While traditionally considered as a period of good health, adolescence with contemporary lifestyles and environmental factors is facing an alarming rise in cardiovascular risk factors. This was a school based cross sectional study including adolescents aged 10 to 19 years old in the city of Garoua. Physical activity, smoking, overweight, obesity, elevated blood pressure, hypertension, prediabetes and diabetes were evaluated. We included 938 participants (68.8% female) with a mean age of 16 ± 2 years. The most frequent risk factor was physical inactivity (52.8%). Overweight/obesity was more frequent in private schools (ORa = 2.76 [1.80 – 4.22], p < 0.001). Prediabetes/diabetes was significantly more frequent in the [10-15[ age category, in female participants, and in private schools (ORa = 2.16 [1.53 – 3.07]; p < 0.001, ORa = 1.50 [1.01 – 2.22]; p = 0.045, and ORa = 2,56 [1.79 – 3.66]; p < 0,001 respectively). Physical inactivity was significantly more frequent in female students and in the [10-15[ age category (ORa = 2.22 [1.68 – 2.95]; p < 0.001 and ORa = 1.37 [1.04 – 1.82]; p = 0.026 respectively). Male adolescents had 7-fold higher risk of smoking. There was no significant difference in the proportions of elevated blood pressure/hypertension, and abdominal obesity. Cardiovascular risk factors are present among secondary school adolescents in the city of Garoua. Public health policies should be implemented for the prevention and early management of these risk factors.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Cardiovascular diseases are among the leading causes of death globally, with a high burden particularly in low-middle income countries
[1]
Naghavi M, Ong KL, Aali A, Ababneh HS, Abate YH, Abbafati C, et al. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet. 2024; 403(10440): 2100-32.
. Teenagers are not left aside. Many risk factors are present since young age. While traditionally considered as a period of good health, adolescence with contemporary lifestyles and environmental factors is facing an alarming rise in cardiovascular risk factors
[2]
Hecht EM, Williams A-YP, Abrams GA, Passman RS. Cardiovascular Risk Factors in Young Adolescents: Results from the National Health and Nutrition Examination Survey 1988-2016. South Med J. 2021; 114(5): 261-5.
. Rodrigez et al found in the central region of Portugal, prevalences of abdominal obesity, overweight and obesity of 15.5%, 6.1% and 21.9% respectively
[3]
Rodrigues D, Padez C, Machado-Rodrigues AM. Prevalence of abdominal obesity and excess weight among Portuguese children and why abdominal obesity should be included in clinical practice. Acta Med Port. 2018; 31(3): 159-64.
. In Sub Saharan Africa, a systematic review by Kwansa et al described high prevalence levels of childhood, and adolescence obesity in countries such as Sierra Leone 16.9%, Cameroon 15.6% and Malawi 14.5%
[4]
Kwansa AL, Akparibo R, Cecil JE, Solar GI, Caton SJ. Risk Factors for Overweight and Obesity within the Home Environment of Preschool Children in Sub-Saharan Africa: A Systematic Review. Nutrients. 2022; 14(9).
. It is well known that cardiovascular risk factors in childhood are associated to cardiovascular diseases later in life
[5]
Kartiosuo N, Raitakari OT, Juonala M, Viikari JSA, Sinaiko AR, Venn AJ, et al. Cardiovascular Risk Factors in Childhood and Adulthood and Cardiovascular Disease in Middle Age. JAMA Netw Open. 2024; 7(6): e2418148.
. Therefore, their prevention and management may reduce the overall burden of cardiovascular disease. Much is known about these factors in developed countries but little scientific evidence exists in sub-Saharan African countries, and in Cameroon in particular. In a previous study in the southern part of the country in 2023, Kamdem et al studied 771 adolescents and found respectively 11.5%; 5.6%; 5.4%, and 3.0% for overweight/obesity, abdominal obesity, smoking, glucose homeostasis abnormalities, and high blood pressure
[6]
Kamdem F, Bika Léle EC, Mekoulou Ndongo J, Ba H, Obe Meyong MAP, Fenkeu Kweban J, et al. Cardiovascular risk factors among Cameroonian adolescents: Comparison between public and private schools and association with physical activity practice-a cross-sectional study. JRSM Cardiovasc Dis. 2023; 12: 20480040231210371.
. A better characterization of both presence and number of risk factors in young people in all regions of our country can significantly contribute to the implementation of early prevention strategies that may modify their natural history, and prevent cardiovascular disease onset. This study aimed to contribute with valuable data to inform public health strategies, to reduce the burden of cardiovascular risk factors among school youth in Cameroon.
2. Materials and Methods
2.1. Study Design, Setting and Duration
We conducted a school-based cross-sectional study from February to June 2024 in the city of Garoua, Benue division, North region, Cameroon.
2.2. Participants and Sampling
We included secondary school adolescents aged 10 to 19 years who accepted to participate and whose parents gave written informed consent. Our sample was selected using a multistage cluster random sampling method. In the first stage, the population was divided in two clusters represented by the Garoua 1 and Garoua 2 health districts. In the second stage, three public and private schools respectively, were randomly selected in each health district. In the third stage, we randomly selected classes, then 100 students who fulfilled the inclusion criteria, in each school.
