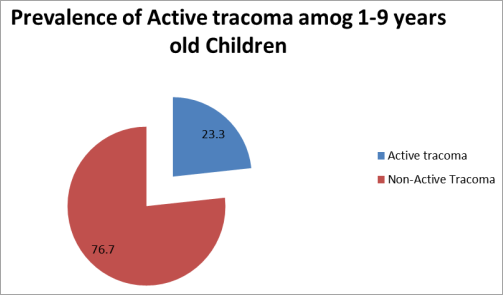
Background: The most common cause of blindness and one of the most neglected tropical diseases is trachoma. It is a significant public health issue in underdeveloped nations. Hands, fomites, and eye-seeking flies can spread it through direct contact with contaminated nasal and ocular secretions. The main objective of this study is to assess the prevalence and risk factors of active trachoma among 1–9-year-old children in Gulele Sub City in Addis Ababa, Ethiopia. Methods: A community-based cross-sectional study was conducted in the Gulele sub-city from May 1 to July 30. A systematic random sampling technique was implemented to select study participants. To assure and control the quality of the data, a validated tool, and a cross-checked system were implemented. Bivariable and multi-variable binary logistic regression were used to identify factors associated with active trachoma. 95% confidence intervals and P-values were used to measure the strength of the association, and a P-value <0.05 was considered statistically significant. Result: The result shows that the overall prevalence of active trachoma among preschool-aged children was 23.3% [95% CI: (19–25.1)]. Age of a child (AOR=1.63, 95% CI: 1.33, 2.03), frequently washing faces (AOR=1.46, 95% CI: 1.26, 2.42), a child with Unclean faces (AOR=2.83, 95% CI: 1.43, 3.64), improper solid waste disposal (AOR=4.24, 95% CI: 3.25, 5.25), were factors associated with active trachoma. Conclusion: The prevalence of active trachoma among preschool-aged children was high. The age of a child, frequently washing faces, the unclean face of the child, and proper solid waste disposal are important factors associated with active trachoma. This study indicated that trachoma is a public health problem Recommendation: to address the high prevalence of active trachoma among preschool-aged children, the following recommendations are essential: Enhance Hygiene Practices: Implement community education programs promoting regular face washing to reduce infection rates. Improve Sanitation: Ensure proper solid waste disposal and enhance access to clean water and sanitation facilities in endemic areas. Regular Health Surveillance: Conduct periodic trachoma prevalence surveys to monitor infection rates and identify at-risk populations. Integrate SAFE Strategy: Adopt the WHO's SAFE strategy, which includes surgery for advanced cases, mass antibiotic distribution, facial cleanliness promotion, and environmental improvements.
| Published in | International Journal of Infectious Diseases and Therapy (Volume 10, Issue 1) |
| DOI | 10.11648/j.ijidt.20251001.11 |
| Page(s) | 1-10 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Active Trachoma, Associated Factor, Ethiopia, Prevalence, Addis Ababa, Ethiopia
S.No | Proportion/factor | AOR | Calculated sample size | References | |
|---|---|---|---|---|---|
1 | The cooking room has a window | % exposed=3.5% | 0.28 | 78.1 | [16 ] |
% unexposed=33.5% | |||||
2. | Face wash using soap | % exposed=1.2% | 5.28 | 108 | [16 ] |
% unexposed=30.6% | |||||
Variables | Variables categories | Frequency (N=610) | Percentage (%) |
|---|---|---|---|
Sex of the child | Male | 254 | 41.7 |
female | 356 | 58.3 | |
The age group of a child | 1 to 4 years old | 342 | 56.1 |
5 to 9 years old | 268 | 43.9 | |
Education status of child | Preschool | 402 | 65.9 |
Student | 144 | 23.6 | |
not attending school | 64 | 10.5 | |
Number of children under 9 years in the household | Only one | 319 | 52.3 |
Two and above | 219 | 47.7 |
Variables | Variables categories | Frequency (N=610) | Percentage (%) |
|---|---|---|---|
Marital status of the mother or caregiver | Single | 126 | 20.7 |
Married | 302 | 49.5 | |
