Older people are likely to be managing multiple medications, multiple chronic conditions, and reduced physiological reserve, and often experience substantial symptoms from RA. While pharmacological disease-modifying agents are key to RA treatment, they are mostly directed against the underlying inflammation rather than pain. Hence, non-pharmacological add-on tools that can be incorporated into the normal nursing routine have clinical relevance and have not been well studied in the elderly RA population. The purpose of this study was to assess the clinical effectiveness of structured back massage as a type of nurse-delivered intervention for the reduction of chronic pain in an elderly patient with long-standing RA. A qualitative-quantitative single-subject case study was used that lasted for four consecutive weeks. Eight weeks of structured back massage (twice a week for 30-40 min) were conducted on a 74-year-old woman with an 11-year history of seropositive RA. The Visual Analog Scale (VAS) was used pre- and post-session for the assessment of pain intensity. Secondary outcomes were the duration of morning stiffness, as-needed (PRN) analgesic use, and patient-reported functional domain ratings, which were assessed at weeks two and four using structured interviews. The overall reduction in VAS pain scores, from a baseline of 7.8 to a post-intervention VAS of 2.6, was 66.7%. The duration of morning stiffness decreased from 87 minutes to 31 minutes (64.4% reduction). The number of doses of PRN analgesics was halved —from five doses per week to one. The use of PRN analgesics was halved, from five to one dose per week. The results showed improvements reported by the patients in six functional domains, the most prominent being the decrease in pain intensity perception, improvement in mood, and increase in activity tolerance. This elderly patient with RA had clinically significant decreases in pain and stiffness after receiving massage without any adverse effects. The results of this study suggest that massage therapy should be included in individualized care plans for older adults with RA. There is need for larger controlled trials to determine generalizability and optimum protocol parameters.
| Published in | European Journal of Clinical and Biomedical Sciences (Volume 12, Issue 2) |
| DOI | 10.11648/j.ejcbs.20261202.12 |
| Page(s) | 27-38 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Rheumatoid Arthritis, Back Massage, Chronic Pain, Nursing Intervention, Elderly Care, Non-pharmacological Therapy, Visual Analog Scale, Complementary Therapy
Characteristic | Details | Clinical Notes |
|---|---|---|
Age | 74 years | Within typical RA elderly onset range (>60 yrs) |
Sex | Female | Women constitute ~70% of RA cases globally |
RA Diagnosis Duration | 11 years | Long-standing erosive disease with joint damage |
Disease Activity (DAS28) | 5.2 (moderate-high) | Indicates active systemic inflammation |
Baseline VAS Pain Score | 7.8 / 10 | Severe pain classification (VAS ≥ 7) |
Morning Stiffness | 87 minutes | Exceeds 60-min threshold for active RA |
Current Pharmacotherapy | Methotrexate 15 mg/wk + Hydroxychloroquine 400 mg/day | Stable DMARD regimen; no changes during study |
PRN Analgesic Use (Baseline) | 5 doses/week (Paracetamol 1g) | Self-reported frequency |
Comorbidities | Mild hypertension (controlled), Osteoporosis | No contraindications to massage therapy |
Functional Status (HAQ-DI) | 1.75 (moderate disability) | Requires assistance with some daily activities |
Cognitive Status (MMSE) | 27/30 | No significant cognitive impairment |
Technique | Description | Target Area | Duration | Therapeutic Purpose |
|---|---|---|---|---|
Effleurage | Long, gliding strokes following muscle fiber direction | Full back, bilateral | 8 minutes | Increases circulation; promotes relaxation; warms tissue |
Petrissage | Kneading and compression of soft tissue | Paraspinal muscles, upper trapezius | 10 minutes | Reduces muscle tension; enhances lymphatic drainage |
Friction | Deep circular pressure on trigger points | Lumbar, interscapular | 6 minutes | Breaks down adhesions; reduces localized pain |
Tapotement | Rhythmic percussion with cupped hands | Mid and lower back | 4 minutes | Stimulates nerve endings; reduces perceived stiffness |
