Introduction: Male infertility remains a neglected public health problem in sub-Saharan Africa, characterized by significant diagnostic delays due to sociocultural and economic barriers. This study aims to analyze the epidemiological, clinical, and paraclinical profiles of male infertility and to identify factors contributing to delayed consultation at the Yalgado Ouédraogo University Hospital (CHU-YO). Methods: A descriptive cross-sectional study was conducted from October 2021 to September 2023, including 111 men evaluated for infertility. Data were collected retrospectively from medical records and supplemented by structured interviews. Statistical analyses were performed using EPI Info 7.2. Results: The hospital prevalence of male infertility was 5.39%. The mean age was 35.87 years; 41.44% were civil servants and 29.73% had no formal education. The mean consultation delay was 50 months. Oligospermia (45%) and azoospermia (32%) were the most frequent sperm abnormalities. A varicocele was detected in 48.65% of patients. The main factors for delay included financial constraints (65.52%), initial consultations with non-specialists (61.25%), and cultural beliefs attributing infertility to women (24.14%). Conclusion: Male infertility in Burkina Faso is associated with significant diagnostic delays influenced by socioeconomic and cultural factors. A multisectoral approach - combining public health, anthropology, and social policies - is essential to improve access to andrological care in resource-limited countries.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
, with a particularly concerning prevalence in sub-Saharan Africa. In Burkina Faso, this condition primarily affects a young and active population
[2]
Kirakoya B, Zongo B, Pare A, et al. Epidemiological and Clinical Profile of Male Hypofertility in Consultation at the Urology-Andrology of Yalgado Ouedraogo Teaching Hospital (Burkina Faso). Adv Sex Med. 2015; 5(1): 1-6.
, but is characterized by significant consultation delays often exceeding three years
[2]
Kirakoya B, Zongo B, Pare A, et al. Epidemiological and Clinical Profile of Male Hypofertility in Consultation at the Urology-Andrology of Yalgado Ouedraogo Teaching Hospital (Burkina Faso). Adv Sex Med. 2015; 5(1): 1-6.
These delays are explained by multifactorial obstacles including economic barriers, the persistence of traditional beliefs attributing infertility to women
[3]
Tabong PTN, Adongo PB. Infertility and childlessness: a qualitative study of the experiences of infertile couples in Northern Ghana. BMC Pregnancy Childbirth. 2013; 13: 72.
Niang L, Ndoye M, Labou I, et al. [Epidemiological and clinical profile of male infertility at the General Hospital of Grand-Yoff, Senegal: about 492 cases]. Basic Clin Androl. 2009; 19(2): 103-107. [French]
[3, 4]
, and the stigmatization of infertile men. However, as highlighted by international recommendations
[5]
Huyghe E, Boitrelle F, Methorst C, et al. [Recommendations from the AFU and SALF concerning the evaluation of the infertile man]. Prog Urol. 2021; 31(3): 131-144. [French]
[5]
, early andrological evaluation is essential to optimize the chances of therapeutic success.
This study aims to update data on the profile of male infertility in Burkina Faso and to identify the specific determinants of consultation delays, in order to develop public health strategies adapted to the local context.
2. Methods
2.1. Study Type and Setting
A descriptive cross-sectional study was conducted in the Urology-Andrology Department of CHU-YO, one of the reference hospitals in Ouagadougou.
2.2. Participants
111 men presenting for infertility evaluation between October 2021 and September 2023 were included. Inclusion criteria: more than 12 months of unprotected sexual intercourse without conception, with a confirmed fertile female partner.
2.3. Data Collection
Data were extracted from medical records and supplemented by interviews using a structured questionnaire. Variables included sociodemographic characteristics, clinical history, sperm parameters (according to WHO 2021 criteria), hormonal assays (FSH, testosterone), and scrotal ultrasounds.
2.4. Statistical Analysis
Data were analyzed with EPI Info 7.2. Categorical variables were expressed as frequencies/percentages, continuous variables as means ± standard deviation. The Chi² test and Fisher's exact test were used for associations (p<0.05 significant).
