The use of cardiopulmonary bypass in coronary artery bypass grafting (CABG) surgery can lead to red blood cell damage (hemolysis). Postoperative arrhythmias, such as atrial fibrillation, are frequent and serious complications after CABG. However, the relationship between the hemolysis that occurs during the surgery intraoperative hemolysis and the subsequent development of arrhythmias is not well-understood. This study will examine the connection between the level of IOH and the incidence of cardiac rhythm disturbances in patients with coronary artery disease who have undergone CABG surgery. The mechanisms causing arrhythmias after CABG are complex and involve various factors including changes in blood flow, the damage caused by restoring blood flow after cardiopulmonary bypass, and oxidative stress. Clarifying the role of surgery intraoperative hemolysis could help improve prevention and treatment strategies for these potentially dangerous complications. To establish the connection of IOH with the development of cardiac rhythm disturbances in patients with coronary artery disease after coronary shunting in conditions of cardiopulmonary bypass (CB). All patients underwent CB surgery in a planned manner under IR conditions. According to the level of free hemoglobin [Hb] in blood plasma, which is a marker of the degree of IOH, patients are divided into three groups: group 1 – without IOH (Hb≤ 0.1 g/l), n=43, group 2 - with low IOH (lIOH) - with [Hb]>0.1g/l and <0.5 g/l, n=42, group 3 – with a high IOH (hIOH) corresponded to [Hb] ≥0.5 g/l, n=38.
| Published in | Clinical Medicine Research (Volume 14, Issue 2) |
| DOI | 10.11648/j.cmr.20251402.11 |
| Page(s) | 28-36 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Coronary Artery Bypass Grafting, Hemolysis, Arrhythmias, Сomplications
Indicator | Group 1 n=43 | Group 2 n=42 | Group 3 n=38 |
|---|---|---|---|
Age, years | 60 (56; 63) | 64 (58; 66) | 66 (60; 68) |
Gender (male), % | 36 (87,8%) | 32 (78,0%) | 31 (78,0%) |
BMI (kg/m2) | 27,8 (24,7; 29,2) | 27,7 (24,8; 29,2) | 29,1 (25,9; 32,2) |
Total protein (g/l) | 69 (62; 71) | 69 (58; 68) | 66 (57; 67) |
Glucose, mmol/L | 5,0 (4,5; 5,6) | 5,2 (4,4; 6,1) | 5,3 (4,5; 6,2) |
Cholesterol, mmol/L | 4,1 (3,3; 5,0) | 4,6 (3,2; 5,7) | 5,0 (4,6; 5,6) |
Urea, mmol/L | 5,3 (4,8; 5,6) | 6,0 (5,5; 7,6) | 6,4 (5,5; 7,2) |
Creatinine, mmol/L | 99 (89; 104) | 105 (98; 110) | 106 (99; 112) |
CRP (mg/ml) | 1,2 (0,8; 1,4) | 1,1 (0,8; 1,3) | 1,0 (0,6; 1,2) |
Indicator | Group 1 n=43 | Group 2 n=42 | Group 3 n=38 |
|---|---|---|---|
Ischemia-reperfusion time (min) | 69 (65; 89) | 74 (68; 78) | 80 (75; 94) |
Ischemia time (min) | 46 (39; 64) | 58 (56; 62) | 59 (51; 68) |
Number of shunts | Group 1 n=43 | Group 2 n=42 | Group 3 n=38 | p1-2 | p1-3 | p2-3 |
|---|---|---|---|---|---|---|
1 | 9,9 | 7,5 | 10,8 | 0,412 | 0,510 | 0,314 |
2 | 31,0 | 26,8 | 39,2 | 0,510 | 0,610 | 0,094 |
3 and more | 59,1 | 65,7 | 50,0 | 0,462 | 0,130 | 0,318 |
Left anterior interventricular coronary artery | 87,8 | 100 | 100 | 0,21 | 0,31 | 0,31 |
Left circumflex artery | 4,9 | 7,3 | 19,5 | 0,644 | 0,420 | 0,105 |
Posterior interventricular branch of left circumflex artery | 14,6 | 39,0 | 61,0 | 0,210 | 0,310 | 0,406 |
Left marginal artery | 56,1 | 65,9 | 80,5 | 0,172 | 0,22 | 0,324 |
