The objectives of this study were to assess the prevalence of anemia in patients with heart failure, analyze the characteristics of anemia in this population, and identify prognostic factors related to anemia and heart failure. We conducted a descriptive and analytical retrospective study over a period of nine months, from April 1, 2018, to December 31, 2018. The study included patients aged over 18 years who were hospitalized in a cardiology department for heart failure of all causes, with hemoglobin levels strictly below 12 g/dl for women and 13 g/dl for men. Heart failure diagnosis was based on ESC 2016 criteria. The study was approved by the ethics committee of Cheikh Anta Diop University, Dakar. Data analysis was performed using SPSS 18 (Statistical Package for Social Sciences version 18), with a p-value of ≤ 0.05 considered statistically significant. We identified 182 patients with anemia, representing a hospital prevalence of 11.61%. The average age was 58.9 ± 15.93 years, with a female predominance in those under 50 years and a male predominance in those over 50. Most patients (77.1%) had a low socioeconomic status. Major cardiovascular risk factors included physical inactivity (56%) and hypertension (47%). Clinically, 78% of patients had dyspnea, 31.9% had chest pain, 40.7% had cutaneous-mucosal pallor, and 72.2% had global heart failure. Ischemic heart disease was the main cause of heart failure (49.2%). Diagnostic investigations revealed elevated ferritin in 50% of cases, elevated CRP in 88.1%, and elevated creatinine in 37.4%. The mean hemoglobin level was 11.6 ± 7.15 g/dl, with 71.4% of patients having hemoglobin between 10 and 13 g/dl. Normocytic normochromic anemia predominated. The study showed that anemia was more common in patients with an ejection fraction > 50% (48.1%) and those with global heart failure (72.2%). Statistically significant associations with severe and mild anemia were observed in the age groups 20-29 years (p=0.003) and 50-59 years (p=0.014) and with endocarditis (p=0.03). Only women showed severe and very severe anemia (p=0.21). The hospital mortality rate was 15.38%. In conclusion, this study reveals a significant prevalence of anemia among hospitalized patients, with important correlations between anemia and various clinical and socioeconomic factors.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
According to the World Health Organization (WHO), anemia is defined as a decrease in hemoglobin concentration below the reference values based on age, sex, and physiological state of individuals
[1]
Abrahams OG, Eklund DL, Kohrs MB, O’neal RM. The incidence of anemia in residents of Missouri. Am J Clin Nutr 1976; 29: 1158-66.
. It is characterized by a hemoglobin concentration below 13g/dl in adult men, 12g/dl in non-menopausal women, and 14g/dl in newborns
[2]
Al-Ahmad A, Rand WM, Manjunath G et al. Reduced kidney function and anemia as risk factors for mortality in patients with left ventricular dysfunction. J Am Coll Cardiol 2001; 38: 955-62.
EzekowitzJA, Mc Alister FA, Armstrong PW. Anaemia is common in heart failure and is associated with poor outcomes: insights from a cohort of 12,065 patients with a new-onset heart failure. Circulation 2003; 107: 223-5.
. It is common among people over 65 years old living in the community, with an estimated prevalence of 11% in men and 10.2% in women. Beyond 85 years of age, its prevalence exceeds 20%
[7]
Guralnik JM, Eisenstaedt RS, Ferrucci L, Klein HG, Woodman RC. Prevalence of anemia in persons 65 years and older in the United States: Evidence for a high rate of unexplained anemia. Blood 2004; 104: 2263-8.
. It also raises other concerns regarding its prevalence and impact among individuals with heart disease, as anemia is associated with an increased risk of cardiovascular diseases. Anemia has been recognized as a risk factor for ischemic heart disease (IHD)
[10]
Shulman LN, Braunwald E, Rosenthal DS. Hematological-oncological disorders and heart disease. In: Braunwald E. Heart Disease: A Textbook of Cardiovascular Medicine. 5th edn. Phildadelphia: WB Saunders, 1997: 1786±808.
[10]
. The role of reduced oxygenation due to decreased hemoglobin and hematocrit on myocardial performance has also been studied, particularly at the physiological level
[10]
Shulman LN, Braunwald E, Rosenthal DS. Hematological-oncological disorders and heart disease. In: Braunwald E. Heart Disease: A Textbook of Cardiovascular Medicine. 5th edn. Phildadelphia: WB Saunders, 1997: 1786±808.
[11]
Brannon ES, Merrill AJ, Warren JV, Stead EA. The cardiac output in patients with chronic anemia as measured by the technique of right atrial catheterization. J Clin Invest 1945; 24: 332.
. However, the precise impact of anemia on the clinical presentation of IHD, such as manifestations, severity, and complications, has been scarcely studied.
In another study conducted among 417 Israeli patients with ischemic heart disease, Zeidman et al. (2004) reported greater disease severity in anemic patients (80%) compared to non-anemic patients. Consequently, mortality was also higher in the anemic group (18%) compared to the non-anemic group (4%)
[12]
Zeidman A, fradin Z, Blecher A, Oster HS, Avrahami Y, Mittelman M. Anemia as arisk factor for ischemic heart disease. Isr Med Assoc J. 2004; 6(1): 16-8. PMID: 14740503
[12]
.
In Senegal, the prevalence of anemia among individuals with heart disease has been minimally studied. Therefore, we initiated this study among patients hospitalized in the cardiology department of Idrissa Pouye General Hospital (HOGIP). The objectives of this study were to evaluate the prevalence of anemia in heart failure patients, analyze the characteristics of anemia in this population, and identify prognostic factors of anemia in heart failure.