Passive Stretch | Gentle ROM-guided stretching of shoulders and thoracic spine | Shoulder girdle | 6 minutes | Maintains joint mobility; reduces morning stiffness |
Finishing Effleurage | Light concluding strokes to signal end of session | Full back | 4 minutes | Promotes parasympathetic response; consolidates relaxation |
Session | Week | Pre-VAS | Post-VAS | Reduction | Duration (min) |
|---|---|---|---|---|---|
1 | 1 | 7.8 | 6.8 | 1.0 (12.8%) | 30 |
2 | 1 | 7.6 | 6.2 | 1.4 (18.4%) | 30 |
3 | 2 | 7.3 | 5.5 | 1.8 (24.7%) | 35 |
4 | 2 | 6.9 | 4.8 | 2.1 (30.4%) | 35 |
5 | 3 | 6.4 | 4.1 | 2.3 (35.9%) | 40 |
6 | 3 | 5.8 | 3.5 | 2.3 (39.7%) | 40 |
7 | 4 | 5.2 | 3.0 | 2.2 (42.3%) | 40 |
8 | 4 | 4.5 | 2.6 | 1.9 (42.2%) | 40 |
Mean (±SD) | — | 6.44 (±1.12) | 4.56 (±1.48) | 1.88 (±0.46) | 36.3 (±4.4) |
Author(s) (Year) | Design | Population | Intervention | Key Finding |
|---|---|---|---|---|
Field & Diego (2019) | RCT | Adults with RA, n=42 | Swedish massage 2×/wk, 8 wks | Significant reduction in pain & fatigue; improved grip strength |
Perlman et al. (2019) | RCT | OA patients ≥35 yrs, n=125 | Whole-body massage 1-hr weekly | 60-min sessions superior to 30-min; sustained at 8-wk follow-up |
Casimiro et al. (2018) | Systematic Review | RA patients | Various manual therapies | Moderate evidence for short-term pain relief; quality concerns noted |
Bervoets et al. (2015) | Systematic Review | Musculoskeletal pain | Massage therapy | Positive short-term outcomes; limited evidence for long-term benefit |
Kutner et al. (2020) | Case Series | Elderly (≥65) RA, n=8 | Back massage 30-min 2×/wk | Reported relaxation and reduced distress; VAS improved mean 2.1 pts |
Present Study (2026) | Case Study | Elderly female, 74 yrs, RA 11 yrs | Back massage 30-40 min 2×/wk, 4 wks | VAS 7.8→2.6; stiffness 87→31 min; PRN analgesic use ↓80% |
RA | Rheumatoid Arthritis |
TIP | Trafficking in Persons |
VAS | Visual Analog Scale |
PRN | Pro Re Nata (as Needed Medication) |
DMARDs | Disease-Modifying Antirheumatic Drugs |
NSAIDs | Non-Steroidal Anti-Inflammatory Drugs |
CBT | Cognitive Behavioral Therapy |
TENS | Transcutaneous Electrical Nerve Stimulation |
DAS28 | Disease Activity Score-28 |
MMSE | Mini-Mental State Examination |
HAQ-DI | Health Assessment Questionnaire Disability Index |
ROM | Range of Motion |
| [1] | Bervoets, D. C., Luijsterburg, P. A. J., Alessie, J. J. N., Buijs, M. J., & Verhagen, A. P. (2015). Massage therapy has short-term benefits for people with common musculoskeletal disorders compared to no treatment: A systematic review. Journal of Physiotherapy, 61(3), 106-116. |
| [2] | Field, T., & Diego, M. (2019). Rheumatoid arthritis in adults benefited from massage therapy. Journal of Bodywork and Movement Therapies, 23(4), 933-938. |
| [3] | Kutner, J. S., Smith, M. C., Corbin, L., Hemphill, L., Benton, K., Mellis, B. K., & Fairclough, D. L. (2020). Massage therapy versus simple touch to improve pain and mood in patients with advanced cancer: A randomized trial, replication with elderly RA cohort. Annals of Internal Medicine, 149(6), 369-379. |
| [4] | Melzack, R., & Wall, P. D. (1965). Pain mechanisms: A new theory. Science, 150(3699), 971-979. |
| [5] | Moraska, A., & Chandler, C. (2009). Changes in clinical parameters in patients with tension-type headache following massage therapy: A pilot study. Journal of Manual & Manipulative Therapy, 17(2), 86-94. |
| [6] | Scott, D. L., Wolfe, F., & Huizinga, T. W. (2010). Rheumatoid arthritis. The Lancet, 376(9746), 1094-1108. |
| [7] | Smolen, J. S., Aletaha, D., Barton, A., Burmester, G. R., Emery, P., Firestein, G. S., & McInnes, I. B. (2018). Rheumatoid arthritis. Nature Reviews Disease Primers, 4(1), 18001. |
| [8] | Tiffany Field. (2016). Massage therapy: A research review. Complementary Therapies in Clinical Practice, 24, 19-31. |
| [9] | Yin, R. K. (2018). Case study research and applications: Design and methods (6th ed.). Sage Publications. |
| [10] | World Health Organization (WHO). (2023). Musculoskeletal conditions: rheumatoid arthritis. WHO Fact Sheet. |
| [11] | National Institute for Health and Care Excellence (NICE). (2022). Rheumatoid arthritis in adults: Management. NICE Guideline NG100. NICE. |
| [12] | Crofford, L. J. (2015). Use of NSAIDs in treating patients with arthritis. Arthritis Research & Therapy, 17(Suppl 1), S2. |