The minimum sample size was determined using the Cochrane’s formula as follows:
With:
P = prevalence of Cardiovascular Risk Factors, we used the prevalence of 38.4% reported by Kamdem et al in Douala, Cameroon in 2023
[6]
Kamdem F, Bika Léle EC, Mekoulou Ndongo J, Ba H, Obe Meyong MAP, Fenkeu Kweban J, et al. Cardiovascular risk factors among Cameroonian adolescents: Comparison between public and private schools and association with physical activity practice-a cross-sectional study. JRSM Cardiovasc Dis. 2023; 12: 20480040231210371.
Z = standard normal variation. With a confidence interval to be 95% and by accepting an error of 5%, level of significance (α) 0.05, it corresponds to 1.96.
n = minimum sample size = 364
Considering an anticipated 10% non-response rate, we had to include a minimum of 401 students.
2.3. Procedure
We obtained for this study an ethical clearance of the institutional ethics committee for research in human health of the University of Douala. We also had a research authorization of the school medicine inspectorate of the regional delegation for secondary education of the North region. We had a little talk with students on cardiovascular diseases and their risk factors, the importance of an early detection and management. Students selected received an information sheet, and consent form for their parents to fill and sign. The students were explained on how to fill the consent form, and told to be fasting for at least 8 hours prior to blood testing. The next morning, we collected the signed consent forms, then the questionnaires were filled. Anthropometric parameters were measured and fasting blood sugar (FBS) tested. The information collected concerned socio-demographic data (age, gender, class, school), medical history and life style (smoking, alcohol habits, physical activity), and family history (diabetes, hypertension, obesity, others). Participants were considered as occasional smoker when smoking less than one cigarette a day. Occasional alcohol consumption was considered for taking at least one drink in 7 days.
2.4. Physical Activity Assessment
Physical activity (PA) was assessed using a modified version of the International Physical Activity Questionnaire (IPAQ) short form. The questionnaire was modified according to recent validated studies. The modified version covered four domains of PA: (1) school-related PA including activity during physical education classes and breaks, (2) transportation, (3) housework and (4) leisure time. In each of the four domains, the numbers of days per week and time per day spent in walking, moderate activity and vigorous activity were recorded, and used to calculate Metabolic Equivalent Task (METs) minutes per week. A MET is the ratio of the metabolic work rate to the resting metabolic rate. One MET is defined as 1 Kcal/kg/hour, and is roughly equivalent to the energy cost of sitting quietly. The intensity of physical activity is considered as light intensity for activities requiring less than 3.0 METs like walking at a leisure pace or standing in line at the store; moderate intensity for activities requiring 3.0 to 6.0 METs like walking briskly and vigorous intensity for activities requiring more than 6.0 METs examples walking very quickly, running
[7]
Robert-McComb JJ, Carnero EÁ, Iglesias-Gutiérrez E. Estimating Energy Requirements. In: Robert-McComb JJ, Norman RL, Zumwalt M, éditeurs. The Active Female [Internet]. New York, NY: Springer New York; 2014 [cité 9 févr 2025]. p. 411-49. Disponible sur:
a) High (vigorous-intensity activity on at least three days achieving a minimum total PA of 1500 MET min/week or seven or more days of any combination of walking, moderate intensity or vigorous intensity activities achieving at least 3000 MET min/week total PA),
b) Moderate (three or more days of vigorous intensity activity and/ or walking of at least 30 min per day; or at least five days of moderate intensity activity and/or walking of at least 30 min per day or at least five days of any combination of walking, moderate intensity or vigorous intensity activities achieving a minimum total PA of 600 MET min/week).
c) Low (not meeting any of the criteria for either moderate of high levels of PA).
2.5. Anthropometric Measurements
Weight was measured using a SECA® analog Scale while the student was standing at the center of the scale, and dressed in light clothes without shoes. Height was measured using a stadiometer graduated in centimeters. Students were standing upright arms hanging along the body, palms facing thighs, barefoot and head placed according to Frankfurt plan. The data obtained were projected unto world health organization curves for assessment of nutritional status. Body mass index (BMI) was calculated as the ratio of weight in kilograms divided by the square of height in meters. BMI between the 85th and 95th percentile was considered as overweight, while obesity was considered when BMI was greater than 95th percentile
[8]
Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000; 320(7244): 1240-3.
. Waist circumference (WC) was measured with a metric tape graduated in centimeters, midway between the lowest rib and the iliac crest to the nearest 0.1 cm after inhalation and exhalation. Waist to height ratio (WHtR) was calculated as the ratio of waist and height using the cut-off value of ≥ 0.5
[9]
Eslami M, Pourghazi F, Khazdouz M, Tian J, Pourrostami K, Esmaeili-Abdar Z, et al. Optimal cut-off value of waist circumference-to-height ratio to predict central obesity in children and adolescents: A systematic review and meta-analysis of diagnostic studies. Front Nutr [Internet]. Frontiers; 2023 [cité 9 févr 2025]; 9. Disponible sur:
We used an electronic BP monitor OMRON® 705 IT for children and adolescents with adapted cuffs according to standard recommendations. The students were in a quiet room, resting in a sitting position on a chair, with both feet on the ground, for at least 10 minutes. Blood pressure was measured twice with a 5 minutes interval. The cuff was placed 2 cm above the elbow joint and covered 2/3 arm’s length. The values obtained were projected onto the 2017 National High Blood Pressure (NHBP) curves with respect to age and gender. Elevated blood pressure was considered for blood pressure between 90th and the 95th percentiles, and hypertension for blood pressure greater than the 95th percentile, with respect to age and gender
[10]
National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004; 114(2 Suppl 4th Report): 555-76.