2. Methodology
This was a descriptive and analytical study with retrospective data collection. The study was conducted over a 9-month period from April 1, 2018, to December 31, 2018. Included in the study were patients aged at least 18 years, who were hospitalized in the cardiology department of Idrissa Pouye General Hospital during the study period for heart failure of any cause, and had a hemoglobin level strictly below 12 g/dl in women and strictly below 13 g/dl in men. The diagnosis of heart failure was based on the ESC 2016 criteria.
We studied socio-demographic aspects, cardiovascular risk factors, clinical, paraclinical, therapeutic, and evolutionary data. The duration of hospitalization was expressed in days. These various parameters were collected using a questionnaire and recorded on a data collection sheet. The survey form was validated by an expert committee consisting of two cardiologists, a hematologist, and an epidemiologist, each with at least 4 years of experience. This work was carried out in collaboration with the hospital management after obtaining approval from the cardiology department by signing the access form to the patients' records. It was also approved by the ethics committee of Cheikh Anta Diop University in Dakar.
Data were entered using Sphinx software version 5.1.0.2. The analysis was performed using SPSS 18 software (Statistical Package for Social Sciences version 18). The descriptive study involved calculating frequencies and proportions for qualitative variables and calculating means and standard deviations for quantitative variables. The analytical study was conducted using cross-tabulations. To compare frequencies, we used Pearson's chi-square test or Fisher's exact bilateral test according to their applicability conditions. The comparison of means was made using the analysis of variance test with a significance threshold of p < 0.05.
3. Results
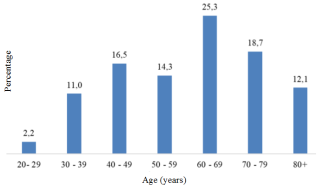
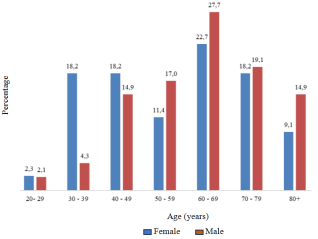
During our study period, we identified 182 patients with anemia from all causes, representing a hospital prevalence of 11.61%. The average age of the patients was 58.9 ± 15.93 years, with extremes ranging from 20 to 89 years. The most represented age group was 60 to 69 years (25.3%) (Figure 1). Our study population showed a slight male predominance with a male-to-female ratio of 1.07. The distribution of patients by age and gender shows a clear female predominance among patients under 50 years old with a sex ratio of 0.55. However, the predominance became male beyond 50 years old with a sex ratio of 1.28 (Figure 2).
Figure 2. Distribution of Patients by Age and Gender (n=182).
The majority of patients resided in urban areas (54%), 30% in rural areas, and 16% in semi-urban areas. Most patients were unemployed, accounting for 58.2%. More than half of the patients (77.1%) had a low socioeconomic status (Table 1).
Table 1. Demographic and Clinical Characteristics of Patients.
Variable
Value
Total number of patients
182
Mean age (years)
58.9 ± 15.9
Most represented age group
60-69 years (25.3%)
Male/female ratio
1.07
Urban residence (%)
54
Rural & semi-urban residence
46
Illiterate (%)
59
Unemployed (%)
58.2
Low socioeconomoic status (%)
77.1
Regarding medical history, 29.7% of patients had a history of heart disease, with 30% having valvular heart disease and 26% ischemic heart disease. Cardiovascular risk factors were dominated by physical inactivity (56%) and hypertension (47%), dyslipidemia (13%), diabetes (12%), and smoking (8%) (Table 2).
Table 2. Medical History and Risk Factors.
Variable
Value (%)
Cardiopathies
29.7
Valvulopathies
30
Ischemic heart disease
26
Sedentary lifestyle
56
Hypertension (HTN)
47
Dyslipidemia
13
Diabetes
12
Tabacco
8
Clinically, the most common symptoms were dyspnea (78%), with a significant proportion of patients in stage III (49.3%) and IV (43.7%) according to the NYHA classification. Additionally, 34.1% had lower limb edema and 31.9% experienced chest pain. A cutaneous-mucosal pallor was observed in 40.7% of the patients. Physical examination revealed global heart failure in 72.2% of patients, left heart failure in 15.3%, and right heart failure in 12.5% (Table 3).
Table 3. Clinical Signs and Physical Examinations.
Variable
Value %
Dyspnea
78
NYHA Stage III
49.3
NYHA Stage IV
43.7
Lower limb sdema
34.1
Chest pain
31.9
Global heart failure
72.2
Left heart failure
15.3
Right heart failure
12.5
Regarding diagnostic investigations, iron studies could not be performed. Ferritin levels were elevated in 50% of cases. C-reactive protein (CRP) was elevated in 88.1% of our patients. The mean creatinine level was 13.04 ± 9.4 g/l, and 37.4% of patients had a creatinine level above 11.3 mg/l (Table 4).
Table 4. Diagnostic Investigations.
Variable
Value
Elevated ferritin
50%
Elevated C-Reactive
88.1%
Mean creatinine (g)
13.04 ± 9.4
Creatinine > 11.3 mg/l
37.4%
Hyperkalimia > 4,5 mmol/l
33 %
Hypokalimia < 3,5 mmol/l
8.9 %
Hyponatrimia < 135 mmol/l
41.8%
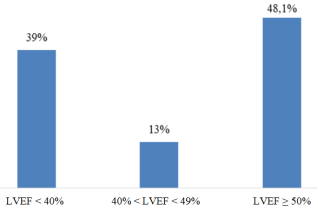
Electrocardiogram anomalies were dominated by repolarization disorders (45.1%), conduction disorders (25.3%), rhythm disorders (25.3%), and necrosis sequelae (19.8%) (Table 5). Radiological signs were dominated by cardiomegaly (79.2%) and interstitial and alveolar infiltrates (37.4%). Echocardiography showed a left ventricular ejection fraction (LVEF) below 50% in 51.9% (Figure 3).
