Abstract
Spontaneous bacterial peritonitis (SBP) is a severe complication of decompensated cirrhosis, associated with high mortality and poor prognosis. This study aimed to evaluate the efficacy of a combined therapeutic approach-peritoneal catheter lavage, intraperitoneal antibiotic injection, and oral rifaximin-on top of standard intravenous antibiotics for SBP in cirrhotic patients. A total of 90 cirrhotic patients with SBP were randomly assigned to either the treatment group (n=45) or the control group (n=45). Both groups received basic care including hepatoprotective therapy, albumin supplementation, and electrolyte correction. The control group was treated with intravenous ceftriaxone (2 g/day for 14 days), while the treatment group was added peritoneal lavage (daily cycles of draining ascites, infusing warm saline, and injecting intraperitoneal ceftriaxone) plus oral rifaximin (200 mg three times daily) to the same intravenous regimen. Baseline characteristics, including demographic data, cirrhosis severity (Child-Pugh grade), and comorbidities, were comparable between the two groups (all P>0.05). After 14 days of treatment, the treatment group showed significantly greater improvements in clinical symptoms (fever, abdominal pain, tenderness) and laboratory markers: liver function parameters (ALT, AST, TBil) decreased more markedly, and inflammatory indicators (WBC, CRP, PCT) were reduced to a larger extent compared to the control group (all P<0.05). Notably, the ascitic fluid polymorphonuclear leukocyte count, a key marker of SBP resolution, dropped from 1200±350×106/L to 150±50×106/L in the treatment group, versus 1180±320×106/L to 450±120×106/L in the control group (P<0.001). The total effective rate was significantly higher in the treatment group (88.9%) than in the control group (62.3%, P<0.01). These findings suggest that combining peritoneal lavage, intraperitoneal antibiotics, and oral rifaximin with standard intravenous therapy enhances SBP control, improves liver function, and reduces systemic inflammation in cirrhotic patients, thereby offering a more effective strategy for managing this life-threatening complication.
|
Published in
|
International Journal of Gastroenterology (Volume 9, Issue 2)
|
|
DOI
|
10.11648/j.ijg.20250902.13
|
|
Page(s)
|
103-110 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Spontaneous Bacterial Peritonitis, Liver Cirrhosis, Peritoneal Lavage, Rifaximin, Intraperitoneal Antibiotics, Refractory Ascites
1. Introduction
Ascites is a sign of decompensation in patients with cirrhosis, indicating a further deterioration of liver disease and a poorer prognosis
| [1] | Gordon FD: Ascites. Clinics in liver disease 2012, 16(2): 285-299. |
[1]
. Its pathogenesis in cirrhosis is primarily driven by portal hypertension and systemic vasodilation. Portal hypertension leads to splanchnic arterial vasodilation, reducing effective arterial blood volume. This activates neurohumoral systems (renin-angiotensin-aldosterone system, sympathetic nervous system, vasopressin), resulting in sodium and water retention. Concurrently, increased hepatic sinusoidal pressure and hypoalbuminemia promote fluid transudation into the peritoneal cavity. In these patients, ascites not only increases the mortality rate but can also lead to other serious complications, such as spontaneous bacterial peritonitis and hepatorenal syndrome
| [2] | Garcia-Tsao G: Current Management of the Complications of Cirrhosis and Portal Hypertension: Variceal Hemorrhage, Ascites, and Spontaneous Bacterial Peritonitis. Digestive diseases (Basel, Switzerland) 2016, 34(4): 382-386. |
[2]
. Research papers indicate that the presence of ascites is closely linked to systemic inflammation and various complications, which collectively contribute to an increased mortality rate
| [3] | Tonon M, Piano S, Gambino CG, Romano A, Pilutti C, Incicco S, Brocca A, Sticca A, Bolognesi M, Angeli P: Outcomes and Mortality of Grade 1 Ascites and Recurrent Ascites in Patients with Cirrhosis. Clinical gastroenterology and hepatology: the official clinical practice journal of the American Gastroenterological Association 2021, 19(2): 358-366. e358. |
[3]
. Traditionally, the management of ascites has relied on diuretics and sodium restriction. However, in some cases, ascites may develop resistance to these treatments, leading to refractory ascites, which further complicates the patient's condition
| [4] | Adebayo D, Neong SF, Wong F: Refractory Ascites in Liver Cirrhosis. The American journal of gastroenterology 2019, 114(1): 40-47. |
[4]
. Managing refractory ascites may require more invasive treatments, such as transjugular intrahepatic portosystemic shunt (TIPS), to reduce portal hypertension and improve ascites control
| [5] | Iannone G, Pompili E, De Venuto C, Pratelli D, Tedesco G, Baldassarre M, Caraceni P, Zaccherini G: The Role of Transjugular Intrahepatic Portosystemic Shunt for the Management of Ascites in Patients with Decompensated Cirrhosis. Journal of clinical medicine 2024, 13(5). |
[5]
.
Moreover, the presence of ascites is associated with a decline in the quality of life for patients with liver cirrhosis, particularly in cases of refractory ascites, where patients may require frequent paracentesis to alleviate symptoms
| [6] | Kozaki K, M II, Takagi T, Fukuda T, Sanpei T, Terunuma Y, Yatabe Y, Akano K: Cell-Free and Concentrated Ascites Reinfusion Therapy for Decompensated Liver Cirrhosis. Therapeutic apheresis and dialysis: official peer-reviewed journal of the International Society for Apheresis, the Japanese Society for Apheresis, the Japanese Society for Dialysis Therapy 2016, 20(4): 376-382. |
[6]
. Therefore, effectively managing ascites is crucial not only to extend the patients' survival but also to improve their quality of life. In summary, the development of ascites is a significant indicator of decompensation in liver cirrhosis, indicating the need for more proactive treatment and management strategies.