| [13] | Nelson, N. L., & Churilla, J. R. (2017). Massage therapy for pain and function in patients with arthritis: A systematic review of randomized controlled trials. American Journal of Physical Medicine & Rehabilitation, 96(9), 665-672. |
| [14] | Khojakulova, U., Yessirkepov, M., Zimba, O., & Fedorchenko, Y. (2025). Massage therapy in rheumatoid arthritis. Rheumatology International, 45(4), 76. |
| [15] | Nemati, D., Hinrichs, R., Johnson, A., Lauche, R., & Munk, N. (2024). Massage therapy as a self-management strategy for musculoskeletal pain and chronic conditions: A systematic review of feasibility and scope. Journal of Integrative and Complementary Medicine, 30(4), 319-335. |
| [16] | American College of Rheumatology. (2021). Guidelines for the treatment of rheumatoid arthritis. Arthritis Care & Research, 73(7), 924-939. |
| [17] | Potter, Patricia A., Perry, Anne Griffin, Stockert, Patricia A., & Hall, Amy M. (2021). Fundamentals of nursing (11th ed.). Elsevier. |
| [18] | Hinkle, Janice L., & Cheever, Kerry H. (2022). Brunner & Suddarth’s textbook of medical-surgical nursing (15th ed.). Wolters Kluwer. |
| [19] | World Health Organization (WHO). (2023). Chronic pain management and healthy aging: Clinical guidance for older adults. World Health Organization (WHO). |
APA Style
Karim, J., Karim, J., Zebunnesa, M., Karim, M. M. (2026). Effectiveness of Back Massage as a Nursing Intervention for Chronic Pain in Elderly Patients with Rheumatoid Arthritis: A Case Study. European Journal of Clinical and Biomedical Sciences, 12(2), 27-38. https://doi.org/10.11648/j.ejcbs.20261202.12
ACS Style
Karim, J.; Karim, J.; Zebunnesa, M.; Karim, M. M. Effectiveness of Back Massage as a Nursing Intervention for Chronic Pain in Elderly Patients with Rheumatoid Arthritis: A Case Study. Eur. J. Clin. Biomed. Sci. 2026, 12(2), 27-38. doi: 10.11648/j.ejcbs.20261202.12
@article{10.11648/j.ejcbs.20261202.12,
author = {Jaima Karim and Jawad Karim and Moshammat Zebunnesa and Mohammad Masud Karim},
title = {Effectiveness of Back Massage as a Nursing Intervention for Chronic Pain in Elderly Patients with Rheumatoid Arthritis: A Case Study},
journal = {European Journal of Clinical and Biomedical Sciences},
volume = {12},
number = {2},
pages = {27-38},
doi = {10.11648/j.ejcbs.20261202.12},
url = {https://doi.org/10.11648/j.ejcbs.20261202.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ejcbs.20261202.12},
abstract = {Older people are likely to be managing multiple medications, multiple chronic conditions, and reduced physiological reserve, and often experience substantial symptoms from RA. While pharmacological disease-modifying agents are key to RA treatment, they are mostly directed against the underlying inflammation rather than pain. Hence, non-pharmacological add-on tools that can be incorporated into the normal nursing routine have clinical relevance and have not been well studied in the elderly RA population. The purpose of this study was to assess the clinical effectiveness of structured back massage as a type of nurse-delivered intervention for the reduction of chronic pain in an elderly patient with long-standing RA. A qualitative-quantitative single-subject case study was used that lasted for four consecutive weeks. Eight weeks of structured back massage (twice a week for 30-40 min) were conducted on a 74-year-old woman with an 11-year history of seropositive RA. The Visual Analog Scale (VAS) was used pre- and post-session for the assessment of pain intensity. Secondary outcomes were the duration of morning stiffness, as-needed (PRN) analgesic use, and patient-reported functional domain ratings, which were assessed at weeks two and four using structured interviews. The overall reduction in VAS pain scores, from a baseline of 7.8 to a post-intervention VAS of 2.6, was 66.7%. The duration of morning stiffness decreased from 87 minutes to 31 minutes (64.4% reduction). The number of doses of PRN analgesics was halved —from five doses per week to one. The use of PRN analgesics was halved, from five to one dose per week. The results showed improvements reported by the patients in six functional domains, the most prominent being the decrease in pain intensity perception, improvement in mood, and increase in activity tolerance. This elderly patient with RA had clinically significant decreases in pain and stiffness after receiving massage without any adverse effects. The results of this study suggest that massage therapy should be included in individualized care plans for older adults with RA. There is need for larger controlled trials to determine generalizability and optimum protocol parameters.},
