Introduction: The advent of biologicals and small molecules have changed treatment strategies in ulcerative colitis (UC) as therapies now aim for complete mucosal healing. Real-world data on the outcome of UC patients after first trial of biologics is still lacking and is investigated here. Materials and Methods: UC patients treated with at least one biological at Tampere University Hospital between January 2009 and January 2020 were identified and reviewed from patient records. Results: A total of 192 patients were included. The median follow-up was 3.8 years (range 0-11 years). Seventy-four (40%) of the 185 patients treated with tumour necrosis factor α (TNFα) inhibitors (anti-TNF) and four out of the seven treated with vedolizumab continued treatment after follow-up with no need for treatment enhancement or colectomy. Seventy (36%) of all patients needed at least one consecutive treatment and 58 (30%) required surgery with median time of 1 year (range 0-5 years) from initiation of first biological to colectomy. Of the operated patients 34% had at least two different treatment trials with biologicals or janus kinase inhibitors (JAKs) prior to surgery. There was no significant difference in the persistence of different treatments nor between treatment with infliximab alone or in combination with immunomodulator. When analysing predictive factors for colectomy females and patients treated prior the year 2015 had slightly higher colectomy rates. Conclusion: Two fifth of the patients benefitted from the first trial of biological. However, in third subsequent treatment trials merely postponed colectomy while patients suffered from prolonged symptoms. Means are needed to identify patients benefitting from surgery early on.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
. Medical treatment strategies in UC have evolved within the last few decades due to successfully expanding therapeutic repertoire.
In the 90´s infliximab (IFX), a monoclonal antibody (mAb) against TNFα was approved for the treatment of IBD followed by another anti-TNF adalimumab a decade later
[2]
Guo Y, Lu N, Bai A. Clinical Use and Mechanisms of Infliximab Treatment on Inflammatory Bowel Disease: A Recent Update. Biomed Res Int. 2013; 2013: 1-9.
. Since 2014 third anti-TNF golimumab as well as mAb targeting against α4β7integrin vedolizumab (VDZ) and interleukin (IL)-12 and IL-23 antagonist ustekinumab have been used for the treatment of moderate to severe UC
[3]
Palasik BN, Wang H. Tofacitinib, the First Oral Janus Kinase Inhibitor Approved for Adult Ulcerative Colitis. J Pharm Pract. 2021; 34(6): 913-921.
. Since then, several new IL-23 antagonists and JAKs have hit the market and expanded the treatment options in IBD.
Although there is no cure for UC, present therapies aim for inducing and maintaining clinical and endoscopic remission and improving quality of life
[4]
Turner D, Ricciuto A, Lewis A, et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD. Gastroenterol. 2021; 160(5): 1570-1583.
. However, one-third of patients are either intolerant or non-responsive to treatment and in up to 40% efficacy is lost during long-term follow-up
[5]
Khanna R, Sattin BD, Afif W, et al. a clinician’s guide for therapeutic drug monitoring of infliximab in inflammatory bowel disease. Aliment Pharmacol Ther. 2013; 38: 447-459.
. Wider selection of therapies targeting different inflammatory pathways has led to consecutive treatment trials. Despite of the widespread use of these advanced therapies the impact on chancing natural course of the disease has not been established and the need for surgery in UC has remained unchanged
[6]
Verdon C, Reinglas J, Coulombe J, et al. No Change in Surgical and Hospitalization Trends Despite Higher Exposure to Anti-Tumor Necrosis Factor in Inflammatory Bowel Disease in the Québec Provincial Database From 1996 to 2015. Inflamm Bowel Dis. 2021; 27(5): 655-661.
Atia O, Orlanski-Meyer E, Lujan R, et al. Colectomy Rates did not Decrease in Paediatric- and Adult-Onset Ulcerative Colitis During the Biologics Era: A Nationwide Study From the epi-IIRN. J Crohns Colitis. Published online November 20, 2021.
Burisch J, Katsanos KH, Christodoulou DK, et al. Natural Disease Course of Ulcerative Colitis During the First Five Years of Follow-up in a European Population-based Inception Cohort-An Epi-IBD Study. J Crohns Colitis. Published online 2018: 198-208.
Kin C, Bundorf & MK. As Infliximab Use for Ulcerative Colitis Has Increased, so Has the Rate of Surgical Resection. J Gastrointest Surg. 2017; 21: 1159-1165.
Kayal M, Saha A, Poojary P, et al. Emergent colectomy rates decreased while elective ileal pouch rates were stable over time: a nationwide inpatient sample study.
Murthy sanjay K, Begum J, Benchimol eric, Bernstein charles, Kaplan gilaad, Mccurdy JD. Inflammatory bowel disease Introduction of anti-TNF therapy has not yielded expected declines in hospitalisation and intestinal resection rates in inflammatory bowel diseases: a population-based interrupted time series study. Gut. 2020; 69: 274-282.
. The data of long-term disease evolution after first trial of biological therapy is lacking and investigated here.