Divorced | 115 | 18.9 | |
widowed | 67 | 11.0 | |
Age of the mother or caregiver | 19–24 years | 39 | 6.4 |
25-34 years | 167 | 27.4 | |
35–49 years | 278 | 45.6 | |
≥49 years | 126 | 20.7 | |
Educational status of the mother or caregiver | Not educated | 183 | 30 |
Primary education | 152 | 24.9 | |
Secondary education | 227 | 37.2 | |
Diploma and above | 48 | 7.9 | |
Occupational status of the head of the household | Employed | 283 | 46.4 |
Unemployed | 127 | 20.8 | |
housewife | 200 | 32.8 | |
The economic status of Hhds | Poor | 199 | 32.6 |
Medium | 314 | 51.5 | |
high | 97 | 15.9 | |
Residency | Urban | 506 | 83 |
rural | 104 | 17 |
Variables | Variables categories | Frequency (N=610) | Percentage (%) |
|---|---|---|---|
Protected primary water Source of | Yes | 480 | 78.7 |
no | 130 | 21.3 | |
Time is taken to obtain water on a walk | <15 minute | 385 | 63.1 |
>15 minute | 225 | 36.9 | |
Access to sustainable water supply | Regional | 447 | 73.3 |
General | 163 | 26.7 | |
Utilization of adequate water for bathing | Yes | 424 | 69.5 |
No | 186 | 30.5 | |
Frequency of washing children’s face | Ones per day | 292 | 47.9 |
Two or more | 318 | 52.1 | |
Children facial cleanness | Clean | 288 | 47.2 |
Not clean | 322 | 52.8 | |
Ocular discharge | Yes | 103 | 16.9 |
No | 507 | 83.1 | |
Nasal discharge | Yes | 130 | 21.3 |
No | 480 | 78.7 | |
Cattle ownership | Yes | 181 | 29.7 |
No | 429 | 70.3 | |
A place where cattle pass night (n=181) | In the cattle house | 43 | 23.6 |
Living house but separately | 119 | 65.9 | |
Same room with the family | 19 | 10.5 | |
Having separated human and animal dowelling | Yes | 260 | 42.6 |
No | 350 | 57.4 | |
Separated cooking room | Yes | 320 | 52.5 |
No | 290 | 47.5 | |
Sharing towels | Yes | 118 | 19.3 |
No | 492 | 80.7 | |
improper solid waste disposal | Yes | 234 | 38.3 |
No | 376 | 61.6 | |
proper liquid waste disposal | Yes | 571 | 93.6 |
No | 39 | 6.4 | |
Having a clean house compound | Yes | 531 | 87 |
No | 79 | 13 |
Variables | Variables categories | Frequency (N=610) | Percentage (%) |
|---|---|---|---|
Observed factors: animal faces around the house | Yes | 57 | 9.3 |
No | 553 | 90.7 | |
Observed factors: flies around the house | Yes | 164 | 26.9 |
No | 446 | 73.1 | |
Self-reported hygiene and behavior change: Wash children’s face | Yes | 429 | 70.3 |
No | 181 | 29.7 | |
Self-reported hygiene and behavior change: wipe faces with shawls /towel | Yes | 423 | 69.3 |
No | 187 | 30.7 |
Variables | Active Trachoma | NO Active Trachoma | Crude OR (95%CI) | Adjusted OR (95%CI) | P-Value |
|---|---|---|---|---|---|
Age | |||||
Being1-4 years | 81 | 207 | 2.001(0.001-3) | 1.63(1.33-2.03)** | 0.001 |
Being5-9 years | 61 | 261 | 1 | 1 | |
frequently washing faces | |||||
yes | 65 | 207 | 3.00(1.23-4.02) | 1.46(1.26-2.42)** | 0.000 |
no | 77 | 261 | 1 | 1 | |
Unclean faces | |||||
Yes | 117 | 371 | 2.60(2.05-8.05) | 2.83(1.43-3.64) ** | 0.001 |
no | 25 | 97 | 1 | 1 | |
Improper solid waste disposal | |||||
Yes | 134 | 100 | 5.16(2.17-10.29 | 4.24(3.25-5.25) ** | 0.002 |
no | 76 | 300 | 1 | 1 |
CDC | Center for Disease Control and Prevention |
CI | Confidence Interval |
CO | Corneal Opacity |
GET | Global Elimination of Trachoma |
ITI | International Trachoma Initiative |
MOH | Ministry of Health |
TF | Trachoma Follicular |
TS | Trachomatous Scaring |
RRR | Relative Risk Ratio |
WHO | World Health Organization |
| [1] | Solomon, A. W., et al., How much trachomatous trichiasis is there? A guide to calculating district-level estimates. Community eye health, 2019. 31(104): p. S5. |
| [2] | Habtamu, E., et al., Trachoma and relative poverty: a case-control study. PLoS neglected tropical diseases, 2015. 9(11): p. e0004228. |
