, autoantibodies, lymphocytes, cytokines, and chemokines may play an important role in the development of myasthenia gravis (MG) with hyperthyroidism, and genetic susceptibility is also an integral part
[3]
Lee SY, Pearce EN. Hyperthyroidism: A Review. JAMA 2023 Oct 17; 330(15): 1472-1483.
Vinciguerra M, Romiti S, et al. Mitral Plasticity: The Way to Prevent the Burden of Ischemic Mitral Regurgitation? Front Cardiovasc Med. 2022 Jan 4; 8: 794574.
A 5-year-old child, who underwent cardiac surgery for mitral valve prolapse, presented with concurrent hyperthyroidism and MG, as detailed in this report. The cooccurrence of these three diseases is extremely rare, and the association among those diseases has not been discussed in the previous literature. Written informed consent was obtained from the patient for the publication of this case report.
2. Case Presentation
A 5-year-old girl with a height of 108 cm and a weight of 13 kg, born at 38 weeks by cesarean section, weighing 2.65 kg at birth, breastfed for 1+ years, was admitted with right upper eyelid ptosis, hand tremors with shortness of breath after activity for 3+ years. At the age of 1 year, she was admitted with recurrent diarrhea after changing formula, and at the age of 2 years, she was found to have right upper eyelid ptosis with lightness in the morning and heaviness in the evening, hand tremors, and a heart murmur during mid to late systole on auscultation. Based on the symptoms, neostigmine test, and cardiac ultrasound, she was diagnosed with myasthenia gravis and mitral valve prolapse and then treated with prednisone and bromipyridamole, the dosage was gradually reduced until January 2021, when symptoms subsided. Later, she was diagnosed with hyperthyroidism due to significant bulging eyes and was treated with Sage when she was five, with moderate control of thyroid-related indicators. Notably, there was no family history of the thyroid disease. Then, the child was admitted to the hospital for further physical examination, which revealed a marked convexity of the eyes; the heart border was enlarged to the lower left, the heart rate was fast, the rhythm was uniform, and a systolic murmur was heard in the apical region. Laboratory tests showed that Thyroid Stimulating H (TSH) was <0.005, T3=3.37noml/L, and FT3=10.4pmol/L.
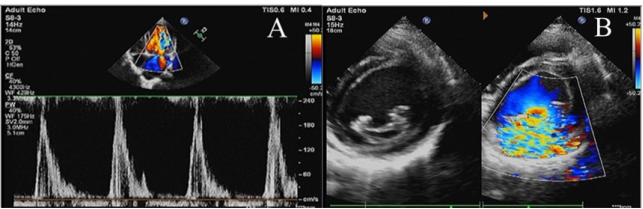
The preoperative transthoracic echocardiography (TTE) (Figure 1) suggested that the left heart was significantly enlarged. The mitral valve was slightly thickened, with slightly enhanced echogenicity. The -valve was open in diastole, but in systole, the A2 area of the anterior valve was prolapsed into the left atrium, resulting in misalignment of closure. Doppler test: mitral inflow acceleration Vmax=2.0m/s, supravalvular massive eccentric regurgitation; diagnostic opinion: Regurgitation secondary to mitral anterior valve prolapse.
Figure 1. Apical4-Chamber View (A4C) showed that the mitral inflow acceleration is 2m/s (A); Short axis view of the papillary muscle of left ventricle also showed that the mitral regurgitation is severe indicated by aliasing in color doppler (B).