2. Materials and Methods
2.1. Patients
All patients treated in Tampere University Hospital for UC between January 2009 and January 2020 were identified from the digital patient records. Patients at the age of 16 years or over with biological treatment initiated for treatment of moderate to severe UC were included. Patients were followed-up from the date of initialization of the first biological at least for the induction and until surgery, death, or the end of observation period. Collected data included demographic (gender, age, smoking, other diseases), clinical (UC extent and duration of the disease), and treatment data (prior treatments, need for thiopurines, need for other biologicals or JAKs, cause for discontinuance of treatment and need for colectomy within follow-up).
2.2. Assesments
The diagnosis of UC was made on basis of patient history, clinical symptoms, endoscopic and histological features. The Montreal´s classification was used to categorize the extent of the disease
[12]
Magro F, Gionchetti P, Eliakim R, et al. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-anal Pouch Disorders. J Crohns Colitis. 2017; 11(6): 649-670.
. The risk for comorbidity was assessed by using the Charlson comorbidity index
[13]
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J Chronic Dis. 1987; 40(5): 373-383.
. The dosing of different treatments used in induction and maintenance therapy followed generally accepted guidelines
[14]
Rawla P, Sunkara T, Raj JP. Role of biologics and biosimilars in inflammatory bowel disease: current trends and future perspectives. J Inflamm Res. Published online 2018: 11-215.
. Because proactive drug monitoring was initiated in 2018 and was mainly performed in non-responder’s drug levels were measured in only subset of patients in this series.
Clinical response was defined as alleviation of symptoms with no need for colectomy or further therapy enhancement with other biologicals or JAKs. Duration of treatment was determined as time from the reported date of initiation of first trial until reported discontinuance, colectomy, or initiation date of next treatment trial. The use of treatment was characterized as a single trial despite of temporary interruptions.
2.3. Statistics
Continuous variables are expressed as median with range and categorical variables are expressed as n with percentage (%). Fisher exact test was used to compare categorical variables when assessing the need colectomy. A p-value of <.05 was considered statistically significant. All statistical analyses were conducted using SPSS 28 (IMB Corp, Armonk, NY).
2.4. Ethical Considerations
Study was evaluated and approved by the regional review board (R20543). Without contact with study subjects no informed consent was required based on the Finnish regulations for registry-based studies.
3. Results
A total of 192 patients were included and the median follow-up was 3.8 years (range 0-11). Baseline characteristics are shown in Table 1. Of all patients 81% were under 45 years of age and 80% without significant comorbidity. Altogether 171 (89%) patients had prior usage of thiopurines with median duration of one year (range 0-17 years) from initiation of thiopurines to exposure to first biological.
Table 1. Baseline characteristics of the 192 patients with ulcerative colitis treated with first biological. Data expressed as absolute and relative frequencies and median (interquartile range).
n/median
% (range)
Follow-up time (yr)
3.8
0–11
Male
106
55
Smoker/ex-smoker/never smoked
20/45/100
10/23/52
Age at the initiation of first biological (yr)
33
17–74
Age distribution at initiation of first biological (yr)
< 30
76
40
30–44
79
41
45–59
25
13
≥60
12
6
Disease duration at initiation of first biological (yr)
2
0–28
Montreal score
E1
6
3
E2
52
27
E3
134
70
First biological initiated before year 2015
36
19
Charlson Comorbidity Index
0
0–5
Concomitant medication
Corticosteroids
145
76
Thiopurines
109
57
Aminosalicylates
86
44
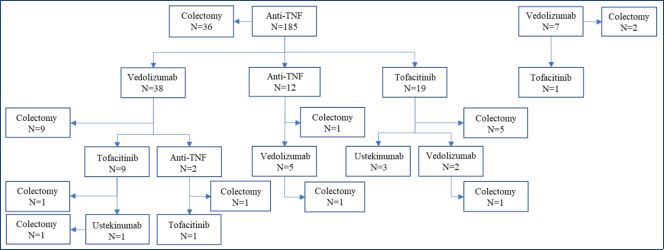
The long-term outcomes of patients is shown in Figure 1. A total of 185 (96%) patients were treated with anti-TNF as primary biological while seven were treated with VDZ. Seventy-four (40%) of the anti-TNF users and four (57%) of the VDZ users continued treatment with first biological with no need for enhancement of treatment or colectomy.
A total of 70 (36%), 21 (11%), and 2 (1%) patients needed one, two, and three subsequent therapy trials with biologicals or JAKs of which 34 (49%), 14 (67%), and 1 (50%) benefitted from treatment, respectively (Figure 1). IFX was the most commonly used and was initiated in 167 (59%) of all 285 trials in this series. At the end of follow-up 121 (63%) of all patients continued using biologicals or JAKs.
Figure 1. Outcome of the 192 patients with ulcerative colitis treated with first trial of biological.