Spontaneous bacterial peritonitis (SBP) is a common and serious complication in patients with liver cirrhosis. Its clinical manifestations are often non-specific, making early diagnosis crucial for improving the prognosis. The prevalence of SBP among cirrhotic patients with ascites ranges from 3% to 10%, and it is associated with a high mortality rate, estimated between 30% and 50%
| [7] | Sapey T, Mena E, Fort E, Laurin C, Kabissa D, Runyon BA, Mendler MH: Rapid diagnosis of spontaneous bacterial peritonitis with leukocyte esterase reagent strips in a European and in an American center. Journal of gastroenterology and hepatology 2005, 20(2): 187-192. |
[7]
. The exact mechanism of SBP is not fully understood, but it is generally believed to be closely linked to the congestion and edema of the intestinal wall and the dysfunction of the mucosal barrier caused by portal hypertension. The congestion and edema of the intestinal wall due to portal hypertension can lead to the destruction of the intestinal mucosal barrier, thereby increasing the risk of bacterial translocation and potentially leading to SBP. This perspective has been further supported and expanded in research.
First, portal hypertension is common in patients with liver cirrhosis and is a significant cause of SBP. Studies show that portal hypertension caused by liver cirrhosis can lead to visceral vasodilation and systemic hypotension, resulting in inadequate renal perfusion and renal insufficiency. This pathological process is particularly evident in hepatorenal syndrome (HRS)
| [8] | Liu PMF, de Carvalho ST, Fradico PF, Cazumbá MLB, Campos RGB, Simões ESAC: Hepatorenal syndrome in children: a review. Pediatric nephrology (Berlin, Germany) 2021, 36(8): 2203-2215. |
[8]
. The development of HRS is closely linked to SBP, as SBP often serves as one of the triggers for HRS
| [9] | Song Y, Yang X, Yu C: Understanding and Treating Hepatorenal Syndrome: Insights from Recent Research. Seminars in liver disease 2025. |
[9]
. Therefore, understanding the relationship between portal hypertension and intestinal wall congestion and edema is crucial for elucidating the pathogenesis of SBP.
Moreover, the integrity of the intestinal mucosal barrier plays a crucial role in preventing SBP. Research indicates that by enhancing the permeability of the intestinal epithelium and suppressing inflammatory responses, it is possible to effectively reduce intestinal damage and maintain the function of the mucosal barrier
| [10] | Rao K, Qin S, Yang Y, Zhan K, Wu H, Zheng H, Huang S: Shenling Baizhu Powder Alleviates TNBS-Induced Colitis in Rats by Improving Intestinal Epithelial Permeability and Inhibiting Inflammation Through the TLR5/MyD88/NF-κB Pathway. Frontiers in pharmacology 2022, 13: 883918. |
[10]
. For instance, Shenling Baizhu Powder (SBP) has shown potential in experimental colitis models to improve gut health by strengthening the epithelial barrier and reducing inflammation. This finding suggests that similar mechanisms may have therapeutic value in the prevention and treatment of SBP.
According to the 2023 edition of the guidelines for the diagnosis and treatment of ascites in liver cirrhosis
| [11] | Singh V, De A, Mehtani R, Angeli P, Maiwall R, Satapathy S, Singal AK, Saraya A, Sharma BC, Eapen CE et al: Asia-Pacific association for study of liver guidelines on management of ascites in liver disease. Hepatology international 2023, 17(4): 792-826. |
[11]
, early diagnosis primarily relies on the following aspects: first, symptoms or signs, including those of acute peritonitis such as abdominal pain and tenderness. Although these symptoms are common, they are not specific, so they need to be combined with other diagnostic methods for a comprehensive assessment. Secondly, laboratory tests are also a crucial basis for early diagnosis. Typically, the analysis of ascitic fluid is a key step in diagnosing SBP. An increase in polymorphonuclear leukocyte count in the ascites fluid is an important indicator of SBP. Moreover, although bacterial culture has lower sensitivity, it remains a necessary method to identify the pathogen. When managing community-acquired SBP, guidelines typically recommend third-generation cephalosporins, such as cefotaxime or ceftriaxone. These drugs have good coverage for Gram-negative enterobacteria, typically covering 95% of such infections
| [12] | Hsieh CC, Lee CH, Li MC, Hong MY, Chi CH, Lee CC: Empirical third-generation cephalosporin therapy for adults with community-onset Enterobacteriaceae bacteraemia: Impact of revised CLSI breakpoints. International journal of antimicrobial agents 2016, 47(4): 297-303. |
[12]
. However, with the rise in antibiotic resistance, particularly in hospital-acquired infections, the effectiveness of third-generation cephalosporins may be limited. In such cases, carbapenems are considered a more effective option, as they remain active against multidrug-resistant strains
| [13] | Rahal JJ: The role of carbapenems in initial therapy for serious Gram-negative infections. Critical care (London, England) 2008, 12 Suppl 4(Suppl 4): S5. |
[13]
. Research indicates that the resistance rate of third-generation cephalosporins in hospital-acquired sepsis is significantly higher than in community-acquired infections. This difference in resistance may be due to the more widespread spread of multidrug-resistant strains in hospitals
| [14] | Fiore M, Gentile I, Maraolo AE, Leone S, Simeon V, Chiodini P, Pace MC, Gustot T, Taccone FS: Are third-generation cephalosporins still the empirical antibiotic treatment of community-acquired spontaneous bacterial peritonitis? A systematic review and meta-analysis. European journal of gastroenterology & hepatology 2018, 30(3): 329-336. |
[14]
. Therefore, empirical antimicrobial therapy for hospital-acquired Sepsis typically recommends the use of carbapenems to ensure effective coverage of potential resistant pathogens. Furthermore, the selection of antimicrobial drugs should not only consider the drug's coverage but also take into account local resistance patterns and the patient's specific condition. For patients at high risk of severe infection or with compromised immune systems, choosing broad-spectrum antibiotics like carbapenems might be a safer strategy to prevent treatment failure and improve patient survival rates
| [13] | Rahal JJ: The role of carbapenems in initial therapy for serious Gram-negative infections. Critical care (London, England) 2008, 12 Suppl 4(Suppl 4): S5. |
[13]
. Rifaximin can effectively inhibit the growth of intestinal bacteria in a broad spectrum and potently, has bactericidal/antibacterial, immunomodulatory and anti-inflammatory activities, and has a good effect on the prevention and treatment of SBP and refractory ascites in liver cirrhosis
| [15] | Praharaj DL, Premkumar M, Roy A, Verma N, Taneja S, Duseja A, Dhiman RK: Rifaximin Vs. Norfloxacin for Spontaneous Bacterial Peritonitis Prophylaxis: A Randomized Controlled Trial. Journal of clinical and experimental hepatology 2022, 12(2): 336-342. |
[15]
. However, in clinical practice, intravenous antibiotics are usually used to control SBP, but in some patients, this method is not effective in controlling the disease.