Right coronary artery | 24,4 | 58,5 | 61,0 | 0,231 | 0,341 | 0,821 |
Right interventricular branch artery | 17,07 | 34,15 | 26,8 | 0,706 | 0,285 | 0,471 |
Indicator | Gr 1 n=43 | Gr 2 n=42 | Gr 3 n=38 |
|---|---|---|---|
Ischemic heart disease duration | 8,5 (4,2; 11,4) | 8,9 (4,6; 10,8) | 9,5 (6,2; 12,1) |
Duration of hypertension | 10 (6; 11) | 8 (5; 10) | 11,5 (9; 15) |
Functional class II | 9 (20,1%) | 11 (26,2%) | 6 (15,8%) |
Functional class III | 34 (79,9%) | 31 (73,8%) | 32 (84,2%) |
Postinfarction cardiosclerosis | 37 (86,1%) | 36 (85,7%) | 33 (86,8%) |
The number of myocardial infarction (2 MI) in the history | 16 (37,2%) | 18 (42,8%) | 13 (34,2%) |
NYHAII | 36 (83,7%) | 31 (73,8%) | 33 (86,8%) |
NYHAIII | 7 (16,3%) | 11 (26,2%) | 5 (13,2%) |
Ischemic cardiomyopathy | 2 (0,86%) | 3 (1,26%) | 2 (0,76%) |
History of arrhythmias | 7 (16,3%) | 7 (16,6%) | 6 (15,4%) |
Paroxysm of atrial fibrillation | 0 (9%) | 1 (0,42) | 1 (0,38%) |
supraventricular extrasystole | 4 (1,72%) | 2 (0,84) | 2 (0,76%) |
ventricular extrasystole | 1 (0,43%) | 1 (0,42%) | 1 (0,38%) |
right His bundle branch block | 1 (0,43%) | 1 (0,42%) | 1 (0,38%) |
left His bundle branch block | 1 (0,43%) | 2 (0,42%) | 2 (0,76%) |
blood hypertension | 36 (87,8%) | 38 (90,2%) | 38 (92,7%) |
chronic bronchitis without exacerbation | 7 (16,3%) | 9 (21,4%) | 12 (31,6%) |
gastropathy | 18 (41,9%) | 17 (40,5%) | 20 (52,6%) |
urolithiasis | 6 (13,9%) | 9 (21,4%) | 7 (18,4%) |
osteoarthritis | 0 (0%) | 3 (7,1%) | 1 (2,6%) |
excess BMI and obesity | 36 (83,7%) | 31 (73,8%) | 33 (86,8%) |
excess BMI | 22 (51,2%) | 18 (42,9%) | 18 (47,4%) |
obesity | 14 (32,6%) | 13 (31%) | 15 (39,5%) |
Index (%) | Gr 1 n=43 | Gr 2 n=42 | Gr 3 n=38 | Gr 1-3 n=123 | χ2 | p |
|---|---|---|---|---|---|---|
beta blockers | 86,0 | 90,5 | 76,3 | 84,6 | 3,18 | 0,204 |
ACE inhibitors | 88,4 | 76,2 | 63,2° | 76,4 | 7,13 | 0,028 |
statins | 90,7 | 78,6 | 57,9°• | 76,4 | 12,2 | 0,006 |
antianginal | 93,0 | 83,3 | 60,5°• | 79,7 | 13,7 | 0,0001 |
antiplatelet agents | 88,4 | 81,0 | 68,4 | 79,7 | 5,35 | 0,069 |
Types of arrhythmias | Arrhythmia frequency (%) | p | |||||
|---|---|---|---|---|---|---|---|
all | PP | EP | |||||
n | % | n | % | n | % | ||
Total arrhythmias | 27 | 22,0 | 14 | 11,4 | 13 | 10,6 | NS |
ventricular fibrillation | 3 | 2,43 | 2 | 1,63 | 1 | 0,81 | NS |
ventricular tachycardia | 3 | 3,25 | 3 | 2,43 | - | - | NS |
atrial fibrillation | 7 | 5,70 | 3 | 2,43 | 4 | 3,25 | NS |
atrial flutter | 2 | 1,62 | 1 | 0,81 | 1 | 0,81 | NS |
supraventricular tachycardia | 1 | 0,81 | - | - | 1 | 0,81 | NS |
others: | 11 | 8,9 | 5 | 4,07 | 4 | 3,25 | NS |
AV block 1-2 degree | 2 | 1,6 | - | - | 2 | 1,6 | NS |
ventricular extrasystole | 5 | 4,1 | 4 | 3,25 | 3 | 2,43 | NS |
supraventricular extrasystole | 4 | 3,3 | 1 | 0,81 | 3 | 2,43 | NS |
Types of complications | Group 1 n=43 | Group 2 n=42 | Group 3 n=38 | All n=123 | χ2 | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|
n | % | n | % | n | % | n | % | |||
Arrhythmias | 2 | 4,7 | 5 | 11,9 | 20 | 52,6 | 27 | 22,0 | 21,95 | 0,000 |
Arrhythmias in the perioperative period | 2 | 4,7 | 2 | 4,8 | 10 | 26,3 | 14 | 11,4 | 14,8 | 0.0052 |
Arrhythmias in the early period | - | - | 3 | 7,14 | 10 | 26,3 | 13 | 10,6 | 15,6 | 0,0004 |