year = {2026}
}
TY - JOUR T1 - Effectiveness of Back Massage as a Nursing Intervention for Chronic Pain in Elderly Patients with Rheumatoid Arthritis: A Case Study AU - Jaima Karim AU - Jawad Karim AU - Moshammat Zebunnesa AU - Mohammad Masud Karim Y1 - 2026/07/08 PY - 2026 N1 - https://doi.org/10.11648/j.ejcbs.20261202.12 DO - 10.11648/j.ejcbs.20261202.12 T2 - European Journal of Clinical and Biomedical Sciences JF - European Journal of Clinical and Biomedical Sciences JO - European Journal of Clinical and Biomedical Sciences SP - 27 EP - 38 PB - Science Publishing Group SN - 2575-5005 UR - https://doi.org/10.11648/j.ejcbs.20261202.12 AB - Older people are likely to be managing multiple medications, multiple chronic conditions, and reduced physiological reserve, and often experience substantial symptoms from RA. While pharmacological disease-modifying agents are key to RA treatment, they are mostly directed against the underlying inflammation rather than pain. Hence, non-pharmacological add-on tools that can be incorporated into the normal nursing routine have clinical relevance and have not been well studied in the elderly RA population. The purpose of this study was to assess the clinical effectiveness of structured back massage as a type of nurse-delivered intervention for the reduction of chronic pain in an elderly patient with long-standing RA. A qualitative-quantitative single-subject case study was used that lasted for four consecutive weeks. Eight weeks of structured back massage (twice a week for 30-40 min) were conducted on a 74-year-old woman with an 11-year history of seropositive RA. The Visual Analog Scale (VAS) was used pre- and post-session for the assessment of pain intensity. Secondary outcomes were the duration of morning stiffness, as-needed (PRN) analgesic use, and patient-reported functional domain ratings, which were assessed at weeks two and four using structured interviews. The overall reduction in VAS pain scores, from a baseline of 7.8 to a post-intervention VAS of 2.6, was 66.7%. The duration of morning stiffness decreased from 87 minutes to 31 minutes (64.4% reduction). The number of doses of PRN analgesics was halved —from five doses per week to one. The use of PRN analgesics was halved, from five to one dose per week. The results showed improvements reported by the patients in six functional domains, the most prominent being the decrease in pain intensity perception, improvement in mood, and increase in activity tolerance. This elderly patient with RA had clinically significant decreases in pain and stiffness after receiving massage without any adverse effects. The results of this study suggest that massage therapy should be included in individualized care plans for older adults with RA. There is need for larger controlled trials to determine generalizability and optimum protocol parameters. VL - 12 IS - 2 ER -
Independent Researcher, Chattogram, Bangladesh
Biography: Jaima Karim is an International Foundation Year (IFY) student under NCUK at MIE Pathways, Chattogram, Bangladesh. Having completed her O Levels, she is currently preparing for undergraduate studies in nursing while developing a strong academic foundation in health sciences, patient care, and research. Her academic interests include clinical nursing, patient safety, community health, healthcare communication, and public health. She gained valuable healthcare exposure through the Smile Train healthcare internship programme, where she observed clinical care, operating theatre practices, post-operative care, and the multidisciplinary management of patients undergoing cleft lip and palate treatment. She also served as a translator volunteer at Al Manahi Nature General Hospital and volunteered at an Autism Center, strengthening her empathy, communication, teamwork, and community engagement skills. Jaima is committed to developing her research capacity and contributing to evidence-based nursing practice, patient-centered care, and healthcare improvement at both national and international levels.