Table 2. Clinical outcome of 192 patients with ulcerative colitis treated with biologicals or JAKs. Data expressed as absolute and relative frequencies and median (interquartile range).
n/median
%/(min-max)
First trial continuing at the end of follow-up
77
40
Thiopurine used in combination
130
68
Treatment persistance (mo)
1st trial
30
0–117
Infliximab (n=163)
26
0–115
Adalimumab (n=11)
30
7–77
Golimumab (n=11)
37
3–81
Vedolizumab (n=7)
30
6–56
2nd trial
18
0–90
Infliximab (n=3)
5
1–7
Adalimumab (n=7)
19
4–68
Golimumab (n=2)
60
31–88
Vedolizumab (n=38)
22
2–67
Tofacitinic (n=20)
16
0–30
3rd trial
17
0–44
Infliximab (n=1)
11
Golimumab (n=1)
38
Vedolizumab (n=7)
26
6–43
Tofacitinic (n=9)
16
0–36
Ustekinumab (n=3)
15
2–20
4th trial
23
11–33
Tofacitinib (n=1)
32
Ustekinumab (n=1)
8
Age at colectomy (yr)
34
21–74
Time from diagnosis to surgery (yr)
3
0–30
Need for surgery from initiation of first biological within
6 months
21
11
12 months
34
18
Long-term follow-up
58
30
As shown in Table 2. there was no significant difference in the duration of first biological. When comparing the 66 patients treated with IFX alone (median time 2.5 years [range 0-10]) and those 97 treated with the combination of IFX and immunomodulator (median time 2.3 years [range 0-9]) there were no significant difference in the duration of treatment.
Inadequate response was the most common reason for discontinuation of treatment in 161 (56%) trials while in 28 (10%) development of antibodies led to discontinuation. In seven trials treatment was discontinued due to severe infections (6 anti-TNF and 1 VDZ). Other causes for discontinuance where patients demand (5 anti-TNF, 1 TOFA), pregnancy (3), hepatotoxicity (2 anti-TNF), rash (1 anti-TNF, 1 VDZ), intolerance or discomfort (2 VDZ), cutaneous lupus (1 anti-TNF), pulmonary reaction (1 anti-TNF), diagnosed malignancy (1 VDZ), and economical reasons (1 anti-TNF). Two patients treated with anti-TNF had anaphylaxis as severe adverse event (SAE).
In 13 patients achieving remission with first trial of anti-TNF treatment was discontinued after pre-planned duration median of 2 years (range 1-4 years). Six of those patients continued treatment after relapse and for one treatment was restarted twice after failing planned discontinuation for the second time. Two of those patients whose had biological re-started needed enhancement of treatment with other biological or JAKs within follow-up.
As shown in Table 2. 58 (30%) patients required surgery within follow-up of whom one had colectomy due to colorectal carcinoma (CRC) and one due to dysplasia. The median time from initiation of first biological to colectomy was 1 year (range 0-5 years), respectively. Twenty (34%) of the operated patients had at least two treatment trials with different biologicals or JAKs (Figure 1). There were five patients receiving IFX as rescue therapy for acute severe UC of whom three had IFX after failing Cyclosporine. Altogether four of those five patients had colectomy and one needed surgery after failing subsequent treatment attempt with VDZ.
Predictive factors for colectomy are presented in Table 3. Extent of the disease, smoking, age at initiation of treatment, used biological, or number of different treatment trials did not predict the need for surgery. Of those patients with first trial initiated before the year 2015 42% needed colectomy when compared to 28% in those treated 2015 or after (p=0.146). A total of 35% of women had surgery when compared to 26% of men (p=0.14). When analysing differences between gender men were more likely to have 3rd and 4th subsequent treatment trials (14% and 2% vs 7% and 0% in women).
Table 3. Predictive factors for colectomy in 192 patients with ulcerative colitis treated with first trial of biological. Data expressed as absolute and relative frequencies.
Colectomy
n/N (%)
p-value
Gender
0.14
Male
28/106 (26)
Female
30/86 (35)
Age distribution at initiation of biologicals
0.617
< 30 years
22/76 (29)
30–44
25/79 (32)
45–59
9/25 (36)
≥ 60
2/12 (17)
Montreal score
0.514
E1
3/6 (50)
E2
15/52 (29)
E3
40/134 (30)
Smoking
0.068
non-smoking
38/145 (26)
smoker
7/20 (35)
Initiation year of 1st biological
0.146
Prior 2015
15/36 (42)
2015 or after
43/156 (28)
First biological
0.912
Infliximab
51/163 (31)
Adalimumab
2/11 (18)
Golimumab
3/11 (27)
Vedolizumab
2/7 (29)
Number of treatment trials
0.658
one
38/122 (31)
two
15/49 (31)
three
4/19 (21)
four
1/2 (50)
Seven of the patients in this series had malignancies of whom four were diagnosed prior to initiation of first biological. Two with CRC and one with glioblastoma were treated with anti-TNF for one to eight years prior to diagnosis of cancer. There was one non-treatment related death reported in this series.
