Abstract
Background: Brachytherapy has been part of the standard of care in the treatment of cervical cancer. Brachytherapy has evolved from two to three-dimensional treatment for better volume delineation for target and OAR thus leading to better LC and reduced toxicities. Presently, MR Brachytherapy is the gold standard. However, its use is limited by its availability and patient logistics. To combat this barrier, CT-guided brachytherapy guidelines were established over time and have been proven non-inferior to MR brachytherapy. The recent IBS-GEC-ESTRO recommendation 2021 has advised the use of contrast to delineate tumor and normal tissue. The objective of this study is to assess LRR and normal tissue toxicities at 3 months with the use of contrast versus non-contrast CT-based contouring. Material and methods: Data from all patients with proven LACC, treated by brachytherapy after CCRT between May 2023 and Sep'2024 were reviewed. CCRT followed by BT. Two patient data sets included arm1; without and arm2; with contrast during brachytherapy CT simulation. 1-2 ml contrast in the bladder and 4-5 ml rectum contrast diluted in 20 ml and 10-15 ml NS, respectively. I.V. contrast was given only to patients with residual disease. CT-based contouring and planning were done similarly in both arms. Results: Forty patients with LACC, as per recent FIGO stage (II A: 5.72%, II B: 22.86%, III B: 17.41%, III C: 40%, and IV: 14.29%), who completed treatment were part of this study. Out of 40 patients, 11 (27%) underwent adaptive brachytherapy. Higher stages were observed more commonly in arm 1. LRR was higher in arm 1 (85%) than arm2 42%. Defaulters in arm 2 were more (23.81%) than in arm 1 (5%). In a median follow-up of 3 months, 10% of local failure was observed in arm 1 and 33.33% in arm 2. No acute toxicities were seen in 55% of the cases (22/35 patients). No High-grade acute toxicity events (> grade 2) were reported. A significant difference was observed in the G1 bladder and rectal toxicity in both arms. G2 rectal toxicity was reported only in arm 2 in 1 patient. Only G1 Bowel toxicity was seen and was insignificant between both arms. Conclusion: Local control was significantly more in arm 1 (p- 0.019). Only G1 toxicities were observed in both arms. No significant difference was observed in the D2cc volume of any of the OARs between both groups. This implies, no significance of implementing contrast material in CT-based brachytherapy treatment.
Keywords
Cervical Cancer, Contrast, Local Control, Toxicity Assessment
1. Introduction
Cervical cancer incidence has decreased by more than one-half since the mid‐1970s because of the widespread use of screening methods. Although disease trend varies by age, race, and ethnicity. Recently data suggest that the rate of cervical cancer is increasing in women younger than 65 years, perhaps due to lack of vaccination in the early stage of life. Hence, increased HPV prevalence and suboptimal screening in this age group lead to a suspected increase in the incidence of disease in the younger age group. However, the incidence of invasive cervical cancer has declined by 33% globally annually during the previous 7 years.
GLOBOCON 2022 Indian data ranks cervical cancer as 2nd most common cancer in females and 3rd most common overall with around 1,27,526 new cases reported in 2022
.
For stage IB to IV Chemoradiotherapy remains the main treatment modality. It includes EBRT (External Beam Radiation Therapy) with concurrent chemotherapy and BT (brachytherapy). Todd and Meredith in 1930 did dose reporting based on the ICRU 38 protocol, where the dose was prescribed to POINT A, plotted with the help of orthogonal radiograph post brachytherapy applicator insertion. The drawback was the blind implementation of the applicator and dosing based on its anatomical landmarks. Variation in applicator geometry changed position of point A in every implementation and hence it didn't correlate with the local control rate (LCR)
| [2] | Anis Bandyopadhyay, Arnab Kumar Ghosh, Bappaditya Chhatui. Dosimetric and clinical outcomes of CT based HR-CTV delineation for HDR intracavitary brachytherapy in carcinoma cervix — a retrospective study. Reports of Practical Oncology and Radiotherapy 2021, Volume 26, Number 2, pages: 170-178. https://doi.org/10.5603/RPOR.a2021.0023 |
[2]
.
With advances in brachytherapy planning and the evolution of concept of IGABT (Image Guided Adaptive Brachytherapy) came in. Organ delineation became precise, and prescribing dose to POINT A seemed less accurate.
Then, EMBRACE STUDY introduced the concept of image-guided brachytherapy. EMBRACE I was the first prospective multicentric study with gathered technical and clinical experience of certain European institutions and conceptualized work from the Gyn GEC-ESTRO group for target and dose volume reporting. Yet, there were no dose prescription constraints, it was a institutional based practice. Found that local failures (LF) were located inside the MR-IGABT target volumes in 90% of patients
| [3] | Maximilian P. Schmid, MD; Jacob C. Lindegaard, MD. Risk Factors for Local Failure Following Chemoradiation and Magnetic Resonance Image-Guided Brachytherapy in Locally Advanced Cervical Cancer: Results From the EMBRACE-I Study. January 4, 2023. Volume 41, Issue 10. https://doi.org/10.1200/JCO.22.01096 |
[3]
. Dose-response analysis showed that a minimal dose of 90% of 85 Gy to the HR-CTV led to 95% LC in 3 years. Retro-EMBRACE was multi-institutional data and was the first comprehensive report on clinical outcomes complied retrospectively for IGABT treatment. It showed a significantly high local control, overall survival, and cause-specific survival with limited normal tissue toxicity. This made MR-based imaging and planning as standard of care for brachytherapy treatment
| [4] | Alina Sturdza, Richard Pötter. Image guided brachytherapy in locally advanced cervical cancer: Improved pelvic control and survival in RetroEMBRACE, a multicenter cohort study. 2016 Published by Elsevier Ireland Ltd. Radiotherapy and Oncology 120 (2016) 428-43. http://dx.doi.org/10.1016/j.radonc.2016.03.011 |
[4]
. However, its applicability is limited by its availability and logistics, especially in developing countries. Hence use of alternative imaging has been attempted for IGABT treatment which can lead to similar local control rates and normal tissue toxicities as that of MR-IGABT.
EMBRACE II study, with the help of the above 2 studies, established that a target dose of >85Gy EQD2 to HR-CTV-D90 is associated with a 3 yr LC of >96% in tumor volume of <30cc and >91% in tumor of >30cc with the application of advanced EBRT, BT techniques and chemotherapy within limited overall treatment time and thus maintaining good QOL with reduced morbidity
| [5] | Richard Pötter, Kari Tanderup. The EMBRACE II study: The outcome and prospect of two decades of evolution within the GEC-ESTRO GYN working group and the EMBRACE studies. version v.1.0. 2018 Jan 11: 9: 48-60. https://doi.org/10.1016/j.ctro.2018.01.001 |
[5]
. It also led to the concept of adaptive brachytherapy which resulted in better tumor coverage and decreased morbidity which further increased LC
| [6] | Leonel Varela Cagetti, MD, Christophe Zemmour. Early clinical outcomes of hybrid brachytherapy for locally advanced cervical cancer: making adverse situations in a favorable scenario. 2022; 14, 4: 321-331. https://doi.org/10.5114/jcb.2022.118831 |
[6]
.
In this study, we have compiled a small data of 40 patients by using 3D-based imaging with and without the use of contrast in bladder and rectal or using intra-venous line, as per recent GEC-ESTRO recommendations for CT-based contouring. Which would help evaluate local tumor control and normal tissue toxicity with and without the use of contrast material. With the aim of proven non-inferiority, restricted use or omission of contrast can be considered and studied further. As in a developing country, treatment affordability and logistics have a major role. Also, this might reduce contrast-related undue side effects caused to patients.
2. Data and Statistical Analyses
All statistical data analysis was performed with an alpha level of 5%, i.e. if any p value is less than 0.05 it has been considered as significant.
Categorical variables are expressed as patients characteristics which was compared across the groups using Pearson's Chi Square test for Independence of Attributes/ Fisher's Exact Test as appropriate.