The purpose of this study was to investigate the efficacy of intraperitoneal catheter lavage combined with intraperitoneal injection of sensitive antibiotics on the basis of intravenous antibiotics, albumin transfusion with or without teripressin or rifaximin on SBP in liver cirrhosis.
2. Material and Methods
2.1. Patients
A total of 90 cirrhotic patients with SBP were admitted to our hospital from June 2024 to June 2025 and randomly assigned to either the treatment group (n=45) or the control group (n=45). Both groups received basic care including hepatoprotective therapy, albumin supplementation, and electrolyte correction. The control group was treated with intravenous ceftriaxone (2 g/day for 14 days), while the treatment group received peritoneal catheter lavage (daily cycles of draining ascites, infusing warm saline, and intraperitoneal ceftriaxone injection) plus oral rifaximin (200 mg three times daily) in addition to intravenous ceftriaxone.
Diagnostic criteria for SBP: (1) The number of neutrophils in ascites > 250×106/L; (2) The number of neutrophils in ascites < 250×106/L, but the ascites culture was positive; (3) The patient had different degrees of clinical manifestations such as fever, abdominal pain, and abdominal distension, as well as abdominal tenderness, rebound tenderness and other signs. SBP is diagnosed if either (3) and (1) (2) are met. Exclusion criteria: (1) Patients with abdominal infection caused by rupture of abdominal organs were excluded; (2) Patients with cholecystitis, pancreatitis and other intra-abdominal infections; (3) Patients with malignant tumors; (4) Those who cannot cooperate with the treatment. The clinical study protocol was approved by the Human Research Ethics Committee of Shaoyang Central Hospital (ethics approval number KY-2025-06) and conducted in accordance with the principles of the Declaration of Helsinki. All participants provided written informed consent prior to inclusion.
2.2. Treatment
Patients in both groups of basic treatment were given hepatoprotection, diuretic, albumin and fresh plasma supplementation, correction of electrolyte disorders, and anticoma, antipyretic, antidiarrheal and other treatments if necessary.
The control group was treated with empirical anti-infective therapy with the third generation of head holders, and the specific medication was 0.9% sodium chloride injection 100 mL ceftriaxone for injection 2 g intravenous infusion, once a day, for 14 days. If ascetic fluid cultures or blood cultures are positive, susceptible antibiotics can be adjusted based on susceptibility results. On the basis of the control group, the treatment group was given peritoneal catheter lavage combined with intraperitoneal injection of antibiotic treatment, specific methods: (1) Peritoneal catheterization: the patient was placed in a supine position, routine disinfection, after the successful local anesthesia of 2% lidocaine, the reverse McCedar point was taken as the puncture point, the puncture needle was used to insert the needle, the ascites fluid was withdrawn, the guidewire was inserted along the puncture needle, after the guidewire entered, the puncture needle was withdrawn, the skin and subcutaneous tissue were dilated with the dilation sheath, and the 8F drainage tube was inserted along the guidewire, and the guidewire was pulled out and the drainage tube was fixed. (2) Lavage combined with intraperitoneal injection of antibiotics: first drain out 1000 mL of ascites, infuse 1000 mL of warm normal saline into the peritoneal cavity, and then drain 1000 mL of ascites, and after the color of the ascites was obviously clear, intraperitoneal injection of 20 mL of normal saline and 2 g of ceftriaxone for injection once a day for 14 days. If ascites or blood cultures were positive, susceptible antibiotics can be adjusted based on susceptibility results. (3) On the basis of the above treatment, oral rifaximin 800 mg is administered in three divided doses.
2.3. Observation Indicators and Evaluation Criteria
To observe the changes in (1) symptoms and signs such as fever, abdominal pain, abdominal distension, abdominal tenderness, and rebound tenderness after treatment in the two groups; (2) The liver function indexes of the two groups before and after treatment were recorded: alanine aminotransferase (ALT), aspartate aminotransferase (AST), and total bilirubin (TBil); (3) The inflammatory indexes of the two groups before and after treatment: white blood cell count (WBC), procalcitonin (PCT), and C-reactive protein (CRP) were recorded.