4. Discussion
In this series 41% of patients achieved remission with the first treatment trial of biological with no need for treatment enhancement or colectomy. Half of the patients failing the first biological benefitted of consecutive treatment trials. Despite of the additional treatment attempts third of all patients required surgery within follow-up.
The published data of the impact of biologicals in the natural course of UC is still controversial. Some studies show decreasing colectomy rates while several studies have reported need for surgery remaining unchanged despite of the wide use of anti-TNFs
[6]
Verdon C, Reinglas J, Coulombe J, et al. No Change in Surgical and Hospitalization Trends Despite Higher Exposure to Anti-Tumor Necrosis Factor in Inflammatory Bowel Disease in the Québec Provincial Database From 1996 to 2015. Inflamm Bowel Dis. 2021; 27(5): 655-661.
Kin C, Bundorf & MK. As Infliximab Use for Ulcerative Colitis Has Increased, so Has the Rate of Surgical Resection. J Gastrointest Surg. 2017; 21: 1159-1165.
Murthy sanjay K, Begum J, Benchimol eric, Bernstein charles, Kaplan gilaad, Mccurdy JD. Inflammatory bowel disease Introduction of anti-TNF therapy has not yielded expected declines in hospitalisation and intestinal resection rates in inflammatory bowel diseases: a population-based interrupted time series study. Gut. 2020; 69: 274-282.
Mao EJ, Hazlewood GS, Kaplan GG, Peyrin-Biroulet L, Ananthakrishnan AN. Systematic review with meta-analysis: comparative efficacy of immunosuppressants and biologics for reducing hospitalisation and surgery in Crohn’s disease and ulcerative colitis. Aliment Pharmacol Ther. 2017; 45: 3-13.
. American population-based study reported decline in colectomy rates in UC after wider use of these new therapies while recent study by Atia et al. showed no substantial difference
[7]
Atia O, Orlanski-Meyer E, Lujan R, et al. Colectomy Rates did not Decrease in Paediatric- and Adult-Onset Ulcerative Colitis During the Biologics Era: A Nationwide Study From the epi-IIRN. J Crohns Colitis. Published online November 20, 2021.
Barnes EL, Jiang Y, Kappelman MD, et al. Decreasing Colectomy Rate for Ulcerative Colitis in the United States Between 2007 and 2016: A Time Trend Analysis. Inflamm Bowel Dis. 2020; 26(8).
. So far it seems uncertain whether wide repertoire of therapy options succeed in improving outcomes not to mention the cost effectiveness of these treatments. However, the newcomer upadacitinib has proven to be very effective in the treatment of UC so far
[18]
Lasa, J. S., Olivera, P. A., Danese, S., & Peyrin-Biroulet, L. (2022). Efficacy and safety of biologics and small molecule drugs for patients with moderate-to-severe ulcerative colitis: a systematic review and network meta-analysis. The lancet. Gastroenterology & hepatology, 7(2), 161–170.
Gao, J., Nie, R., Chen, Y., Yang, W., & Ren, Q. (2023). Comparative of the effectiveness and safety of biological agents, small molecule drugs, and microbiome therapies in ulcerative colitis: Systematic review and network meta-analysis. Medicine, 102(43), e35689.
. Also, new options in treatment strategies are evolving as shown by the PROFILE study in patients with Crohn´s disease
[20]
Noor N., Lee J., Bond S. et al. (2024). A biomarker-stratified comparison of top-down versus accelerated step-up treatment strategies for patients with newly diagnosed Crohn´s disease (PROFILE): a multicentre, open-label randomised controlled trial. The Lancet Gastroenterology & hepatology, 9(5): 415-427.
A subset of patients with treatment refractory UC would most likely benefit from colectomy early on instead of subsequent medical therapy trials. However, in effort to avoid surgery some patients are willing to tolerate prolonged symptoms while waiting for response to various treatments. In our series half of the patients benefitted of consecutive therapy trials after failing first biological. Favourable result encourages to continue treatment with additional experiments. However, multiple treatment attempts only postponed surgery in many possibly increasing the risk for postoperative complications
[21]
Randall J, Singh B, Warren BF, Travis SP, Mortensen NJ, George BD. Delayed surgery for acute severe colitis is associated with increased risk of postoperative complications. Br J Surg. 2010; 97(3): 404-409.
. While specific biomarkers are still lacking physician is challenging to find the right therapy for optimized treatment.
In this series two thirds of all treatment trials were discontinued due to lack of response or lose of efficacy. Almost half of those patients who had pre-planned cessation of anti-TNF after deep remission relapsed during follow-up. However, as in prior studies re-treatment was effective in two thirds of those patients
[22]
Molander P, Sipponen T, Kemppainen H, et al. Achievement of deep remission during scheduled maintenance therapy with TNFα-blocking agents in IBD. J Crohns Colitis. 2013; 7(9): 730-735.
. When comparing treatment persistence, we found no difference between therapies. In all trials IFX was the most common used in 60% of the treatment trials. Combination of IFX and thiopurines is recommended to optimize the treatment outcomes and durability of response
[23]
Torres J, Bonovas S, Doherty G, et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Medical Treatment. J Crohns Colitis. 2019; 2020: 4-22.
