Abstract
Introduction: The management of acute coronary syndromes (ACS) in Senegal continues to pose challenges, despite significant progress in medical care. To comprehensively understand the current state of ACS in Senegal, a systematic review with meta-analysis was deemed essential. The main objective of this study was to determine the prevalence of ACS in Senegal and its trajectory over time. Methods: A systematic review of grey literature, encompassing theses and dissertations on ACS conducted in public hospitals in Senegal between 1990 and 2023, was undertaken. The selected studies provided valuable insights into the prevalence, epidemiological characteristics, cardiovascular risk factors, diagnostic approaches, therapeutic interventions, and prognostic outcomes associated with ACS. A meta-analysis of prevalence and mortality data was performed using the DerSimonian-Laird random-effects model, while the remaining data were synthesized descriptively. Results: The systematic review yielded 15 eligible studies from 1998 to 2020, out of an initial 101 identified documents. The overall prevalence of ACS was determined to be 9% (95% Cl: 7-11%, 12 = 96%, p < 0.01). Notably, in Dakar, the prevalence exhibited a significant increase between 1998 to 2010 and 2013 to 2020 (p < 0.01), rising from 6% (95% Cl: 4-8%, 12 = 96%, p < 0.01) to 13% (95% CI: 9-16%, 12 = 95%, p < 0.01). The proportion of patients presenting with ST-elevation ACS ranged from 44 to 94%. The average age of patients varied between 57 and 64 years, with a consistent male predominance across all studies. A notable improvement in mean admission delay to cardiology services in Dakar was observed, decreasing from 186 hours in 2002 to 28 hours in 2018. Thrombolysis utilization for ST-elevation ACS patients in Dakar ranged from 2.1 to 64.8%, while other regions reported rates of 10% in Kaolack, 53.8% in Saint-Louis, and 52.6% in Thies. In Dakar, the rate of coronary angiography increased substantially from 0% to 60.6% between 1998 and 2020, with percutaneous coronary intervention performed in 4.3% to 35.3% of cases. The frequency of heart failure ranged from 6.7 to 52.9%, and cardiogenic shock occurred in 1 to 18.5% of patients. The overall mortality rate was 10% (95% CI: 7-13%, 12 = 64%, p < 0.01). Conclusion: Our study demonstrates that despite an increase in prevalence, there is an improvement in the management of ACS. However, the establishment of a national registry and a comprehensive network for ACS management is crucial to further improve morbidity and mortality outcomes.
|
Published in
|
Cardiology and Cardiovascular Research (Volume 9, Issue 2)
|
|
DOI
|
10.11648/j.ccr.20250902.13
|
|
Page(s)
|
54-63 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Acute Coronary Syndromes, Meta-analysis, Senegal
1. Introduction
Acute coronary syndromes (ACS) encompass a spectrum of conditions that include patients presenting with recent changes in clinical symptoms or signs, with or without changes on 12-lead electrocardiogram (ECG) and with or without acute elevations in cardiac troponin concentrations
| [1] | Byrne RA, Rossello X, Coughlan JJ, Barbato E, Berry C, Chieffo A et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023; ehad191. |
[1]
. It is estimated that over seven million people worldwide are diagnosed with ACS annually
| [1] | Byrne RA, Rossello X, Coughlan JJ, Barbato E, Berry C, Chieffo A et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023; ehad191. |
[1]
. Additionally, cardiovascular diseases were the leading cause of death globally in 2019, according to the World Health Organization (WHO), with coronary artery disease (CAD) being the primary cause of mortality
. These deaths attributed to CAD have shown the most significant increase since 2000
.
The prevalence of ACS varies across different regions worldwide. In France, the France PCI 2022 registry estimates 120,000 myocardial infarctions annually
. A recent systemic review revealed that the hospital frequency of ACS in 13 sub-Saharan African countries ranged from 0.21 to 22.3% between 2011 and 2020
| [4] | Yao H, Ekou A, Niamkey T, Hounhoui Gan S, Kouamé I, Afassinou Y, et al. Acute Coronary Syndromes in Sub‐Saharan Africa: A 10‐Year Systematic Review. Journal of the American Heart Association. 2022; 11(1): e021107. |
[4]
.
In Senegal, the actual national prevalence of acute coronary syndrome remains elusive due to limited data in certain regions. However, several studies, primarily conducted in Dakar, indicates that prevalence, similar to other countries, is rising
| [5] | Guissé PM, Sall SAB, Niang T, Doucouré TS, Mboup MC, Ngaïdé AA and al. Acute coronary syndromes in diabetes mellitus: A comparative study between diabetics and non-diabetics patients in Senegalese urban environment. Annales de Cardiologie et d’Angéiologie. 2024 Jun; 73(3): 101767. |
| [6] | Ndiaye LH. Epidemiological, diagnostic, therapeutic, and prognostic aspects of ST-segment elevation acute coronary syndromes (STEMI) admitted beyond the 12th hour: a study of 50 cases collected from four cardiology departments in Dakar. PhD Thesis, Dakar El Hadji Ibrahima NIASSE University, 2023. |
[5, 6]
. While advancements in coronary reperfusion have enhanced ACS management and outcomes, the development of comprehensive national strategies in Senegal requires a thorough understanding of the epidemiology and unique challenges associated with ACS.
This systematic review and meta-analysis aim to assess the state of ACS management in Senegal, with the main objective of determining the prevalence of ACS and its evolution over the years.
The secondary objectives were to:
1) Describe the epidemiological characteristics of the patients and their progression over the years
2) Describe the management of ACS in Senegal and its evolution over the years
3) Determine the morbidity and mortality of ACS in Senegal and its evolution over the years.
2. Methods
We conducted an exclusively gray literature search focusing on thesis and dissertations related to ACS conducted in Senegalese public hospitals between 1990 and 2023 as the vast majority of peer-reviewed articles on the subject originate from these dissertations and thesis. Search was conducted on June 19, 2023, using the digital library of Cheikh Anta Diop University of Dakar and other public and private university medical libraries across Senegal.
We included observational studies conducted between 1998 and 2020 that focused on ACS, with or without persistent ST-segment elevation. Studies involving specific populations such as only men, women, young, or elderly individuals, reperfused or non-reperfused patients, diabetics, or those with angiographically healthy coronary arteries, were excluded.
The selection of studies was conducted by a single examiner (PMG), a fourth-year cardiology resident during the study. In case of uncertainty regarding a study's inclusion, the final decision was made by (MD), a professor of cardiology.
The data analyzed encompassed a range of factors, including epidemiological aspects, cardiovascular risk factors, transportation methods, admission delays, clinical presentation, coronary angiography performance, therapeutic data (reperfusion methods and adjunct therapies), and prognostic data (complications and in-hospital mortality).