The evaluation criteria were: (1) Efficacy: clinical symptoms and signs basically disappeared, B ultrasound showed a small amount of ascites or no ascites, the total number of white blood cells in ascites < 250×106/L, and the ascetic fluid culture was negative. (2) Effective: the clinical symptoms and signs were significantly alleviated, and the B-ultrasound showed that the ascites volume was reduced by >50%, the total number of white blood cells in the ascites < 250×106/L, and the ascetic fluid culture was negative. (3) Ineffective: no improvement or aggravation of clinical symptoms and signs, no decrease or increase in ascites amount, total number of white blood cells in ascites > 500×106/L, and positive ascetic fluid culture. Total effective rate of treatment = (number of effective cases/ total number of cases) × 100%
2.4. Statistical Analysis
R software was used to statistically analyze the data, and the continuous data were expressed as mean standard deviation (x±s), the paired t-test was used for the difference between the data before and after treatment, and the t-test was used for the comparison of the difference between the two groups before and after treatment. The counting data were described as percentages (%), chi-square test, and P<0.05 is statistically significant.
3. Results
3.1. Baseline Characteristics
As shown in
Table 1, there were no statistically significant differences in demographic characteristics, cirrhosis-related indicators, etiology of cirrhosis, or comorbidities between the experimental group (n=45) and the control group (n=45) at baseline (all P>0.05). Specifically, variables such as age, gender distribution, duration of cirrhosis, Child-Pugh grade, albumin levels, total bilirubin, prothrombin time, and the prevalence of comorbidities (e.g., diabetes, hypertension, renal insufficiency) were comparable between the two groups. This indicated that the two groups were well-balanced and suitable for subsequent comparative analysis.
Table 1. Baseline Characteristics of Cirrhosis Patients with SBP.
| Experimental Group (n=45) | Control Group (n=45) | P-value |
Demographic Characteristics |
Gender (Male) | 28 (62.2%) | 26 (57.8%) | 0.67 |
Age (years) | 52.4 ± 7.8 | 50.9 ± 8.2 | 0.36 |
Liver Cirrhosis Related Indicators |
Duration of cirrhosis (years) | 6.8 ± 2.4 | 6.3 ± 2.1 | 0.28 |
Child-Pugh class | | | 0.82 |
Class A | 7 (15.6%) | 6 (13.3%) | |
Class B | 22 (48.9%) | 24 (53.3%) | |
Class C | 16 (35.6%) | 15 (33.3%) | |
Hepatic encephalopathy (Present) | 12 (26.7%) | 11 (24.4%) | 0.80 |
Albumin (g/L) | 30.2 ± 4.1 | 29.8 ± 4.3 | 0.62 |
Total bilirubin (μmol/L) | 46.5 ± 12.3 | 48.1 ± 13.2 | 0.53 |
Prolonged PT (>16 s) | 28 (62.2%) | 30 (66.7%) | 0.66 |
Etiology of Liver Cirrhosis |
Viral hepatitis | 29 (64.4%) | 27 (60.0%) | 0.85 |
Alcoholic | 10 (22.2%) | 11 (24.4%) |
Other (autoimmune/cryptogenic) | 6 (13.3%) | 7 (15.6%) |
Comorbidities |
Diabetes | 16 (35.6%) | 14 (31.1%) | 0.65 |
Hypertension | 20 (44.4%) | 18 (40.0%) | 0.67 |
Coronary heart disease | 9 (20.0%) | 8 (17.8%) | 0.79 |
Renal insufficiency (eGFR<60) | 11 (24.4%) | 10 (22.2%) | 0.81 |
SBP: Spontaneous Bacterial Peritonitis; PT: Prothrombin Time; eGFR: estimated Glomerular Filtration Rate
3.2. Improvement in Clinical Symptoms and Signs
After 14 days of treatment, both groups showed improvements in clinical symptoms and signs, including reduction in fever, abdominal pain, abdominal distension, abdominal tenderness, and rebound tenderness. However, the improvement was more rapid and pronounced in the treatment group. For instance, fever resolution occurred earlier (median 3.2 ± 1.1 days vs. 5.6 ± 1.5 days, P<0.01) and abdominal tenderness/rebound tenderness alleviated more completely in the treatment group compared to the control group (P<0.05 for both).
3.3. Changes in Liver Function Parameters
As depicted in the
Figure 1, liver function parameters (ALT, AST, and TBil) improved in both groups after treatment, but the treatment group exhibited more significant improvements.
Alanine Aminotransferase (ALT): At baseline, there was no significant difference in ALT levels between the two groups (P>0.05). After treatment, ALT decreased from 85.6 ± 18.3 IU/L to 42.3 ± 10.5 IU/L in the treatment group, while in the control group, it decreased from 83.9 ± 17.6 IU/L to 61.5 ± 12.8 IU/L. The reduction in the treatment group was significantly greater (P<0.01).
Aspartate Aminotransferase (AST): Similar trends were observed for AST. Baseline AST levels were comparable (P>0.05). Post-treatment, AST declined from 92.4 ± 21.5 IU/L to 45.6 ± 11.2 IU/L in the treatment group, versus a decline from 90.8 ± 20.3 IU/L to 65.3 ± 13.7 IU/L in the control group (P<0.01).
Total Bilirubin (TBil): TBil levels in the treatment group decreased from 46.5 ± 12.3 μmol/L to 28.2 ± 8.6 μmol/L, whereas in the control group, they decreased from 48.1 ± 13.2 μmol/L to 38.7 ± 10.1 μmol/L. The treatment group showed a more significant reduction (P<0.05).