Continuous variables are expressed as Mean, Median and Standard Deviation and compared across the groups using Mann-Whitney U test since the data does not follow normal distribution. With means ± standard deviations of Univariate and multivariate analysis, local failures and acute toxicities were evaluated.
As this study is analyzed based on acute events after brachytherapy treatment, Local failure (at 1st follow-up visit i.e. at 3 months) was defined as any clinical and/or radiological evidence of disease persistence in the pelvis after completion of brachytherapy. The secondary objective of the study was to evaluate acute toxicities in the rectum, bladder, bowel, and vagina at 1st follow-up based on CTCAE version 5.
2.1. Figures
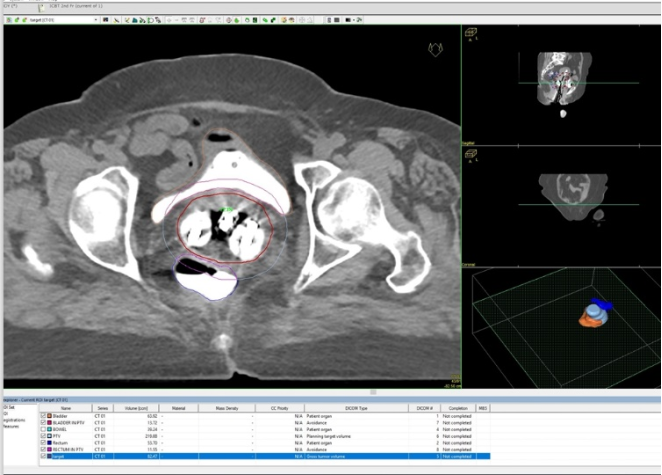
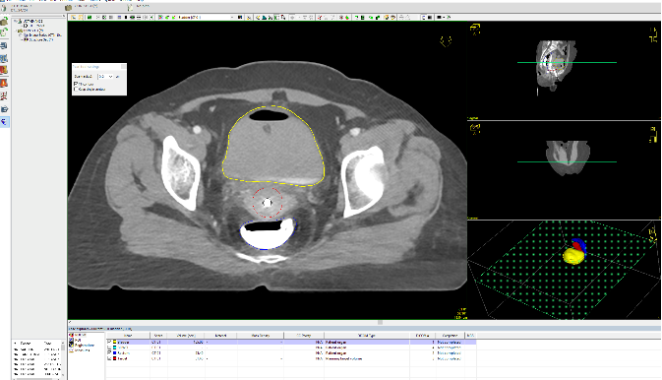
Figure 1. It shows the contours of HR-CTV, Bladder, and Rectum with contrast. Sagittal sections shows the extent of HR-CTV. HR-CTV was commonly contoured to include the lower uterine segment, cervix, and upper one-third vagina.
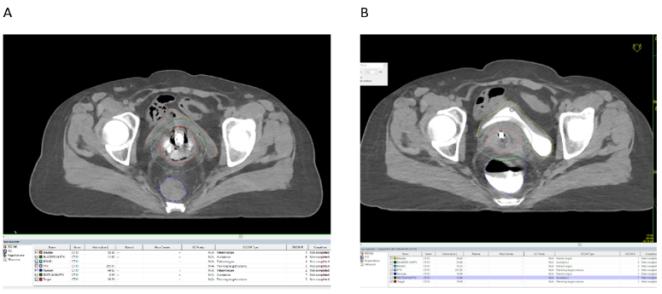
Figure 2. A - Shows non-contrast delineation of bladder and rectum. B- shows contrast delineation of the bladder, rectum and disease. It also shows changes in volume of the bladder and rectum after contrast instillation.
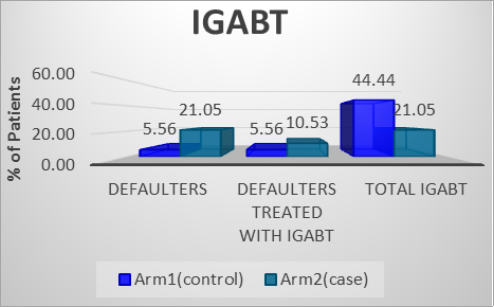
Figure 3. Percentage (%) of IGABT performed in control group was more and number of defaulters were less. Which might imply to less toxicity and better control rate. But this difference was not significant.
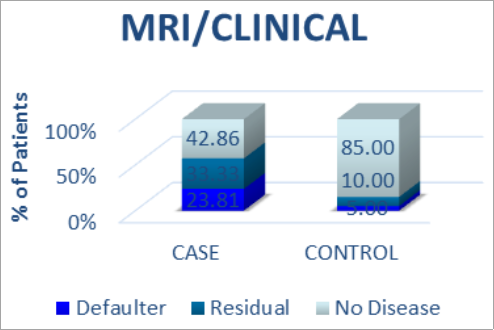
Figure 4. It shows the percentage (%) of cases that had a good local control rate. And also gives knowledge about the percentage of defaulters and disease persistence in each group.
Figure 5. Shows how defected filling of dye in OARs can lead to change in contours. As seen here, due to filling of rectal gas while injecting contrast led to rectal inflation, which results in more rectum coming in the field of radiation. Scanty visualization of contrast in the bladder leads to difficult visualize of bladder wall.
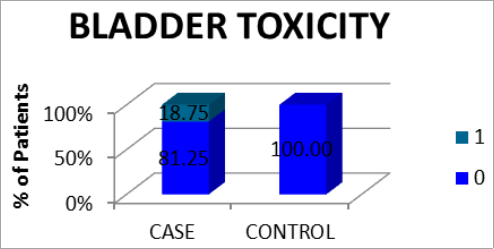
Figure 6. Bladder toxicities were significantly low in control (arm1) with a p-value of 0.048.
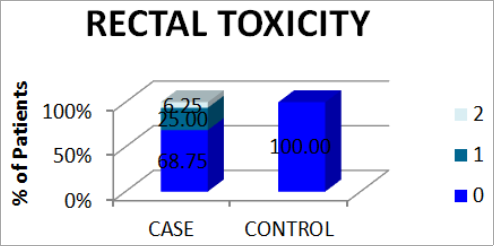
Figure 7. Rectal toxicities were significantly low in control (arm1) with a p-value of 0.031.
2.2. Tables
Table 1. Baseline characteristics.
| Control (arm1) | Cases (arm2) | p Value |
Mean age | 44.80 | 55.00 | 0.013 |
Stage | | | |
IIA | 0 (0%) | 1 (5.56%) | |
IIA1 | 1 (5.88%) | 0 (0%) | |
IIB | 4 (23.53%) | 4 (22.22%) | 0.049 |
IIIB | 3 (17.65%) | 3 (16.67%) | |
IIIC | 5 (29.41%) | 0 (0%) | |
IIIC1 | 1 (5.88%) | 8 (44.44%) | |
IVA | 3 (17.65%) | 2 (11.11%) | |
EBRT doses | | | |
45-46Gy in 23-25 Fractions | 10 (55.6%) | 10 (52.3%) | 0.858 |
50-55Gy in 25-28Fractions | 8 (44.4%) | 9 (47.4%) | |
BT doses | | | |
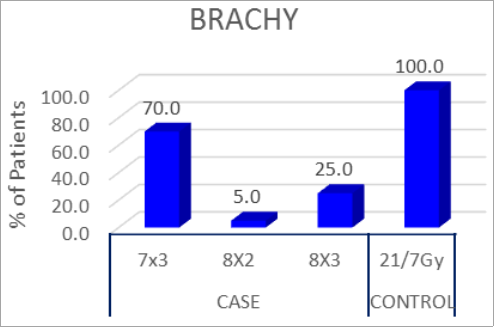
7Gy in 3 fractions | 18 (100%) | 14 (70%) | |
8 Gy in 2 fractions | 0 | 1 (5%) | 0.009 |
8Gy in 3 fractions | 0 | 5 (25%) | |
Table 2. Local Control Rate.