3. Results
3.1. Sociodemographic Characteristics
Our study included 111 patients consulting for male infertility. The mean age was 35.87 years (standard deviation: 6.2; range: 23–55 years). The most represented age group was 30–39 years (58.56%). Professionally, a majority of patients were civil servants (41.44%), followed by merchants/traders (31.53%). Educational level was variable: 33.33% had a secondary level education, 29.73% had no formal education, and 19.82% had a higher education level. Regarding marital status, 98.2% were married, with a predominance of primary infertility (81%).
3.2. Consultation Delay and Care Pathway
The mean consultation delay was 50 months (4 years and 2 months), with a range from 1 to 216 months. Only 13.51% of patients had consulted directly in urology-andrology. The majority (61.25%) had first consulted other professionals: gynecologists (36.03%), general practitioners (15.32%), or traditional healers (9.9%).
3.3. Clinical Data and History
The most frequent medical histories included alcohol consumption (24.32%), urethritis (21.62%), and childhood urogenital schistosomiasis (16.22%). Physical examination revealed a varicocele in 48.65% of patients (including 53 bilateral cases), testicular hypotrophy (26.13%), and cryptorchidism (2.7%).
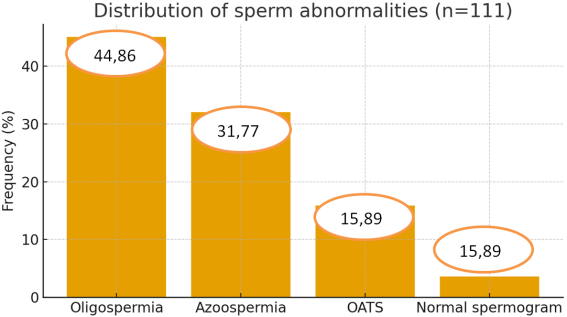
3.4. Sperm and Hormonal Profile
The semen analysis was abnormal in 96.4% of cases. The main abnormalities are illustrated in Figure 1.
Figure 1. Distribution of patients according to semen analysis abnormalities.
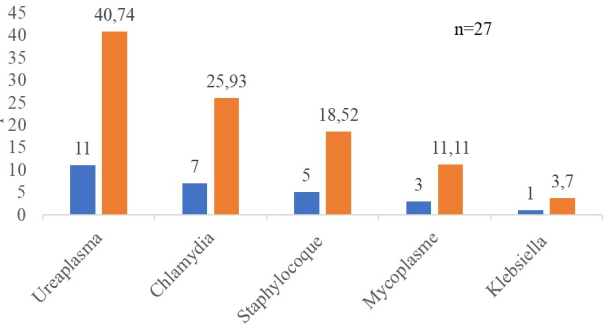
Sperm culture, performed in 89% of patients, was positive in 24.32% of cases. The most frequent pathogens were Ureaplasma urealyticum (40.74%) and Chlamydia trachomatis (25.93%). Figure 2 illustrates the distribution of patients according to the isolated pathogen.
Among patients who underwent hormonal testing (41.44% for FSH, 38.74% for testosterone), 13 azoospermic patients had elevated FSH, suggesting a secretory origin.
Figure 2. Distribution of patients according to pathogens isolated on sperm culture. Orange bars indicate frequency (%), blue bars indicate number of patients (n).
3.5. Doppler Scrotal Ultrasound Profile
The Doppler scrotal ultrasound was abnormal in 68.5% (n=76) of patients; 27% (n=30) had not undergone ultrasound and 4.5% (n=5) had a normal ultrasound. Scrotal ultrasound identified a varicocele in 47.75% of patients and testicular hypotrophy in 40.54%.
Table 1. Distribution of patients according to scrotal ultrasound abnormalities.
Ultrasound abnormalities
Number (n)
Frequency (%)
Varicocele
53
47.75
- Bilateral
52
46.85
- Right
0
0
- Left
1
0.9
Testicular hypotrophy
45
40.54
- Bilateral
36
32.43
- Left
8
7.2
- Right
1
0.9
Hydrocele
12
10.81
Epididymal cyst
15
13.51
Atrophy
7
6.3
The varicocele was grade II in 79.25% and grade III in 20.75% of cases.