3. TEE Guidance
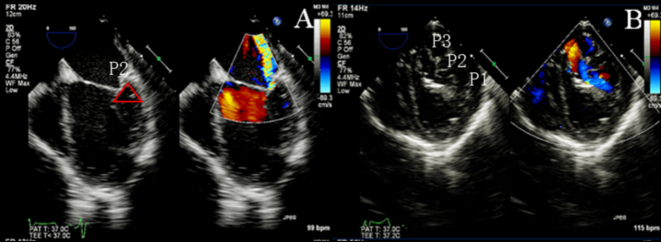
Preoperative transesophageal echocardiography (TEE) on Median Esophagus 4 Chamber (ME 4C) view showed severe eccentric mitral regurgitation with restricted motion in the P2 region and an enlarged triangle formed between P2 and the ventricular wall due to tethering of the triangle (Supplemental Material 1); the anterolateral papillary muscle was abnormal and extended towards the mitral valve (Figure 2A); The transgastric short-axis (TG SAX) view showed prolapse in the P2 and P3 regions (Figure 2B). Therefore, it is likely that the mitral regurgitation was caused by tethering of the P2 and P3 regions of the mitral valve, and TEE revealed abnormal proliferation of myofibroblasts in the anterolateral papillary muscle that had grown into the subvalvular mitral valve.
Based on TEE ultrasound results, proper growth of the annulus and leaflet movement can be restricted by taking into account scar tissue caused by suturing during mitral valvuloplasty and the annulus itself. Mitral valve lengthening is a better option
[5]
Lakew F, Sodah A, et al. Augmentation of the posterior mitral leaflet in secondary mitral valve insufficiency, mid-term results. Eur J Cardiothorac Surg. 2022 Oct 4; 62(5): ezac125.
Kakuta T, Fukushima S, et al. What Is the Optimal Mitral Valve Repair for Isolated Posterior Leaflet Prolapse to Achieve Long-Term Durability? J Am Heart Assoc. 2023 Jun 6; 12(11): e028607.
. The detailed procedure was described as follows: after extracorporeal circulation, the right atrium and septum were incised; the posterior mitral valve and some of the secondary tendons were incised, and the posterior mitral valve was extended using autologous pericardium; one artificial tendon was employed and sutured distally to the papillary muscle and proximally to the prolapsed vavle to shape the mitral valve. The post-operative period was uneventful and the patient was discharged in 5 days.
Figure 2. A: ME 4C without Doppler blood flow showed that the triangle formed by the P2 region and the left ventricular wall becomes larger indicated by the red triangle; ME 4C with Doppler blood flow shows that mitral eccentric regurgitation indicated by aliasing in color doppler; B: TG SAX showed that P1, P2, and P3 regions of the mitral valve.
4. Discussion
Mitral valve prolapse is one of the most common cardiac valve diseases in pediatric patients and is mainly manifested by prolapse of the mitral valve leaflet into the left atrium during ventricular systole
[7]
Essayagh B, Sabbag A, et al. Arrhythmic mitral valve prolapse and mitral annular disjunction: pathophysiology, risk stratification, and management. Eur Heart J. 2023 Sep 1; 44(33): 3121-3135.
Ronco D, Buttiglione G, et al. Biology of mitral valve prolapse: from general mechanisms to advanced molecular patterns-a narrative review. Front Cardiovasc Med. 2023 Jun 2; 10: 1128195.
. However, children primarily present with posterior mitral leaflet tethering as well as the abnormal proliferation of the anterolateral papillary muscle. The mitral leaflets are divided into three main layers: the atrial side elastin, the intermediate layer of spongy tissue, and the ventricular side fibrous layer
[9]
Atoui R, de Varennes B. Repair of chronic ischemic mitral regurgitation with posterior leaflet extension. Eur J Cardiothorac Surg. 2010; 38(4): 510-511.
. The fibrous layer on the ventricular side as well as the myofibers of the left ventricular wall constitute the triangular region of the tethering, which may be associated with increased fibrin. In the case, the anterolateral papillary muscle had extended below the posterior mitral valve, indicating the abnormal growth of the anterolateral mitral papillary muscle may also be associated with increased fibrin. In addition, the child had a combination of hyperthyroidism and myasthenia gravis, which are closely related in terms of autoimmunity and genetic susceptibility
In the case, the child was not diagnosed with hyperthyroidism at an early stage due to a lack of thyroid function tests. Hyperthyroidism can be congenital, secondary to MG as well as mitral valve problems. The superimposed effect of the three disorders led to ventricular remodeling in the child with thickening of the anterior mitral valve and tethering of the posterior mitral leaflet. Pediatric mitral valve prolapse, unlike adults, is reversible to some extent. This may be related to left ventricular remodeling after control of hyperthyroidism
[11]
Griffith E, Nunlist E. Mitral valve prolapse in adolescent female with hyperthyroidism. Prog Pediatr Cardiol. 2020 Sep; 58: 101264.