Types of arrhythmias | Gr 1 n=43 | Gr 2 n=42 | Gr 3 n=38 | χ2 | p | |||
|---|---|---|---|---|---|---|---|---|
n | % | n | % | n | % | |||
all arrhythmias | 2 | 4,65 | 5 | 11,9 | 20 | 52,6 | 39,54 | 0,0000 |
ventricular fibrillation | - | - | 1 | 2,38 | 2 | 5,26 | 4,547 | 0.1020 |
ventricular tachycardia | - | - | - | - | 3 | 7,89 | 6,878 | 0,032 |
atrial fibrillation | 1 | - | 1 | 2,38 | 5 | 15,8 | 4,132 | 0.1260 |
atrial flutter | - | - | 1 | 2,38 | 1 | 2,63 | 1,100 | 0.5760 |
supraventricular tachycardia | - | - | - | - | 1 | 2,63 | 2,255 | 0,3238 |
other | 1 | 2,32 | 2 | 4,80 | 8 | 23,7 | 10,06 | 0,0066 |
CPB | Cardiopulmonary Bypass |
CABG | Coronary Artery Bypass Grafting |
IOH | Intraoperative Hemolysis |
CHD | Coronary Heart Disease |
CB | Cardiopulmonary Bypass |
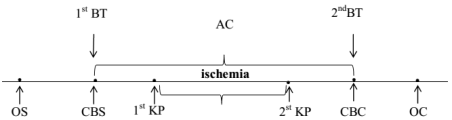
KP | Cardioplegia |
OS | Operation Start |
OC | Operation Completion |
1st BT | First Blood Test |
2nd BT | Second Blood Test |
| [1] | Bokeriya, L. A. Neposredstvenny`e rezul`taty` xirurgicheskogo i e`ndovaskulyarnogo lecheniya bol`ny`x ishemicheskoj bolezn`yu serdcza: perioperacionny`e oslozhneniya, faktory` riska, prognoz//L. A. Bokeriya, E. Z. Goluxova, B. G. Alekyani dr./Kreativnaya kardiologiya, 2011. – №1. – S. 41– 60. |
| [2] | Maksimovich E. N. Aritmii kak prichina letal'nogo iskhoda u pacientov posle operacii koronarnogo shuntirovaniya/Maksimovich E. N., Dementej A. I., Lavrinajt' V. V. i dr.//Sbornik tezisov XII mezhdunarodnoj (XXI Vserossijskoj) Pirogovskoj nauchnoj medicinskoj konferencii studentov i molodyh uchenyh. – 2017, Moskva. – S. 82. |
| [3] | Kim, L. K. Outcomes in patients undergoing coronary artery bypass graft surgery in the United States based on hospital volume, 2007 to 2011/P. Looser, R. V. Swaminathan, R. M. Minutello et al.//J. Thorac. Cardiovasc. Surg. – 2016. – V. 151(6). – P. 1686–1692. |
| [4] | Maksimovich, E. N. Aritmii u pacientov s IBS posle koronarnogo shunktirovaniya i raznoj spen`yu intraoperacionnogo gemoliza/E. N. Maksimovich, T. P. Pron`ko, V. A. Snezhiczkij//I s`ezd Evrazijskoj aritmologicheskoj associacii: sbornik materialov EURA Congress, 13-14 sentyabrya 2018 g. – Grodno, 2018. – S. 46 – 47. |
| [5] | Gel'fand, I. M. Prognosis of ventricular arrhythmias in myocardial infarct patients/I. M. Gel'fand, M. N. Starkova, A. L. Syrkin//Kardiologiia. – 1983. – V. 23, №5. – P. 9 –12. |
| [6] | Omer, S. Incidence, predictors, and impact of postoperative atrial fibrillation after coronary artery bypass grafting in military veterans//S. Omer, L. Cornwell, A. Bakshi//Tex. Heart Inst. J. – 2016, V. 43 (5). – P. 397 – 403. |
| [7] | Fengsrud, E. Pre- and postoperative atrial fibrillation in CABG patients have similar prognostic impact/E. Fengsrud, A. Englund, A. Ahlsson//Scand. Cardiovasc. J. – 2017. – V. 51 (1). – P. 21 – 27. |
| [8] | Venetucci, L. A. The sarcoplasmic reticulum and arrhythmogenic calcium release/L. A. Venetucci, A. W. Trafford, S. C. O'Neill, D. A. Eisner//Cardiovasc. Res. – 2008. – V. 77 (2). – P 285 – 292. |
| [9] | Valeri, C. R. Effects of centrifugal and roller pumps on survival of autologous red cells in cardiopulmonary bypass surgery/C. R. Valeri, H. MacGregor, G. Ragno, N. Healey//Perfusion. – 2006. – V. 21(5). – P. 291–296. |