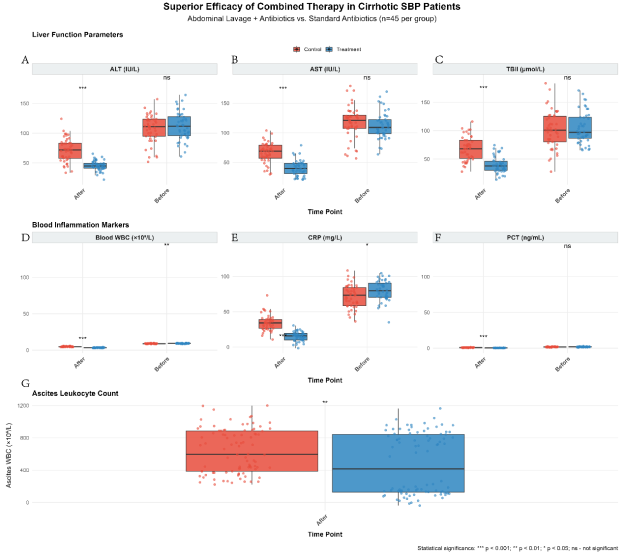
Figure 1. Changes in liver function and inflammatory markers before and after treatment in both groups.
The figure displays the dynamic changes in key liver function parameters and systemic inflammatory markers in patients with cirrhosis complicated by spontaneous bacterial peritonitis (SBP) before and after 14 days of treatment. A: Comparison of alanine aminotransferase (ALT) levels before and after treatment. The treatment group (peritoneal catheter lavage + intraperitoneal antibiotics + oral rifaximin + standard therapy) showed a more significant reduction in ALT compared to the control group (standard therapy with third-generation cephalosporins alone). B: Changes in aspartate aminotransferase (AST) levels. Similar to ALT, the treatment group exhibited a greater decrease in AST post-treatment, indicating improved hepatic parenchymal injury. C: Total bilirubin (TBil) levels before and after intervention. The treatment group demonstrated a more pronounced decline in TBil, reflecting better improvement in liver synthetic function and cholestasis. D: White blood cell (WBC) count changes, showing a more substantial reduction in systemic leukocytosis in the treatment group, consistent with effective control of infection. E: C-reactive protein (CRP) levels, with a marked decrease in the treatment group, indicating a stronger suppression of systemic inflammatory responses. F: Procalcitonin (PCT) levels, where the treatment group achieved a more significant reduction, further confirming superior control of bacterial infection. G: Ascites leukocyte count changes, showing a more substantial reduction in systemic leukocytosis in the treatment group, consistent with effective control of infection. ALT = alanine aminotransferase; AST = aspartate aminotransferase; TBil = total bilirubin; WBC = white blood cell; CRP = C-reactive protein; PCT = procalcitonin.
3.4. Changes in Inflammatory Markers
Marked improvements in systemic inflammatory markers were observed in both groups, with the treatment group demonstrated superior outcomes (
Figure 1):
White Blood Cell (WBC) Count: Baseline WBC counts were similar between groups (P>0.05). After treatment, the treatment group’s WBC count decreased from 12.6 ± 3.2 × 109/L to 6.2 ± 1.5 × 109/L, while the control group’s count decreased from 12.3 ± 3.0 × 109/L to 8.5 ± 2.1 × 109/L (P<0.05).
C-Reactive Protein (CRP): CRP levels showed the most pronounced difference. In the treatment group, CRP decreased from 85.3 ± 18.6 mg/L to 15.2 ± 5.3 mg/L, compared to a reduction from 83.7 ± 17.9 mg/L to 35.6 ± 9.8 mg/L in the control group (***P<0.001).
Procalcitonin (PCT): PCT levels in the treatment group declined from 2.8 ± 0.7 ng/mL to 0.3 ± 0.1 ng/mL, while the control group’s PCT decreased from 2.7 ± 0.6 ng/mL to 0.8 ± 0.2 ng/mL, with a statistically significant difference (**P<0.01).
Ascitic Fluid Leukocyte Count: A key indicator of SBP resolution, the ascitic fluid polymorphonuclear leukocyte count, showed a dramatic reduction in both groups post-treatment. However, the treatment group achieved a more substantial decrease. At baseline, ascitic fluid leukocyte counts were comparable (P>0.05). After 14 days, the treatment group’s ascitic fluid leukocyte count dropped from 1200 ± 350 × 106/L to 150 ± 50 × 106/L, whereas the control group’s count decreased from 1180 ± 320 × 106/L to 450 ± 120 × 106/L (***P<0.001), indicating more effective control of intraperitoneal infection in the treatment group.
3.5. Clinical Efficacy
The clinical efficacy evaluation revealed that the treatment group had a significantly higher total effective rate compared to the control group. In the treatment group, 22 patients (48.9%) achieved complete resolution (cure), 18 patients (40.0%) showed significant improvement (effective), and 5 patients (11.1%) were ineffective, resulting in a total effective rate of 88.9%. In contrast, the control group had 12 patients (26.7%) cured, 16 patients (35.6%) effective, and 17 patients (37.7%) ineffective, with a total effective rate of 62.3%. The difference in total effective rates between the two groups was statistically significant (χ²=7.86, P<0.01).
4. Discussion
Studies
| [14] | Fiore M, Gentile I, Maraolo AE, Leone S, Simeon V, Chiodini P, Pace MC, Gustot T, Taccone FS: Are third-generation cephalosporins still the empirical antibiotic treatment of community-acquired spontaneous bacterial peritonitis? A systematic review and meta-analysis. European journal of gastroenterology & hepatology 2018, 30(3): 329-336. |
| [16] | M RR, Llopis Roca F, Rubio Díaz R, Eduardo García D, Julián-Jiménez A: Early empirical antibiotherapy in patients attended for suspected sepsis in emergency departments: a systematic review. Emergencias: revista de la Sociedad Espanola de Medicina de Emergencias 2025, 37(1): 44-55. |
| [17] | Yim HJ, Kim TH, Suh SJ, Yim SY, Jung YK, Seo YS, Kang SH, Kim MY, Baik SK, Kim HS et al: Response-Guided Therapy with Cefotaxime, Ceftriaxone, or Ciprofloxacin for Spontaneous Bacterial Peritonitis: A Randomized Trial: A Validation Study of 2021 AASLD Practice Guidance for SBP. The American journal of gastroenterology 2023, 118(4): 654-663. |
[14, 16, 17]
indicate that for patients diagnosed or suspected of having SBP, empirical treatment should be initiated immediately, without waiting for the results of ascites culture and in vitro sensitivity tests. The current recommended approach is to use third-generation cephalosporins for empirical treatment. This treatment strategy has been supported by multiple studies in terms of its effectiveness and necessity. This paper discusses the efficacy of combining peritoneal lavage and rifoxacin with conventional treatment. The results show that the effective rate of the treatment group is higher than that of the control group. This result is supported and supplemented by many studies.