We assessed the risk of bias in the included studies using the Loney scoring system, which evaluates the quality of prevalence or incidence studies. A score ≥5 indicates a high-quality study, whereas a score <5 suggests low quality
| [7] | Loney PL, Chambers LW, Bennett KJ, Roberts JG, Stratford PW. Critical appraisal of the health research literature: prevalence or incidence of a health problem. Chronic Dis Can. 1998; 19(4): 170-6. |
| [8] | Pourhoseingholi MA, Vahedi M, Rahimzadeh M. Sample size calculation in medical studies. Gastroenterology and Hepatology From Bed to Bench. 2013; 6(1): 14-7. |
[7, 8]
.
A meta-analysis was conducted to estimate the prevalence and mortality of ACS using OpenStat version 6.5, a statistical software based on R. The Freeman-Tukey double arcsine transformation was employed to stabilize the variance of proportions, and the DerSimonian- Laird random-effects model was used to pool the estimates
| [9] | Freeman MF, Tukey JW. Transformations Related to the Angular and the Square Root. The Annals of Mathematical Statistics. 1950; 21(4): 607-11. |
| [10] | DerSimonian R, Laird N. Meta-analysis in clinical trials. Controlled Clinical Trials. 1986; 7(3): 177-88. |
[9, 10]
. Confidence intervals for individual studies were determined using the score test, while those for pooled estimates were derived using Wald's test
| [11] | Nyaga VN, Arbyn M, Aerts M. Metaprop: a Stata command to perform meta-analysis of binomial data. Arch Public Health. 2014; 72(1): 39. |
[11]
. Heterogeneity among studies was assessed using the I² statistic
| [12] | Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003; 327(7414): 557-60. |
[12]
.
We conducted subgroup analysis based on location (Dakar vs. other regions between 2013 and 2020) and time periods for Dakar alone (Period 1: 1998–2010; Period 2: 2013–2020). A descriptive synthesis of the remaining data was also provided.
This systematic review adhered to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 guidelines. Since no human intervention was involved, no patient consent or ethics committee approval was required.
3. Results
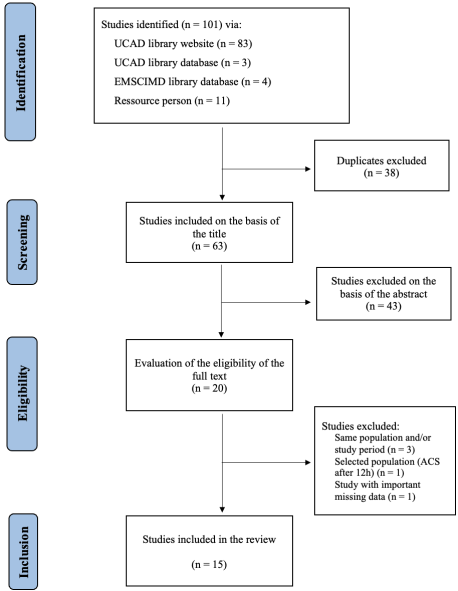
A total of 101 documents were identified, and 15 studies were ultimately included in the review. The flow diagram in
Figure 1 illustrates this selection process. Studies covered a period from 1998 to 2020. Ten studies addressed ACS broadly, while four focused specifically on ST-segment elevation myocardial infarction (STEMI) and one on non-ST-segment elevation ACS (NSTE-ACS). breakdown is further detailed in
Table 1.
Figure 1. Flow diagram of studies selection.
Table 1. Characteristics of studies included.
Author | Type of document | University | Study period | Type of study | Hospital | Study population | Patients included |
Ba | [13] | Ba A. Ischemic heart diseases: a prospective study of 69 cases collected at the cardiology clinic of Dakar. PhD Thesis, Dakar Cheikh Anta Diop University, 2002. |
[13] | Thesis | UCAD | 1998-2000 | Prospective | HALD | ACS | 68 |
Mboup | [14] | Mboup MC. Acute coronary syndromes: a multicenter prospective study of 59 cases collected in a in-hospital setting. PhD Thesis, Dakar Cheikh Anta Diop University, 2006. |
[14] | Thesis | UCAD | 2005-2006 | Prospective | HALD-HPD | ACS | 59 |
Diallo | [15] | Diallo MB. Diagnostic, therapeutic, and prognostic aspects of ST-segment elevation acute coronary syndromes: a retrospective study of 54 cases. PhD Thesis, Dakar Cheikh Anta Diop University, 2008. |
[15] | Thesis | UCAD | 2005-2007 | Retrospective | HOGIP | STEMI | 54 |
Hakim | [16] | Hakim Radwane. Diagnostic, therapeutic, and prognostic aspects of acute coronary syndromes with and without persistent ST-segment elevation: a retrospective study of 134 cases. PhD Thesis, Dakar Cheikh Anta Diop University, 2009. |
[16] | Thesis | UCAD | 2004-2008 | Retrospective | HOGIP | ACS | 134 |
Ndene | [17] | Ndene JMC. Non-ST-segment elevation acute coronary syndromes: epidemiological, clinical, therapeutic, and prognostic study at the cardiology clinic of Aristide Le Dantec Hospital in Dakar. PhD Thesis, Dakar Cheikh Anta Diop University, 2011. |
[17] | Thesis | UCAD | 2004-2010 | Retrospective | HALD | NSTE-ACS | 30 |
Savadogo | [18] | Savadogo S. Analysis of treatment delays and outcomes in the management of acute coronary syndromes at Grand-Yoff General Hospital: a retrospective study of 133 cases. Dissertation, Dakar Cheikh Anta Diop University, 2016. |
[18] | Dissertation | UCAD | 2013-2014 | Retrospective | HOGIP | ACS | 133 |
Samb | [19] | Samb C. Assessment of the management of ST-segment elevation acute coronary syndromes at Aristide Le Dantec university hospital in Dakar. Dissertation, Dakar Cheikh Anta Diop University, 2016. |
[19] | Dissertation | UCAD | 2014-2015 | Retrospective | HALD | STEMI | 40 |