| [3] | Karimurio, J., et al., Prevalence of trachoma in six districts of Kenya. East African medical journal, 2006. 83(4): p. 63-68. |
| [4] | Al-Rifai, K. M., Trachoma through history. International ophthalmology, 1988. 12(1): p. 9-14. |
| [5] | Southisombath, K., et al., National trachoma assessment in the Lao People’s Democratic Republic in 2013–2014. Ophthalmic epidemiology, 2016. 23(sup1): p. 8-14. |
| [6] | Dawson, C., et al., A comparison of oral azithromycin with topical oxytetracycline/polymyxin for the treatment of trachoma in children. Clinical Infectious Diseases, 1997. 24(3): p. 363-368. |
| [7] | NYAMWARO, C. M., BARRIERS TO EFFECTIVE TRACHOMA CONTROL AMONG CHILDREN AGED 1-9 YEARS OLD IN MAGADI DIVISION, KAJIADO COUNTY, KENYA. 2014, KENYATTA UNIVERSITY. |
| [8] | Last, A. R., et al., Risk factors for active trachoma and ocular Chlamydia trachomatis infection in treatment-naïve trachoma-hyperendemic communities of the Bijagós Archipelago, Guinea Bissau. PLoS Negl Trop Dis, 2014. 8(6): p. e2900. |
| [9] | Bourne, R. R., et al., Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: a systematic review and meta-analysis. The Lancet Global Health, 2017. 5(9): p. e888-e897. |
| [10] | Admassu, F., S. Bayu, A. Bejiga, and B. Amare, Active trachoma two years after three rounds of azithromycin mass treatment in Cheha district Gurage zone, Southern Ethiopia. BMC pediatrics, 2013. 13(1): p. 1-5. |
| [11] | Hu, V. H., et al., Epidemiology and control of trachoma: systematic review. Tropical Medicine & International Health, 2010. 15(6): p. 673-691. |
| [12] | Demissie Gizaw, G., Z. Aderaw Alemu, and K. T. Kibret, Assessment of knowledge and practice of health workers towards tuberculosis infection control and associated factors in public health facilities of Addis Ababa, Ethiopia: A cross-sectional study. Archives of public health, 2015. 73: p. 1-9. |
| [13] | Kassaw, M. W., et al., Prevalence and associations of active trachoma among rural preschool children in Wadla district, northern Ethiopia. BMC ophthalmology, 2020. 20(1): p. 1-10. |
| [14] | Quigley, H. A., Number of people with glaucoma worldwide. British journal of ophthalmology, 1996. 80(5): p. 389-393. |
| [15] | Mesfin, M. M., et al., A community-based trachoma survey: prevalence and risk factors in the Tigray region of northern Ethiopia. Ophthalmic epidemiology, 2006. 13(3): p. 173-181. |
| [16] | Abebo, T. A. and D. J. Tesfaye, Prevalence and distribution of active trachoma among children 1-9 years old at Leku town, southern Ethiopia. Curr Pediatr Res, 2017. |
| [17] | Burton, M. J. and D. C. Mabey, The global burden of trachoma: a review. PLoS Negl Trop Dis, 2009. 3(10): p. e460. |
| [18] | Muhammad, N., M. Damina, M. M. Umar, and S. Isiyaku, Trachoma prevalence and risk factors in eight local government areas of Zamfara State. Nigerian Journal of Ophthalmology, 2015. 23(2): p. 48-53. |
| [19] | Gebrie, A., et al., Prevalence and associated factors of active trachoma among children in Ethiopia: a systematic review and meta-analysis. BMC infectious diseases, 2019. 19(1): p. 1-12. |
| [20] | mondiale de la Santé, O. and W. H. Organization, WHO Alliance for the Global Elimination of Trachoma by 2020: progress report, 2019 360 COVID-19 update–Alliance de l’OMS pour l’élimination mondiale du trachome d’ici 2020: Rapport de situation, 2019 360 Le point sur la maladie à coronavirus 2019 (COVID-19). Weekly Epidemiological Record= Relevé épidémiologique hebdomadaire, 2020. 95(30): p. 349-360. |
| [21] | Bailey, R., et al., The duration of human ocular Chlamydia trachomatis infection is age dependent. Epidemiology & Infection, 1999. 123(3): p. 479-486. |
| [22] | Reda, G., D. Yemane, and A. Gebreyesus, Prevalence and associated factors of active trachoma among 1–9 years old children in Deguatemben, Tigray, Ethiopia, 2018: community cross-sectional study. BMC ophthalmology, 2020. 20: p. 1-9. |