[10]
.
2.7. Fasting Blood Sugar Measurements
FBS was obtained after eight hours overnight fasting using ONETOUCH® and ACCU CHEK® glucometers with appropriate test strips. Prediabetes and diabetes were defined according to the 2018 standards of medical care in diabetes of the American Diabetes Association
[11]
American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2018. Diabetes Care. 2017; 41(Supplement_1): S13-27.
Data was analyzed using Statistical Package for Social Sciences (SPSS) version 26.0. Quantitative variables were presented as mean ± standard deviation, and qualitative variables as numbers and percentages. The Student T-test was used to compare means. The Chi-square test and multivariate logistic regression analysis were employed to determine factors associated with the presence of cardiovascular risk factors. Differences were considered statistically significant at p<0.05.
3. Results
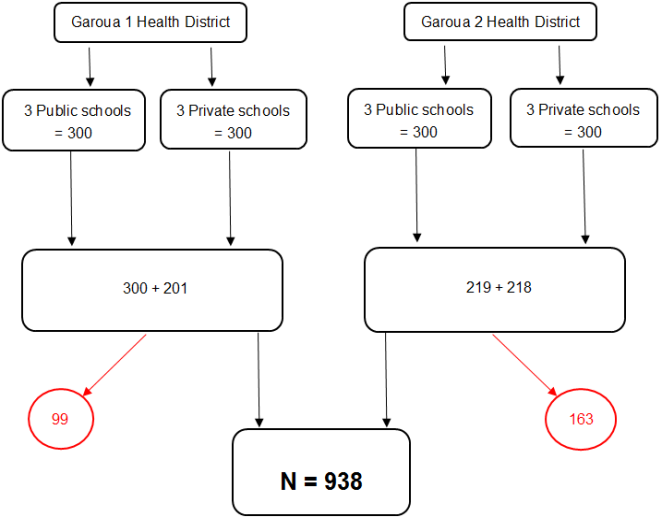
Figure 1 shows the flow chart of participants. We sampled 1200 students from both 3 public and 3 private secondary schools in both Garoua 1 and Garoua 2 health districts. The number of students who completed the study was 938. We had a female predominance (68.8%), and 55.6% were in public schools. Two third of the students were in lower secondary education level. We found a family history of hypertension, diabetes and obesity in respectively 22.7, 13.0 and 8.7% of cases (Table 1). There were significantly more female participants in public than in private schools (71.6% vs 63.0%; p = 0.005). The mean age was 16 ± 2 years. It was significantly higher in public than in private schools (16 ± 2 vs 15 ± 2 years; p < 0.001).
Table 1. Sociodemographic and lifestyle characteristics of the study population.
Variables
Categories
Number
Percentage (%)
Age group
[10 – 15]
333
35.5
[15 – 20]
605
64.5
Gender
Male
302
32.2
Female
636
68.8
Type of school
Public
522
55.6
Private
416
44.4
Level of secondary education
Lower*
622
66.3
Upper**
316
33.7
Family history
Hypertension
213
22.7
Diabetes
122
13.0
Obesity
82
8.7
Physical activity level
Low
515
53.3
Moderate
292
30.2
High
159
16.5
Smoking
29
3.1
Alcohol consumption
166
17.7
*Lower: form 1 to 4; **Upper: form 5, lower sixth and upper sixth
Table 2 presents the prevalences of cardiovascular risk factors in the study population. The tree most frequent cardiovascular risk factors were low physical activity, which was present in more than half of the participants, prediabetes and overweight. Of note, 29 (3.1%) participants were smokers. We looked for factors associated with the presence of cardiovascular risk factors (Table 3). Low physical activity was significantly more frequent in female students and in the [10-15[ age category. The differences persisted even after multivariate analysis (ORa = 2.22 [1.68 – 2.95]; p < 0.001 and ORa = 1.37 [1.04 – 1.82]; p = 0.026 respectively). Overweight/obesity was more frequent in private schools and the difference persisted after adjustment for gender and age category (ORa = 2.76 [1.80 – 4.22], p < 0.001). Prediabetes/diabetes was significantly more frequent in the [10-15[ age category, in female participants, and in private schools, even after multivariate analysis (ORa = 2.16 [1.53 – 3.07]; p < 0.001, ORa = 1.50 [1.01 – 2.22]; p = 0.045, and ORa = 2,56 [1.79 – 3.66]; p < 0,001 respectively). Male students had 7-fold higher risk of smoking and were all aged 15 years or more. There was no significant difference in the proportions of abdominal obesity. There was no significant difference in the proportion of elevated blood pressure/hypertension with respect to gender, age category and school type.