Loum | [20] | Loum MD. Diagnostic, therapeutic, and prognostic aspects of ST-segment elevation acute coronary syndromes at Grand Yoff General Hospital: a retrospective analysis of 164 cases. PhD Thesis, Dakar Cheikh Anta Diop University, 2017. |
[20] | Thesis | UCAD | 2013-2015 | Retrospective | HOGIP | STEMI | 164 |
Dieye | [21] | Dièye M. Short- and mid-term evaluation of acute coronary syndromes: a longitudinal study of 100 cases at the cardiology department of Grand Yoff General Hospital in Dakar. PhD Thesis, Dakar Cheikh Anta Diop University, 2018. |
[21] | Thesis | UCAD | 2016 | Prospective | HOGIP | ACS | 100 |
Sene | [22] | Sène Fama. Prevalence and management of hyperglycemic states during acute coronary syndromes: a retrospective study of 141 cases at the cardiology department of Grand Yoff General Hospital. PhD Thesis, Dakar Cheikh Anta Diop University, 2018. |
[22] | Thesis | UCAD | 2016-2018 | Retrospective | HOGIP | ACS | 141 |
Ibouroi | [23] | Ismael Ibouroi MH. Acute coronary syndromes: diagnostic, therapeutic, and outcome aspects at Aristide Le Dantec Hospital, about 343 cases. PhD Thesis, Dakar Cheikh Anta Diop University, 2021. |
[23] | Thesis | UCAD | 2019-2020 | Retrospective | HALD | ACS | 343 |
Sabaly | [24] | Sabaly A. Management of ST-segment elevation acute coronary syndromes at the El Hadji Ibrahima Niass Regional Hospital Center in Kaolack: a retrospective study of 40 cases. PhD Thesis, Dakar Cheikh Anta Diop University, 2019. |
[24] | Thesis | UCAD | 2014-2017 | Retrospective | CHREINK | STEMI | 40 |
Mbaye | [25] | Mbaye MD. Epidemiological, clinical, paraclinical, therapeutic, and outcome aspects of acute coronary syndromes in the city of Ziguinchor: a cross-sectional and descriptive study of 57 cases. PhD Thesis, Ziguinchor Assane Seck University, 2020. |
[25] | Thesis | UAAS | 2016-2019 | Retrospective | CHRZ - HPZ | ACS | 57 |
Ndao | [26] | Ndao I. Acute coronary syndromes: clinical, electrocardiographic, echocardiographic, and outcome aspects in Saint-Louis based on 47 cases. PhD Thesis, Saint-Louis Gaston Berger University, 2020. |
[26] | Thesis | UGB | 2018-2019 | Retrospective | CHRSL | ACS | 47 |
Akouete | [27] | Akouètè JPD. Management of acute coronary syndromes: epidemiological, diagnostic, and therapeutic aspects at Saint-Jean de Dieu Hospital in Thiès. PhD Thesis, Thiès: Iba Der Thiam University, 2020. |
[27] | Thesis | UIDT | 2018-2019 | Prospective | HSJDT | ACS | 29 |
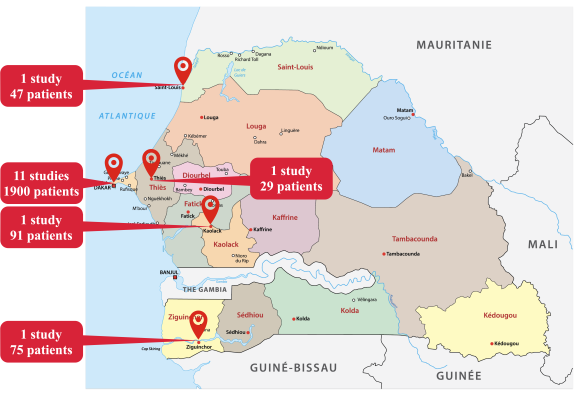
The studies were conducted in Dakar and four other regions: Ziguinchor, Thies, Saint-Louis, and Kaolack as illustrated in
Figure 2. Thirteen studies were deemed high quality based on the Loney scoring system represented in
table 2.
Figure 2. Distribution of studies by region of Senegal.
Table 2. Quality bias assessment according to Loney’s criteria. Green crosses indicate the fulfilled criteria.
| Random sample | Unbiased sampling | Adequate size | Validated criteria | Unbiased interviewers | Response rate | Confidence interval, Subgroup analysis | Subjects description |
Ba | [13] | Ba A. Ischemic heart diseases: a prospective study of 69 cases collected at the cardiology clinic of Dakar. PhD Thesis, Dakar Cheikh Anta Diop University, 2002. |
[13] | X | X | | X | X | X | | X |
Mboup | [14] | Mboup MC. Acute coronary syndromes: a multicenter prospective study of 59 cases collected in a in-hospital setting. PhD Thesis, Dakar Cheikh Anta Diop University, 2006. |
[14] | X | X | | X | X | X | | X |
Diallo | [15] | Diallo MB. Diagnostic, therapeutic, and prognostic aspects of ST-segment elevation acute coronary syndromes: a retrospective study of 54 cases. PhD Thesis, Dakar Cheikh Anta Diop University, 2008. |
[15] | X | X | | X | X | X | | X |
Hakim | [16] | Hakim Radwane. Diagnostic, therapeutic, and prognostic aspects of acute coronary syndromes with and without persistent ST-segment elevation: a retrospective study of 134 cases. PhD Thesis, Dakar Cheikh Anta Diop University, 2009. |
[16] | | | X | X | X | | | X |
Ndene | [17] | Ndene JMC. Non-ST-segment elevation acute coronary syndromes: epidemiological, clinical, therapeutic, and prognostic study at the cardiology clinic of Aristide Le Dantec Hospital in Dakar. PhD Thesis, Dakar Cheikh Anta Diop University, 2011. |
[17] | X | X | | X | X | X | | X |
Savadogo | [18] | Savadogo S. Analysis of treatment delays and outcomes in the management of acute coronary syndromes at Grand-Yoff General Hospital: a retrospective study of 133 cases. Dissertation, Dakar Cheikh Anta Diop University, 2016. |
[18] | | | | X | X | | | X |
Samb | [19] | Samb C. Assessment of the management of ST-segment elevation acute coronary syndromes at Aristide Le Dantec university hospital in Dakar. Dissertation, Dakar Cheikh Anta Diop University, 2016. |
[19] | X | X | | | X | X | | X |
Loum | [20] | Loum MD. Diagnostic, therapeutic, and prognostic aspects of ST-segment elevation acute coronary syndromes at Grand Yoff General Hospital: a retrospective analysis of 164 cases. PhD Thesis, Dakar Cheikh Anta Diop University, 2017. |