. In prior studies combining IFX with immunomodulator increased the persistence of treatment while in this series no such difference was seen
[24]
Kobayashi T, Udagawa E, Uda A, Hibi T, Hisamatsu T. Impact of immunomodulator use on treatment persistence in patients with ulcerative colitis: A claims database analysis. J Gastroenterol hepatol. 2019; 35: 225-232.
In our series, patients with biologicals initiated at the age of 60 years or older had lower colectomy rates when compared to younger age groups. Result is probably explained by patient selection and small sample size. Contrary to prior studies, women were more likely to need surgery when compared to men
[25]
Khalil MA, Boutros M, Nedjar H, et al. Incidence Rates and Predictors of Colectomy for Ulcerative Colitis in the Era of Biologics: Results from a Provincial Database. J Gastrointest Surg. 2018; 22: 124-132.
Sceats LA, Morris AM, Bundorf MK, Park KT, Kin C. Sex Differences in Treatment Strategies among Patients with Ulcerative Colitis: A Retrospective Cohort Analysis of Privately Insured Patients. Diss Colon Rectum. 2019; 62: 586-594.
. Result may be explained by difference in treatment strategies while men were more likely to have several subsequent treatment trials when compared to women. In this study 42% of patients with biologicals initiated prior to 2015 had colectomy when compared to 28% of patients introduced to biologicals 2015 or after. Difference was not statistically significant and may be due to longer duration of the disease or change in treatment practises. Clinical studies with long-term surveillance are required to assess the impact of these new therapies in the clinical outcome of UC.
Two patients had anaphylaxis as SAE. Severe infections, hepatotoxicity, and pulmonary reaction were significant adverse effects of which 90% were associated with the use of anti-TNFs. The type and number of adverse events reported were commonly associated with treatment and could be expected
[27]
Haens GD’. Risks and benefits of biologic therapy for inflammatory bowel diseases. Gut. 2007; 56: 725-732.
. Three patients were diagnosed with malignancies (one glioblastoma and two CRC) after treatment with anti-TNF. IBD is known to increase the risk for CRC. However, increased risk for glioblastoma related to anti-TNF has been reported
[28]
Guo M, Luo H, Samii A, Etminan M. The Risk of Glioblastoma with TNF Inhibitors. Pharmacother. 2016; 36(4): 449–454.
This is a single tertiary centres experience of clinical outcome of UC patients after first course of biological therapy. While biologicals are widely used the real-world data of the long-term clinical outcome of UC patients treated with biologicals and JAKs is still lacking. Existing guidelines are based on studies evaluating response to individual medications. However, as the selection of therapies expands patients will use several consecutive treatment trials more often in the future. The limitations of this study are due to the register-based nature and relying on computerized data. In this study response was evaluated based on need for enhancement of treatment or surgery while no biomarkers, clinical or endoscopic evaluation were used. Every fourth of all treatment trials were self-administered and treatment adherence could not be assessed. The effects of dose optimization could not be evaluated because only subset of patients had routine drug level monitoring performed.
5. Conclusion
In conclusion, less than half of the UC patients benefitted of the first trial of biological. However, substantial portion needed consecutive trials with biologicals or JAKs within follow-up. Despite of the wider range of therapeutic molecules colectomy rate remained high and consecutive trials of different therapies merely postponed surgery in many. Educating patients of the possibility for surgery when initiating biologicals is advised.
Heini Huhtala: Data curation, Methodology, Software, Visualization
Tuire Ilus: Supervision
Funding
HE reports receiving personal research grant from Emil Aaltonen foundation, congress, and travel fees from Abbvie, Pfizer, Takeda, and Tillots Pharma. Speakers’ fees from Tillots Pharma, Takeda, Abbvie. Advisory board Lilly. PO reports congress fees from Ferring, Abbvie, Pfizer, and consultant fees from Tillotts and Gilead. AJ has received speaker or consultant fees from Abbvie, Pfizer, and Takeda. HH have nothing to declare. TI advisory Board Janssen, Celltrion, Takeda and speaker´s fee Tillotts, Takeda, Janssen.
Guo Y, Lu N, Bai A. Clinical Use and Mechanisms of Infliximab Treatment on Inflammatory Bowel Disease: A Recent Update. Biomed Res Int. 2013; 2013: 1-9.
Turner D, Ricciuto A, Lewis A, et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD. Gastroenterol. 2021; 160(5): 1570-1583.
Khanna R, Sattin BD, Afif W, et al. a clinician’s guide for therapeutic drug monitoring of infliximab in inflammatory bowel disease. Aliment Pharmacol Ther. 2013; 38: 447-459.
Verdon C, Reinglas J, Coulombe J, et al. No Change in Surgical and Hospitalization Trends Despite Higher Exposure to Anti-Tumor Necrosis Factor in Inflammatory Bowel Disease in the Québec Provincial Database From 1996 to 2015. Inflamm Bowel Dis. 2021; 27(5): 655-661.