| [10] | Maksimovich, E. N. Faktory` intraoperacionnogo gemoliza pri koronarnom shuntirovanii s ispol`zovaniem ickusstvennogo krovoobrashheniya/E. N. Maksimovich, V. V. Vasilevich, D. D. Truxovskaya, Yu. A. Koshheev, V. V. Kruglik//Sbornik materialov konferencii studentov i molody`x ucheny`x, posvyashhennoj 60-letiyu uchrezhdeniya obrazovaniya "Grodnenskij gosudarstvenny`j medicinskij universitet", 26-27 aprelya 2018 g.: sbornik statej. – Grodno, 2018. – S. 315 –316. |
| [11] | Vercaemst, L. Hemolysis in cardiac surgery patients undergo¬ing cardiopulmonary bypass: A review in search of a treatment algorithm/L. Vercaemst//J. of Extra. Corporeal. Technology. – 2008. – V. 40, № 4. – P. 257 – 267. |
| [12] | Pan, K. C. The meaning of a high plasma free hemoglobin: retrospective review of the prevalence of hemolysis and circuit thrombosis in an adult ECMO centre over 5 years/K. C. Pan, D. P. McKenzie, V. Pellegrino, D. Murphy//Perfusion. – 2016, V. 31 (3). – P. 223 – 231. |
| [13] | Svenmarker, S., Red blood cell trauma during cardiopulmonary bypass: Narrow pore filterability versus free hemoglobin/S. Svenmarker, E. Jansson, H. Stenlund, K. Engström//Perfusion. – 2000. – №15 (1). – P. 33 – 40. |
| [14] | Maksimovich E. N. Uroven` svobodnogo gemoglobina v plazme krovi pacientov s oslozhneniyami posle operacii koronarnogo shuntirovaniya/Maksimovich E. N., Vasilevich V. V., Koshheev Yu. A., Pron`ko T. P., Truсhovskaya D. D.//Mat. itogovoj nauchno-prakticheskoj konferencii «Aktual`ny`e problemy` mediciny`» 25 yanvarya 2019 g. – Grodno, 2018. – S. – 360 – 362. |
| [15] | Chikwe, J. Long-term outcomes after off-pump versus on-pump coronary artery bypass grafting by experienced surgeons/Chikwe J., Lee T., Itagaki S. et al.//J. Am. Coll Cardiol. – 2018. – V. 72. – P. 1478–1486. |
| [16] | Daniel, J. F. Improving coronary artery bypass grafting: a systematic review and meta-analysis on the impact of adopting transit-time flow measurement/J. F. Daniel, Thuijs M., Margreet W. A. David P. Taggart//Eur. J. Cardiothorac. – 2019. – V. 56(4). – P. 654–663. |
APA Style
Yelizaveta, M. (2025). Connection of Intraoperative Hemolysis with the Development of Cardiac Rhythm Disturbances. Clinical Medicine Research, 14(2), 28-36. https://doi.org/10.11648/j.cmr.20251402.11
ACS Style
Yelizaveta, M. Connection of Intraoperative Hemolysis with the Development of Cardiac Rhythm Disturbances. Clin. Med. Res. 2025, 14(2), 28-36. doi: 10.11648/j.cmr.20251402.11
@article{10.11648/j.cmr.20251402.11,
author = {Maksimovich Yelizaveta},
title = {Connection of Intraoperative Hemolysis with the Development of Cardiac Rhythm Disturbances
},
journal = {Clinical Medicine Research},
volume = {14},
number = {2},
pages = {28-36},
doi = {10.11648/j.cmr.20251402.11},
url = {https://doi.org/10.11648/j.cmr.20251402.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cmr.20251402.11},