[20] | X | X | | X | X | X | | X |
Dieye | [21] | Dièye M. Short- and mid-term evaluation of acute coronary syndromes: a longitudinal study of 100 cases at the cardiology department of Grand Yoff General Hospital in Dakar. PhD Thesis, Dakar Cheikh Anta Diop University, 2018. |
[21] | X | X | | X | X | X | | X |
Sene | [22] | Sène Fama. Prevalence and management of hyperglycemic states during acute coronary syndromes: a retrospective study of 141 cases at the cardiology department of Grand Yoff General Hospital. PhD Thesis, Dakar Cheikh Anta Diop University, 2018. |
[22] | X | X | | X | X | X | | X |
Ibouroi | [23] | Ismael Ibouroi MH. Acute coronary syndromes: diagnostic, therapeutic, and outcome aspects at Aristide Le Dantec Hospital, about 343 cases. PhD Thesis, Dakar Cheikh Anta Diop University, 2021. |
[23] | X | X | X | X | X | X | | X |
Sabaly | [24] | Sabaly A. Management of ST-segment elevation acute coronary syndromes at the El Hadji Ibrahima Niass Regional Hospital Center in Kaolack: a retrospective study of 40 cases. PhD Thesis, Dakar Cheikh Anta Diop University, 2019. |
[24] | X | X | | X | X | X | | X |
Mbaye | [25] | Mbaye MD. Epidemiological, clinical, paraclinical, therapeutic, and outcome aspects of acute coronary syndromes in the city of Ziguinchor: a cross-sectional and descriptive study of 57 cases. PhD Thesis, Ziguinchor Assane Seck University, 2020. |
[25] | X | X | | X | X | X | | X |
Ndao | [26] | Ndao I. Acute coronary syndromes: clinical, electrocardiographic, echocardiographic, and outcome aspects in Saint-Louis based on 47 cases. PhD Thesis, Saint-Louis Gaston Berger University, 2020. |
[26] | X | X | | X | X | X | | X |
Akouete | [27] | Akouètè JPD. Management of acute coronary syndromes: epidemiological, diagnostic, and therapeutic aspects at Saint-Jean de Dieu Hospital in Thiès. PhD Thesis, Thiès: Iba Der Thiam University, 2020. |
[27] | X | X | | X | X | X | | X |
3.1. Epidemiological Data
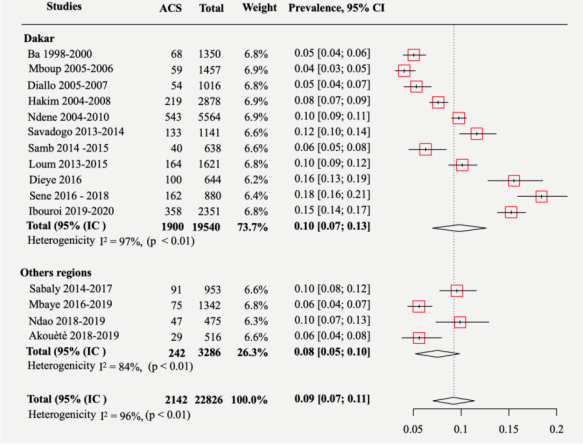
The overall prevalence was 9% (95% CI: 7–11%, I² = 96%, p < 0.01), as shown in
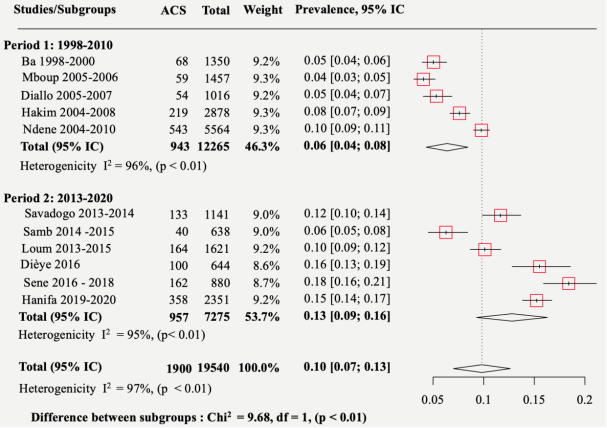
Figure 3. In Dakar, prevalence gradually increased, with a significant difference between period 1 (1998–2010) and period 2 (2013–2020) (p < 0.01), rising from 6% (95% CI: 4–8%, I² = 96%, p < 0.01) to 13% (95% CI: 9–16%, I² = 95%, p < 0.01) as represented in
figure 4.
Figure 3. Overall prevalence.
Figure 4. Prevalence difference in Dakar between 2 periods (1998-2010) and (2013-2020).
All but one study found a predominance of STEMI, with its frequency ranging from 44 to 94%. The mean age of patients ranged from 57.1 to 64 years. Across all studies, there was a male predominance, with the proportion of men ranging from 51 to 79%.
The prevalence of hypertension ranged from 47.5 to 69%; diabetes from 15 to 41.3%; obesity from 6.9 to 40.7%; smoking from 14 to 60%; physical inactivity from 12.5 to 96.5%; and a family history of cardiovascular disease from 2.5 to 6.1%.
3.2. Diagnostic Data
In Dakar, the average admission time to the cardiology department decreased significantly from 186 hours in 2002 to 28 hours in 2018. In other regions, the average admission time varied: 47 hours in Kaolack, 81.6 hours in Ziguinchor, 50 hours in Saint-Louis, and 31 hours in Thies.
In Dakar, the percentage of STEMI patients admitted within 12 hours of pain onset ranged from 42.5 to 72.3%. In other regions, this percentage was 37.5% in Kaolack, 32.5% in Ziguinchor, 66% in Saint-Louis and 58% in Thies.
Four studies analyzed transport methods, showing that the proportion of patients transported by ambulance ranged from 1.9 to 30%. The proportion of patients experiencing typical anginal chest pain varied between 36.6 and 95%.
In Dakar, the use of coronary angiography increased from 0 to 60.6% between 1998 and 2020. In other regions, no patients underwent coronary angiography during hospitalization.
3.3. Therapeutic Data
In Dakar, the proportion of STEMI patients who received thrombolysis ranged from 2.1 to 64.8%. The average thrombolysis time varied between 5.2 and 6.3 hours, with a success rate of 49 to 62.7%. In other regions, the percentage of patients who received thrombolysis was 10% in Kaolack (with an average time of 3.8 hours), 53.8% in Saint-Louis (6 hours), and 52.6% in Thiès (5.6 hours). In Ziguinchor, no patients received thrombolysis.
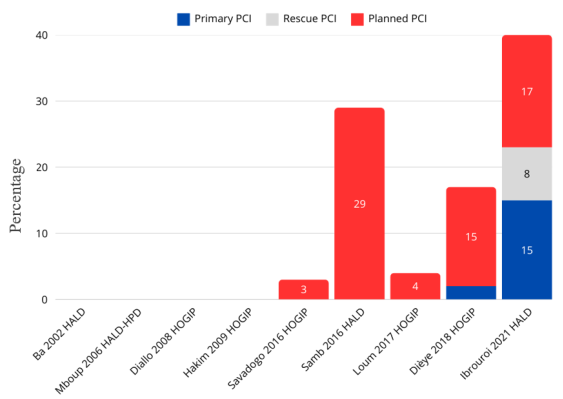
Streptokinase was the only thrombolytic agent used in all studies, except for the most recent study in Dakar, where four patients were treated with tenecteplase. No patients in other regions underwent angioplasty during hospitalization. In Dakar, the percentage of percutaneous coronary intervention (PCI) increased from 4.3% to 35.3%, with primary PCI performed only in the latest study as shown in
Figure 5. Across all studies, no patients underwent coronary artery bypass grafting during hospitalization.