Table 2. Cardiovascular risk factors in the study population.
Variables
Number (Percentage)
Male (n=302)
Female (n=636)
All gender (N=938)
Overweight
31 (10.3)
62 (9.8)
93 (9.9)
Obesity
4 (1.3)
12 (1.9)
16 (1.7)
Elevated blood pressure
25 (8.3)
41 (6.5)
66 (7.0)
Hypertension
7 (2.3)
13 (2.0)
20 (2.1)
Prediabetes
44 (14.6)
115 (18.3)
159 (17.1)
Diabetes
0 (0.0)
3 (0.5)
3 (0.3)
Abdominal obesity (WC)
13 (4.3)
42 (6.6)
55 (5.9)
Abdominal obesity (WHtR)
12 (4.0)
46 (7.2)
58 (6.2)
Smoking
17 (5.6)
12 (1.9)
29 (3.1)
Low physical activity
119 (39.4)
376 (59.1)
495 (52.8)
WC: waist circumference; WHtR: waist to height ratio
Table 3. Factors associated to cardiovascular risk factors.
We conducted this study in order to contribute with valuable data, to a better understanding of the burden of cardiovascular risk factors in adolescents in Cameroon. Some studies have been done in southern Cameroon
[6]
Kamdem F, Bika Léle EC, Mekoulou Ndongo J, Ba H, Obe Meyong MAP, Fenkeu Kweban J, et al. Cardiovascular risk factors among Cameroonian adolescents: Comparison between public and private schools and association with physical activity practice-a cross-sectional study. JRSM Cardiovasc Dis. 2023; 12: 20480040231210371.
Wamba PCF, Enyong Oben J, Cianflone K. Prevalence of Overweight, Obesity, and Thinness in Cameroon Urban Children and Adolescents. J Obes. 2013; 2013: 737592.
, but never in the North, which is geographically and culturally different. Similarly, we had a female predominance in our sample. The prevalence of low physical activity was also similar to the result of Kamdem et al
[6]
Kamdem F, Bika Léle EC, Mekoulou Ndongo J, Ba H, Obe Meyong MAP, Fenkeu Kweban J, et al. Cardiovascular risk factors among Cameroonian adolescents: Comparison between public and private schools and association with physical activity practice-a cross-sectional study. JRSM Cardiovasc Dis. 2023; 12: 20480040231210371.
, and its association to female gender his well-documented in the literature
[13]
Wenthe PJ, Janz KF, Levy SM. Gender Similarities and Differences in Factors Associated with Adolescent Moderate-Vigorous Physical Activity. Pediatr Exerc Sci. 2009; 21(3): 291-304.
Lenhart CM, Hanlon A, Kang Y, Daly BP, Brown MD, Patterson F. Gender Disparity in Structured Physical Activity and Overall Activity Level in Adolescence: Evaluation of Youth Risk Behavior Surveillance Data. ISRN Public Health. 2012; 2012: 1-8.
Overweight/obesity on the other hand was less frequent, and this may be explained by the fact that Cameroonians originating from the North are constitutionally thinner than in the South. Moreover, overweight/obesity was more frequent in private schools, likewise prediabetes/diabetes. This can be explained by the fact that adolescents in private schools, are more likely to come from high-income families, with easy access to high caloric food. It is known that private schools are expensive in Cameroon, and cannot be afforded by everyone
[16]
Eboue R, Dudjo Yen GB. L’impact de l’offre privée d’éducation sur le taux de scolarisation au secondaire : cas du Cameroun. Rev Econ Gest Société. 2021; 1(31).
. Prediabetes/diabetes was also more frequent in younger students. This is concordant with the recent findings of Kandemir et al, in a report of 50-year experience in Turkey showing that the mean age at diagnosis of type 1 diabetes, the most frequent type of diabetes in adolescents, is under 10
[17]
Kandemir N, Vuralli D, Ozon A, Gonc N, Ardicli D, Jalilova L, et al. Epidemiology of type 1 diabetes mellitus in children and adolescents: A 50-year, single-center experience. J Diabetes. 2024; 16(5): e13562.
Regarding smoking, we found a low prevalence, like Kamdem et al, compare to the findings in Europe, Asia, America, and even in other sub-Saharan countries
[6]
Kamdem F, Bika Léle EC, Mekoulou Ndongo J, Ba H, Obe Meyong MAP, Fenkeu Kweban J, et al. Cardiovascular risk factors among Cameroonian adolescents: Comparison between public and private schools and association with physical activity practice-a cross-sectional study. JRSM Cardiovasc Dis. 2023; 12: 20480040231210371.
Morgenstern M, Sargent JD, Engels RCME, Florek E, Hanewinkel R. Smoking in European adolescents: Relation between media influences, family affluence, and migration background. Addict Behav. 2013; 38(10): 2589-95.
Han J, Chen X. A Meta-Analysis of Cigarette Smoking Prevalence among Adolescents in China: 1981-2010. Int J Environ Res Public Health. 2015; 12(5): 4617-30.
Tezera N, Endalamaw A. Current Cigarette Smoking and Its Predictors among School-Going Adolescents in East Africa: A Systematic Review and Meta-Analysis. Int J Pediatr. 2019; 2019: 4769820.