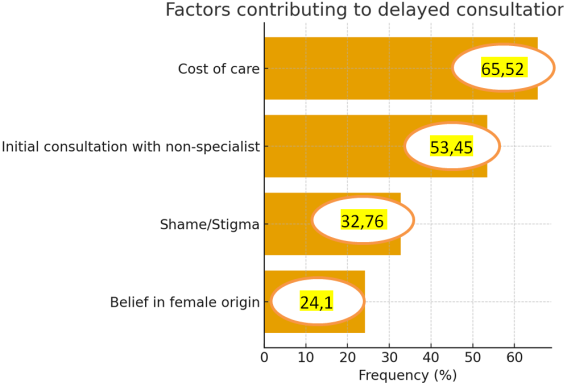
3.6. Factors for Consultation Delay
The main reported factors are illustrated in Figure 3.
Figure 3. Distribution of patients according to the factor for consultation delay.
In multivariate analysis, cost of care (OR = 3.41; 95% CI: 1.43–8.10; p=0.008) and initial referral pathway (OR = 14.11; 95% CI: 3.59–55.44; p<0.001) were significantly associated with a prolonged consultation delay.
4. Discussion
Our study confirms that male infertility in Burkina Faso primarily affects young men (mean age: 35.87 years), who are active and often poorly educated. These results are consistent with those reported by Kirakoya et al. in Ouagadougou
[2]
Kirakoya B, Zongo B, Pare A, et al. Epidemiological and Clinical Profile of Male Hypofertility in Consultation at the Urology-Andrology of Yalgado Ouedraogo Teaching Hospital (Burkina Faso). Adv Sex Med. 2015; 5(1): 1-6.
Niang L, Ndoye M, Labou I, et al. [Epidemiological and clinical profile of male infertility at the General Hospital of Grand-Yoff, Senegal: about 492 cases]. Basic Clin Androl. 2009; 19(2): 103-107. [French]
[4]
. The predominance of civil servants and traders probably reflects a recruitment bias in a tertiary hospital setting, where access to care remains limited for rural and disadvantaged populations
[6]
Somé EN, Bouncoungou J, Poda JN. Prevalence of the Infertility Among Couples in Ouagadougou (Burkina Faso): a Population-based Survey. Open Public Health J. 2016; 9(1): 88-97.
The mean consultation delay (50 months) is particularly concerning. It exceeds that observed in other West African studies, such as that of Kbirou et al. in Morocco (36 months)
[7]
Kbirou A, Jandou I, Adnane E, et al. [Epidemiological and clinical profile of male infertility: a descriptive and analytical cross-sectional observational study]. Sexologies. 2022; 31(2): 117-122. [French]
[7]
or Epoupa Ngalle et al. in Cameroon (40 months)
[8]
Epoupa Ngalle FG, Mbouche LO, Mody Mpah EH, et al. Clinical and morphological profile of male infertility in 3 reference hospitals in the city of Douala in Cameroon. Afr J Urol. 2023; 29(1): 77-81.
[8]
. This delay is largely explained by profound sociocultural factors: persistence of beliefs attributing infertility to women, stigmatization of infertile men, and primary recourse to traditional healers
[3]
Tabong PTN, Adongo PB. Infertility and childlessness: a qualitative study of the experiences of infertile couples in Northern Ghana. BMC Pregnancy Childbirth. 2013; 13: 72.
. These severe disturbances could be linked to neglected genital infections (ureaplasma, chlamydia), as highlighted by Saint et al.
[9]
Saint F, Huyghe E, Methorst C, et al. [Infections and male infertility]. Prog Urol. 2023; 33(13): 636-652. [French]
[9]
, environmental exposure to pesticides and heavy metals (mercury), common in artisanal mining contexts
[10]
Bendayan M, Alter L, Swierkowski-Blanchard N, et al. [Toxics, lifestyle, environment: what impacts on male fertility?]. Gynecol Obstet Fertil Senol. 2018; 46(1): 47-56. [French]
[10]
and underdiagnosed conditions like varicocele (48.65% here), whose impact on spermatogenesis is well established
[11]
Schill WB, Comhaire FH, Hargreave TB. Andrology for the Clinician. New York, Springer; 2006. 645 p. ISBN 978-3-540-23171-4.