Atia O, Orlanski-Meyer E, Lujan R, et al. Colectomy Rates did not Decrease in Paediatric- and Adult-Onset Ulcerative Colitis During the Biologics Era: A Nationwide Study From the epi-IIRN. J Crohns Colitis. Published online November 20, 2021.
Burisch J, Katsanos KH, Christodoulou DK, et al. Natural Disease Course of Ulcerative Colitis During the First Five Years of Follow-up in a European Population-based Inception Cohort-An Epi-IBD Study. J Crohns Colitis. Published online 2018: 198-208.
Kin C, Bundorf & MK. As Infliximab Use for Ulcerative Colitis Has Increased, so Has the Rate of Surgical Resection. J Gastrointest Surg. 2017; 21: 1159-1165.
Kayal M, Saha A, Poojary P, et al. Emergent colectomy rates decreased while elective ileal pouch rates were stable over time: a nationwide inpatient sample study.
Murthy sanjay K, Begum J, Benchimol eric, Bernstein charles, Kaplan gilaad, Mccurdy JD. Inflammatory bowel disease Introduction of anti-TNF therapy has not yielded expected declines in hospitalisation and intestinal resection rates in inflammatory bowel diseases: a population-based interrupted time series study. Gut. 2020; 69: 274-282.
Magro F, Gionchetti P, Eliakim R, et al. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-anal Pouch Disorders. J Crohns Colitis. 2017; 11(6): 649-670.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J Chronic Dis. 1987; 40(5): 373-383.
Rawla P, Sunkara T, Raj JP. Role of biologics and biosimilars in inflammatory bowel disease: current trends and future perspectives. J Inflamm Res. Published online 2018: 11-215.
Mao EJ, Hazlewood GS, Kaplan GG, Peyrin-Biroulet L, Ananthakrishnan AN. Systematic review with meta-analysis: comparative efficacy of immunosuppressants and biologics for reducing hospitalisation and surgery in Crohn’s disease and ulcerative colitis. Aliment Pharmacol Ther. 2017; 45: 3-13.
Barnes EL, Jiang Y, Kappelman MD, et al. Decreasing Colectomy Rate for Ulcerative Colitis in the United States Between 2007 and 2016: A Time Trend Analysis. Inflamm Bowel Dis. 2020; 26(8).
Lasa, J. S., Olivera, P. A., Danese, S., & Peyrin-Biroulet, L. (2022). Efficacy and safety of biologics and small molecule drugs for patients with moderate-to-severe ulcerative colitis: a systematic review and network meta-analysis. The lancet. Gastroenterology & hepatology, 7(2), 161–170.
Gao, J., Nie, R., Chen, Y., Yang, W., & Ren, Q. (2023). Comparative of the effectiveness and safety of biological agents, small molecule drugs, and microbiome therapies in ulcerative colitis: Systematic review and network meta-analysis. Medicine, 102(43), e35689.
Noor N., Lee J., Bond S. et al. (2024). A biomarker-stratified comparison of top-down versus accelerated step-up treatment strategies for patients with newly diagnosed Crohn´s disease (PROFILE): a multicentre, open-label randomised controlled trial. The Lancet Gastroenterology & hepatology, 9(5): 415-427.
Randall J, Singh B, Warren BF, Travis SP, Mortensen NJ, George BD. Delayed surgery for acute severe colitis is associated with increased risk of postoperative complications. Br J Surg. 2010; 97(3): 404-409.
Molander P, Sipponen T, Kemppainen H, et al. Achievement of deep remission during scheduled maintenance therapy with TNFα-blocking agents in IBD. J Crohns Colitis. 2013; 7(9): 730-735.
Kobayashi T, Udagawa E, Uda A, Hibi T, Hisamatsu T. Impact of immunomodulator use on treatment persistence in patients with ulcerative colitis: A claims database analysis. J Gastroenterol hepatol. 2019; 35: 225-232.
Khalil MA, Boutros M, Nedjar H, et al. Incidence Rates and Predictors of Colectomy for Ulcerative Colitis in the Era of Biologics: Results from a Provincial Database. J Gastrointest Surg. 2018; 22: 124-132.
Sceats LA, Morris AM, Bundorf MK, Park KT, Kin C. Sex Differences in Treatment Strategies among Patients with Ulcerative Colitis: A Retrospective Cohort Analysis of Privately Insured Patients. Diss Colon Rectum. 2019; 62: 586-594.