. Smoking is not well perceived in the Cameroonian society in general. We also found, like in the literature, a significantly higher risk of smoking in male adolescents.
Elevated blood pressure and hypertension prevalences were similar to the results of Chelo et al, and Kamdem et al in Cameroon
[6]
Kamdem F, Bika Léle EC, Mekoulou Ndongo J, Ba H, Obe Meyong MAP, Fenkeu Kweban J, et al. Cardiovascular risk factors among Cameroonian adolescents: Comparison between public and private schools and association with physical activity practice-a cross-sectional study. JRSM Cardiovasc Dis. 2023; 12: 20480040231210371.
Chelo D, Mah EM, Chiabi EN, Chiabi A, Koki Ndombo PO, Kingue S, et al. Prevalence and factors associated with hypertension in primary school children, in the centre region of Cameroon. Transl Pediatr. 2019; 8(5): 391-7.
. But il was lower than the findings of Ejike et al in Nigeria and Sungwa et al in Tanzania
[22]
Ejike CE, Ugwu CE, Ezeanyika LU. Variations in the prevalence of point (pre)hypertension in a Nigerian school-going adolescent population living in a semi-urban and an urban area. BMC Pediatr. 2010; 10: 13.
Sungwa EE, Kibona SE, Dika HI, Laisser RM, Gemuhay HM, Kabalimu TK, et al. Prevalence and factors that are associated with elevated blood pressure among primary school children in Mwanza Region, Tanzania. Pan Afr Med J. 2020; 37: 283.
. This difference may be explained by different population characteristics, and differences in methodology. Moreover, we did not find any factors associated to elevated blood pressure/hypertension. In contrary, Sungwa et al found that, older age, female gender, obesity, overweight, eating fried food and not eating fruits, all increased significantly the odds of elevated blood pressure
[23]
Sungwa EE, Kibona SE, Dika HI, Laisser RM, Gemuhay HM, Kabalimu TK, et al. Prevalence and factors that are associated with elevated blood pressure among primary school children in Mwanza Region, Tanzania. Pan Afr Med J. 2020; 37: 283.
. Some of these factors were not studied in our research.
5. Strengths and Limitations
This was a school-based study, and we used a multistage cluster random sampling method for the selection of participants. Our results can therefore be extrapolated to all the population of school adolescents of 10 to 19 years. However, our sample does not represent de entire population of equally aged adolescents, since some of them are not enrolled in school. Moreover, we did not determine lipid profile. This is mainly due to the reticence of students and their parents, who did not want us to collect and carry their blood to the lab.
6. Conclusions
We conducted this study to contribute with valuable data, in order to inform public health strategies targeting cardiovascular risk factors among school adolescents in Cameroon. We found that cardiovascular risk factors are frequent among secondary school adolescents in the city of Garoua. Many appear to be more frequent in private schools, female and younger adolescents. Smoking odds was 7-fold higher in male students. Public health policies should be implemented for the prevention and early management of these risk factors. Long term follow-up studies are also needed, to determine outcomes in the affected students.
Abbreviations
BMI
Body Mass Index
FBS
Fasting Blood Sugar
IPAQ
International Physical Activity Questionnaire
MET
Metabolic Equivalent Task
NHBP
National High Blood Pressure
PA
Physical Activity
SPSS
Statistical Package for Social Sciences
WC
Waist Circumference
WHtR
Waist to Height Ratio
Author Contributions
Ba Hamadou: Conceptualization, Methodology, Validation
Jocelyn Tony Nengom: Conceptualization, Methodology, Validation
Jean Bugin: Conceptualization, Methodology, Validation
Chris Nadège Nganou-Gnindjio: Visualization, Writing-original draft preparation, Review and editing
Dieudonné Danwe: Visualization, Writing-original draft preparation, Review and editing
Félicité Kamdem: Supervision
Data Availability Statement
Data supporting the results of this study is available upon reasonable request to the corresponding author.
Funding
The authors did not receive any fund for this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Naghavi M, Ong KL, Aali A, Ababneh HS, Abate YH, Abbafati C, et al. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet. 2024; 403(10440): 2100-32.
Hecht EM, Williams A-YP, Abrams GA, Passman RS. Cardiovascular Risk Factors in Young Adolescents: Results from the National Health and Nutrition Examination Survey 1988-2016. South Med J. 2021; 114(5): 261-5.
Rodrigues D, Padez C, Machado-Rodrigues AM. Prevalence of abdominal obesity and excess weight among Portuguese children and why abdominal obesity should be included in clinical practice. Acta Med Port. 2018; 31(3): 159-64.
Kwansa AL, Akparibo R, Cecil JE, Solar GI, Caton SJ. Risk Factors for Overweight and Obesity within the Home Environment of Preschool Children in Sub-Saharan Africa: A Systematic Review. Nutrients. 2022; 14(9).
Kartiosuo N, Raitakari OT, Juonala M, Viikari JSA, Sinaiko AR, Venn AJ, et al. Cardiovascular Risk Factors in Childhood and Adulthood and Cardiovascular Disease in Middle Age. JAMA Netw Open. 2024; 7(6): e2418148.