| Group | Total | p Value |
Local Control Rate | CASE | CONTROL |
Defaulter | 5 (23.81) | 1 (5) | 6 (14.63) | 0.019 |
Residual | 7 (33.33) | 2 (10) | 9 (21.95) |
No Disease | 9 (42.86) | 17 (85) | 26 (63.41) |
Total | 21 (100) | 20 (100) | 41 (100) | |
Table 3. IGABT treatment.
| Arm1 (control) | Arm2 (case) |
Defaulters | 1 | 4 |
Defaulters treated with IGABT | 1 | 2 |
Total IGABT | 8 | 4 |
Table 4. Bladder toxicity.
| Group | Total (%) | p Value |
CASE | CONTROL |
Toxicity Grade | 0 | 13 (81.25) | 19 (100) | 32 (91.43) | 0.048 |
1 | 3 (18.75) | 0 (0) | 3 (8.57) |
Total | 16 (100) | 19 (100) | 35 (100) | |
Table 5. Rectal toxicity.
| Group | Total | p Value |
CASE (%) | CONTROL (%) |
Toxicity Grade | 0 | 11 (68.75) | 19 (100) | 30 (85.71) | 0.031 |
1 | 4 (25) | 0 (0) | 4 (11.43) |
2 | 1 (6.25) | 0 (0) | 1 (2.86) |
Total | 16 (100) | 19 (100) | 35 (100) | |
3. Materials and Methods
Historically, Target delineation was not routinely done until 2013, only after that CT-based HR-CTV contouring was started. Now, we have tried to compare recent CT based GEC-ESTRO and commonly practiced, non-contrast CT-based planning in a prospective observational manner, to provide maximum clinical and logistic benefit to the patient by using minimal resources. This can be highly useful for developing nations with limited resources. Our, control group (arm1) contained 20 patients, taken by choosing a retrospective set of patients (who took brachytherapy using non-contrast CT-based simulation and planning). Another set of 20 patients, cases (arm2), were prospectively analyzed in whom contrast was pushed inside the bladder, Rectal, or through the intravenous route (only in case of residual disease for this study).
3.1. Patient Selection
The inclusion criteria included all biopsy proven cases of locally advanced cervical carcinoma between 18 to 85 years of age, proven inoperable, and had completed external beam radiotherapy with a total dose of 45-50 Gy in 23-25 fractions in 5 to 6 weeks along with concurrent Cisplatin chemotherapy. As shown in
table 1. Post-EBRT clinical examination and/or MRI was done to assess disease response. Only patients with frank residual disease on clinical examination or minimal residual disease on MRI scan were considered for intra-venous contrast during ICBT in arm2. Irrespective of residual disease status all cases in the prospective arm (arm2) received bladder and rectal contrast (
Figure 1). ICBT doses were with 3 fractions of 7 - 8 Gy per fraction with dose prescription to POINT A and optimized to cover HR-CTV volume with >80-85Gy EQD2 value. Other inclusion criteria were a Performance Status of 0 or 2 before starting brachytherapy, normal blood, and biochemistry profile. Cases of recurrence, previous history or radiation therapy in or around the pelvic area, or use of any altered fractionation during EBRT treatment were excluded from the study.
3.2. External Beam Radiotherapy
All patients in the study had completed EBRT to the whole pelvis to a total dose of 45 to 50 Gy in 23 to 25 fractions over 5 to 6 weeks with concurrent weekly Cisplatin 40 mg/m2. The EBRT machine was a LINAC true beam, Hyper Arc machine. The treatment was done using a conformal (3DCRT, IMRT, or VMAT) technique.
The stringent normal tissue dose contraints were maintained while planning on all these techniques to ensure the limitations of the EBRT technique and reporting had less control on the disease outcome and as well on patient related toxicities.
3.3. Brachytherapy
After defining disease extent clinically and radiologically. Especially in the case of residual disease, adaptive radiotherapy, by hybrid approach was preferred (more commonly in arm 1). Different applications used were cylinder with tandem, tandem with different sized ovoids, and different degrees/sizes of tandem or interstitial brachytherapy application in each session were considered after assessing all the risks and benefits. This decision was taken on the table after the final per-vaginal assessment under general anesthesia. After which the uterus was sounded with the help of transabdominal ultrasonography and the length and degree of tandem to be used for BT was decided. After application, the patient was taken for CT simulation, where bladder and rectal emptying were checked and then instilled with diluted contrast, just before the scan. Brachytherapy was delivered using an Iridium 192 remote after loader (Elekta Flexitron HDR Brachytherapy) for 3 fractions to a dose of 7-8 Gy per fraction weekly. Brachytherapy was done with the help of CT and both CT and MR-compatible applicators. The applicators consisted of uterine tandem with 15°, 30°, and 45° angulation. Before each BT application, pre-anesthetic clearance was taken. The procedure was done in minor OT under general anesthesia, after giving a rectal enema. Maintaining all aseptic precautions, painting, and draping were done followed by urinary catheterization, and the catheter balloon was inflated with normal saline to 7 mL. The procedure starts with a per-vaginal examination which helps locate the position of uterine Os, assess the extent of disease and parametrial involvement, and to assess the adequacy of vaginal space for insertion of appropriate-sized ovoids. It also helps to assess the health of rectal mucosa after EBRT, which guides towards a better dose distribution during brachytherapy treatment. Applicators are chosen as per vaginal findings. The size and degree of tandem insertion were decided while performing trans abdominal ultra-sonography-guided uterine sounding. Appropriate anterior and posterior vaginal packing was done to fix the applicator in place and to displace the bladder and rectum away from the applicator. After the intracavitary application, the applicator was fixed with the help of roller gauze bandages. All patients underwent a CT scan. A plain non-contrast was done to check bladder emptiness, and the presence of minimal residual urine was observed and accepted for all the cases. Now, During scanning, the bladder was filled retrogradely with 20 ml normal saline mixed with 1-2 ml contrast (iohexol- 3mg iodine /ml). Similarly, the rectum was evenly filled with 10-15 ml normal saline mixed in 4-5ml contrast using Ryle's tube. Intra-venous contrast was given only to patients having significant residual tumours. Serum creatinine was done for all cases for whom intra-venous contrast was given. The difference in rectal and bladder filling with and without contrast is shown in
Figure 2.
To minimize patient movement during CT scans and to keep the applicator in position. The scan was taken with a 3 mm slice thickness through the pelvis, from the highest point of the iliac crest to the upper thigh using a CT simulator. CT scan was then transferred to the treatment planning computer. Contouring of the organs at risk (OARS) i.e. bladder, rectum, and sigmoid colon, was done on axial sections. And was matched in the rest of the two views (coronal and sagittal sections). After receiving all CT images in the contouring system, 1st planning was done with a uniform loading pattern with dose prescriptions to point A after which contouring was done for organ and disease delineation. The plan was further optimized volumetrically to maintain HR-CTV D90 coverage to 80-85 Gy EQD2 (equivalent dose in 2 Gy fraction) and bladder, we tried to limit bladder, rectum, and sigmoid colon dose to 85 Gy EQD2, 65-70 Gy EQD2, and 65-70 Gy3 EQD2, respectively, strictly maintaining required coverage to residual disease. In case of no residue during brachytherapy, pre-EBRT disease volume and additional volume including lower uterine segment, cervix, and upper vagina was included in HR-CTV for ideal dose coverage. As gold standard approach for contouring remains clinical examination & documentation, and MRI at diagnosis and before Brachytherapy.
3.4. Study Technique and Data Collection
HR-CTV contouring was done following IBS-GEC ESTRO-ABS recommendations 2021 with the help of available pre-brachytherapy MR images and Pre-EBRT disease extent. Vaginal Ring applicator with interstitial catheters was used in the presence of any post-EBRT viable disease in the parametrium. Contouring was rechecked by another radiation oncologist, and with any discordance by more than 10%, the volumes were redrawn. HRCTV D90 dose coverage was prioritized and maintained. The volume of the bowel, bladder, and rectum was collected for dose statistics. D2cc (minimum dose received by maximally irradiated 2cc OAR volume) rectal dose, bladder dose, and sigmoid dose were collected from DVH (Dose Volume Histogram). Dimensions of HR-CTV were recorded from appropriate sagittal, coronal, and axial sections. Follow-up information was evaluated from records, and data on disease recurrence was noted down.