Figure 5. Distribution of different types of PCI.
The use of parenteral anticoagulants ranged from 63.2 to 100%. Antiplatelet agents were prescribed in 59.7 to 100% of patients. Statins were administered to between 54.2 and 100% of patients, while beta-blockers were prescribed in 57.9 to 88.3% of cases. Renin-angiotensin-aldosterone system blockers were also commonly used, with prescription rates ranging from 63.2 to 96.6%.
In Dakar, the average hospital stay for patients significantly decreased from 20.2 days in 1998 to 7 days in 2020. In other regions, the average length of stay ranged from 5 to 8.5 days.
3.4. Prognostic Data
The frequency of complications varied as follows:
1) Heart failure: 6.7 to 52.9%
2) Cardiogenic shock: 1 to 18.5%
3) Atrial fibrillation: 0 to 13.4%
4) Severe ventricular arrhythmias: 0 to 6.7%
5) Significant atrioventricular conduction block: 0 to 8.5%
6) Left ventricular thrombus: 0 to 20.3%
7) Hemorrhages: 2 to 6.7%
Notably, most of these complications have decreased in frequency over time.
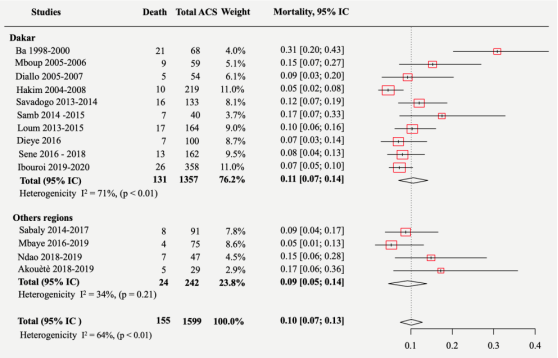
The overall mortality rate was 10% (95% CI: 7–13%, I² = 64%, p < 0.01), as illustrated in
figure 6. In Dakar, mortality decreased over time, but there was no significant difference between period 1 and period 2 (p = 0.31). The mortality rate was 14% (95% CI: 3–25%, I² = 88%, p < 0.01) between 1998 and 2010 and 9% (95% CI: 9–16%, I² = 11%, p = 0.34) between 2013 and 2020.
Figure 6. Overall mortality.
4. Discussion
In sub-Saharan Africa, existing data on CAD suggest that it is one of the three leading causes of death
| [4] | Yao H, Ekou A, Niamkey T, Hounhoui Gan S, Kouamé I, Afassinou Y, et al. Acute Coronary Syndromes in Sub‐Saharan Africa: A 10‐Year Systematic Review. Journal of the American Heart Association. 2022; 11(1): e021107. |
[4]
. These data are primarily based on hospital surveys of ACS, whose frequency is steadily increasing. Indeed, the prevalence rose from 3.17% in 1991 in the multicenter prospective CORONAFRIC-I study
| [28] | Ticolat P, Bertrand E, Longo-Mbenza, Monkam Y, Motte, Diouf S et al. Epidemiological aspects of coronary artery disease in Black Africans: a study of 103 cases. Results from the prospective multicenter CORONAFRIC survey. Cardiol trop. 1991; 17: 7-20. |
[28]
, which covered 11 sub-Saharan African countries, to 16% in the CORONAFRIC-II study
| [29] | Kassé Maryam. Coronary artery disease in Africa: results of the multicenter CORONAFRIC II survey conducted in 11 sub-Saharan African countries. PhD Thesis, Dakar Cheikh Anta Diop University, 2016. |
[29]
in 2017.
In Ivory Coast according to one study
| [30] | Yao H, Ekou A, Brou I, Niamkey T, Koffi F, Tano S et al. Trends in the epidemiology and management of acute coronary syndromes in Abidjan: a cross-sectional study of 1,011 patients. Annales de Cardiologie et d’Angéiologie. 2022; 71(3): 130-5. |
[30]
, prevalence increased from 7.3% between 2002 and 2009 to 22.6% between 2010 and 2016. Senegal is no exception to this trend, as evidenced by our findings. In Dakar, prevalence doubled between period 1 (1998–2010) and period 2 (2013–2020). A more recent study reported an even higher prevalence of 22% in four public hospitals in Dakar in 2022
| [6] | Ndiaye LH. Epidemiological, diagnostic, therapeutic, and prognostic aspects of ST-segment elevation acute coronary syndromes (STEMI) admitted beyond the 12th hour: a study of 50 cases collected from four cardiology departments in Dakar. PhD Thesis, Dakar El Hadji Ibrahima NIASSE University, 2023. |
[6]
.
This rise in ACS prevalence is partly due to significant lifestyle changes that promote cardiovascular risk factors and partly to improvements in diagnostic methods. A paradigm shift in the fight against cardiovascular diseases is therefore essential to reduce their incidence and associated morbidity and mortality.
Overall, the relative incidences of STEMI and NSTEMI are decreasing and increasing, respectively. In France, for example, the proportion of NSTEMI cases in the FAST-MI registry
| [31] | Puymirat E, Simon T, Cayla G, Cottin Y, Elbaz M, Coste P et al. Acute Myocardial Infarction: Changes in Patient Characteristics, Management, and 6-Month Outcomes Over a Period of 20 Years in the FAST-MI Program (French Registry of Acute ST-Elevation or Non-ST-Elevation Myocardial Infarction) 1995 to 2015. Circulation. 2017; 136(20): 1908-19. |
[31]
rose from one-third in 1995 to more than half in 2015. This shift is primarily due to improved diagnosis of NSTEMI, particularly with the advent of high-sensitivity troponin assays and modern cardiac imaging techniques.
In Senegal, although there has been a slight increase in the proportion of NSTEMI cases over the years, as evidenced by our study, STEMI remains significantly more prevalent. Similar findings have been reported across sub-Saharan Africa, where, according to a systematic review by Yao et al.
| [4] | Yao H, Ekou A, Niamkey T, Hounhoui Gan S, Kouamé I, Afassinou Y, et al. Acute Coronary Syndromes in Sub‐Saharan Africa: A 10‐Year Systematic Review. Journal of the American Heart Association. 2022; 11(1): e021107. |
[4]
, STEMI is the predominant clinical presentation in most studies.