Kamdem F, Bika Léle EC, Mekoulou Ndongo J, Ba H, Obe Meyong MAP, Fenkeu Kweban J, et al. Cardiovascular risk factors among Cameroonian adolescents: Comparison between public and private schools and association with physical activity practice-a cross-sectional study. JRSM Cardiovasc Dis. 2023; 12: 20480040231210371.
Robert-McComb JJ, Carnero EÁ, Iglesias-Gutiérrez E. Estimating Energy Requirements. In: Robert-McComb JJ, Norman RL, Zumwalt M, éditeurs. The Active Female [Internet]. New York, NY: Springer New York; 2014 [cité 9 févr 2025]. p. 411-49. Disponible sur:
Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000; 320(7244): 1240-3.
Eslami M, Pourghazi F, Khazdouz M, Tian J, Pourrostami K, Esmaeili-Abdar Z, et al. Optimal cut-off value of waist circumference-to-height ratio to predict central obesity in children and adolescents: A systematic review and meta-analysis of diagnostic studies. Front Nutr [Internet]. Frontiers; 2023 [cité 9 févr 2025]; 9. Disponible sur:
National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004; 114(2 Suppl 4th Report): 555-76.
[11]
American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2018. Diabetes Care. 2017; 41(Supplement_1): S13-27.
Wamba PCF, Enyong Oben J, Cianflone K. Prevalence of Overweight, Obesity, and Thinness in Cameroon Urban Children and Adolescents. J Obes. 2013; 2013: 737592.
Wenthe PJ, Janz KF, Levy SM. Gender Similarities and Differences in Factors Associated with Adolescent Moderate-Vigorous Physical Activity. Pediatr Exerc Sci. 2009; 21(3): 291-304.
Lenhart CM, Hanlon A, Kang Y, Daly BP, Brown MD, Patterson F. Gender Disparity in Structured Physical Activity and Overall Activity Level in Adolescence: Evaluation of Youth Risk Behavior Surveillance Data. ISRN Public Health. 2012; 2012: 1-8.
Eboue R, Dudjo Yen GB. L’impact de l’offre privée d’éducation sur le taux de scolarisation au secondaire : cas du Cameroun. Rev Econ Gest Société. 2021; 1(31).
Kandemir N, Vuralli D, Ozon A, Gonc N, Ardicli D, Jalilova L, et al. Epidemiology of type 1 diabetes mellitus in children and adolescents: A 50-year, single-center experience. J Diabetes. 2024; 16(5): e13562.
Morgenstern M, Sargent JD, Engels RCME, Florek E, Hanewinkel R. Smoking in European adolescents: Relation between media influences, family affluence, and migration background. Addict Behav. 2013; 38(10): 2589-95.
Han J, Chen X. A Meta-Analysis of Cigarette Smoking Prevalence among Adolescents in China: 1981-2010. Int J Environ Res Public Health. 2015; 12(5): 4617-30.
Tezera N, Endalamaw A. Current Cigarette Smoking and Its Predictors among School-Going Adolescents in East Africa: A Systematic Review and Meta-Analysis. Int J Pediatr. 2019; 2019: 4769820.
Chelo D, Mah EM, Chiabi EN, Chiabi A, Koki Ndombo PO, Kingue S, et al. Prevalence and factors associated with hypertension in primary school children, in the centre region of Cameroon. Transl Pediatr. 2019; 8(5): 391-7.
Ejike CE, Ugwu CE, Ezeanyika LU. Variations in the prevalence of point (pre)hypertension in a Nigerian school-going adolescent population living in a semi-urban and an urban area. BMC Pediatr. 2010; 10: 13.
Sungwa EE, Kibona SE, Dika HI, Laisser RM, Gemuhay HM, Kabalimu TK, et al. Prevalence and factors that are associated with elevated blood pressure among primary school children in Mwanza Region, Tanzania. Pan Afr Med J. 2020; 37: 283.