Figure 3. Distribution of Patients by LVEF (n=182).
The causes of heart failure were dominated by ischemic heart disease (49.2%), followed by dilated cardiomyopathies (17.6%), valvular heart diseases (13.2%), and rhythm disturbances (12.1%) (Table 6).
Table 6. Causes of Heart Failure.
Variable
Value
Ischemic cardiomyopaties
42.9
Dilated cardiomyopathies
17.6
Valvulopathies
13.2
Rhythmic cardiomyopathies
12.1
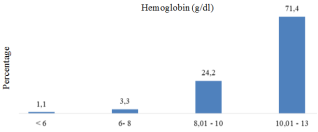
The average hemoglobin level in the study population was 11.6 ± 7.15 g/dl, with an average of 10.5 ± 1.6 g/dl in women and 11.02 ± 1.26 g/dl in men. It was noted that 71.4% of patients had hemoglobin levels between 10 g/dl and 13 g/dl, and 1.1% had hemoglobin levels below 6 g/dl (Figure 4). Normocytic anemia represented 54.9% of cases, while microcytic anemia represented 44%. According to the mean corpuscular hemoglobin concentration (MCHC), normochromic anemia predominated (81.1%), followed by hypochromic anemia (18.9%). In terms of anemia type, 47.3% of cases were normochromic normocytic, 33% normochromic microcytic, and 11% hypochromic microcytic. Anemia was severe in 1.1% of cases, moderate in 20.9% of cases, and mild in 73.6% of cases. (Table 7)
Figure 4. Distribution of Patients by Hemoglobin Level (n=182).
Table 7. Anemia Characteristics.
Variable
Value (%)
Cutaneomucous pallor
40.7
Mean hemoglobin (g/dl)
11.6 +- 7.15
Mean hemoglobin (females)
10.5 +- 1.6
Mean hemoglobin (males)
11.02 +- 1.26
Hb between 10 and 13 g/dl
71.4
Hb inf 6 g/dl
1.1
Normocytic anemia
54.9
Microcytic anemia
44
Normochromic anemia
81.1
Hypochromic anemia
18.9
Normochromic normocytic anemia
47.3
Normochromic microcytic anemia
33
Hypochromic microcytic anemia
11
Severe anemia
1.1
Moderate anemia
20.9
Mild anemia
73.3
During hospitalization, 5.5% of patients were treated with iron and 5.5% received blood transfusions. The remaining treatments generally concerned heart failure and the underlying pathology. The outcome was marked by persistent anemia in 58.7% of patients, regression in 17.4%, and correction in 23.9%. It was also marked by persistent signs of right heart failure in 13.8% of cases and left heart failure in 7.6%. Cardiovascular complications observed included atrial fibrillation (6.6%), cardiovascular collapse (3.3%), cardiorespiratory arrest (3.3%), and thromboembolic events (2.2%). Finally, deaths were noted in 15.38% of cases (Table 8).
Table 8. Treatments and Outcomes.
Variable
Value (%)
Iron treatmant
5.5
Blood transfusion
5.5
Persistence of anemia
58.7
Regression of anemia
17.4
Correction of anemia
23.9
Death
15.38
Regarding the global analysis of anemia distribution, the study shows that anemia was more frequent in patients with an LVEF > 50% (48.1%) compared to those with an LVEF < 40% (39%). Additionally, it was more present in patients with global heart failure (72.2%) compared to those with right heart failure (12.5%) and left heart failure (15.3%).
A statistically significant association between severe and mild anemia was observed in the age group 20-29 years (p=0.003), representing 2.2% of the study population, and the age group 50-59 years (p=0.014). Furthermore, only women had severe and severe anemia, although without statistical significance (p=0.21). There was no statistically significant difference between the severity of anemia and profession or education level. Finally, a statistically significant relationship was found between anemia and endocarditis (p=0.03).
4. Discussion
The hospital prevalence of anemia in our study was 11.61%, indicating a significant frequency of this condition among hospitalized patients. The prevalence of anemia in the literature is highly variable, ranging from 4% to 61%, with most studies placing it around 18% to 20%
[13]
Tang Y, Katz SD. Anemia in chronic heart failure: prevalence, etiology, clinical correlates, and treatment options. Circulation 2006; 113: 2454-61.
[14]
Tang WH, Tong W, Francis GS, et al. Evaluation and long-term prognosisof new onset transient and persistent anaemia in ambulatory patients withchronic heart failure. J Am Coll Cardiol 2008; 51(5): 569-76.
. Comparisons remain difficult due to varying definitions.
The average age of patients was 58.9 years, similar to the study conducted in Koudougou in 2022
[15]
J. K Kologo1, G. R. C Millogo, Y Kambiré, H Adoko, L. J Kagambéga, A Thiam/Tall1, N. V Yaméogo et al. Heart failure and anemia in the cardiology department of the Yalgado Ouedraogo university teaching Hospital: epidemiology, management and prognosis. Health Sci. Dis, 2022; 23(2): 143-7.