First, rifamycin, a non-absorbable antibiotic, has been shown to be highly effective in preventing SBP in patients with liver cirrhosis. Biecker
et al. | [18] | Kalambokis GN, Mouzaki A, Rodi M, Tsianos EV: Rifaximin for the prevention of spontaneous bacterial peritonitis. World journal of gastroenterology 2012, 18(14): 1700-1702. |
[18]
found that the use of rifamycin significantly reduced the neutrophil count in ascites and plasma endotoxin levels in patients with liver cirrhosis, thereby lowering the risk of SBP. Additionally, Lv
et al. | [19] | Lv XY, Ding HG, Zheng JF, Fan CL, Li L: Rifaximin improves survival in cirrhotic patients with refractory ascites: A real-world study. World journal of gastroenterology 2020, 26(2): 199-218. |
[19]
indicated that rifamycin improves systemic inflammation in patients with liver cirrhosis by regulating the structure and function of the gut microbiota, thus enhancing survival rates. These findings suggest that rifamycin has potential therapeutic advantages in managing complications associated with liver cirrhosis. Secondly, as a therapeutic approach, peritoneal lavage has shown positive outcomes in treating various abdominal infections and complications. Matsumoto
et al. | [20] | Matsumoto K, Miyake Y, Nakatsu M, Toyokawa T, Ando M, Hirohata M, Kato H, Yamamoto K: Usefulness of early-phase peritoneal lavage for treating severe acute pancreatitis. Internal medicine (Tokyo, Japan) 2014, 53(1): 1-6. |
[20]
have shown that early peritoneal lavage can effectively reduce the incidence of complications and mortality in patients with severe acute pancreatitis. Furthermore, Jallouli
et al. | [21] | Jallouli M, Hakim A, Znazen A, Sahnoun Z, Kallel H, Zghal K, Hammami A, Mhiri R: Rifamycin lavage in the treatment of experimental intra-abdominal infection. The Journal of surgical research 2009, 155(2): 191-194. |
[21]
the combination of peritoneal lavage with antibiotics, such as rifoxacin, can significantly decrease the number of bacteria in the abdominal cavity, thereby enhancing the treatment of infectious peritonitis. These findings underscore the critical role of peritoneal lavage in managing complex abdominal infections. In summary, the treatment regimen combining peritoneal lavage and rifoxacin has shown significant advantages in improving patient outcomes. By regulating the gut microbiota and reducing the bacterial load in the abdominal cavity, this combined therapy not only enhances both the effectiveness and success rate of treatment but also potentially reduces the risk of related complications. This finding provides new insights and evidence for optimizing the treatment of abdominal infections and complications associated with liver cirrhosis.
This study has the following limitations. First, the number of patients included is not large. This problem is common in many medical studies, especially in observational and experimental studies. Small sample size may lead to uncertainty in results and insufficient statistical power, thus affecting the reliability and generalizability of the research conclusions. Secondly, we did not analyze the long-term survival rate. The analysis of long-term survival rate is of great significance for evaluating the treatment effect and patient prognosis.
5. Conclusion
This study confirms that peritoneal lavage combined with rifaximin has a clear therapeutic effect on spontaneous peritonitis to a certain extent, increases the body's ability to metabolize ammonia, effectively prevents the occurrence of hepatic encephalopathy, and has relatively few complications. It is a method worthy of clinical promotion.
Abbreviations
ALT | Alanine Aminotransferase |
AST | Aspartate Aminotransferase |
Tbil | Total Bilirubin |
WBC | White Blood Cell |
CRP | C-Reactive Protein |
PCT | Procalcitonin |
SBP | SPONTANEOUS Bacterial Peritonitis |
TIPS | Transjugular Intrahepatic Portosystemic Shunt |
HRS | Hepatorenal Syndrome |
Author Contributions
Qin Peng: Conceptualization, Funding acquisition, Supervision, Writing - review & editing
Heng Shi: Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing - original draft, Writing - review & editing
Ethics Approval and Consent to Participate
The study was approved by the Human Research Ethics Committee of Shaoyang Central Hospital (KY-2024-33).
Funding
The research was financially supported by the Shaoyang Science and Technology Plan Project (No. 2024PT6170).
Conflicts of Interest
The authors have no conflicts of interest to declare.