[11]
.
The low proportion of hormonal tests performed (≤41%) reflects limited access to specialized investigations. However, as recommended by Huyghe et al.
[5]
Huyghe E, Boitrelle F, Methorst C, et al. [Recommendations from the AFU and SALF concerning the evaluation of the infertile man]. Prog Urol. 2021; 31(3): 131-144. [French]
[5]
, the minimal hormonal workup (FSH, testosterone) is essential to guide the etiological diagnosis.
Our analysis identifies two major determinants of delay:
1) Cost of care: a predominant factor in a context where infertility management remains the responsibility of patients
[12]
World Health Organization. WHO Laboratory Manual for the Examination and Processing of Human Semen. 6th ed. WHO; 2021.
2) Care pathway: the majority of patients first consult gynecology or general medicine, where male infertility is often under-evaluated
[13]
Huyghe E, Salloum A. [When and why to resort to an andrology consultation?]. J Gynecol Obstet Biol Reprod. 2009; 38: F19-F25. [French]
[13]
.
These results corroborate the work of Tabong and Adongo in Ghana
[3]
Tabong PTN, Adongo PB. Infertility and childlessness: a qualitative study of the experiences of infertile couples in Northern Ghana. BMC Pregnancy Childbirth. 2013; 13: 72.
, who emphasize the role of social norms in diagnostic delay. The stigmatization of infertile men discourages them from consulting early, while traditional beliefs steer them towards unvalidated management approaches.
To reduce consultation delay, an integrated strategy is necessary: community awareness to demystify male infertility, training of frontline professionals (general practitioners, midwives) in basic andrological screening, subsidizing investigations (semen analysis, hormonal assays) in the public system and development of andrological care services outside regional capitals.
Our study presents several limitations. First, the sample size (n=111) is modest, and recruitment from a single university hospital introduces selection bias, as rural and primary care populations are underrepresented. Second, genetic analyses such as Y-chromosome microdeletions and karyotyping were not available, which limited the etiological evaluation of azoospermic patients. These genetic data (Y deletions, karyotype) are nevertheless crucial in azoospermia
[14]
Gonçalves C, Cunha M, Rocha E, et al. Y-chromosome microdeletions in nonobstructive azoospermia and severe oligozoospermia. Asian J Androl. 2017; 19(3): 338-345.
[14]
. Third, only 41% of patients benefited from hormonal testing (FSH, testosterone), restricting the completeness of endocrine assessment. These limitations highlight the need for larger, multicenter studies with broader access to genetic and hormonal investigations.
5. Conclusion
This study highlights the epidemiological and clinical profile of male infertility in Burkina Faso and identifies the main factors for consultation delay. The combination of financial, cultural, and systemic barriers significantly delays management, worsening the reproductive prognosis for couples. A multisectoral approach - combining public health, anthropology, and social policies - is essential to improve access to andrological care in resource-limited countries.
Kirakoya B, Zongo B, Pare A, et al. Epidemiological and Clinical Profile of Male Hypofertility in Consultation at the Urology-Andrology of Yalgado Ouedraogo Teaching Hospital (Burkina Faso). Adv Sex Med. 2015; 5(1): 1-6.
Tabong PTN, Adongo PB. Infertility and childlessness: a qualitative study of the experiences of infertile couples in Northern Ghana. BMC Pregnancy Childbirth. 2013; 13: 72.
Niang L, Ndoye M, Labou I, et al. [Epidemiological and clinical profile of male infertility at the General Hospital of Grand-Yoff, Senegal: about 492 cases]. Basic Clin Androl. 2009; 19(2): 103-107. [French]
[5]
Huyghe E, Boitrelle F, Methorst C, et al. [Recommendations from the AFU and SALF concerning the evaluation of the infertile man]. Prog Urol. 2021; 31(3): 131-144. [French]
[6]
Somé EN, Bouncoungou J, Poda JN. Prevalence of the Infertility Among Couples in Ouagadougou (Burkina Faso): a Population-based Survey. Open Public Health J. 2016; 9(1): 88-97.