. However, in the present case, the child presented with mitral valve leaflet tethering, surgical treatment might be more effective, compared to mitral annuloplasty. Satisfactory outcomes and improved quality of life were achieved during the follow-up period of hospitalization.
TTE is an important tool in the diagnosis of mitral valve prolapse, and transesophageal echocardiography is essential to further clarify the diagnosis as well as to guide the surgical procedure. In accordance with the preoperative ultrasound, mitral annuloplasty was proposed. However, TTE can be limited in diagnosis by patient position and gas interference. TTE cannot monitor the patient's cardiac activity dynamically like TEE because of the time limitation of the examination
[12]
Marchetti D, Di Lenarda F, et al. Contemporary Echocardiographic Evaluation of Mitral Regurgitation and Guidance for Percutaneous Mitral Valve Repair. J Clin Med. 2023 Nov 15; 12(22): 7121.
After TEE evaluation, posterior mitral motion restriction was found. Further observation revealed the presence of tethering in the posterior mitral triangle, which was the main cause of posterior mitral motion restriction. Continued follow-up revealed the extent of tethering on the short axis of the left ventricle, originating from P2 involving P3. In addition, there was significant growth in the length of the anterolateral papillary muscle, which had grown into the subvalvular mitral valve. This condition not only interferes with mitral valve closure but also allows turbulent subvalvular flow, which may be a cause of anterior mitral valve thickening and posterior mitral valve tethering. At this point, mitral valvuloplasty alone is not sufficient and mitral valve extension may be a better option. After effective communication with the surgeon, the surgeon decided to change the surgical approach to mitral valve lengthening.
Mitral annuloplasty is indicated for mitral stenosis or mitral regurgitation due to altered annular diameter from various causes, and surgical intervention is performed to restore normal annular diameter for therapeutic purposes
[13]
Schulte LJ, Melby SJ. Mitral annuloplasty ring design and selection: Flexible bands are (mostly) all you need. J Thorac Cardiovasc Surg. 2023 Jul; 166(1): 88-90.
. In the case, the main manifestation was mitral regurgitation due to mitral leaflet tethering, and mitral valvuloplasty only addresses the enlarged annulus and does not address the patient's limited posterior mitral valve motion. Therefore, mitral leaflet extension may be a better option. Mitral leaflet extension is a complementary technique that can be used to correct leaflet tissue deficiencies and allow proper leaflet alignment. Patients with recurrent mitral valve insufficiency after mitral valvuloplasty alone have some degree of exacerbation of posterior leaflet tethering. In these patients, anterior leaflet tethering improved significantly and remained stable, posterior leaflet tethering worsened, and more importantly, progressive posterior leaflet tethering was associated with recurrent mitral regurgitation after mitral valvuloplasty. Consequently, mitral regurgitation will be improved to a greater extent by extension of the posterior mitral valve
[14]
de Varennes B, Chaturvedi R, et al. Initial results of posterior leaflet extension for severe type IIIb ischemic mitral regurgitation. Circulation. 2009; 119(21): 2837-2843.
Biondi R, Ribeyrolles S, et al. Mapping of the myxomatous mitral valve: The three-dimensional extension of mitral annular disjunction in surgically repaired mitral prolapse. Front Cardiovasc Med. 2022 Nov 29; 9: 1036400.