3.5. Treatment Response and Follow-up
On the first follow-up, after 3 months, local failure was detected clinically and confirmed radiologically either by MRI/PET- CT (positron emission tomography-computed tomography). Local failure (at 1st follow-up visit i.e. at 3 months) was defined as any clinical and/or radiological evidence of disease persistence in the pelvis after completion of brachytherapy. The secondary objective of the study was to evaluate acute toxicities in the rectum, bladder, bowel, and vagina at 1st follow-up based on CTCAE version 5.
4. Results
Total 40 patients were included in the study. Patients and tumor characteristics are summarized in
Table 1. Arm 1 had individuals with significant higher stage than arm 2, p value 0.049. Similarly, adaptive BT doses were used in Arm 2. This difference was significant with a p value of 0.009.
At the end of CCRT (concurrent chemoradiotherapy), clinical examination and MRI were performed to plan the brachytherapy strategy. Including both arms, 3 patients (7.5%) underwent combined brachytherapy (Intracavitary and interstitial brachytherapy with a median number of implanted catheters were in the range of, 1-6; 11 patients (27%), underwent image-guided adaptive brachytherapy (IGABT). This group of IGABT includes patients in whom the implant was planned only with intra-cavitary technique but the volume target coverage was insufficient, hence, a second implant with interstitial technique e was performed, with the aim of even dose distribution around the target, maintaining normal tissue constraints within normal limits. A similar graphical representation is depicted in (
Figure 3).
4.1. Local Control Rates
As primary outcome of this study is to assess local failure and complete response rate at 1st follow-up. HR-CTV coverage was prioritized and maintained at 80-85Gy EQD2 value in all the cases. Arm 1 has better local control and fewer defaulters than Arm 2. This difference is statistically significant with a p-value of 0.019., as shown in
Table 2. It was seen in 42.86% of cases in arm 2, whereas it reaches up to 85% in arm 1, the control arm, As shown in
Figure 4. 7 patients in arm 2 had residual disease. Hence were eligible for Intravenous contrast. However, only in 3 patients I.V. contrast was given due to deranged serum creatinine in one patient, and known contrasts induced allergy in 2 patients. And one case was not given contrast due to advanced age. However, This difference was not significantly relatable with the more common use of IGABT in arm 1. Total IGABT performed in arm 1 was 8 in number, out of which only one patient defaulted, which comes to around 36% cases reporting for follow-up. This patient was the only single defaulter in arm 1 and was enrolled for IGABT. Whereas in arm 2 only 4 patients underwent IGABT, out of which 2 patients defaulted for 1st and 2nd follow-up. The total number of defaulters in this arm was 4 in number. Therefore, only 12.5% of patients were treated with IGABT in Arm 2 (
Table 3).
4.2. Acute Treatment-Related Toxicities
Acute toxicities were evaluated for the bladder, rectum, and bowel using D2cc volumes for each of the OARs and calculating EQD2 values for each organ.
The main objective of collecting these values is to assess differences in CT-based contours with and without used of contrast and to reciprocate it clinically to patient related grade of toxicities.
For which, the average difference in D2cc volumes between both the arms, for each OAR was taken out as a representation of the difference in point dose due to change in volume of respected contours. The differences were statistically significant only for bowel contours and only during 1st fraction of brachytherapy with a p-value of 0.011. The differences in the bladder (G1) and rectum (G1, 2) toxicity were significant with a p-value of 0.048 and 0.031 respectively. As explained in
Tables 4 and 5. In the bladder, only G1 acute toxicity was noticed, and that too only in arm 2. No toxicity in arm 1. It could be justified by an increment in the volume of the bladder (other than residual urine) during the instillation of diluted contrast which eventually leads to sagging of the bladder bag and leads to increased doses in the bladder. In the rectum, G1 and G2 toxicities were more in arm 2 which would be again observed due to the filling of contrast material unevenly throughout the rectum. The pouching of contrast material and residual air which flows from Ryle's tube during injection of contrast in the rectum, around the area of interest leads to increased doses to rectum. (
Figure 5). G1 toxicity was 25% and G2 was 6.86% and was statistically significant with a p-value of 0.031 between the two arms. (
Table 5).
Only G1 bowel toxicities were obsereved and was not significant. When grades of each toxicities were compared with its respective D2cc and EQD2 values between two arms, the difference was not significant in any of them. Hence, direct correlation between the control rates and toxicities cannot be established due to change in contouring in between two groups.
5. Discussion
There are multiple studies on IGABT, mainly MR-based and recently CT-based. However, data on contrast CT-based brachytherapy as per recent GEC-ASTRO-based recommendations is still scarce. Some studies like one from Anis Bandyopadhyay et al, retrospectively contoured on planning CT for brachytherapy and planned each case based on point A
| [2] | Anis Bandyopadhyay, Arnab Kumar Ghosh, Bappaditya Chhatui. Dosimetric and clinical outcomes of CT based HR-CTV delineation for HDR intracavitary brachytherapy in carcinoma cervix — a retrospective study. Reports of Practical Oncology and Radiotherapy 2021, Volume 26, Number 2, pages: 170-178. https://doi.org/10.5603/RPOR.a2021.0023 |
[2]
. However, dose optimization was done to reduce bladder and rectal dose. EQD2 doses were calculated for HR-CTV and point A. He found out that patients with HR-CTV D90 EQD2 dose greater ≥ 79.75 Gy had better locoregional control than patients receiving a dose less than that and he confirmed the feasibility of HR-CTV based planning in cervical cancer. Then, EMBRACE I was a prospective observational multicentric study. It was based on the concept of MR-IGABT (magnetic resonance-guided adaptive brachytherapy). The study showed that 85Gy of EQD2 to 90% of HR-CTV led to 95% of 3-year LC. This study provides large-scale evidence for dose prescription and helped us set a baseline for HR-CTV coverage to be around ≥ 80Gy EQD2
| [3] | Maximilian P. Schmid, MD; Jacob C. Lindegaard, MD. Risk Factors for Local Failure Following Chemoradiation and Magnetic Resonance Image-Guided Brachytherapy in Locally Advanced Cervical Cancer: Results From the EMBRACE-I Study. January 4, 2023. Volume 41, Issue 10. https://doi.org/10.1200/JCO.22.01096 |
[3]
.