Hamadou, B., Nengom, J. T., Maryam, D. P., Bugin, J., Nganou-Gnindjio, C. N., et al. (2025). Cardiovascular Risk Factors Among Secondary School Adolescents in the City of Garoua, Cameroon. Cardiology and Cardiovascular Research, 9(2), 39-46. https://doi.org/10.11648/j.ccr.20250902.11
Hamadou, B.; Nengom, J. T.; Maryam, D. P.; Bugin, J.; Nganou-Gnindjio, C. N., et al. Cardiovascular Risk Factors Among Secondary School Adolescents in the City of Garoua, Cameroon. Cardiol. Cardiovasc. Res.2025, 9(2), 39-46. doi: 10.11648/j.ccr.20250902.11
Hamadou B, Nengom JT, Maryam DP, Bugin J, Nganou-Gnindjio CN, et al. Cardiovascular Risk Factors Among Secondary School Adolescents in the City of Garoua, Cameroon. Cardiol Cardiovasc Res. 2025;9(2):39-46. doi: 10.11648/j.ccr.20250902.11
@article{10.11648/j.ccr.20250902.11,
author = {Ba Hamadou and Jocelyn Tony Nengom and Dasso Pendo Maryam and Jean Bugin and Chris Nadège Nganou-Gnindjio and Dieudonné Danwe and Félicité Kamdem},
title = {Cardiovascular Risk Factors Among Secondary School Adolescents in the City of Garoua, Cameroon},
journal = {Cardiology and Cardiovascular Research},
volume = {9},
number = {2},
pages = {39-46},
doi = {10.11648/j.ccr.20250902.11},
url = {https://doi.org/10.11648/j.ccr.20250902.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20250902.11},
abstract = {While traditionally considered as a period of good health, adolescence with contemporary lifestyles and environmental factors is facing an alarming rise in cardiovascular risk factors. This was a school based cross sectional study including adolescents aged 10 to 19 years old in the city of Garoua. Physical activity, smoking, overweight, obesity, elevated blood pressure, hypertension, prediabetes and diabetes were evaluated. We included 938 participants (68.8% female) with a mean age of 16 ± 2 years. The most frequent risk factor was physical inactivity (52.8%). Overweight/obesity was more frequent in private schools (ORa = 2.76 [1.80 – 4.22], p < 0.001). Prediabetes/diabetes was significantly more frequent in the [10-15[ age category, in female participants, and in private schools (ORa = 2.16 [1.53 – 3.07]; p < 0.001, ORa = 1.50 [1.01 – 2.22]; p = 0.045, and ORa = 2,56 [1.79 – 3.66]; p < 0,001 respectively). Physical inactivity was significantly more frequent in female students and in the [10-15[ age category (ORa = 2.22 [1.68 – 2.95]; p < 0.001 and ORa = 1.37 [1.04 – 1.82]; p = 0.026 respectively). Male adolescents had 7-fold higher risk of smoking. There was no significant difference in the proportions of elevated blood pressure/hypertension, and abdominal obesity. Cardiovascular risk factors are present among secondary school adolescents in the city of Garoua. Public health policies should be implemented for the prevention and early management of these risk factors.},
year = {2025}
}
TY - JOUR
T1 - Cardiovascular Risk Factors Among Secondary School Adolescents in the City of Garoua, Cameroon
AU - Ba Hamadou
AU - Jocelyn Tony Nengom
AU - Dasso Pendo Maryam
AU - Jean Bugin
AU - Chris Nadège Nganou-Gnindjio
AU - Dieudonné Danwe
AU - Félicité Kamdem
Y1 - 2025/03/26
PY - 2025
N1 - https://doi.org/10.11648/j.ccr.20250902.11
DO - 10.11648/j.ccr.20250902.11
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 39
EP - 46
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20250902.11
AB - While traditionally considered as a period of good health, adolescence with contemporary lifestyles and environmental factors is facing an alarming rise in cardiovascular risk factors. This was a school based cross sectional study including adolescents aged 10 to 19 years old in the city of Garoua. Physical activity, smoking, overweight, obesity, elevated blood pressure, hypertension, prediabetes and diabetes were evaluated. We included 938 participants (68.8% female) with a mean age of 16 ± 2 years. The most frequent risk factor was physical inactivity (52.8%). Overweight/obesity was more frequent in private schools (ORa = 2.76 [1.80 – 4.22], p < 0.001). Prediabetes/diabetes was significantly more frequent in the [10-15[ age category, in female participants, and in private schools (ORa = 2.16 [1.53 – 3.07]; p < 0.001, ORa = 1.50 [1.01 – 2.22]; p = 0.045, and ORa = 2,56 [1.79 – 3.66]; p < 0,001 respectively). Physical inactivity was significantly more frequent in female students and in the [10-15[ age category (ORa = 2.22 [1.68 – 2.95]; p < 0.001 and ORa = 1.37 [1.04 – 1.82]; p = 0.026 respectively). Male adolescents had 7-fold higher risk of smoking. There was no significant difference in the proportions of elevated blood pressure/hypertension, and abdominal obesity. Cardiovascular risk factors are present among secondary school adolescents in the city of Garoua. Public health policies should be implemented for the prevention and early management of these risk factors.