References
| [1] |
Gordon FD: Ascites. Clinics in liver disease 2012, 16(2): 285-299.
|
| [2] |
Garcia-Tsao G: Current Management of the Complications of Cirrhosis and Portal Hypertension: Variceal Hemorrhage, Ascites, and Spontaneous Bacterial Peritonitis. Digestive diseases (Basel, Switzerland) 2016, 34(4): 382-386.
|
| [3] |
Tonon M, Piano S, Gambino CG, Romano A, Pilutti C, Incicco S, Brocca A, Sticca A, Bolognesi M, Angeli P: Outcomes and Mortality of Grade 1 Ascites and Recurrent Ascites in Patients with Cirrhosis. Clinical gastroenterology and hepatology: the official clinical practice journal of the American Gastroenterological Association 2021, 19(2): 358-366. e358.
|
| [4] |
Adebayo D, Neong SF, Wong F: Refractory Ascites in Liver Cirrhosis. The American journal of gastroenterology 2019, 114(1): 40-47.
|
| [5] |
Iannone G, Pompili E, De Venuto C, Pratelli D, Tedesco G, Baldassarre M, Caraceni P, Zaccherini G: The Role of Transjugular Intrahepatic Portosystemic Shunt for the Management of Ascites in Patients with Decompensated Cirrhosis. Journal of clinical medicine 2024, 13(5).
|
| [6] |
Kozaki K, M II, Takagi T, Fukuda T, Sanpei T, Terunuma Y, Yatabe Y, Akano K: Cell-Free and Concentrated Ascites Reinfusion Therapy for Decompensated Liver Cirrhosis. Therapeutic apheresis and dialysis: official peer-reviewed journal of the International Society for Apheresis, the Japanese Society for Apheresis, the Japanese Society for Dialysis Therapy 2016, 20(4): 376-382.
|
| [7] |
Sapey T, Mena E, Fort E, Laurin C, Kabissa D, Runyon BA, Mendler MH: Rapid diagnosis of spontaneous bacterial peritonitis with leukocyte esterase reagent strips in a European and in an American center. Journal of gastroenterology and hepatology 2005, 20(2): 187-192.
|
| [8] |
Liu PMF, de Carvalho ST, Fradico PF, Cazumbá MLB, Campos RGB, Simões ESAC: Hepatorenal syndrome in children: a review. Pediatric nephrology (Berlin, Germany) 2021, 36(8): 2203-2215.
|
| [9] |
Song Y, Yang X, Yu C: Understanding and Treating Hepatorenal Syndrome: Insights from Recent Research. Seminars in liver disease 2025.
|
| [10] |
Rao K, Qin S, Yang Y, Zhan K, Wu H, Zheng H, Huang S: Shenling Baizhu Powder Alleviates TNBS-Induced Colitis in Rats by Improving Intestinal Epithelial Permeability and Inhibiting Inflammation Through the TLR5/MyD88/NF-κB Pathway. Frontiers in pharmacology 2022, 13: 883918.
|
| [11] |
Singh V, De A, Mehtani R, Angeli P, Maiwall R, Satapathy S, Singal AK, Saraya A, Sharma BC, Eapen CE et al: Asia-Pacific association for study of liver guidelines on management of ascites in liver disease. Hepatology international 2023, 17(4): 792-826.
|
| [12] |
Hsieh CC, Lee CH, Li MC, Hong MY, Chi CH, Lee CC: Empirical third-generation cephalosporin therapy for adults with community-onset Enterobacteriaceae bacteraemia: Impact of revised CLSI breakpoints. International journal of antimicrobial agents 2016, 47(4): 297-303.
|
| [13] |
Rahal JJ: The role of carbapenems in initial therapy for serious Gram-negative infections. Critical care (London, England) 2008, 12 Suppl 4(Suppl 4): S5.
|
| [14] |
Fiore M, Gentile I, Maraolo AE, Leone S, Simeon V, Chiodini P, Pace MC, Gustot T, Taccone FS: Are third-generation cephalosporins still the empirical antibiotic treatment of community-acquired spontaneous bacterial peritonitis? A systematic review and meta-analysis. European journal of gastroenterology & hepatology 2018, 30(3): 329-336.
|
| [15] |
Praharaj DL, Premkumar M, Roy A, Verma N, Taneja S, Duseja A, Dhiman RK: Rifaximin Vs. Norfloxacin for Spontaneous Bacterial Peritonitis Prophylaxis: A Randomized Controlled Trial. Journal of clinical and experimental hepatology 2022, 12(2): 336-342.
|
| [16] |
M RR, Llopis Roca F, Rubio Díaz R, Eduardo García D, Julián-Jiménez A: Early empirical antibiotherapy in patients attended for suspected sepsis in emergency departments: a systematic review. Emergencias: revista de la Sociedad Espanola de Medicina de Emergencias 2025, 37(1): 44-55.
|
| [17] |
Yim HJ, Kim TH, Suh SJ, Yim SY, Jung YK, Seo YS, Kang SH, Kim MY, Baik SK, Kim HS et al: Response-Guided Therapy with Cefotaxime, Ceftriaxone, or Ciprofloxacin for Spontaneous Bacterial Peritonitis: A Randomized Trial: A Validation Study of 2021 AASLD Practice Guidance for SBP. The American journal of gastroenterology 2023, 118(4): 654-663.
|
| [18] |
Kalambokis GN, Mouzaki A, Rodi M, Tsianos EV: Rifaximin for the prevention of spontaneous bacterial peritonitis. World journal of gastroenterology 2012, 18(14): 1700-1702.
|
| [19] |
Lv XY, Ding HG, Zheng JF, Fan CL, Li L: Rifaximin improves survival in cirrhotic patients with refractory ascites: A real-world study. World journal of gastroenterology 2020, 26(2): 199-218.
|
| [20] |
Matsumoto K, Miyake Y, Nakatsu M, Toyokawa T, Ando M, Hirohata M, Kato H, Yamamoto K: Usefulness of early-phase peritoneal lavage for treating severe acute pancreatitis. Internal medicine (Tokyo, Japan) 2014, 53(1): 1-6.
|
| [21] |
Jallouli M, Hakim A, Znazen A, Sahnoun Z, Kallel H, Zghal K, Hammami A, Mhiri R: Rifamycin lavage in the treatment of experimental intra-abdominal infection. The Journal of surgical research 2009, 155(2): 191-194.