, whereas Zeidman's study on patients meeting the criteria for both ischemic heart disease (IHD) and anemia found an average age of 76.1 ± 4.2 years
[12]
Zeidman A, fradin Z, Blecher A, Oster HS, Avrahami Y, Mittelman M. Anemia as arisk factor for ischemic heart disease. Isr Med Assoc J. 2004; 6(1): 16-8. PMID: 14740503
[12]
. This average age was also lower than in the EuroHeart Failure Survey (71 years)
[16]
Cleland JGF, Swedberg K, Cohen-Solal A et al. The Euroheart failure survey programme - a survey on the quality of care among patients with heart failure in Europe. EuropeanHeart Journal 2003; 24: 442-63.
The slight male predominance with a male-to-female ratio of 1.07 is consistent with trends observed in other similar studies, although this predominance reverses in patients under 50, suggesting variations linked to hormonal factors or gender-specific comorbidities. However, the Euro Heart Survey found a female predominance with a prevalence of 18% for men and 23% for women
[16]
Cleland JGF, Swedberg K, Cohen-Solal A et al. The Euroheart failure survey programme - a survey on the quality of care among patients with heart failure in Europe. EuropeanHeart Journal 2003; 24: 442-63.
The majority of patients resided in urban areas (54%), while 30% lived in rural areas and 16% in semi-urban areas. This distribution reflects a geographical diversity that can influence access to care and the prevalence of anemia. The high proportion of unschooled (59%) and unemployed (58.2%) patients highlights the potential link between low socioeconomic status and the prevalence of anemia. More than half of the patients had a low socioeconomic status (77.1%), which may contribute to poorer nutrition and limited access to healthcare.
A history of heart disease was present in 29.7% of patients, with notable prevalences of valvular heart disease (30%) and ischemic heart disease (26%). Cardiovascular risk factors were dominated by physical inactivity (56%) and hypertension (47%), underscoring the importance of healthy lifestyles in preventing anemia and cardiovascular diseases. Several other studies in adults have also reported that the risk of cardiovascular disease increases with decreased iron reserves
[18]
Klipstein-Grobusch K, Koster JF, Grobbee DE, et al. Serum ferritin and risk of myocardial infarction in the eÏderly: theRotterdam Study. Am J Clin Nutr 1999; 69(6): 1231-6.
Kurl S, Tuomainen T, Laukkanen JA, et al. Plasma vitamin C modifies the association between hypertension and risk ofstroke. Stroke. 2002; 33(6): 156-73.
Clinically, the prevalence of dyspnea (78%), lower limb edema (34.1%), and chest pain (31.9%) reflects the severity of heart failure in this population. The predominance of global heart failure (72.2%) underscores the severity of the cases encountered. These heart failure data differ from those found in Ouagadougou in 2022, where global heart failure represented 44.4%
[15]
J. K Kologo1, G. R. C Millogo, Y Kambiré, H Adoko, L. J Kagambéga, A Thiam/Tall1, N. V Yaméogo et al. Heart failure and anemia in the cardiology department of the Yalgado Ouedraogo university teaching Hospital: epidemiology, management and prognosis. Health Sci. Dis, 2022; 23(2): 143-7.
. Anemia, as well as ischemic heart disease (IHD) and systolic dysfunction, have been shown to be significant independent risk factors for recurrent congestive heart failure
[21]
Harnett JD, Foley RN, Kent GM, Barre PE, Murray D, Partrey PS. Congestive heart failure in dialysis patients: prevalence, incidence, prognosis and risk factors. Kidney Int 1995; 47: 884±90.
. However, unlike patients with myocardial diseases, anemic patients present with high cardiac output, low systemic vascular resistance, and low blood pressure
[22]
Anand IS, Chandrashekhar Y, Ferrari R, Poole-Wilson PE, Harris PS. Pathogenesis of oedema in chronic severe anemia: studies of body water and sodium, renal function, hemodynamic variables, and plasma hormones. Br Heart J 1993; 70: 357±62.
. Successful treatment of anemia is associated with significant improvement in functional class, cardiac and renal function, and a reduction in the need for diuretics and hospitalizations
[23]
Silverberg DS, Wexler D, Blum M, et al. The use of subcutaneous erythropoietin and intravenous iron for the treatment of the anemia of severe, resistant congestive heart failure improves cardiac and renal function and functional cardiac class, and markedly reduces hospitalization. J Am Coll Cardiol 2000; 35: 1737±44.
Diagnostic investigations were limited by the absence of a complete iron profile, although ferritin levels were elevated in 50% of patients, and CRP in 88.1%, indicating a significant inflammatory component. The mean creatinine level was 13.04 ± 9.4 g/l, with 37.4% of patients having a creatinine level above 11.3 mg/l, suggesting frequent renal impairment.
Electrocardiogram anomalies were mainly repolarization disorders (45.1%), conduction disorders (25.3%), rhythm disorders (25.3%), necrosis sequelae (19.8%), and left ventricular hypertrophy (LVH) (15.4%). These results differ from those observed in Lubumbashi, where rhythm disorders and LVH were the most common ECG anomalies
[24]
Lubange K. Etude épidémiologique et clinique de l'Insuffisance cardiaque. Thèse Med: Université de Lubumbashi 2013.
[24]
. Cardiomegaly (79.2%) and interstitial and alveolar infiltrates (37.4%) were the dominant radiological signs, reflecting the extent of cardiac damage. Echocardiography showed a left ventricular ejection fraction (LVEF) below 50% in 51.9% of patients, which is a crucial indicator of cardiac dysfunction. Our data are lower than those found in the Lubanga study, where LVEF was impaired in 57% of heart failure patients. However, in the Sentinel Network study, LVEF was impaired in 42% of cases
[25]
Saudubray T, Saudubray C, Viboud C et al. Prévalence et prise en charge de l’insuffisance cardiaque en France: enquête nationale auprès des médecins généralistes du réseau Sentinelles, Rev Méd Intern 200.