VL - 9
IS - 2
ER -
Faculty of Medicine and Biomedical Sciences, University of Yaoundé I, Yaoundé, Cameroon; Department of Internal Medicine, Garoua General Hospital, Garoua, Cameroon
Faculty of Medicine and Biomedical Sciences, University of Yaoundé I, Yaoundé, Cameroon; Mother and Child Centre, Chantal Biya Foundation, Yaoundé, Cameroon
Higher Institute of Medical Technology, University of Douala, Yaoundé, Cameroon
Jean Bugin
Higher Institute of Medical Technology, University of Douala, Yaoundé, Cameroon
Chris Nadège Nganou-Gnindjio
Faculty of Medicine and Biomedical Sciences, University of Yaoundé I, Yaoundé, Cameroon; Department of Internal Medicine, University Teaching Hospital, Yaoundé, Cameroon
Faculty of Medicine and Pharmaceutical Sciences, University of Douala, Douala, Cameroon; Department of Internal Medicine, Douala General Hospital, Douala, Cameroon
Hamadou, B., Nengom, J. T., Maryam, D. P., Bugin, J., Nganou-Gnindjio, C. N., et al. (2025). Cardiovascular Risk Factors Among Secondary School Adolescents in the City of Garoua, Cameroon. Cardiology and Cardiovascular Research, 9(2), 39-46. https://doi.org/10.11648/j.ccr.20250902.11
Hamadou, B.; Nengom, J. T.; Maryam, D. P.; Bugin, J.; Nganou-Gnindjio, C. N., et al. Cardiovascular Risk Factors Among Secondary School Adolescents in the City of Garoua, Cameroon. Cardiol. Cardiovasc. Res.2025, 9(2), 39-46. doi: 10.11648/j.ccr.20250902.11
Hamadou B, Nengom JT, Maryam DP, Bugin J, Nganou-Gnindjio CN, et al. Cardiovascular Risk Factors Among Secondary School Adolescents in the City of Garoua, Cameroon. Cardiol Cardiovasc Res. 2025;9(2):39-46. doi: 10.11648/j.ccr.20250902.11
@article{10.11648/j.ccr.20250902.11,
author = {Ba Hamadou and Jocelyn Tony Nengom and Dasso Pendo Maryam and Jean Bugin and Chris Nadège Nganou-Gnindjio and Dieudonné Danwe and Félicité Kamdem},
title = {Cardiovascular Risk Factors Among Secondary School Adolescents in the City of Garoua, Cameroon},
journal = {Cardiology and Cardiovascular Research},
volume = {9},
number = {2},
pages = {39-46},
doi = {10.11648/j.ccr.20250902.11},
url = {https://doi.org/10.11648/j.ccr.20250902.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20250902.11},
abstract = {While traditionally considered as a period of good health, adolescence with contemporary lifestyles and environmental factors is facing an alarming rise in cardiovascular risk factors. This was a school based cross sectional study including adolescents aged 10 to 19 years old in the city of Garoua. Physical activity, smoking, overweight, obesity, elevated blood pressure, hypertension, prediabetes and diabetes were evaluated. We included 938 participants (68.8% female) with a mean age of 16 ± 2 years. The most frequent risk factor was physical inactivity (52.8%). Overweight/obesity was more frequent in private schools (ORa = 2.76 [1.80 – 4.22], p < 0.001). Prediabetes/diabetes was significantly more frequent in the [10-15[ age category, in female participants, and in private schools (ORa = 2.16 [1.53 – 3.07]; p < 0.001, ORa = 1.50 [1.01 – 2.22]; p = 0.045, and ORa = 2,56 [1.79 – 3.66]; p < 0,001 respectively). Physical inactivity was significantly more frequent in female students and in the [10-15[ age category (ORa = 2.22 [1.68 – 2.95]; p < 0.001 and ORa = 1.37 [1.04 – 1.82]; p = 0.026 respectively). Male adolescents had 7-fold higher risk of smoking. There was no significant difference in the proportions of elevated blood pressure/hypertension, and abdominal obesity. Cardiovascular risk factors are present among secondary school adolescents in the city of Garoua. Public health policies should be implemented for the prevention and early management of these risk factors.},
year = {2025}
}
TY - JOUR
T1 - Cardiovascular Risk Factors Among Secondary School Adolescents in the City of Garoua, Cameroon
AU - Ba Hamadou
AU - Jocelyn Tony Nengom
AU - Dasso Pendo Maryam
AU - Jean Bugin
AU - Chris Nadège Nganou-Gnindjio
AU - Dieudonné Danwe
AU - Félicité Kamdem
Y1 - 2025/03/26
PY - 2025
N1 - https://doi.org/10.11648/j.ccr.20250902.11
DO - 10.11648/j.ccr.20250902.11
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 39
EP - 46
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20250902.11
AB - While traditionally considered as a period of good health, adolescence with contemporary lifestyles and environmental factors is facing an alarming rise in cardiovascular risk factors. This was a school based cross sectional study including adolescents aged 10 to 19 years old in the city of Garoua. Physical activity, smoking, overweight, obesity, elevated blood pressure, hypertension, prediabetes and diabetes were evaluated. We included 938 participants (68.8% female) with a mean age of 16 ± 2 years. The most frequent risk factor was physical inactivity (52.8%). Overweight/obesity was more frequent in private schools (ORa = 2.76 [1.80 – 4.22], p < 0.001). Prediabetes/diabetes was significantly more frequent in the [10-15[ age category, in female participants, and in private schools (ORa = 2.16 [1.53 – 3.07]; p < 0.001, ORa = 1.50 [1.01 – 2.22]; p = 0.045, and ORa = 2,56 [1.79 – 3.66]; p < 0,001 respectively). Physical inactivity was significantly more frequent in female students and in the [10-15[ age category (ORa = 2.22 [1.68 – 2.95]; p < 0.001 and ORa = 1.37 [1.04 – 1.82]; p = 0.026 respectively). Male adolescents had 7-fold higher risk of smoking. There was no significant difference in the proportions of elevated blood pressure/hypertension, and abdominal obesity. Cardiovascular risk factors are present among secondary school adolescents in the city of Garoua. Public health policies should be implemented for the prevention and early management of these risk factors.
VL - 9
IS - 2
ER -