abstract = {The use of cardiopulmonary bypass in coronary artery bypass grafting (CABG) surgery can lead to red blood cell damage (hemolysis). Postoperative arrhythmias, such as atrial fibrillation, are frequent and serious complications after CABG. However, the relationship between the hemolysis that occurs during the surgery intraoperative hemolysis and the subsequent development of arrhythmias is not well-understood. This study will examine the connection between the level of IOH and the incidence of cardiac rhythm disturbances in patients with coronary artery disease who have undergone CABG surgery. The mechanisms causing arrhythmias after CABG are complex and involve various factors including changes in blood flow, the damage caused by restoring blood flow after cardiopulmonary bypass, and oxidative stress. Clarifying the role of surgery intraoperative hemolysis could help improve prevention and treatment strategies for these potentially dangerous complications. To establish the connection of IOH with the development of cardiac rhythm disturbances in patients with coronary artery disease after coronary shunting in conditions of cardiopulmonary bypass (CB). All patients underwent CB surgery in a planned manner under IR conditions. According to the level of free hemoglobin [Hb] in blood plasma, which is a marker of the degree of IOH, patients are divided into three groups: group 1 – without IOH (Hb≤ 0.1 g/l), n=43, group 2 - with low IOH (lIOH) - with [Hb]>0.1g/l and <0.5 g/l, n=42, group 3 – with a high IOH (hIOH) corresponded to [Hb] ≥0.5 g/l, n=38.
},
year = {2025}
}
TY - JOUR T1 - Connection of Intraoperative Hemolysis with the Development of Cardiac Rhythm Disturbances AU - Maksimovich Yelizaveta Y1 - 2025/03/31 PY - 2025 N1 - https://doi.org/10.11648/j.cmr.20251402.11 DO - 10.11648/j.cmr.20251402.11 T2 - Clinical Medicine Research JF - Clinical Medicine Research JO - Clinical Medicine Research SP - 28 EP - 36 PB - Science Publishing Group SN - 2326-9057 UR - https://doi.org/10.11648/j.cmr.20251402.11 AB - The use of cardiopulmonary bypass in coronary artery bypass grafting (CABG) surgery can lead to red blood cell damage (hemolysis). Postoperative arrhythmias, such as atrial fibrillation, are frequent and serious complications after CABG. However, the relationship between the hemolysis that occurs during the surgery intraoperative hemolysis and the subsequent development of arrhythmias is not well-understood. This study will examine the connection between the level of IOH and the incidence of cardiac rhythm disturbances in patients with coronary artery disease who have undergone CABG surgery. The mechanisms causing arrhythmias after CABG are complex and involve various factors including changes in blood flow, the damage caused by restoring blood flow after cardiopulmonary bypass, and oxidative stress. Clarifying the role of surgery intraoperative hemolysis could help improve prevention and treatment strategies for these potentially dangerous complications. To establish the connection of IOH with the development of cardiac rhythm disturbances in patients with coronary artery disease after coronary shunting in conditions of cardiopulmonary bypass (CB). All patients underwent CB surgery in a planned manner under IR conditions. According to the level of free hemoglobin [Hb] in blood plasma, which is a marker of the degree of IOH, patients are divided into three groups: group 1 – without IOH (Hb≤ 0.1 g/l), n=43, group 2 - with low IOH (lIOH) - with [Hb]>0.1g/l and <0.5 g/l, n=42, group 3 – with a high IOH (hIOH) corresponded to [Hb] ≥0.5 g/l, n=38. VL - 14 IS - 2 ER -
Department of Propaedeutics of Internal Medicine, Grodno State Medical University, Grodno, Belarus
Information