The case highlights the need for thyroid-related laboratory tests in patients with autoimmune diseases, the possible co-occurrence of MVP should also be considered when a patient has heart-related symptoms. The combination of TTE and TEE may clarify the diagnosis and provide clinical decision-making surgery with an early diagnosis of hyperthyroidism and early treatment. Long-term follow-up is required for unexplained posterior mitral leaflet tethering and anterolateral papillary muscle abnormalities.
Abbreviations
MG: Myasthenia Gravis
MVP: Mitral Valve Prolapse
TSH: Thyroid Stimulating H
TTE: Transthoracic Echocardiography
A4C: Apical4-Chamber View
TEE: transesophageal Echocardiography
ME 4C: Median Esophagus 4 Chamber
TG SAX: The Transgastric Short-Axis
Author Contributions
Guowei Wu: Collecting the case, Editing images, and writing the article
Hongwei Xu: Acquiring TEE images and modifying the article
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Zhao CZ, Yan Y, et al. Sequential multidisciplinary minimally invasive therapeutic strategy for heart failure caused by four diseases: A case report. World J Clin Cases. 2022 Aug 16; 10(23): 8255-8261.
Antonelli A, Fallahi P, Elia G, et al. Graves' disease: Clinical manifestations, immune pathogenesis (cytokines and chemokines) and therapy. Best Pract Res Clin Endocrinol Metab. 2020; 34(1): 101388.
Vinciguerra M, Romiti S, et al. Mitral Plasticity: The Way to Prevent the Burden of Ischemic Mitral Regurgitation? Front Cardiovasc Med. 2022 Jan 4; 8: 794574.
Lakew F, Sodah A, et al. Augmentation of the posterior mitral leaflet in secondary mitral valve insufficiency, mid-term results. Eur J Cardiothorac Surg. 2022 Oct 4; 62(5): ezac125.
Kakuta T, Fukushima S, et al. What Is the Optimal Mitral Valve Repair for Isolated Posterior Leaflet Prolapse to Achieve Long-Term Durability? J Am Heart Assoc. 2023 Jun 6; 12(11): e028607.
Ronco D, Buttiglione G, et al. Biology of mitral valve prolapse: from general mechanisms to advanced molecular patterns-a narrative review. Front Cardiovasc Med. 2023 Jun 2; 10: 1128195.
Marchetti D, Di Lenarda F, et al. Contemporary Echocardiographic Evaluation of Mitral Regurgitation and Guidance for Percutaneous Mitral Valve Repair. J Clin Med. 2023 Nov 15; 12(22): 7121.
Schulte LJ, Melby SJ. Mitral annuloplasty ring design and selection: Flexible bands are (mostly) all you need. J Thorac Cardiovasc Surg. 2023 Jul; 166(1): 88-90.
de Varennes B, Chaturvedi R, et al. Initial results of posterior leaflet extension for severe type IIIb ischemic mitral regurgitation. Circulation. 2009; 119(21): 2837-2843.
Biondi R, Ribeyrolles S, et al. Mapping of the myxomatous mitral valve: The three-dimensional extension of mitral annular disjunction in surgically repaired mitral prolapse. Front Cardiovasc Med. 2022 Nov 29; 9: 1036400.