RetroEMBRACE study which was the first retrospective comprehensive clinical multicentre report on IGABT, which allows dose escalation to the high-risk clinical target volume (HR-CTV) while sparing OARs. Showed an excellent LC (91%), PC - Pelvic control (87%), OS (74%), and CSS (79%) with limited severe morbidity. In the centers using MRI-based IGABT, the HR-CTV and the intermediate-risk CTV (IR-CTV) were contoured according to Gyn GEC-ESTRO recommendations I (HRCTV is the whole cervix and the presumed extra cervical tumor extension at the time of Brachytherapy, IRCTV includes the HRCTV along with adequate margin). In those using CT guidance, only the HRCTV was contoured. DVH parameters for the HR-CTV, IR-CTV, and OAR were calculated and reported according to Gyn GEC-ESTRO Recommendations II (i.e. by defining dose-volume parameters)
| [4] | Alina Sturdza, Richard Pötter. Image guided brachytherapy in locally advanced cervical cancer: Improved pelvic control and survival in RetroEMBRACE, a multicenter cohort study. 2016 Published by Elsevier Ireland Ltd. Radiotherapy and Oncology 120 (2016) 428-43. http://dx.doi.org/10.1016/j.radonc.2016.03.011 |
[4]
. Similarly, in this study, HR-CTV includes frank disease plus lower one-third of the uterus and upper one-third of the vagina (for cases with one-third or half vaginal involvement, contours were extended further down). Bladder and rectum were delineated as per visibility, after tracing the counters up and down, in both contrast and non-contrast arms. Point A-based treatment was planned and the plan was optimized as per clinicians' expertise, maintaining HR-CTV dose to around 78-80Gy EQD2. As intended in EMBRACE II. It's an interventional prospective multi-center study that aims to validate a dose prescription protocol, that escalates dose to the GTV and HR-CTV in tumors with large residual volume and de-escalates doses to the vagina and the OARs i.e. bladder and rectum. Hence, improved morbidity and QOL without compromising LC. The results of this study showed that a target dose of >85Gy EQD2 to HR-CTV-D90 is associated with a 3 yr LC of >96% in tumor volume of <30cc and >91% in tumor of >30cc
| [5] | Richard Pötter, Kari Tanderup. The EMBRACE II study: The outcome and prospect of two decades of evolution within the GEC-ESTRO GYN working group and the EMBRACE studies. version v.1.0. 2018 Jan 11: 9: 48-60. https://doi.org/10.1016/j.ctro.2018.01.001 |
[5]
. In our study, HR-CTV coverage was maintained irrespective of its volume and EQD2 doses to HR-CTV were maintained to 80-85 Gy EQD2 for all cases.
Leonel Varela Cagetti et al studied early clinical outcomes of adaptive brachytherapy for locally advanced cervical cancer. And concluded that the adaptability of treatment as per tumor response allows for better delivery of recommended doses and help to achieve comparative better LC then conventional ICBT. Adaptive treatment eventually leads to better target volume coverage, with lower rates of acute morbidity
| [6] | Leonel Varela Cagetti, MD, Christophe Zemmour. Early clinical outcomes of hybrid brachytherapy for locally advanced cervical cancer: making adverse situations in a favorable scenario. 2022; 14, 4: 321-331. https://doi.org/10.5114/jcb.2022.118831 |
[6]
.
Mame Daro Faye et al performed a single institution retrospective review to compare survival and overall toxicities at 50 months in the 2D versus 3D BT group. There was a significant decrease in overall late toxicities in the 3D-IGABT group compared to the 2D-BT group. Late gastrointestinal, genitourinary, and vaginal toxicities were 0% vs. 29.6%. grade ≥ 3 toxicity was low in both groups (2D-BT: 8.2% acute vs. 3D-BT: 6.3% acute
| [7] | Mame Daro Faye, Mariana Petruccelli Araujo. Safety and Efficacy of 2D Brachytherapy vs. 3D Image-Guided Adaptive Brachytherapy for Locally Advanced Cervical Cancer—A Single Institution Retrospective Study. 2023, 30, 4966-4978. https://doi.org/10.3390/curroncol30050375 |
[7]
. In our study, there were no grade 3 events noted, as we have performed 3D-IGABT wherever needed.
Weiping Wang et al performed a prospective single-institution observational study in China, which included only stage IIB patients with IMRT-based EBRT treatment. And dose escalated to pure point-A based MR-based brachytherapy, to a dose of 30-36Gy in 5-7 fractions, post EBRT with a dose of 50.4 Gy in 28 fractions. Although, the study has not documented the local control rate during the first follow-up, but has mentioned better control rates associated with an EQD2 value of > 85Gy. The late toxicity events reached up to G4; 1.3% and 0.8% genito-intestinal (GI) and genitourinary (GU) respectively. Similarly, G3 events were 1.3% for both. The incidence of G2 events was significantly higher for GI toxicity (13.7%) versus 9% for GU toxicity
| [8] | Weiping Wang, Qingyu Meng. Efficacy and toxicity of image-guided intensity-modulated radiation therapy combined with dose-escalated brachytherapy for stage IIB cervical cancer. 2017, Vol. 8, (No. 61), pp: 102965-102973. |
[8]
.
Vitaliana De Sanctis et al is another multicentric prospective study performed in Italy in 2023. Evaluated the outcomes and toxicities in LACC at 3 months and continued to follow up to 3 years with a similar aim. MR MR-based brachytherapy was performed, HR-CTV was defined as the whole cervix and was treated to a median dose of 21Gy in 3 fractions. MRI/PET CT was performed at the end of 3 months as per RECIST 1.1. Acute Grade 1 GU events were observed in 32.83% of patients and Grade 2 in 7.4%, whereas only one patient complained of acute G3 toxicity (1.49%). Acute grade 1 GI events occurred in 12/67 (17.91%) patients while 6/67 patients (8.95%) complained of acute grade 2 toxicity
| [9] | VITALIANA DE SANCTIS, GIUSEPPE FACONDO. Clinical Outcomes and Toxicity of CT-guided High Dose-rate Brachytherapy in Women With Locally-advanced Cervical Cancer. 3: 194-200 (2023). https://doi.org/10.21873/cdp.10201 |
[9]
.
Our study is a prospective observational study, where only organ-related LCR and acute-grade toxicities were assessed at 3 months. The above-mentioned studies have shown a significant reduction in the grade of GI and GU toxicities and better LC with the invention of IGABT treatment. We had similar findings, G2 toxicity was seen only in the rectum, that too only in 1 patient, the rest of the 53 patients either have G0 or G1, GI or GU events. These toxicities were significantly less in patients in whom contrast was not given (i.e. arm1), as shown in
Figures 6, 7. When the average D2cc dose was taken out for all three OARs (bladder, rectum, and bowel), and compared with the grade of toxicity events using the Mann-Whitney U test, none of the values was found to be significant. Whereas, the EMBRACE study showed that a D2cm
3 ≤ 65 Gy was associated with minor rectal morbidity, whereas a D2cm
3 ≥ 75 Gy was associated with major rectal morbidity. Similarly, EQD2 values were also not associated with the grade of toxicities in any of the OARs.
Takeaki Kusada et al analysis was similar to ours and concluded that D 2cc of OAR was not significant predictors of toxicities/complications
| [10] | Takeaki Kusada, Takafumi Toita. Computed tomography-based image-guided brachytherapy for cervical cancer: correlations between dose-volume parameters and clinical outcomes. Vol. 59, No. 1, 2018, pp. 67-76. https://doi.org/10.1093/jrr/rrx065 |
[10]
. It also showed 70 Gy was a marginally significant HR-CTV D90 cut-off affecting local control rates.
Lindegaard et al. developed 3D-printed tandem needle template (3DP TNT) in place of the ring channel. Nulliparous women and patients with vaginal stenosis and elderly were treated using these templates. Despite high tumour load LCR were comparable and incidence of G3 side effects were similar to EMBRACE I and retroEMBRACE group of patients. In our study we didn’t face any G3 toxicity, even with interstitial brachytherapy application
. As per Kaiyue Wang et al., it is advisable to combine physical examination and pre-BT MRI to improve CT-guided delineations. As Contrast enhancement may also reduce the variations in and dose impacts of target tissue. As departmental protocol at our institute, we have performed Pre-BT MRI for every patient and found it very beneficial for tumour delineation
| [12] | Kaiyue Wang, Junjie Wang. High-Dose-Rate Three-Dimensional Image-Guided Adaptive Brachytherapy (3D IGABT) for Locally Advanced Cervical Cancer (LACC): A Narrative Review on Imaging Modality and Clinical Evidence. Curr. Oncol. 2024, 31, 50-65. https://doi.org/10.3390/curroncol31010004 |
[12]
. Where Takeaki Kusada et al showed only a marginal significant LCR with EQD2 dose of 70Gy. Haruka Uezono et al, one of the largest series demonstrated the outcomes of CT-based IGBT along with hybrid IC/IS technique. Concluded that EQD2 for HR-CTV-D90%, if more than or equal to 75Gy leads to significantly better LCR (LCR improved from 80% to 93%)
| [13] | Haruka Uezono, Kayoko Tsujino. CT-based image-guided brachytherapy in uterine cervical cancer: Effect of tumor dose and volume on local control. 2022 Nov-Dec; 21(6): 814-822. https://doi.org/10.1016/j.brachy.2022.08.012 |
[13]
. Yu-Ting Xiu et al prognosticated cervical cancer patients based on different dose regimens given during BT. Mainly stage IIIB treated with ICRT and Interstitial BT tended to improve Disease free survival of patients when compared with ICRT alone, and obtained similar HR-CTV D
90 EQD
2 of 91 ±6 Gy (24Gy BT dose) and 107 ±4.5 Gy (with higher doses of 36Gy BT), whereas decreased OARs doses and its D
2cm3 (up to 7.5 Gy and 7.2 Gy) lowers late GI and GU toxicities, this study did not comment on acute toxicities which was our point of interest. Although, study enhanced importance of HR-CTV-D90% volume but, now we know that this cut-off has been reduced further from 91Gy to 75Gy EQD2 value for tumor control
| [14] | Yu-Ting Xiu, Fan-Xu Meng. Prognostic factors for IB2-IIIB cervical cancer patients treated by radiation therapy with high-dose-rate brachytherapy in a single-institution study. 2022 Aug; 14(4): 332-340. https://doi.org/10.5114/jcb.2022.118674 |
[14]
.