The causes of heart failure were mainly ischemic heart disease (42.9%), followed by dilated cardiomyopathies (17.6%), valvular heart diseases (13.2%), and rhythm disorders (12.1%). Sarnak et al. (2002) report a higher risk of cardiovascular disease in anemic individuals (RR=1.41; 95%CI=1.01-1.95) across the cohort
[26]
Sarnak MJ, Tighiouart H, Manjunath G, et al. Anernia as a risk factor for cardiovascular disease in The Atherosclerosis Risk inCommunities (ARIC) study. J Am CouCardiol 2002 Jul 3; 40(1): 27-33.
The mean hemoglobin level was 11.6 ± 7.15 g/dl, with slightly lower levels in women (10.5 ± 1.6 g/dl) than in men (11.02 ± 1.26 g/dl), whereas Zeidman's study group had a mean hemoglobin level of 8.9 ± 1.6 g/dl
[12]
Zeidman A, fradin Z, Blecher A, Oster HS, Avrahami Y, Mittelman M. Anemia as arisk factor for ischemic heart disease. Isr Med Assoc J. 2004; 6(1): 16-8. PMID: 14740503
[12]
. Normocytic anemia was the most common (54.9%), followed by microcytic anemia (44%). Most cases of anemia were mild (73.6%), moderate (20.9%), or severe (1.1%).
During hospitalization, 5.5% of patients were treated with iron and 5.5% received a blood transfusion. Treatments were mainly focused on heart failure and underlying pathologies. The outcome showed that anemia persisted in 58.7% of patients, regressed in 17.4%, and was corrected in 23.9%. Cardiovascular complications included atrial fibrillation (6.6%), cardiovascular collapse (3.3%), cardiorespiratory arrest (3.3%), and thromboembolic events (2.2%). The mortality rate was 15.38%.
The study has some limitations that hindered the precise determination of the etiology of anemia in the studied patients. The absence of iron studies prevented the assessment of iron stores, essential for distinguishing iron-deficiency anemia from other types of anemia. The lack of reticulocyte count hindered the evaluation of the bone marrow response to anemia, which is crucial for identifying the causes of regenerative and non-regenerative anemia. The lack of information on vitamin B12 levels limited the ability to diagnose megaloblastic anemia, often caused by vitamin B12 deficiency.
The study was conducted in a public hospital frequented mainly by a low socioeconomic status population. This situation could influence the results due to socioeconomic factors that can affect health and access to care, limiting the representativeness of the study's conclusions to a broader and more diverse population. Due to these limitations, the etiology of anemia remained undetermined in 86% of the study patients. These gaps highlight the need for more comprehensive data and a more holistic approach to improve the understanding and treatment of anemia in this population.
5. Conclusion
This study reveals a significant prevalence of anemia among hospitalized patients, with important correlations between anemia and various clinical and socio-economic factors. Limitations in diagnostic investigations highlight the need for a more comprehensive assessment and a holistic approach for a better understanding and management of anemia. The results underscore the importance of tailored prevention and treatment strategies to reduce the impact of anemia, particularly among vulnerable populations.
Abbreviations
HOGIP
Hospital General Idrissa Pouye
IHD
Ischemic Heart Disease
LVEF
Left Ventricular Ejection Fraction
LVH
Left Ventricular Hypertrophy
RR
Relative Risk
WHO
World Health Organization
Ethics Approval and Consent to Participate
This study was approved by the ethics committee of Cheikh Anta Diop University of Dakar and was carried out in collaboration with the hospital management after obtaining approval from the cardiology department by signing the access form to patient records.
Consent for Publication
Not Applicable.
Author Contributions
Ngone Diaba Gaye and Abdoul Kane designed the study protocol, participated in the data collection and writing of the draft manuscript.
Aliou Alassane Ngaide and Mouhamadou Bamba Ndiaye oversaw the execution of the study, participated in data analysis and critically revised the manuscript for important intellectual content.
Mamadou Lamine Diaby and Maboury Diao participated in study design and in data analysis.
Joseph Salvador Mingou and Alassane Mbaye participated in statistical analysis and interpretation of results.
Funding
The study did not receive any funding.
Data Availability Statement
The data and materials of this study are available upon request and ready to be shared. For further information, please contact the corresponding author, Aliou Alassane NGAIDE.
Conflicts of Interests
The authors declare no conflicts of interest.
References
[1]
Abrahams OG, Eklund DL, Kohrs MB, O’neal RM. The incidence of anemia in residents of Missouri. Am J Clin Nutr 1976; 29: 1158-66.
Al-Ahmad A, Rand WM, Manjunath G et al. Reduced kidney function and anemia as risk factors for mortality in patients with left ventricular dysfunction. J Am Coll Cardiol 2001; 38: 955-62.
EzekowitzJA, Mc Alister FA, Armstrong PW. Anaemia is common in heart failure and is associated with poor outcomes: insights from a cohort of 12,065 patients with a new-onset heart failure. Circulation 2003; 107: 223-5.
Thera MA. Nutritionalanaemias. Report of a WHO scientific group. World HealthOrgan Tech Rep Ser 1968; 405: 5-37. PMID: 4975372
[7]
Guralnik JM, Eisenstaedt RS, Ferrucci L, Klein HG, Woodman RC. Prevalence of anemia in persons 65 years and older in the United States: Evidence for a high rate of unexplained anemia. Blood 2004; 104: 2263-8.