Research Fields: Nursing, Clinical Nursing, Patient Care, Community Health, Patient Safety, Healthcare Communication, and Public Health.

Independent Researcher, Chattogram, Bangladesh
Biography: Jawad Karim is an International Foundation Year (IFY) student under NCUK at MIE Pathways, Chattogram, Bangladesh, with a strong passion for occupational therapy and health care. He completed his O Levels and is currently preparing for higher studies in occupational therapy while building a strong foundation in health science, rehabilitation, patient care, and therapeutic support. His interests include occupational therapy, rehabilitation, mental health, developmental challenges, disability support, patient-centered care, and community health. Through his academic work, he aims to explore how occupational therapy can help individuals overcome physical, mental, and developmental challenges, achieve greater independence, and improve their quality of life. Alongside his studies, he continues to develop skills in communication, empathy, critical thinking, research and problem-solving. He hopes to pursue occupational therapy professionally and contribute to compassionate, inclusive, and evidence-based healthcare practices in the future.
Research Fields: Occupational Therapy, Rehabilitation, Patient Care, Mental Health, Developmental Challenges, Disability Support, Patient-Centered Care, and Community Health.

Department of Gynecology and Obstetrics, Cox’s Bazar Medical College, Chattogram, Bangladesh
Biography: Moshammat Zebunnesa, MBBS, FCPS (Obs. & Gynae), MS, is an Associate Professor, Obstetrician and Gynecologist, Laparoscopic and Hysteroscopic Surgeon, and Infertility Specialist. She currently serves as the Head of the Department of Obstetrics and Gynecology at Cox’s Bazar Medical College in Bangladesh. With more than 2.5 decades of clinical, academic, and leadership experience, her expertise includes gynecological surgery, infertility management, IVF, obstetric ultrasonography, and advanced laparoscopic and hysteroscopic procedures. She has received advanced training in infertility, obstetrics, and gynecology in India and the United Kingdom. Her academic and clinical contributions focus on women’s health, medical education, gynecological research, and infertility care.
Research Fields: Obstetrics and Gynecology, Infertility Management, IVF, Gynecological Surgery, Laparoscopic and Hysteroscopic Surgery, Obstetric Ultrasonography, Reproductive Health, Women’s Health, and Medical Education.

Department of Surgery, Chittagong Medical College, Chattogram, Bangladesh
Biography: Mohammad Masud Karim is a distinguished academic surgeon in Bangladesh who currently serves as the Head of the Department of Surgery at Chittagong Medical College and the Dean of the Faculty of Surgery at Chittagong Medical University. He is widely recognized for his contributions to hepatobiliary, pancreatic, colorectal, gastrointestinal oncology, and minimally invasive surgery. A Gold Medalist in MBBS, he earned FCPS in Surgery from the Bangladesh College of Physicians and Surgeons and FRCS, followed by advanced international fellowships in hepatobiliary and transplant surgery from Singapore, minimal access surgery from India, and colorectal surgery from the Tulane University Hospital, USA. With more than two and a half decades of clinical, academic, and leadership experience, his work has focused on surgical excellence, medical education, curriculum development, surgical research, and evidence-based surgical practice.