The variety of ICRT applicators used in our study quite matches Zhougshan Liu et al; this includes Fletchers family; where tandem with full and semi-ovoids of different sizes were used. Tandem and vaginal cylinders were only dedicated for frank vaginal disease, tandem and ring application was used mainly for small and superficial disease. Unlike in our case where vaginal applicators were having additional interstitial catheters for coverage of vagina and hence it was used for locally advanced cases with limited vaginal involvement. The author narrates about the ease and simplicity of these complex application, due to use of these varied applicators which use less training and reduced rate of injury. We, while using these applicators, concluded the same. Patients in both arms faced no serious injury during application
| [15] | Zhongshan Liu, Yangzhi Zhao. Imaging-guided brachytherapy for locally advanced cervical cancer: the main process and common techniques. 2020 Dec 1; 10(12): 4165-4177. |
[15]
.
6. Conclusions
The use of IGABT has definitely reduced the grade of toxicities and improved the local response rate.
The clinical implication of the result of our study suggests the use of non-contrast CT simulation for all brachytherapy patients considering significantly improved local control rates and low-grade acute toxicity events.
Contrast, if used meticulously, might lead to similar outcomes. In which case also use of contrast can be eliminated.
7. Limitations of Study
The average age in arm 2 was more. Which might lead to lesser OAR tolerance and more toxicities.
Although response rates in 1st visit might not be encouraging, but we lack long term data (as it was out of domain of this study) for these patients which can lead us to overall and disease-free survival for these patients.
We need meticulous learning of contrast implementation and refining of protocol for OARs. (As bladder volume and shape change with difference in volume of residual urine. Similarly, rectal volume changes with faulty instillation of rectal contrast without removing air from rectum or tube through which contrast is given. Even filling of rectal contrast is another challenge and needs training).
It is a small study to exactly interpolate the data with accurate results.
Abbreviations
OAR | Organ at Risk |
LC | Local Control |
MR Brachytherapy | Magnetic Resonance Imaging Based Brachytherapy |
CT guided brachytherapy | Computed-tomography- guided Brachytherapy |
IBS-GEC-ESTRO Recommendation | International Brachytherapy Society - Groupe Européen de Curiethérapie - European Society for Therapeutic Radiology and Oncology Recommendation |
LRR | Local Response Rate |
CCRT | Concurrent Chemotherapy and Radiation Therapy |
BT | Brachytherapy |
I.V. | Intra Venous |
LACC | Locally Advanced Cervical Cancer |
FIGO Stage | The International Federation of Gynecology and Obstetrics |
G1, G2 | Grade 1 and 2 |
D2cc | Dose to 2cc Volume of OAR |
EBRT | External Beam Radiation Therapy |
LCR | Local Control Rate |
IGABT | Image Guided Adaptive Brachytherapy |
LF | Local Failures |
MR-IGABT | Magnetic Resonance Imaging Guided Adaptive Brachytherapy |
HR-CTV | High Risk Clinical Target Volume |
EQD2 | Equivalent Dose to 2Gy |
HR-CTV D90 | 90% Dose to High-Risk Clinical Target Volume |
QOL | Quality of Life |
CTCAE | Common Terminology Criteria for Adverse Events |
HDR Brachytherapy | High Dose Rate Brachytherapy |
3DCRT | Three-Dimensional Conformal Radiation Therapy |
IMRT | Intensity Modulated Radiation Therapy |
VMAT | Volumetric Modulated Arc Therapy |
ICBT | Intracavitary Brachytherapy |
OT | Operation Theater |
TAUS | Trans Abdominal Ultra-sonography |
DVH | Dose Volume Histogram |
PET- CT | Positron Emission Tomography Computed Tomography |
PC | Pelvic Control |
OS | Overall Survival |
CSS | Cause Specific Survival |
IR-CTV | Intermediate Risk Clinical Target Volume |
3D-IGABT | 3-Dimensional Image Guided Adaptive Brachytherapy |
2D-BT | 2 Dimensional Brachytherapy |
GI toxicity | Gastro-Intestinal Toxicity |
GU toxicity | Gastro-Urinary Toxicity |
Acknowledgments
I would like to thank all those who have contributed to the completion of this study, including radiation oncologists, physicists, and technologists from the PSG Hospital, Department of Radiation Oncology. Special thanks to all the sisters, Varshini sister, Sophia, and Shakeela sisters. They had made a lot of efforts and had done all technical and monetary work discerningly.
I especially thank Dr. Balaji Sir, Director of PSG Institute of Oncology, for giving me an opportunity to work in a well-equipped department.
Author Contributions
Shreya Dwivedi: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Supervision, Visualization, Writing - original draft
Aswin Chandran Veluthattil: Investigation, Project administration, Resources, Supervision, Validation, Writing - review & editing
Madhulika Vijayakumar: Investigation, Project administration, Resources, Validation
Nithiyaanandan Natarajan: Investigation, Project administration, Resources, Validation
Anjali Thiruthiyil: Data curation, Investigation, Project administration, Validation, Writing - review & editing
Dinesh Babu: Investigation, Project administration, Software, Validation
Shankar Sekar: Investigation, Project administration, Software, Validation
Institutional Review Board Statement
The study was approved by the Institutional Review Board (or Ethics Committee) of the PSG Hospital (Ref. No: PSG/IHEC/20241 Appr lFBl049).
Data Availability Statement
The data is available from the corresponding author upon request.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix
Table 6. Bowel Toxicity.
| Group | Total (%) | p Value |
CASE (%) | CONTROL (%) |
Toxicity Grade | 0 | 14 (87.5) | 19 (100) | 33 (94.29) | 0.112 |
1 | 2 (12.5) | 0 (0) | 2 (5.71) |
Total | 16 (100) | 19 (100) | 35 (100) | |
Table 7. Bowel toxicity when compared with EQD2.
| BO-EQD2 | Total |
60-70 | 71-80 | 81-90 |
Toxicity Grade | 0 | Count | 6 | 6 | 2 | 14 |
% within BO-EQD2 | 100.0 | 85.7 | 66.7 | 87.5 |
1 | Count | 0 | 1 | 1 | 2 |
% within BO-EQD2 | 0.0 | 14.3 | 33.3 | 12.5 |
Total | Count | 6 | 7 | 3 | 16 |
% within BO-EQD2 | 100.0 | 100.0 | 100.0 | 100.0 |
P value: 0.35
Table 8. Bowel toxicity compared with D2cc values.