Kbirou A, Jandou I, Adnane E, et al. [Epidemiological and clinical profile of male infertility: a descriptive and analytical cross-sectional observational study]. Sexologies. 2022; 31(2): 117-122. [French]
[8]
Epoupa Ngalle FG, Mbouche LO, Mody Mpah EH, et al. Clinical and morphological profile of male infertility in 3 reference hospitals in the city of Douala in Cameroon. Afr J Urol. 2023; 29(1): 77-81.
[9]
Saint F, Huyghe E, Methorst C, et al. [Infections and male infertility]. Prog Urol. 2023; 33(13): 636-652. [French]
[10]
Bendayan M, Alter L, Swierkowski-Blanchard N, et al. [Toxics, lifestyle, environment: what impacts on male fertility?]. Gynecol Obstet Fertil Senol. 2018; 46(1): 47-56. [French]
[11]
Schill WB, Comhaire FH, Hargreave TB. Andrology for the Clinician. New York, Springer; 2006. 645 p. ISBN 978-3-540-23171-4.
[12]
World Health Organization. WHO Laboratory Manual for the Examination and Processing of Human Semen. 6th ed. WHO; 2021.
Huyghe E, Salloum A. [When and why to resort to an andrology consultation?]. J Gynecol Obstet Biol Reprod. 2009; 38: F19-F25. [French]
[14]
Gonçalves C, Cunha M, Rocha E, et al. Y-chromosome microdeletions in nonobstructive azoospermia and severe oligozoospermia. Asian J Androl. 2017; 19(3): 338-345.
Sawadogo, H., Yameogo, C. A. M. K. D., Kirakoya, B., Pare, A., Ilachane, A. A., et al. (2025). Male Infertility in Burkina Faso: Epidemiological, Clinical, and Sociocultural Determinants of Delayed Andrological Consultation. International Journal of Clinical Urology, 9(2), 158-162. https://doi.org/10.11648/j.ijcu.20250902.19
Sawadogo, H.; Yameogo, C. A. M. K. D.; Kirakoya, B.; Pare, A.; Ilachane, A. A., et al. Male Infertility in Burkina Faso: Epidemiological, Clinical, and Sociocultural Determinants of Delayed Andrological Consultation. Int. J. Clin. Urol.2025, 9(2), 158-162. doi: 10.11648/j.ijcu.20250902.19
Sawadogo H, Yameogo CAMKD, Kirakoya B, Pare A, Ilachane AA, et al. Male Infertility in Burkina Faso: Epidemiological, Clinical, and Sociocultural Determinants of Delayed Andrological Consultation. Int J Clin Urol. 2025;9(2):158-162. doi: 10.11648/j.ijcu.20250902.19
@article{10.11648/j.ijcu.20250902.19,
author = {Hassami Sawadogo and Clotaire Alexis Marie Kiemdiba Donega Yameogo and Brahima Kirakoya and Abdoul-Karim Pare and Ahmad Almoctar Ilachane and Jean de la Croix Millogo and Adama Ouattara and Fasnewinde Aristide Kabore},
title = {Male Infertility in Burkina Faso: Epidemiological, Clinical, and Sociocultural Determinants of Delayed Andrological Consultation
},
journal = {International Journal of Clinical Urology},
volume = {9},
number = {2},
pages = {158-162},
doi = {10.11648/j.ijcu.20250902.19},
url = {https://doi.org/10.11648/j.ijcu.20250902.19},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20250902.19},
abstract = {Introduction: Male infertility remains a neglected public health problem in sub-Saharan Africa, characterized by significant diagnostic delays due to sociocultural and economic barriers. This study aims to analyze the epidemiological, clinical, and paraclinical profiles of male infertility and to identify factors contributing to delayed consultation at the Yalgado Ouédraogo University Hospital (CHU-YO). Methods: A descriptive cross-sectional study was conducted from October 2021 to September 2023, including 111 men evaluated for infertility. Data were collected retrospectively from medical records and supplemented by structured interviews. Statistical analyses were performed using EPI Info 7.2. Results: The hospital prevalence of male infertility was 5.39%. The mean age was 35.87 years; 41.44% were civil servants and 29.73% had no formal education. The mean consultation delay was 50 months. Oligospermia (45%) and azoospermia (32%) were the most frequent sperm abnormalities. A varicocele was detected in 48.65% of patients. The main factors for delay included financial constraints (65.52%), initial consultations with non-specialists (61.25%), and cultural beliefs attributing infertility to women (24.14%). Conclusion: Male infertility in Burkina Faso is associated with significant diagnostic delays influenced by socioeconomic and cultural factors. A multisectoral approach - combining public health, anthropology, and social policies - is essential to improve access to andrological care in resource-limited countries.