|
Cite This Article
-
APA Style
Heng, S., Qin, P. (2025). Enhanced Spontaneous Bacterial Peritonitis Management in Cirrhosis: Peritoneal Lavage with Targeted Antibiotic. International Journal of Gastroenterology, 9(2), 103-110. https://doi.org/10.11648/j.ijg.20250902.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Heng, S.; Qin, P. Enhanced Spontaneous Bacterial Peritonitis Management in Cirrhosis: Peritoneal Lavage with Targeted Antibiotic. Int. J. Gastroenterol. 2025, 9(2), 103-110. doi: 10.11648/j.ijg.20250902.13
Copy
|
Download
AMA Style
Heng S, Qin P. Enhanced Spontaneous Bacterial Peritonitis Management in Cirrhosis: Peritoneal Lavage with Targeted Antibiotic. Int J Gastroenterol. 2025;9(2):103-110. doi: 10.11648/j.ijg.20250902.13
Copy
|
Download
-
@article{10.11648/j.ijg.20250902.13,
author = {Shi Heng and Peng Qin},
title = {Enhanced Spontaneous Bacterial Peritonitis Management in Cirrhosis: Peritoneal Lavage with Targeted Antibiotic
},
journal = {International Journal of Gastroenterology},
volume = {9},
number = {2},
pages = {103-110},
doi = {10.11648/j.ijg.20250902.13},
url = {https://doi.org/10.11648/j.ijg.20250902.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20250902.13},
abstract = {Spontaneous bacterial peritonitis (SBP) is a severe complication of decompensated cirrhosis, associated with high mortality and poor prognosis. This study aimed to evaluate the efficacy of a combined therapeutic approach-peritoneal catheter lavage, intraperitoneal antibiotic injection, and oral rifaximin-on top of standard intravenous antibiotics for SBP in cirrhotic patients. A total of 90 cirrhotic patients with SBP were randomly assigned to either the treatment group (n=45) or the control group (n=45). Both groups received basic care including hepatoprotective therapy, albumin supplementation, and electrolyte correction. The control group was treated with intravenous ceftriaxone (2 g/day for 14 days), while the treatment group was added peritoneal lavage (daily cycles of draining ascites, infusing warm saline, and injecting intraperitoneal ceftriaxone) plus oral rifaximin (200 mg three times daily) to the same intravenous regimen. Baseline characteristics, including demographic data, cirrhosis severity (Child-Pugh grade), and comorbidities, were comparable between the two groups (all P>0.05). After 14 days of treatment, the treatment group showed significantly greater improvements in clinical symptoms (fever, abdominal pain, tenderness) and laboratory markers: liver function parameters (ALT, AST, TBil) decreased more markedly, and inflammatory indicators (WBC, CRP, PCT) were reduced to a larger extent compared to the control group (all P6/L to 150±50×106/L in the treatment group, versus 1180±320×106/L to 450±120×106/L in the control group (P<0.001). The total effective rate was significantly higher in the treatment group (88.9%) than in the control group (62.3%, P<0.01). These findings suggest that combining peritoneal lavage, intraperitoneal antibiotics, and oral rifaximin with standard intravenous therapy enhances SBP control, improves liver function, and reduces systemic inflammation in cirrhotic patients, thereby offering a more effective strategy for managing this life-threatening complication.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Enhanced Spontaneous Bacterial Peritonitis Management in Cirrhosis: Peritoneal Lavage with Targeted Antibiotic
AU - Shi Heng
AU - Peng Qin
Y1 - 2025/08/12
PY - 2025
N1 - https://doi.org/10.11648/j.ijg.20250902.13
DO - 10.11648/j.ijg.20250902.13
T2 - International Journal of Gastroenterology
JF - International Journal of Gastroenterology
JO - International Journal of Gastroenterology
SP - 103
EP - 110
PB - Science Publishing Group
SN - 2640-169X
UR - https://doi.org/10.11648/j.ijg.20250902.13
AB - Spontaneous bacterial peritonitis (SBP) is a severe complication of decompensated cirrhosis, associated with high mortality and poor prognosis. This study aimed to evaluate the efficacy of a combined therapeutic approach-peritoneal catheter lavage, intraperitoneal antibiotic injection, and oral rifaximin-on top of standard intravenous antibiotics for SBP in cirrhotic patients. A total of 90 cirrhotic patients with SBP were randomly assigned to either the treatment group (n=45) or the control group (n=45). Both groups received basic care including hepatoprotective therapy, albumin supplementation, and electrolyte correction. The control group was treated with intravenous ceftriaxone (2 g/day for 14 days), while the treatment group was added peritoneal lavage (daily cycles of draining ascites, infusing warm saline, and injecting intraperitoneal ceftriaxone) plus oral rifaximin (200 mg three times daily) to the same intravenous regimen. Baseline characteristics, including demographic data, cirrhosis severity (Child-Pugh grade), and comorbidities, were comparable between the two groups (all P>0.05). After 14 days of treatment, the treatment group showed significantly greater improvements in clinical symptoms (fever, abdominal pain, tenderness) and laboratory markers: liver function parameters (ALT, AST, TBil) decreased more markedly, and inflammatory indicators (WBC, CRP, PCT) were reduced to a larger extent compared to the control group (all P6/L to 150±50×106/L in the treatment group, versus 1180±320×106/L to 450±120×106/L in the control group (P<0.001). The total effective rate was significantly higher in the treatment group (88.9%) than in the control group (62.3%, P<0.01). These findings suggest that combining peritoneal lavage, intraperitoneal antibiotics, and oral rifaximin with standard intravenous therapy enhances SBP control, improves liver function, and reduces systemic inflammation in cirrhotic patients, thereby offering a more effective strategy for managing this life-threatening complication.
VL - 9
IS - 2
ER -
Copy
|
Download