| BO-D2 Average | Total |
1-3 | 4-6 |
Toxicity Grade | 0 | Count | 7 | 6 | 13 |
% within BO-D2 AVERAGE | 100.0 | 75.0 | 86.7 |
1 | Count | 0 | 2 | 2 |
% within BO-D2 AVERAGE | 0.0 | 25.0 | 13.3 |
Total | Count | 7 | 8 | 15 |
% within BO-D2 AVERAGE | 100.0 | 100.0 | 100.0 |
p-value: 0.155
Table 9. Bladder toxicity compared with EQD2 values.
| B-EQD2 | Total |
70-80 | 81-90 | 91-100 |
Toxicity Grade | 0 | Count | 1 | 8 | 4 | 13 |
% within B-EQD2 | 100.0 | 72.7 | 100.0 | 81.3 |
1 | Count | 0 | 3 | 0 | 3 |
% within B-EQD2 | 0.0 | 27.3 | 0.0 | 18.8 |
Total | Count | 1 | 11 | 4 | 16 |
% within B-EQD2 | 100.0 | 100.0 | 100.0 | 100.0 |
p-value: 0.43
Table 10. Bladder toxicity compared with D2cc values.
| B-D2 AVERAGE | Total |
4-6 | 7-8 |
Toxicity Grade | 0 | Count | 6 | 7 | 13 |
% within B-D2 Average | 85.7 | 87.5 | 86.7 |
1 | Count | 1 | 1 | 2 |
% within B-D2 Average | 14.3 | 12.5 | 13.3 |
Total | Count | 7 | 8 | 15 |
% within B-D2 Average | 100.0 | 100.0 | 100.0 |
p-value: 0.919
Table 11. Rectum toxicity when compared with EQD2 values.
| R-EQD2 | Total |
72-75 | 75-80 | 80-85 |
Toxicity Grade | 0 | Count | 1 | 7 | 3 | 11 |
% within R-EQD2 | 50.0 | 63.6 | 100.0 | 68.8 |
1 | Count | 1 | 3 | 0 | 4 |
% within R-EQD2 | 50.0 | 27.3 | 0.0 | 25.0 |
2 | Count | 0 | 1 | 0 | 1 |
% within R-EQD2 | 0.0 | 9.1 | 0.0 | 6.3 |
Total | Count | 2 | 11 | 3 | 16 |
% within R-EQD2 | 100.0 | 100.0 | 100.0 | 100.0 |
P: 0.681
Table 12. Rectum toxicity when compared with EQD2 values.
| R-D2 AVERAGE | Total |
4-6 |
Toxicity Grade | 0 | Count | 11 | 11 |
% within R-D2 AVERAGE | 73.3 | 73.3 |
1 | Count | 3 | 3 |
% within R-D2 AVERAGE | 20.0 | 20.0 |
2 | Count | 1 | 1 |
% within R-D2 AVERAGE | 6.7 | 6.7 |
Total | Count | 15 | 15 |
% within R-D2 AVERAGE | 100.0 | 100.0 |
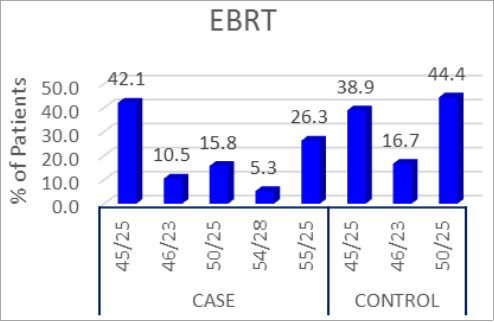
Figure 8. Percentage of patients with different EBRT doses in both the groups.
Figure 9. Percentage (%) of patients who have undergone different brachytherapy doses in each group.
References
| [1] |
Rebecca L Siegel, Kimberly D Miller. Cancer statistics, 2023. 2023 Jan; 73(1): 17-48.
https://doi.org/10.3322/caac.21763
|
| [2] |
Anis Bandyopadhyay, Arnab Kumar Ghosh, Bappaditya Chhatui. Dosimetric and clinical outcomes of CT based HR-CTV delineation for HDR intracavitary brachytherapy in carcinoma cervix — a retrospective study. Reports of Practical Oncology and Radiotherapy 2021, Volume 26, Number 2, pages: 170-178.
https://doi.org/10.5603/RPOR.a2021.0023
|
| [3] |
Maximilian P. Schmid, MD; Jacob C. Lindegaard, MD. Risk Factors for Local Failure Following Chemoradiation and Magnetic Resonance Image-Guided Brachytherapy in Locally Advanced Cervical Cancer: Results From the EMBRACE-I Study. January 4, 2023. Volume 41, Issue 10.
https://doi.org/10.1200/JCO.22.01096
|
| [4] |
Alina Sturdza, Richard Pötter. Image guided brachytherapy in locally advanced cervical cancer: Improved pelvic control and survival in RetroEMBRACE, a multicenter cohort study. 2016 Published by Elsevier Ireland Ltd. Radiotherapy and Oncology 120 (2016) 428-43.
http://dx.doi.org/10.1016/j.radonc.2016.03.011
|
| [5] |
Richard Pötter, Kari Tanderup. The EMBRACE II study: The outcome and prospect of two decades of evolution within the GEC-ESTRO GYN working group and the EMBRACE studies. version v.1.0. 2018 Jan 11: 9: 48-60.
https://doi.org/10.1016/j.ctro.2018.01.001
|
| [6] |
Leonel Varela Cagetti, MD, Christophe Zemmour. Early clinical outcomes of hybrid brachytherapy for locally advanced cervical cancer: making adverse situations in a favorable scenario. 2022; 14, 4: 321-331.
https://doi.org/10.5114/jcb.2022.118831
|
| [7] |
Mame Daro Faye, Mariana Petruccelli Araujo. Safety and Efficacy of 2D Brachytherapy vs. 3D Image-Guided Adaptive Brachytherapy for Locally Advanced Cervical Cancer—A Single Institution Retrospective Study. 2023, 30, 4966-4978.
https://doi.org/10.3390/curroncol30050375
|
| [8] |
Weiping Wang, Qingyu Meng. Efficacy and toxicity of image-guided intensity-modulated radiation therapy combined with dose-escalated brachytherapy for stage IIB cervical cancer. 2017, Vol. 8, (No. 61), pp: 102965-102973.
|
| [9] |
VITALIANA DE SANCTIS, GIUSEPPE FACONDO. Clinical Outcomes and Toxicity of CT-guided High Dose-rate Brachytherapy in Women With Locally-advanced Cervical Cancer. 3: 194-200 (2023).
https://doi.org/10.21873/cdp.10201
|
| [10] |
Takeaki Kusada, Takafumi Toita. Computed tomography-based image-guided brachytherapy for cervical cancer: correlations between dose-volume parameters and clinical outcomes. Vol. 59, No. 1, 2018, pp. 67-76.
https://doi.org/10.1093/jrr/rrx065
|
| [11] |
Jacob Christian Lindegaard. Individualised 3D printed vaginal template for MRI guided brachytherapy in locally advanced cervical cancer. 2016 Jan; 118(1): 173-5.
https://doi.org/10.1016/j.radonc.2015.12.012
|
| [12] |
Kaiyue Wang, Junjie Wang. High-Dose-Rate Three-Dimensional Image-Guided Adaptive Brachytherapy (3D IGABT) for Locally Advanced Cervical Cancer (LACC): A Narrative Review on Imaging Modality and Clinical Evidence. Curr. Oncol. 2024, 31, 50-65.
https://doi.org/10.3390/curroncol31010004
|
| [13] |
Haruka Uezono, Kayoko Tsujino. CT-based image-guided brachytherapy in uterine cervical cancer: Effect of tumor dose and volume on local control. 2022 Nov-Dec; 21(6): 814-822.
https://doi.org/10.1016/j.brachy.2022.08.012
|
| [14] |
Yu-Ting Xiu, Fan-Xu Meng. Prognostic factors for IB2-IIIB cervical cancer patients treated by radiation therapy with high-dose-rate brachytherapy in a single-institution study. 2022 Aug; 14(4): 332-340.