Eronen, H., Oksanen, P., Jussila, A., Huhtala, H., Ilus, T. (2025). The Long-term Outcomes of Patients with Ulcerative Colitis Treated with First Trial of Biological. International Journal of Gastroenterology, 9(1), 1-8. https://doi.org/10.11648/j.ijg.20250901.11
Eronen, H.; Oksanen, P.; Jussila, A.; Huhtala, H.; Ilus, T. The Long-term Outcomes of Patients with Ulcerative Colitis Treated with First Trial of Biological. Int. J. Gastroenterol.2025, 9(1), 1-8. doi: 10.11648/j.ijg.20250901.11
Eronen H, Oksanen P, Jussila A, Huhtala H, Ilus T. The Long-term Outcomes of Patients with Ulcerative Colitis Treated with First Trial of Biological. Int J Gastroenterol. 2025;9(1):1-8. doi: 10.11648/j.ijg.20250901.11
@article{10.11648/j.ijg.20250901.11,
author = {Heli Eronen and Pia Oksanen and Airi Jussila and Heini Huhtala and Tuire Ilus},
title = {The Long-term Outcomes of Patients with Ulcerative Colitis Treated with First Trial of Biological
},
journal = {International Journal of Gastroenterology},
volume = {9},
number = {1},
pages = {1-8},
doi = {10.11648/j.ijg.20250901.11},
url = {https://doi.org/10.11648/j.ijg.20250901.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20250901.11},
abstract = {Introduction: The advent of biologicals and small molecules have changed treatment strategies in ulcerative colitis (UC) as therapies now aim for complete mucosal healing. Real-world data on the outcome of UC patients after first trial of biologics is still lacking and is investigated here. Materials and Methods: UC patients treated with at least one biological at Tampere University Hospital between January 2009 and January 2020 were identified and reviewed from patient records. Results: A total of 192 patients were included. The median follow-up was 3.8 years (range 0-11 years). Seventy-four (40%) of the 185 patients treated with tumour necrosis factor α (TNFα) inhibitors (anti-TNF) and four out of the seven treated with vedolizumab continued treatment after follow-up with no need for treatment enhancement or colectomy. Seventy (36%) of all patients needed at least one consecutive treatment and 58 (30%) required surgery with median time of 1 year (range 0-5 years) from initiation of first biological to colectomy. Of the operated patients 34% had at least two different treatment trials with biologicals or janus kinase inhibitors (JAKs) prior to surgery. There was no significant difference in the persistence of different treatments nor between treatment with infliximab alone or in combination with immunomodulator. When analysing predictive factors for colectomy females and patients treated prior the year 2015 had slightly higher colectomy rates. Conclusion: Two fifth of the patients benefitted from the first trial of biological. However, in third subsequent treatment trials merely postponed colectomy while patients suffered from prolonged symptoms. Means are needed to identify patients benefitting from surgery early on.
},
year = {2025}
}
TY - JOUR
T1 - The Long-term Outcomes of Patients with Ulcerative Colitis Treated with First Trial of Biological
AU - Heli Eronen
AU - Pia Oksanen
AU - Airi Jussila
AU - Heini Huhtala
AU - Tuire Ilus
Y1 - 2025/01/07
PY - 2025
N1 - https://doi.org/10.11648/j.ijg.20250901.11
DO - 10.11648/j.ijg.20250901.11
T2 - International Journal of Gastroenterology
JF - International Journal of Gastroenterology
JO - International Journal of Gastroenterology
SP - 1
EP - 8
PB - Science Publishing Group
SN - 2640-169X
UR - https://doi.org/10.11648/j.ijg.20250901.11
AB - Introduction: The advent of biologicals and small molecules have changed treatment strategies in ulcerative colitis (UC) as therapies now aim for complete mucosal healing. Real-world data on the outcome of UC patients after first trial of biologics is still lacking and is investigated here. Materials and Methods: UC patients treated with at least one biological at Tampere University Hospital between January 2009 and January 2020 were identified and reviewed from patient records. Results: A total of 192 patients were included. The median follow-up was 3.8 years (range 0-11 years). Seventy-four (40%) of the 185 patients treated with tumour necrosis factor α (TNFα) inhibitors (anti-TNF) and four out of the seven treated with vedolizumab continued treatment after follow-up with no need for treatment enhancement or colectomy. Seventy (36%) of all patients needed at least one consecutive treatment and 58 (30%) required surgery with median time of 1 year (range 0-5 years) from initiation of first biological to colectomy. Of the operated patients 34% had at least two different treatment trials with biologicals or janus kinase inhibitors (JAKs) prior to surgery. There was no significant difference in the persistence of different treatments nor between treatment with infliximab alone or in combination with immunomodulator. When analysing predictive factors for colectomy females and patients treated prior the year 2015 had slightly higher colectomy rates. Conclusion: Two fifth of the patients benefitted from the first trial of biological. However, in third subsequent treatment trials merely postponed colectomy while patients suffered from prolonged symptoms. Means are needed to identify patients benefitting from surgery early on.