Shulman LN, Braunwald E, Rosenthal DS. Hematological-oncological disorders and heart disease. In: Braunwald E. Heart Disease: A Textbook of Cardiovascular Medicine. 5th edn. Phildadelphia: WB Saunders, 1997: 1786±808.
[11]
Brannon ES, Merrill AJ, Warren JV, Stead EA. The cardiac output in patients with chronic anemia as measured by the technique of right atrial catheterization. J Clin Invest 1945; 24: 332.
Zeidman A, fradin Z, Blecher A, Oster HS, Avrahami Y, Mittelman M. Anemia as arisk factor for ischemic heart disease. Isr Med Assoc J. 2004; 6(1): 16-8. PMID: 14740503
[13]
Tang Y, Katz SD. Anemia in chronic heart failure: prevalence, etiology, clinical correlates, and treatment options. Circulation 2006; 113: 2454-61.
[14]
Tang WH, Tong W, Francis GS, et al. Evaluation and long-term prognosisof new onset transient and persistent anaemia in ambulatory patients withchronic heart failure. J Am Coll Cardiol 2008; 51(5): 569-76.
J. K Kologo1, G. R. C Millogo, Y Kambiré, H Adoko, L. J Kagambéga, A Thiam/Tall1, N. V Yaméogo et al. Heart failure and anemia in the cardiology department of the Yalgado Ouedraogo university teaching Hospital: epidemiology, management and prognosis. Health Sci. Dis, 2022; 23(2): 143-7.
Cleland JGF, Swedberg K, Cohen-Solal A et al. The Euroheart failure survey programme - a survey on the quality of care among patients with heart failure in Europe. EuropeanHeart Journal 2003; 24: 442-63.
Klipstein-Grobusch K, Koster JF, Grobbee DE, et al. Serum ferritin and risk of myocardial infarction in the eÏderly: theRotterdam Study. Am J Clin Nutr 1999; 69(6): 1231-6.
Kurl S, Tuomainen T, Laukkanen JA, et al. Plasma vitamin C modifies the association between hypertension and risk ofstroke. Stroke. 2002; 33(6): 156-73.
Anand IS, Chandrashekhar Y, Ferrari R, Poole-Wilson PE, Harris PS. Pathogenesis of oedema in chronic severe anemia: studies of body water and sodium, renal function, hemodynamic variables, and plasma hormones. Br Heart J 1993; 70: 357±62.
Silverberg DS, Wexler D, Blum M, et al. The use of subcutaneous erythropoietin and intravenous iron for the treatment of the anemia of severe, resistant congestive heart failure improves cardiac and renal function and functional cardiac class, and markedly reduces hospitalization. J Am Coll Cardiol 2000; 35: 1737±44.
Lubange K. Etude épidémiologique et clinique de l'Insuffisance cardiaque. Thèse Med: Université de Lubumbashi 2013.
[25]
Saudubray T, Saudubray C, Viboud C et al. Prévalence et prise en charge de l’insuffisance cardiaque en France: enquête nationale auprès des médecins généralistes du réseau Sentinelles, Rev Méd Intern 200.
Sarnak MJ, Tighiouart H, Manjunath G, et al. Anernia as a risk factor for cardiovascular disease in The Atherosclerosis Risk inCommunities (ARIC) study. J Am CouCardiol 2002 Jul 3; 40(1): 27-33.
Gaye, N. D., Ngaide, A. A., Mingou, J. S., Diaby, M. L., Ndiaye, M. B., et al. (2024). Prevalence of Anemia in Heart Failure Patients Hospitalized in a Cardiology Department in Dakar, Senegal. Cardiology and Cardiovascular Research, 8(4), 96-103. https://doi.org/10.11648/j.ccr.20240804.12
Gaye, N. D.; Ngaide, A. A.; Mingou, J. S.; Diaby, M. L.; Ndiaye, M. B., et al. Prevalence of Anemia in Heart Failure Patients Hospitalized in a Cardiology Department in Dakar, Senegal. Cardiol. Cardiovasc. Res.2024, 8(4), 96-103. doi: 10.11648/j.ccr.20240804.12
Gaye ND, Ngaide AA, Mingou JS, Diaby ML, Ndiaye MB, et al. Prevalence of Anemia in Heart Failure Patients Hospitalized in a Cardiology Department in Dakar, Senegal. Cardiol Cardiovasc Res. 2024;8(4):96-103. doi: 10.11648/j.ccr.20240804.12
@article{10.11648/j.ccr.20240804.12,
author = {Ngone Diaba Gaye and Aliou Alassane Ngaide and Joseph Salvador Mingou and Mamadou Lamine Diaby and Mouhamadou Bamba Ndiaye and Alassane Mbaye and Maboury Diao and Abdoul Kane},
title = {Prevalence of Anemia in Heart Failure Patients Hospitalized in a Cardiology Department in Dakar, Senegal
},
journal = {Cardiology and Cardiovascular Research},
volume = {8},
number = {4},
pages = {96-103},
doi = {10.11648/j.ccr.20240804.12},
url = {https://doi.org/10.11648/j.ccr.20240804.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20240804.12},
abstract = {The objectives of this study were to assess the prevalence of anemia in patients with heart failure, analyze the characteristics of anemia in this population, and identify prognostic factors related to anemia and heart failure. We conducted a descriptive and analytical retrospective study over a period of nine months, from April 1, 2018, to December 31, 2018. The study included patients aged over 18 years who were hospitalized in a cardiology department for heart failure of all causes, with hemoglobin levels strictly below 12 g/dl for women and 13 g/dl for men. Heart failure diagnosis was based on ESC 2016 criteria. The study was approved by the ethics committee of Cheikh Anta Diop University, Dakar. Data analysis was performed using SPSS 18 (Statistical Package for Social Sciences version 18), with a p-value of ≤ 0.05 considered statistically significant. We identified 182 patients with anemia, representing a hospital prevalence of 11.61%. The average age was 58.9 ± 15.93 years, with a female predominance in those under 50 years and a male predominance in those over 50. Most patients (77.1%) had a low socioeconomic status. Major cardiovascular risk factors included physical inactivity (56%) and hypertension (47%). Clinically, 78% of patients had dyspnea, 31.9% had chest pain, 40.7% had cutaneous-mucosal pallor, and 72.2% had global heart failure. Ischemic heart disease was the main cause of heart failure (49.2%). Diagnostic investigations revealed elevated ferritin in 50% of cases, elevated CRP in 88.1%, and elevated creatinine in 37.4%. The mean hemoglobin level was 11.6 ± 7.15 g/dl, with 71.4% of patients having hemoglobin between 10 and 13 g/dl. Normocytic normochromic anemia predominated. The study showed that anemia was more common in patients with an ejection fraction > 50% (48.1%) and those with global heart failure (72.2%). Statistically significant associations with severe and mild anemia were observed in the age groups 20-29 years (p=0.003) and 50-59 years (p=0.014) and with endocarditis (p=0.03). Only women showed severe and very severe anemia (p=0.21). The hospital mortality rate was 15.38%. In conclusion, this study reveals a significant prevalence of anemia among hospitalized patients, with important correlations between anemia and various clinical and socioeconomic factors.