In France, the median delay between symptom onset and hospital admission for STEMI decreased from 240 minutes in 1995 to 168 minutes in 2015, according to the FAST-MI registry
| [31] | Puymirat E, Simon T, Cayla G, Cottin Y, Elbaz M, Coste P et al. Acute Myocardial Infarction: Changes in Patient Characteristics, Management, and 6-Month Outcomes Over a Period of 20 Years in the FAST-MI Program (French Registry of Acute ST-Elevation or Non-ST-Elevation Myocardial Infarction) 1995 to 2015. Circulation. 2017; 136(20): 1908-19. |
[31]
. In Africa, however, admission delays are significantly longer than in Western countries. Yao et al., in their systematic review, found that the average time to admission in cardiology units ranged from 2.3 hours in South Africa to 6.6 days in Tanzania
| [4] | Yao H, Ekou A, Niamkey T, Hounhoui Gan S, Kouamé I, Afassinou Y, et al. Acute Coronary Syndromes in Sub‐Saharan Africa: A 10‐Year Systematic Review. Journal of the American Heart Association. 2022; 11(1): e021107. |
[4]
.
In Senegal, particularly in Dakar, the average admission delay has significantly decreased, from 186 hours in 2002 to 28 hours in 2018, according to our findings. However, this delay remains well above the recommended delays. Several factors contribute to these prolonged delays, including:
1) Limited public awareness of ACS symptoms, leading to late healthcare-seeking behavior in both prehospital and hospital settings.
2) Unavailability of electrocardiograms in some healthcare facilities, causing diagnostic delays.
3) An inadequately structured prehospital transport system.
Our study observed a significant increase in the use of coronary angiography and PCI among patients hospitalized for ACS. This intervention only began routinely in 2013 in Dakar’s public hospitals. Primary PCI was first performed in the most recent study conducted at HALD between 2019 and 2020
| [23] | Ismael Ibouroi MH. Acute coronary syndromes: diagnostic, therapeutic, and outcome aspects at Aristide Le Dantec Hospital, about 343 cases. PhD Thesis, Dakar Cheikh Anta Diop University, 2021. |
[23]
. However, it was performed more frequently than scheduled angioplasty, accounting for 17.8% of all STEMI patients.
These findings contrast with those from European countries. For example, in France, according to the FAST-MI registry, the proportion of patients undergoing coronary angiography was 99% in 2015, while the percentage of STEMI patients receiving primary PCI increased from 12% in 1995 to 76% in 2015
| [31] | Puymirat E, Simon T, Cayla G, Cottin Y, Elbaz M, Coste P et al. Acute Myocardial Infarction: Changes in Patient Characteristics, Management, and 6-Month Outcomes Over a Period of 20 Years in the FAST-MI Program (French Registry of Acute ST-Elevation or Non-ST-Elevation Myocardial Infarction) 1995 to 2015. Circulation. 2017; 136(20): 1908-19. |
[31]
. According to the 2022 France PCI annual report, this percentage further rose to 89.8%
.
The primary reasons for this discrepancy are financial and organizational. Financially, coronary angiography is costly in Senegal, as it is a paid procedure. The cost of a diagnostic coronary angiography in most hospitals is 500,000 CFA francs (approximately 800 US dollars), whereas the Guaranteed inter-professional minimum wage in the country does not exceed 65,000 CFA francs (about 100 US dollars)
.
Organizationally, there is still no well-structured ACS management network, leading to prolonged intervention delays.
Globally, improved ACS management—particularly through thrombolysis and coronary angioplasty—has contributed to reduced mortality rates. For instance, in France, the 30-day mortality rate for STEMI decreased from 14% to 3% between 1995 and 2015
| [31] | Puymirat E, Simon T, Cayla G, Cottin Y, Elbaz M, Coste P et al. Acute Myocardial Infarction: Changes in Patient Characteristics, Management, and 6-Month Outcomes Over a Period of 20 Years in the FAST-MI Program (French Registry of Acute ST-Elevation or Non-ST-Elevation Myocardial Infarction) 1995 to 2015. Circulation. 2017; 136(20): 1908-19. |
[31]
. In sub-Saharan Africa, although mortality remains high, there is a decreasing trend
| [30] | Yao H, Ekou A, Brou I, Niamkey T, Koffi F, Tano S et al. Trends in the epidemiology and management of acute coronary syndromes in Abidjan: a cross-sectional study of 1,011 patients. Annales de Cardiologie et d’Angéiologie. 2022; 71(3): 130-5. |
[30]
.
In Senegal, specifically in Dakar, we observed a reduction in mortality rates from 14% in 1998–2010 to 9% in 2013–2020, although this decline was not statistically significant.
However, our study has certain limitations, including:
1) Literature screening and data extraction performed by a single reviewer
2) The limited number of studies conducted in regions outside Dakar.
3) The absence of studies in major hospitals such as the National University Hospital Center of Fann and the Dalal Jamm National Hospital Center.
4) The lack of recent studies (2021–2023) covering ACS as a whole, with most recent research focusing on specific aspects like coronary reperfusion techniques.
5. Conclusion
Our study has provided comprehensive data on the evolving epidemiology and management of ACS. It could serve as a starting point for further research into the burden of ACS in our country. The findings highlight that while the implementation of well-established ACS management guidelines remains a significant challenge, there has been notable progress over the years.
Key areas for improvement include:
1) Establishing a national ACS registry to obtain more reliable data on epidemiology, treatment delays, and patient outcomes with the following key steps: define objectives, standardize case definitions and inclusion criteria, design data collection tools, select participating centers, train healthcare staff, implement data management system, ensure ethical compliance, pilot and monitor the registry, use and disseminate results.
2) Developing an ACS care network linking peripheral healthcare facilities with PCI-equipped centers through an efficient emergency medical system.
Abbreviations
ACS | Acute Coronary Syndromes |
CAD | Coronary Artery Disease |
CHREINK | Centre Hospitalier Régional El Hadji Ibrahima Niasse de Kaolack |
CHRSL | Centre Hospitalier Régional de Saint-Louis |
CHRZ | Centre Hospitalier Régional de Ziguinchor |
HALD | Hôpital Aristide Le Dantec |
HOGIP | Hôpital Général Idrissa Pouye |
HPD | Hôpital Principal de Dakar |
HPZ | Hôpital de la Paix de Ziguinchor |
HSJDT | Hôpital Saint Jean De Dieu de Thiès |
NSTE-ACS | Non-ST-segment Elevation Acute Coronary Syndromes |
PCI | Percutaneous Coronary Intervention |
PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
STEMI | ST-segment Elevation Myocardial Infarction |
UAAS | Université Amadou Assane Seck |
UCAD | Université Cheikh Anta Diop de Dakar |
UGB | Université Gaston Berger |
UIDT | Université Iba Der Thiam de Thiès |
WHO | World Health Organization |
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Byrne RA, Rossello X, Coughlan JJ, Barbato E, Berry C, Chieffo A et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023; ehad191.