},
year = {2025}
}
TY - JOUR
T1 - Male Infertility in Burkina Faso: Epidemiological, Clinical, and Sociocultural Determinants of Delayed Andrological Consultation
AU - Hassami Sawadogo
AU - Clotaire Alexis Marie Kiemdiba Donega Yameogo
AU - Brahima Kirakoya
AU - Abdoul-Karim Pare
AU - Ahmad Almoctar Ilachane
AU - Jean de la Croix Millogo
AU - Adama Ouattara
AU - Fasnewinde Aristide Kabore
Y1 - 2025/10/27
PY - 2025
N1 - https://doi.org/10.11648/j.ijcu.20250902.19
DO - 10.11648/j.ijcu.20250902.19
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 158
EP - 162
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20250902.19
AB - Introduction: Male infertility remains a neglected public health problem in sub-Saharan Africa, characterized by significant diagnostic delays due to sociocultural and economic barriers. This study aims to analyze the epidemiological, clinical, and paraclinical profiles of male infertility and to identify factors contributing to delayed consultation at the Yalgado Ouédraogo University Hospital (CHU-YO). Methods: A descriptive cross-sectional study was conducted from October 2021 to September 2023, including 111 men evaluated for infertility. Data were collected retrospectively from medical records and supplemented by structured interviews. Statistical analyses were performed using EPI Info 7.2. Results: The hospital prevalence of male infertility was 5.39%. The mean age was 35.87 years; 41.44% were civil servants and 29.73% had no formal education. The mean consultation delay was 50 months. Oligospermia (45%) and azoospermia (32%) were the most frequent sperm abnormalities. A varicocele was detected in 48.65% of patients. The main factors for delay included financial constraints (65.52%), initial consultations with non-specialists (61.25%), and cultural beliefs attributing infertility to women (24.14%). Conclusion: Male infertility in Burkina Faso is associated with significant diagnostic delays influenced by socioeconomic and cultural factors. A multisectoral approach - combining public health, anthropology, and social policies - is essential to improve access to andrological care in resource-limited countries.