},
year = {2024}
}
TY - JOUR
T1 - Prevalence of Anemia in Heart Failure Patients Hospitalized in a Cardiology Department in Dakar, Senegal
AU - Ngone Diaba Gaye
AU - Aliou Alassane Ngaide
AU - Joseph Salvador Mingou
AU - Mamadou Lamine Diaby
AU - Mouhamadou Bamba Ndiaye
AU - Alassane Mbaye
AU - Maboury Diao
AU - Abdoul Kane
Y1 - 2024/12/12
PY - 2024
N1 - https://doi.org/10.11648/j.ccr.20240804.12
DO - 10.11648/j.ccr.20240804.12
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 96
EP - 103
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20240804.12
AB - The objectives of this study were to assess the prevalence of anemia in patients with heart failure, analyze the characteristics of anemia in this population, and identify prognostic factors related to anemia and heart failure. We conducted a descriptive and analytical retrospective study over a period of nine months, from April 1, 2018, to December 31, 2018. The study included patients aged over 18 years who were hospitalized in a cardiology department for heart failure of all causes, with hemoglobin levels strictly below 12 g/dl for women and 13 g/dl for men. Heart failure diagnosis was based on ESC 2016 criteria. The study was approved by the ethics committee of Cheikh Anta Diop University, Dakar. Data analysis was performed using SPSS 18 (Statistical Package for Social Sciences version 18), with a p-value of ≤ 0.05 considered statistically significant. We identified 182 patients with anemia, representing a hospital prevalence of 11.61%. The average age was 58.9 ± 15.93 years, with a female predominance in those under 50 years and a male predominance in those over 50. Most patients (77.1%) had a low socioeconomic status. Major cardiovascular risk factors included physical inactivity (56%) and hypertension (47%). Clinically, 78% of patients had dyspnea, 31.9% had chest pain, 40.7% had cutaneous-mucosal pallor, and 72.2% had global heart failure. Ischemic heart disease was the main cause of heart failure (49.2%). Diagnostic investigations revealed elevated ferritin in 50% of cases, elevated CRP in 88.1%, and elevated creatinine in 37.4%. The mean hemoglobin level was 11.6 ± 7.15 g/dl, with 71.4% of patients having hemoglobin between 10 and 13 g/dl. Normocytic normochromic anemia predominated. The study showed that anemia was more common in patients with an ejection fraction > 50% (48.1%) and those with global heart failure (72.2%). Statistically significant associations with severe and mild anemia were observed in the age groups 20-29 years (p=0.003) and 50-59 years (p=0.014) and with endocarditis (p=0.03). Only women showed severe and very severe anemia (p=0.21). The hospital mortality rate was 15.38%. In conclusion, this study reveals a significant prevalence of anemia among hospitalized patients, with important correlations between anemia and various clinical and socioeconomic factors.