VL - 9
IS - 1
ER -
Department of Gastroenterology, Kanta-Häme Central Hospital, Hämeenlinna, Finland; Faculty of Medicine and Health Technology, Tampere University, Tampere, Finland
Faculty of Medicine and Health Technology, Tampere University, Tampere, Finland; Department of Gastroenterology and Alimentary Tract Surgery, Tampere University Hospital, Tampere, Finland
Eronen, H., Oksanen, P., Jussila, A., Huhtala, H., Ilus, T. (2025). The Long-term Outcomes of Patients with Ulcerative Colitis Treated with First Trial of Biological. International Journal of Gastroenterology, 9(1), 1-8. https://doi.org/10.11648/j.ijg.20250901.11
Eronen, H.; Oksanen, P.; Jussila, A.; Huhtala, H.; Ilus, T. The Long-term Outcomes of Patients with Ulcerative Colitis Treated with First Trial of Biological. Int. J. Gastroenterol.2025, 9(1), 1-8. doi: 10.11648/j.ijg.20250901.11
Eronen H, Oksanen P, Jussila A, Huhtala H, Ilus T. The Long-term Outcomes of Patients with Ulcerative Colitis Treated with First Trial of Biological. Int J Gastroenterol. 2025;9(1):1-8. doi: 10.11648/j.ijg.20250901.11
@article{10.11648/j.ijg.20250901.11,
author = {Heli Eronen and Pia Oksanen and Airi Jussila and Heini Huhtala and Tuire Ilus},
title = {The Long-term Outcomes of Patients with Ulcerative Colitis Treated with First Trial of Biological
},
journal = {International Journal of Gastroenterology},
volume = {9},
number = {1},
pages = {1-8},
doi = {10.11648/j.ijg.20250901.11},
url = {https://doi.org/10.11648/j.ijg.20250901.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20250901.11},
abstract = {Introduction: The advent of biologicals and small molecules have changed treatment strategies in ulcerative colitis (UC) as therapies now aim for complete mucosal healing. Real-world data on the outcome of UC patients after first trial of biologics is still lacking and is investigated here. Materials and Methods: UC patients treated with at least one biological at Tampere University Hospital between January 2009 and January 2020 were identified and reviewed from patient records. Results: A total of 192 patients were included. The median follow-up was 3.8 years (range 0-11 years). Seventy-four (40%) of the 185 patients treated with tumour necrosis factor α (TNFα) inhibitors (anti-TNF) and four out of the seven treated with vedolizumab continued treatment after follow-up with no need for treatment enhancement or colectomy. Seventy (36%) of all patients needed at least one consecutive treatment and 58 (30%) required surgery with median time of 1 year (range 0-5 years) from initiation of first biological to colectomy. Of the operated patients 34% had at least two different treatment trials with biologicals or janus kinase inhibitors (JAKs) prior to surgery. There was no significant difference in the persistence of different treatments nor between treatment with infliximab alone or in combination with immunomodulator. When analysing predictive factors for colectomy females and patients treated prior the year 2015 had slightly higher colectomy rates. Conclusion: Two fifth of the patients benefitted from the first trial of biological. However, in third subsequent treatment trials merely postponed colectomy while patients suffered from prolonged symptoms. Means are needed to identify patients benefitting from surgery early on.
},
year = {2025}
}
TY - JOUR
T1 - The Long-term Outcomes of Patients with Ulcerative Colitis Treated with First Trial of Biological
AU - Heli Eronen
AU - Pia Oksanen
AU - Airi Jussila
AU - Heini Huhtala
AU - Tuire Ilus
Y1 - 2025/01/07
PY - 2025
N1 - https://doi.org/10.11648/j.ijg.20250901.11
DO - 10.11648/j.ijg.20250901.11
T2 - International Journal of Gastroenterology
JF - International Journal of Gastroenterology
JO - International Journal of Gastroenterology
SP - 1
EP - 8
PB - Science Publishing Group
SN - 2640-169X
UR - https://doi.org/10.11648/j.ijg.20250901.11
AB - Introduction: The advent of biologicals and small molecules have changed treatment strategies in ulcerative colitis (UC) as therapies now aim for complete mucosal healing. Real-world data on the outcome of UC patients after first trial of biologics is still lacking and is investigated here. Materials and Methods: UC patients treated with at least one biological at Tampere University Hospital between January 2009 and January 2020 were identified and reviewed from patient records. Results: A total of 192 patients were included. The median follow-up was 3.8 years (range 0-11 years). Seventy-four (40%) of the 185 patients treated with tumour necrosis factor α (TNFα) inhibitors (anti-TNF) and four out of the seven treated with vedolizumab continued treatment after follow-up with no need for treatment enhancement or colectomy. Seventy (36%) of all patients needed at least one consecutive treatment and 58 (30%) required surgery with median time of 1 year (range 0-5 years) from initiation of first biological to colectomy. Of the operated patients 34% had at least two different treatment trials with biologicals or janus kinase inhibitors (JAKs) prior to surgery. There was no significant difference in the persistence of different treatments nor between treatment with infliximab alone or in combination with immunomodulator. When analysing predictive factors for colectomy females and patients treated prior the year 2015 had slightly higher colectomy rates. Conclusion: Two fifth of the patients benefitted from the first trial of biological. However, in third subsequent treatment trials merely postponed colectomy while patients suffered from prolonged symptoms. Means are needed to identify patients benefitting from surgery early on.
VL - 9
IS - 1
ER -