VL - 9
IS - 2
ER -
Sawadogo, H., Yameogo, C. A. M. K. D., Kirakoya, B., Pare, A., Ilachane, A. A., et al. (2025). Male Infertility in Burkina Faso: Epidemiological, Clinical, and Sociocultural Determinants of Delayed Andrological Consultation. International Journal of Clinical Urology, 9(2), 158-162. https://doi.org/10.11648/j.ijcu.20250902.19
Sawadogo, H.; Yameogo, C. A. M. K. D.; Kirakoya, B.; Pare, A.; Ilachane, A. A., et al. Male Infertility in Burkina Faso: Epidemiological, Clinical, and Sociocultural Determinants of Delayed Andrological Consultation. Int. J. Clin. Urol.2025, 9(2), 158-162. doi: 10.11648/j.ijcu.20250902.19
Sawadogo H, Yameogo CAMKD, Kirakoya B, Pare A, Ilachane AA, et al. Male Infertility in Burkina Faso: Epidemiological, Clinical, and Sociocultural Determinants of Delayed Andrological Consultation. Int J Clin Urol. 2025;9(2):158-162. doi: 10.11648/j.ijcu.20250902.19
@article{10.11648/j.ijcu.20250902.19,
author = {Hassami Sawadogo and Clotaire Alexis Marie Kiemdiba Donega Yameogo and Brahima Kirakoya and Abdoul-Karim Pare and Ahmad Almoctar Ilachane and Jean de la Croix Millogo and Adama Ouattara and Fasnewinde Aristide Kabore},
title = {Male Infertility in Burkina Faso: Epidemiological, Clinical, and Sociocultural Determinants of Delayed Andrological Consultation
},
journal = {International Journal of Clinical Urology},
volume = {9},
number = {2},
pages = {158-162},
doi = {10.11648/j.ijcu.20250902.19},
url = {https://doi.org/10.11648/j.ijcu.20250902.19},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20250902.19},
abstract = {Introduction: Male infertility remains a neglected public health problem in sub-Saharan Africa, characterized by significant diagnostic delays due to sociocultural and economic barriers. This study aims to analyze the epidemiological, clinical, and paraclinical profiles of male infertility and to identify factors contributing to delayed consultation at the Yalgado Ouédraogo University Hospital (CHU-YO). Methods: A descriptive cross-sectional study was conducted from October 2021 to September 2023, including 111 men evaluated for infertility. Data were collected retrospectively from medical records and supplemented by structured interviews. Statistical analyses were performed using EPI Info 7.2. Results: The hospital prevalence of male infertility was 5.39%. The mean age was 35.87 years; 41.44% were civil servants and 29.73% had no formal education. The mean consultation delay was 50 months. Oligospermia (45%) and azoospermia (32%) were the most frequent sperm abnormalities. A varicocele was detected in 48.65% of patients. The main factors for delay included financial constraints (65.52%), initial consultations with non-specialists (61.25%), and cultural beliefs attributing infertility to women (24.14%). Conclusion: Male infertility in Burkina Faso is associated with significant diagnostic delays influenced by socioeconomic and cultural factors. A multisectoral approach - combining public health, anthropology, and social policies - is essential to improve access to andrological care in resource-limited countries.
},
year = {2025}
}
TY - JOUR
T1 - Male Infertility in Burkina Faso: Epidemiological, Clinical, and Sociocultural Determinants of Delayed Andrological Consultation
AU - Hassami Sawadogo
AU - Clotaire Alexis Marie Kiemdiba Donega Yameogo
AU - Brahima Kirakoya
AU - Abdoul-Karim Pare
AU - Ahmad Almoctar Ilachane
AU - Jean de la Croix Millogo
AU - Adama Ouattara
AU - Fasnewinde Aristide Kabore
Y1 - 2025/10/27
PY - 2025
N1 - https://doi.org/10.11648/j.ijcu.20250902.19
DO - 10.11648/j.ijcu.20250902.19
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 158
EP - 162
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20250902.19
AB - Introduction: Male infertility remains a neglected public health problem in sub-Saharan Africa, characterized by significant diagnostic delays due to sociocultural and economic barriers. This study aims to analyze the epidemiological, clinical, and paraclinical profiles of male infertility and to identify factors contributing to delayed consultation at the Yalgado Ouédraogo University Hospital (CHU-YO). Methods: A descriptive cross-sectional study was conducted from October 2021 to September 2023, including 111 men evaluated for infertility. Data were collected retrospectively from medical records and supplemented by structured interviews. Statistical analyses were performed using EPI Info 7.2. Results: The hospital prevalence of male infertility was 5.39%. The mean age was 35.87 years; 41.44% were civil servants and 29.73% had no formal education. The mean consultation delay was 50 months. Oligospermia (45%) and azoospermia (32%) were the most frequent sperm abnormalities. A varicocele was detected in 48.65% of patients. The main factors for delay included financial constraints (65.52%), initial consultations with non-specialists (61.25%), and cultural beliefs attributing infertility to women (24.14%). Conclusion: Male infertility in Burkina Faso is associated with significant diagnostic delays influenced by socioeconomic and cultural factors. A multisectoral approach - combining public health, anthropology, and social policies - is essential to improve access to andrological care in resource-limited countries.
VL - 9
IS - 2
ER -