Wu, G., Xu, H. (2024). TEE-Guided Cardiac Surgery in a Child with Mitral Valve Prolapse, Hyperthyroidism and Myasthenia Gravis: A Case Report. Cardiology and Cardiovascular Research, 8(2), 51-55. https://doi.org/10.11648/j.ccr.20240802.11
Wu, G.; Xu, H. TEE-Guided Cardiac Surgery in a Child with Mitral Valve Prolapse, Hyperthyroidism and Myasthenia Gravis: A Case Report. Cardiol. Cardiovasc. Res.2024, 8(2), 51-55. doi: 10.11648/j.ccr.20240802.11
Wu G, Xu H. TEE-Guided Cardiac Surgery in a Child with Mitral Valve Prolapse, Hyperthyroidism and Myasthenia Gravis: A Case Report. Cardiol Cardiovasc Res. 2024;8(2):51-55. doi: 10.11648/j.ccr.20240802.11
@article{10.11648/j.ccr.20240802.11,
author = {Guowei Wu and Hongwei Xu},
title = {TEE-Guided Cardiac Surgery in a Child with Mitral Valve Prolapse, Hyperthyroidism and Myasthenia Gravis: A Case Report
},
journal = {Cardiology and Cardiovascular Research},
volume = {8},
number = {2},
pages = {51-55},
doi = {10.11648/j.ccr.20240802.11},
url = {https://doi.org/10.11648/j.ccr.20240802.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20240802.11},
abstract = {Intraoperative transesophageal echocardiography is used to more accurately assess a patient's cardiac condition and is important for the guidance of cardiac surgery. This case reports a pediatric cardiac surgery performed under TEE guidance in a patient with multiple complications. A 5-year-old child presented with diarrhea as the first symptom. At the age of 2 years, she was admitted to the hospital with ptosis of the right upper eyelid, morning lightness and evening heaviness, hand tremor, and the presence of a murmur in the mid to late stages of cardiac systole on auscultation. She was diagnosed with mitral valve prolapse and myasthenia gravis, which resolved with treatment. Subsequently, she was diagnosed with hyperthyroidism due to obvious protrusion of the eyeballs, and was admitted to the hospital for heart valve surgery after her thyroid function was controlled. Intraoperative TEE suggested mitral valve prolapse combined with embolization of the P2 region. In the complex case of this child, the suture points during mitral valvuloplasty and the scar tissue caused by the mitral valvuloplasty annulus may limit the growth of the annulus as well as the leaflet motion. Therefore, it was recommended that the surgeon perform mitral valve extension to maximize the prognosis. TEE herein guided the cardiac surgical decision making to maximize the prognosis of the child.
},
year = {2024}
}
TY - JOUR
T1 - TEE-Guided Cardiac Surgery in a Child with Mitral Valve Prolapse, Hyperthyroidism and Myasthenia Gravis: A Case Report
AU - Guowei Wu
AU - Hongwei Xu
Y1 - 2024/04/11
PY - 2024
N1 - https://doi.org/10.11648/j.ccr.20240802.11
DO - 10.11648/j.ccr.20240802.11
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 51
EP - 55
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20240802.11
AB - Intraoperative transesophageal echocardiography is used to more accurately assess a patient's cardiac condition and is important for the guidance of cardiac surgery. This case reports a pediatric cardiac surgery performed under TEE guidance in a patient with multiple complications. A 5-year-old child presented with diarrhea as the first symptom. At the age of 2 years, she was admitted to the hospital with ptosis of the right upper eyelid, morning lightness and evening heaviness, hand tremor, and the presence of a murmur in the mid to late stages of cardiac systole on auscultation. She was diagnosed with mitral valve prolapse and myasthenia gravis, which resolved with treatment. Subsequently, she was diagnosed with hyperthyroidism due to obvious protrusion of the eyeballs, and was admitted to the hospital for heart valve surgery after her thyroid function was controlled. Intraoperative TEE suggested mitral valve prolapse combined with embolization of the P2 region. In the complex case of this child, the suture points during mitral valvuloplasty and the scar tissue caused by the mitral valvuloplasty annulus may limit the growth of the annulus as well as the leaflet motion. Therefore, it was recommended that the surgeon perform mitral valve extension to maximize the prognosis. TEE herein guided the cardiac surgical decision making to maximize the prognosis of the child.