|
| [2] |
World Health Organisation. The top 1à causes of death. Available from:
https://www.who.int/fr/news-room/fact-sheets/detail/the-top-10-causes-of-death
[Accessed 02 January 2024]
|
| [3] |
France PCI. France PCI registry presentation. Available from:
https://www.francepci.com/
[Accessed 02 janvier 2024].
|
| [4] |
Yao H, Ekou A, Niamkey T, Hounhoui Gan S, Kouamé I, Afassinou Y, et al. Acute Coronary Syndromes in Sub‐Saharan Africa: A 10‐Year Systematic Review. Journal of the American Heart Association. 2022; 11(1): e021107.
|
| [5] |
Guissé PM, Sall SAB, Niang T, Doucouré TS, Mboup MC, Ngaïdé AA and al. Acute coronary syndromes in diabetes mellitus: A comparative study between diabetics and non-diabetics patients in Senegalese urban environment. Annales de Cardiologie et d’Angéiologie. 2024 Jun; 73(3): 101767.
|
| [6] |
Ndiaye LH. Epidemiological, diagnostic, therapeutic, and prognostic aspects of ST-segment elevation acute coronary syndromes (STEMI) admitted beyond the 12th hour: a study of 50 cases collected from four cardiology departments in Dakar. PhD Thesis, Dakar El Hadji Ibrahima NIASSE University, 2023.
|
| [7] |
Loney PL, Chambers LW, Bennett KJ, Roberts JG, Stratford PW. Critical appraisal of the health research literature: prevalence or incidence of a health problem. Chronic Dis Can. 1998; 19(4): 170-6.
|
| [8] |
Pourhoseingholi MA, Vahedi M, Rahimzadeh M. Sample size calculation in medical studies. Gastroenterology and Hepatology From Bed to Bench. 2013; 6(1): 14-7.
|
| [9] |
Freeman MF, Tukey JW. Transformations Related to the Angular and the Square Root. The Annals of Mathematical Statistics. 1950; 21(4): 607-11.
|
| [10] |
DerSimonian R, Laird N. Meta-analysis in clinical trials. Controlled Clinical Trials. 1986; 7(3): 177-88.
|
| [11] |
Nyaga VN, Arbyn M, Aerts M. Metaprop: a Stata command to perform meta-analysis of binomial data. Arch Public Health. 2014; 72(1): 39.
|
| [12] |
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003; 327(7414): 557-60.
|
| [13] |
Ba A. Ischemic heart diseases: a prospective study of 69 cases collected at the cardiology clinic of Dakar. PhD Thesis, Dakar Cheikh Anta Diop University, 2002.
|
| [14] |
Mboup MC. Acute coronary syndromes: a multicenter prospective study of 59 cases collected in a in-hospital setting. PhD Thesis, Dakar Cheikh Anta Diop University, 2006.
|
| [15] |
Diallo MB. Diagnostic, therapeutic, and prognostic aspects of ST-segment elevation acute coronary syndromes: a retrospective study of 54 cases. PhD Thesis, Dakar Cheikh Anta Diop University, 2008.
|
| [16] |
Hakim Radwane. Diagnostic, therapeutic, and prognostic aspects of acute coronary syndromes with and without persistent ST-segment elevation: a retrospective study of 134 cases. PhD Thesis, Dakar Cheikh Anta Diop University, 2009.
|
| [17] |
Ndene JMC. Non-ST-segment elevation acute coronary syndromes: epidemiological, clinical, therapeutic, and prognostic study at the cardiology clinic of Aristide Le Dantec Hospital in Dakar. PhD Thesis, Dakar Cheikh Anta Diop University, 2011.
|
| [18] |
Savadogo S. Analysis of treatment delays and outcomes in the management of acute coronary syndromes at Grand-Yoff General Hospital: a retrospective study of 133 cases. Dissertation, Dakar Cheikh Anta Diop University, 2016.
|
| [19] |
Samb C. Assessment of the management of ST-segment elevation acute coronary syndromes at Aristide Le Dantec university hospital in Dakar. Dissertation, Dakar Cheikh Anta Diop University, 2016.
|
| [20] |
Loum MD. Diagnostic, therapeutic, and prognostic aspects of ST-segment elevation acute coronary syndromes at Grand Yoff General Hospital: a retrospective analysis of 164 cases. PhD Thesis, Dakar Cheikh Anta Diop University, 2017.
|
| [21] |
Dièye M. Short- and mid-term evaluation of acute coronary syndromes: a longitudinal study of 100 cases at the cardiology department of Grand Yoff General Hospital in Dakar. PhD Thesis, Dakar Cheikh Anta Diop University, 2018.
|
| [22] |
Sène Fama. Prevalence and management of hyperglycemic states during acute coronary syndromes: a retrospective study of 141 cases at the cardiology department of Grand Yoff General Hospital. PhD Thesis, Dakar Cheikh Anta Diop University, 2018.
|
| [23] |
Ismael Ibouroi MH. Acute coronary syndromes: diagnostic, therapeutic, and outcome aspects at Aristide Le Dantec Hospital, about 343 cases. PhD Thesis, Dakar Cheikh Anta Diop University, 2021.
|
| [24] |
Sabaly A. Management of ST-segment elevation acute coronary syndromes at the El Hadji Ibrahima Niass Regional Hospital Center in Kaolack: a retrospective study of 40 cases. PhD Thesis, Dakar Cheikh Anta Diop University, 2019.
|
| [25] |
Mbaye MD. Epidemiological, clinical, paraclinical, therapeutic, and outcome aspects of acute coronary syndromes in the city of Ziguinchor: a cross-sectional and descriptive study of 57 cases. PhD Thesis, Ziguinchor Assane Seck University, 2020.
|
| [26] |
Ndao I. Acute coronary syndromes: clinical, electrocardiographic, echocardiographic, and outcome aspects in Saint-Louis based on 47 cases. PhD Thesis, Saint-Louis Gaston Berger University, 2020.
|
| [27] |
Akouètè JPD. Management of acute coronary syndromes: epidemiological, diagnostic, and therapeutic aspects at Saint-Jean de Dieu Hospital in Thiès. PhD Thesis, Thiès: Iba Der Thiam University, 2020.
|
| [28] |
Ticolat P, Bertrand E, Longo-Mbenza, Monkam Y, Motte, Diouf S et al. Epidemiological aspects of coronary artery disease in Black Africans: a study of 103 cases. Results from the prospective multicenter CORONAFRIC survey. Cardiol trop. 1991; 17: 7-20.