VL - 8
IS - 4
ER -
Gaye, N. D., Ngaide, A. A., Mingou, J. S., Diaby, M. L., Ndiaye, M. B., et al. (2024). Prevalence of Anemia in Heart Failure Patients Hospitalized in a Cardiology Department in Dakar, Senegal. Cardiology and Cardiovascular Research, 8(4), 96-103. https://doi.org/10.11648/j.ccr.20240804.12
Gaye, N. D.; Ngaide, A. A.; Mingou, J. S.; Diaby, M. L.; Ndiaye, M. B., et al. Prevalence of Anemia in Heart Failure Patients Hospitalized in a Cardiology Department in Dakar, Senegal. Cardiol. Cardiovasc. Res.2024, 8(4), 96-103. doi: 10.11648/j.ccr.20240804.12
Gaye ND, Ngaide AA, Mingou JS, Diaby ML, Ndiaye MB, et al. Prevalence of Anemia in Heart Failure Patients Hospitalized in a Cardiology Department in Dakar, Senegal. Cardiol Cardiovasc Res. 2024;8(4):96-103. doi: 10.11648/j.ccr.20240804.12
@article{10.11648/j.ccr.20240804.12,
author = {Ngone Diaba Gaye and Aliou Alassane Ngaide and Joseph Salvador Mingou and Mamadou Lamine Diaby and Mouhamadou Bamba Ndiaye and Alassane Mbaye and Maboury Diao and Abdoul Kane},
title = {Prevalence of Anemia in Heart Failure Patients Hospitalized in a Cardiology Department in Dakar, Senegal
},
journal = {Cardiology and Cardiovascular Research},
volume = {8},
number = {4},
pages = {96-103},
doi = {10.11648/j.ccr.20240804.12},
url = {https://doi.org/10.11648/j.ccr.20240804.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20240804.12},
abstract = {The objectives of this study were to assess the prevalence of anemia in patients with heart failure, analyze the characteristics of anemia in this population, and identify prognostic factors related to anemia and heart failure. We conducted a descriptive and analytical retrospective study over a period of nine months, from April 1, 2018, to December 31, 2018. The study included patients aged over 18 years who were hospitalized in a cardiology department for heart failure of all causes, with hemoglobin levels strictly below 12 g/dl for women and 13 g/dl for men. Heart failure diagnosis was based on ESC 2016 criteria. The study was approved by the ethics committee of Cheikh Anta Diop University, Dakar. Data analysis was performed using SPSS 18 (Statistical Package for Social Sciences version 18), with a p-value of ≤ 0.05 considered statistically significant. We identified 182 patients with anemia, representing a hospital prevalence of 11.61%. The average age was 58.9 ± 15.93 years, with a female predominance in those under 50 years and a male predominance in those over 50. Most patients (77.1%) had a low socioeconomic status. Major cardiovascular risk factors included physical inactivity (56%) and hypertension (47%). Clinically, 78% of patients had dyspnea, 31.9% had chest pain, 40.7% had cutaneous-mucosal pallor, and 72.2% had global heart failure. Ischemic heart disease was the main cause of heart failure (49.2%). Diagnostic investigations revealed elevated ferritin in 50% of cases, elevated CRP in 88.1%, and elevated creatinine in 37.4%. The mean hemoglobin level was 11.6 ± 7.15 g/dl, with 71.4% of patients having hemoglobin between 10 and 13 g/dl. Normocytic normochromic anemia predominated. The study showed that anemia was more common in patients with an ejection fraction > 50% (48.1%) and those with global heart failure (72.2%). Statistically significant associations with severe and mild anemia were observed in the age groups 20-29 years (p=0.003) and 50-59 years (p=0.014) and with endocarditis (p=0.03). Only women showed severe and very severe anemia (p=0.21). The hospital mortality rate was 15.38%. In conclusion, this study reveals a significant prevalence of anemia among hospitalized patients, with important correlations between anemia and various clinical and socioeconomic factors.
},
year = {2024}
}
TY - JOUR
T1 - Prevalence of Anemia in Heart Failure Patients Hospitalized in a Cardiology Department in Dakar, Senegal
AU - Ngone Diaba Gaye
AU - Aliou Alassane Ngaide
AU - Joseph Salvador Mingou
AU - Mamadou Lamine Diaby
AU - Mouhamadou Bamba Ndiaye
AU - Alassane Mbaye
AU - Maboury Diao
AU - Abdoul Kane
Y1 - 2024/12/12
PY - 2024
N1 - https://doi.org/10.11648/j.ccr.20240804.12
DO - 10.11648/j.ccr.20240804.12
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 96
EP - 103
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20240804.12
AB - The objectives of this study were to assess the prevalence of anemia in patients with heart failure, analyze the characteristics of anemia in this population, and identify prognostic factors related to anemia and heart failure. We conducted a descriptive and analytical retrospective study over a period of nine months, from April 1, 2018, to December 31, 2018. The study included patients aged over 18 years who were hospitalized in a cardiology department for heart failure of all causes, with hemoglobin levels strictly below 12 g/dl for women and 13 g/dl for men. Heart failure diagnosis was based on ESC 2016 criteria. The study was approved by the ethics committee of Cheikh Anta Diop University, Dakar. Data analysis was performed using SPSS 18 (Statistical Package for Social Sciences version 18), with a p-value of ≤ 0.05 considered statistically significant. We identified 182 patients with anemia, representing a hospital prevalence of 11.61%. The average age was 58.9 ± 15.93 years, with a female predominance in those under 50 years and a male predominance in those over 50. Most patients (77.1%) had a low socioeconomic status. Major cardiovascular risk factors included physical inactivity (56%) and hypertension (47%). Clinically, 78% of patients had dyspnea, 31.9% had chest pain, 40.7% had cutaneous-mucosal pallor, and 72.2% had global heart failure. Ischemic heart disease was the main cause of heart failure (49.2%). Diagnostic investigations revealed elevated ferritin in 50% of cases, elevated CRP in 88.1%, and elevated creatinine in 37.4%. The mean hemoglobin level was 11.6 ± 7.15 g/dl, with 71.4% of patients having hemoglobin between 10 and 13 g/dl. Normocytic normochromic anemia predominated. The study showed that anemia was more common in patients with an ejection fraction > 50% (48.1%) and those with global heart failure (72.2%). Statistically significant associations with severe and mild anemia were observed in the age groups 20-29 years (p=0.003) and 50-59 years (p=0.014) and with endocarditis (p=0.03). Only women showed severe and very severe anemia (p=0.21). The hospital mortality rate was 15.38%. In conclusion, this study reveals a significant prevalence of anemia among hospitalized patients, with important correlations between anemia and various clinical and socioeconomic factors.
VL - 8
IS - 4
ER -