https://doi.org/10.5114/jcb.2022.118674
|
| [15] |
Zhongshan Liu, Yangzhi Zhao. Imaging-guided brachytherapy for locally advanced cervical cancer: the main process and common techniques. 2020 Dec 1; 10(12): 4165-4177.
|
Cite This Article
-
APA Style
Dwivedi, S., Veluthattil, A. C., Vijayakumar, M., Natarajan, N., Thiruthiyil, A., et al. (2025). Comparative Prospective Study Assessing Early Clinical Outcomes with or Without Use of Contrast Enhancement in CT Based Image Guided HDR Brachytherapy. International Journal of Clinical Oncology and Cancer Research, 10(2), 36-50. https://doi.org/10.11648/j.ijcocr.20251002.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Dwivedi, S.; Veluthattil, A. C.; Vijayakumar, M.; Natarajan, N.; Thiruthiyil, A., et al. Comparative Prospective Study Assessing Early Clinical Outcomes with or Without Use of Contrast Enhancement in CT Based Image Guided HDR Brachytherapy. Int. J. Clin. Oncol. Cancer Res. 2025, 10(2), 36-50. doi: 10.11648/j.ijcocr.20251002.11
Copy
|
Download
AMA Style
Dwivedi S, Veluthattil AC, Vijayakumar M, Natarajan N, Thiruthiyil A, et al. Comparative Prospective Study Assessing Early Clinical Outcomes with or Without Use of Contrast Enhancement in CT Based Image Guided HDR Brachytherapy. Int J Clin Oncol Cancer Res. 2025;10(2):36-50. doi: 10.11648/j.ijcocr.20251002.11
Copy
|
Download
-
@article{10.11648/j.ijcocr.20251002.11,
author = {Shreya Dwivedi and Aswin Chandran Veluthattil and Madhulika Vijayakumar and Nithiyaanandan Natarajan and Anjali Thiruthiyil and Dinesh Babu and Shankar Sekar},
title = {Comparative Prospective Study Assessing Early Clinical Outcomes with or Without Use of Contrast Enhancement in CT Based Image Guided HDR Brachytherapy},
journal = {International Journal of Clinical Oncology and Cancer Research},
volume = {10},
number = {2},
pages = {36-50},
doi = {10.11648/j.ijcocr.20251002.11},
url = {https://doi.org/10.11648/j.ijcocr.20251002.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcocr.20251002.11},
abstract = {Background: Brachytherapy has been part of the standard of care in the treatment of cervical cancer. Brachytherapy has evolved from two to three-dimensional treatment for better volume delineation for target and OAR thus leading to better LC and reduced toxicities. Presently, MR Brachytherapy is the gold standard. However, its use is limited by its availability and patient logistics. To combat this barrier, CT-guided brachytherapy guidelines were established over time and have been proven non-inferior to MR brachytherapy. The recent IBS-GEC-ESTRO recommendation 2021 has advised the use of contrast to delineate tumor and normal tissue. The objective of this study is to assess LRR and normal tissue toxicities at 3 months with the use of contrast versus non-contrast CT-based contouring. Material and methods: Data from all patients with proven LACC, treated by brachytherapy after CCRT between May 2023 and Sep'2024 were reviewed. CCRT followed by BT. Two patient data sets included arm1; without and arm2; with contrast during brachytherapy CT simulation. 1-2 ml contrast in the bladder and 4-5 ml rectum contrast diluted in 20 ml and 10-15 ml NS, respectively. I.V. contrast was given only to patients with residual disease. CT-based contouring and planning were done similarly in both arms. Results: Forty patients with LACC, as per recent FIGO stage (II A: 5.72%, II B: 22.86%, III B: 17.41%, III C: 40%, and IV: 14.29%), who completed treatment were part of this study. Out of 40 patients, 11 (27%) underwent adaptive brachytherapy. Higher stages were observed more commonly in arm 1. LRR was higher in arm 1 (85%) than arm2 42%. Defaulters in arm 2 were more (23.81%) than in arm 1 (5%). In a median follow-up of 3 months, 10% of local failure was observed in arm 1 and 33.33% in arm 2. No acute toxicities were seen in 55% of the cases (22/35 patients). No High-grade acute toxicity events (> grade 2) were reported. A significant difference was observed in the G1 bladder and rectal toxicity in both arms. G2 rectal toxicity was reported only in arm 2 in 1 patient. Only G1 Bowel toxicity was seen and was insignificant between both arms. Conclusion: Local control was significantly more in arm 1 (p- 0.019). Only G1 toxicities were observed in both arms. No significant difference was observed in the D2cc volume of any of the OARs between both groups. This implies, no significance of implementing contrast material in CT-based brachytherapy treatment.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Comparative Prospective Study Assessing Early Clinical Outcomes with or Without Use of Contrast Enhancement in CT Based Image Guided HDR Brachytherapy
AU - Shreya Dwivedi
AU - Aswin Chandran Veluthattil
AU - Madhulika Vijayakumar
AU - Nithiyaanandan Natarajan
AU - Anjali Thiruthiyil
AU - Dinesh Babu
AU - Shankar Sekar
Y1 - 2025/03/26
PY - 2025
N1 - https://doi.org/10.11648/j.ijcocr.20251002.11
DO - 10.11648/j.ijcocr.20251002.11
T2 - International Journal of Clinical Oncology and Cancer Research
JF - International Journal of Clinical Oncology and Cancer Research
JO - International Journal of Clinical Oncology and Cancer Research
SP - 36
EP - 50
PB - Science Publishing Group
SN - 2578-9511
UR - https://doi.org/10.11648/j.ijcocr.20251002.11
AB - Background: Brachytherapy has been part of the standard of care in the treatment of cervical cancer. Brachytherapy has evolved from two to three-dimensional treatment for better volume delineation for target and OAR thus leading to better LC and reduced toxicities. Presently, MR Brachytherapy is the gold standard. However, its use is limited by its availability and patient logistics. To combat this barrier, CT-guided brachytherapy guidelines were established over time and have been proven non-inferior to MR brachytherapy. The recent IBS-GEC-ESTRO recommendation 2021 has advised the use of contrast to delineate tumor and normal tissue. The objective of this study is to assess LRR and normal tissue toxicities at 3 months with the use of contrast versus non-contrast CT-based contouring. Material and methods: Data from all patients with proven LACC, treated by brachytherapy after CCRT between May 2023 and Sep'2024 were reviewed. CCRT followed by BT. Two patient data sets included arm1; without and arm2; with contrast during brachytherapy CT simulation. 1-2 ml contrast in the bladder and 4-5 ml rectum contrast diluted in 20 ml and 10-15 ml NS, respectively. I.V. contrast was given only to patients with residual disease. CT-based contouring and planning were done similarly in both arms. Results: Forty patients with LACC, as per recent FIGO stage (II A: 5.72%, II B: 22.86%, III B: 17.41%, III C: 40%, and IV: 14.29%), who completed treatment were part of this study. Out of 40 patients, 11 (27%) underwent adaptive brachytherapy. Higher stages were observed more commonly in arm 1. LRR was higher in arm 1 (85%) than arm2 42%. Defaulters in arm 2 were more (23.81%) than in arm 1 (5%). In a median follow-up of 3 months, 10% of local failure was observed in arm 1 and 33.33% in arm 2. No acute toxicities were seen in 55% of the cases (22/35 patients). No High-grade acute toxicity events (> grade 2) were reported. A significant difference was observed in the G1 bladder and rectal toxicity in both arms. G2 rectal toxicity was reported only in arm 2 in 1 patient. Only G1 Bowel toxicity was seen and was insignificant between both arms. Conclusion: Local control was significantly more in arm 1 (p- 0.019). Only G1 toxicities were observed in both arms. No significant difference was observed in the D2cc volume of any of the OARs between both groups. This implies, no significance of implementing contrast material in CT-based brachytherapy treatment.
VL - 10
IS - 2
ER -
Copy
|
Download