|
| [29] |
Kassé Maryam. Coronary artery disease in Africa: results of the multicenter CORONAFRIC II survey conducted in 11 sub-Saharan African countries. PhD Thesis, Dakar Cheikh Anta Diop University, 2016.
|
| [30] |
Yao H, Ekou A, Brou I, Niamkey T, Koffi F, Tano S et al. Trends in the epidemiology and management of acute coronary syndromes in Abidjan: a cross-sectional study of 1,011 patients. Annales de Cardiologie et d’Angéiologie. 2022; 71(3): 130-5.
|
| [31] |
Puymirat E, Simon T, Cayla G, Cottin Y, Elbaz M, Coste P et al. Acute Myocardial Infarction: Changes in Patient Characteristics, Management, and 6-Month Outcomes Over a Period of 20 Years in the FAST-MI Program (French Registry of Acute ST-Elevation or Non-ST-Elevation Myocardial Infarction) 1995 to 2015. Circulation. 2017; 136(20): 1908-19.
|
| [32] |
Senegalese Press Agency. Here is the new decree setting the minimum wage and the guaranteed minimum agricultural wage. Available from:
https://aps.sn/voici-le-nouveau-decret-fixant-le-smig-et-le-smag/
[Accessed 30 September 2023].
|
Cite This Article
-
APA Style
Momar, G. P., Cheikh, N. S., Salvador, M. J., Nguirane, N. P., Oumar, B., et al. (2025). Epidemiology, Management and Prognosis of Acute Coronary Syndromes in Senegal: A Systematic Review of the Grey Literature with Meta-analysis from 1998 to 2020. Cardiology and Cardiovascular Research, 9(2), 54-63. https://doi.org/10.11648/j.ccr.20250902.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Momar, G. P.; Cheikh, N. S.; Salvador, M. J.; Nguirane, N. P.; Oumar, B., et al. Epidemiology, Management and Prognosis of Acute Coronary Syndromes in Senegal: A Systematic Review of the Grey Literature with Meta-analysis from 1998 to 2020. Cardiol. Cardiovasc. Res. 2025, 9(2), 54-63. doi: 10.11648/j.ccr.20250902.13
Copy
|
Download
AMA Style
Momar GP, Cheikh NS, Salvador MJ, Nguirane NP, Oumar B, et al. Epidemiology, Management and Prognosis of Acute Coronary Syndromes in Senegal: A Systematic Review of the Grey Literature with Meta-analysis from 1998 to 2020. Cardiol Cardiovasc Res. 2025;9(2):54-63. doi: 10.11648/j.ccr.20250902.13
Copy
|
Download
-
@article{10.11648/j.ccr.20250902.13,
author = {Guissé Papa Momar and Ndao Serigne Cheikh and Mingou Joseph Salvador and Ndiaye Papa Nguirane and Bassoum Oumar and Niang Tacko and Mboup Mouhamed Cherif and Sarr Simon Antoine and Ngaïdé Aliou Alassane and Diao Maboury and Diack Bouna and Dioum Momar},
title = {Epidemiology, Management and Prognosis of Acute Coronary Syndromes in Senegal: A Systematic Review of the Grey Literature with Meta-analysis from 1998 to 2020
},
journal = {Cardiology and Cardiovascular Research},
volume = {9},
number = {2},
pages = {54-63},
doi = {10.11648/j.ccr.20250902.13},
url = {https://doi.org/10.11648/j.ccr.20250902.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20250902.13},
abstract = {Introduction: The management of acute coronary syndromes (ACS) in Senegal continues to pose challenges, despite significant progress in medical care. To comprehensively understand the current state of ACS in Senegal, a systematic review with meta-analysis was deemed essential. The main objective of this study was to determine the prevalence of ACS in Senegal and its trajectory over time. Methods: A systematic review of grey literature, encompassing theses and dissertations on ACS conducted in public hospitals in Senegal between 1990 and 2023, was undertaken. The selected studies provided valuable insights into the prevalence, epidemiological characteristics, cardiovascular risk factors, diagnostic approaches, therapeutic interventions, and prognostic outcomes associated with ACS. A meta-analysis of prevalence and mortality data was performed using the DerSimonian-Laird random-effects model, while the remaining data were synthesized descriptively. Results: The systematic review yielded 15 eligible studies from 1998 to 2020, out of an initial 101 identified documents. The overall prevalence of ACS was determined to be 9% (95% Cl: 7-11%, 12 = 96%, p 2 = 96%, p 2 = 95%, p 2 = 64%, p Conclusion: Our study demonstrates that despite an increase in prevalence, there is an improvement in the management of ACS. However, the establishment of a national registry and a comprehensive network for ACS management is crucial to further improve morbidity and mortality outcomes.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Epidemiology, Management and Prognosis of Acute Coronary Syndromes in Senegal: A Systematic Review of the Grey Literature with Meta-analysis from 1998 to 2020
AU - Guissé Papa Momar
AU - Ndao Serigne Cheikh
AU - Mingou Joseph Salvador
AU - Ndiaye Papa Nguirane
AU - Bassoum Oumar
AU - Niang Tacko
AU - Mboup Mouhamed Cherif
AU - Sarr Simon Antoine
AU - Ngaïdé Aliou Alassane
AU - Diao Maboury
AU - Diack Bouna
AU - Dioum Momar
Y1 - 2025/06/18
PY - 2025
N1 - https://doi.org/10.11648/j.ccr.20250902.13
DO - 10.11648/j.ccr.20250902.13
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 54
EP - 63
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20250902.13
AB - Introduction: The management of acute coronary syndromes (ACS) in Senegal continues to pose challenges, despite significant progress in medical care. To comprehensively understand the current state of ACS in Senegal, a systematic review with meta-analysis was deemed essential. The main objective of this study was to determine the prevalence of ACS in Senegal and its trajectory over time. Methods: A systematic review of grey literature, encompassing theses and dissertations on ACS conducted in public hospitals in Senegal between 1990 and 2023, was undertaken. The selected studies provided valuable insights into the prevalence, epidemiological characteristics, cardiovascular risk factors, diagnostic approaches, therapeutic interventions, and prognostic outcomes associated with ACS. A meta-analysis of prevalence and mortality data was performed using the DerSimonian-Laird random-effects model, while the remaining data were synthesized descriptively. Results: The systematic review yielded 15 eligible studies from 1998 to 2020, out of an initial 101 identified documents. The overall prevalence of ACS was determined to be 9% (95% Cl: 7-11%, 12 = 96%, p 2 = 96%, p 2 = 95%, p 2 = 64%, p Conclusion: Our study demonstrates that despite an increase in prevalence, there is an improvement in the management of ACS. However, the establishment of a national registry and a comprehensive network for ACS management is crucial to further improve morbidity and mortality outcomes.
VL - 9
IS - 2
ER -
Copy
|
Download