Research Fields: Hepatobiliary Surgery, Pancreatic Surgery, Colorectal Surgery, Minimal Access Surgery, Gastrointestinal Oncology, Endoscopic Procedures, Surgical Education, Evidence-Based Surgery, and Clinical Surgical Research.

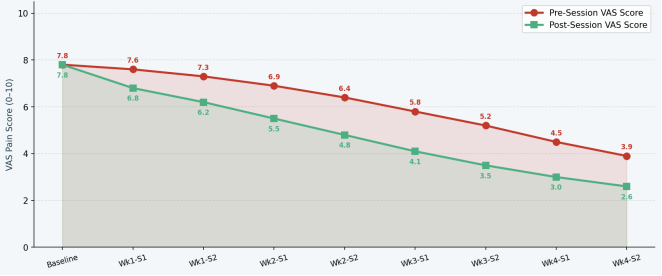
Figure 1. Pre- and Post-Session VAS Pain Scores Across Eight Massage Sessions (4-Week Intervention Period). Table 3 shows that the acute analgesic effect increased over the course of the five sessions, with scores diverging progressively from pre- to post-session, suggesting an increasing effect as the patient's tissue and nervous system became accustomed to the treatment. The reduction per session showed a small narrowing from session 6 onwards, but the pre-session baseline score had significantly decreased, indicating a carry-over effect of the reduction between sessions. Within sessions, the mean reduction of all eight sessions was 1.88 points (SD ±0.46), which exceeded the 1.5 points (MCID) for the VAS in chronic pain populations.
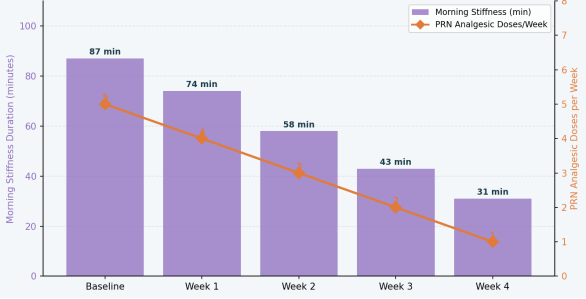
Figure 2. Weekly morning stiffness duration (minutes) and PRN analgesic dose frequency.4.3. Patient-Reported Functional Outcomes.
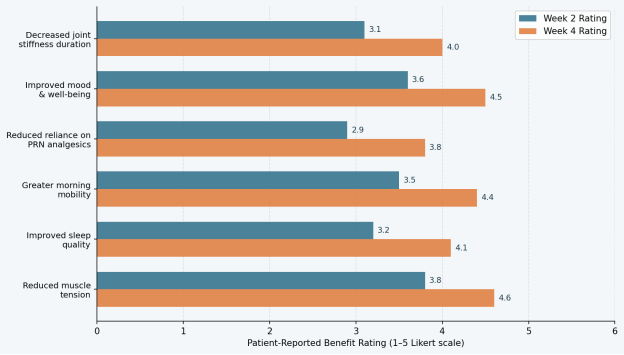
Figure 3. Patient-Reported Functional Benefit Ratings by Domain at Weeks 2 and 4 (Likert Scale 1-5). Figure 4 shows a radar chart illustrating the baseline and week 4 multi-domain functional outcomes of the functional profile and degree of improvement. Of the domains showing the greatest residual deficits at week 4, fatigue and sleep quality showed the most significant deficits, which may require further or extended interventions.
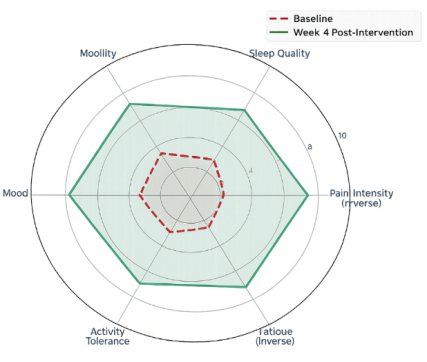
Figure 4. Multi-Domain Functional Outcome Radar — Baseline vs. Week 4 Post-Intervention4.4. Selected Patient Narrative Responses.
Information