VL - 8
IS - 2
ER -
Wu, G., Xu, H. (2024). TEE-Guided Cardiac Surgery in a Child with Mitral Valve Prolapse, Hyperthyroidism and Myasthenia Gravis: A Case Report. Cardiology and Cardiovascular Research, 8(2), 51-55. https://doi.org/10.11648/j.ccr.20240802.11
Wu, G.; Xu, H. TEE-Guided Cardiac Surgery in a Child with Mitral Valve Prolapse, Hyperthyroidism and Myasthenia Gravis: A Case Report. Cardiol. Cardiovasc. Res.2024, 8(2), 51-55. doi: 10.11648/j.ccr.20240802.11
Wu G, Xu H. TEE-Guided Cardiac Surgery in a Child with Mitral Valve Prolapse, Hyperthyroidism and Myasthenia Gravis: A Case Report. Cardiol Cardiovasc Res. 2024;8(2):51-55. doi: 10.11648/j.ccr.20240802.11
@article{10.11648/j.ccr.20240802.11,
author = {Guowei Wu and Hongwei Xu},
title = {TEE-Guided Cardiac Surgery in a Child with Mitral Valve Prolapse, Hyperthyroidism and Myasthenia Gravis: A Case Report
},
journal = {Cardiology and Cardiovascular Research},
volume = {8},
number = {2},
pages = {51-55},
doi = {10.11648/j.ccr.20240802.11},
url = {https://doi.org/10.11648/j.ccr.20240802.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20240802.11},
abstract = {Intraoperative transesophageal echocardiography is used to more accurately assess a patient's cardiac condition and is important for the guidance of cardiac surgery. This case reports a pediatric cardiac surgery performed under TEE guidance in a patient with multiple complications. A 5-year-old child presented with diarrhea as the first symptom. At the age of 2 years, she was admitted to the hospital with ptosis of the right upper eyelid, morning lightness and evening heaviness, hand tremor, and the presence of a murmur in the mid to late stages of cardiac systole on auscultation. She was diagnosed with mitral valve prolapse and myasthenia gravis, which resolved with treatment. Subsequently, she was diagnosed with hyperthyroidism due to obvious protrusion of the eyeballs, and was admitted to the hospital for heart valve surgery after her thyroid function was controlled. Intraoperative TEE suggested mitral valve prolapse combined with embolization of the P2 region. In the complex case of this child, the suture points during mitral valvuloplasty and the scar tissue caused by the mitral valvuloplasty annulus may limit the growth of the annulus as well as the leaflet motion. Therefore, it was recommended that the surgeon perform mitral valve extension to maximize the prognosis. TEE herein guided the cardiac surgical decision making to maximize the prognosis of the child.
},
year = {2024}
}
TY - JOUR
T1 - TEE-Guided Cardiac Surgery in a Child with Mitral Valve Prolapse, Hyperthyroidism and Myasthenia Gravis: A Case Report
AU - Guowei Wu
AU - Hongwei Xu
Y1 - 2024/04/11
PY - 2024
N1 - https://doi.org/10.11648/j.ccr.20240802.11
DO - 10.11648/j.ccr.20240802.11
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 51
EP - 55
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20240802.11
AB - Intraoperative transesophageal echocardiography is used to more accurately assess a patient's cardiac condition and is important for the guidance of cardiac surgery. This case reports a pediatric cardiac surgery performed under TEE guidance in a patient with multiple complications. A 5-year-old child presented with diarrhea as the first symptom. At the age of 2 years, she was admitted to the hospital with ptosis of the right upper eyelid, morning lightness and evening heaviness, hand tremor, and the presence of a murmur in the mid to late stages of cardiac systole on auscultation. She was diagnosed with mitral valve prolapse and myasthenia gravis, which resolved with treatment. Subsequently, she was diagnosed with hyperthyroidism due to obvious protrusion of the eyeballs, and was admitted to the hospital for heart valve surgery after her thyroid function was controlled. Intraoperative TEE suggested mitral valve prolapse combined with embolization of the P2 region. In the complex case of this child, the suture points during mitral valvuloplasty and the scar tissue caused by the mitral valvuloplasty annulus may limit the growth of the annulus as well as the leaflet motion. Therefore, it was recommended that the surgeon perform mitral valve extension to maximize the prognosis. TEE herein guided the cardiac surgical decision making to maximize the prognosis of the child.
VL - 8
IS - 2
ER -