| [23] | Frick, K. D., E. V. Basilion, C. L. Hanson, and M. A. Colchero, Estimating the burden and economic impact of trachomatous visual loss. Ophthalmic epidemiology, 2003. 10(2): p. 121-132. |
APA Style
Mohammed, A. S., Tesfaye, E., Yesuf, M. H., Minda, Z., Yesuf, A. H., et al. (2025). Prevalence and Risk Factors of Active Trachoma Among 1–9-Year-Old Children in Gulele Sub City, Addis Ababa, Ethiopia, 2023. International Journal of Infectious Diseases and Therapy, 10(1), 1-10. https://doi.org/10.11648/j.ijidt.20251001.11
ACS Style
Mohammed, A. S.; Tesfaye, E.; Yesuf, M. H.; Minda, Z.; Yesuf, A. H., et al. Prevalence and Risk Factors of Active Trachoma Among 1–9-Year-Old Children in Gulele Sub City, Addis Ababa, Ethiopia, 2023. Int. J. Infect. Dis. Ther. 2025, 10(1), 1-10. doi: 10.11648/j.ijidt.20251001.11
@article{10.11648/j.ijidt.20251001.11,
author = {Abdurehman Seid Mohammed and Emebet Tesfaye and Mustofa Hassen Yesuf and Zewdu Minda and Ali Hassen Yesuf and Getachew Mekete Diress},
title = {Prevalence and Risk Factors of Active Trachoma Among 1–9-Year-Old Children in Gulele Sub City, Addis Ababa, Ethiopia, 2023},
journal = {International Journal of Infectious Diseases and Therapy},
volume = {10},
number = {1},
pages = {1-10},
doi = {10.11648/j.ijidt.20251001.11},
url = {https://doi.org/10.11648/j.ijidt.20251001.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijidt.20251001.11},
abstract = {Background: The most common cause of blindness and one of the most neglected tropical diseases is trachoma. It is a significant public health issue in underdeveloped nations. Hands, fomites, and eye-seeking flies can spread it through direct contact with contaminated nasal and ocular secretions. The main objective of this study is to assess the prevalence and risk factors of active trachoma among 1–9-year-old children in Gulele Sub City in Addis Ababa, Ethiopia. Methods: A community-based cross-sectional study was conducted in the Gulele sub-city from May 1 to July 30. A systematic random sampling technique was implemented to select study participants. To assure and control the quality of the data, a validated tool, and a cross-checked system were implemented. Bivariable and multi-variable binary logistic regression were used to identify factors associated with active trachoma. 95% confidence intervals and P-values were used to measure the strength of the association, and a P-value Result: The result shows that the overall prevalence of active trachoma among preschool-aged children was 23.3% [95% CI: (19–25.1)]. Age of a child (AOR=1.63, 95% CI: 1.33, 2.03), frequently washing faces (AOR=1.46, 95% CI: 1.26, 2.42), a child with Unclean faces (AOR=2.83, 95% CI: 1.43, 3.64), improper solid waste disposal (AOR=4.24, 95% CI: 3.25, 5.25), were factors associated with active trachoma. Conclusion: The prevalence of active trachoma among preschool-aged children was high. The age of a child, frequently washing faces, the unclean face of the child, and proper solid waste disposal are important factors associated with active trachoma. This study indicated that trachoma is a public health problem Recommendation: to address the high prevalence of active trachoma among preschool-aged children, the following recommendations are essential: Enhance Hygiene Practices: Implement community education programs promoting regular face washing to reduce infection rates. Improve Sanitation: Ensure proper solid waste disposal and enhance access to clean water and sanitation facilities in endemic areas. Regular Health Surveillance: Conduct periodic trachoma prevalence surveys to monitor infection rates and identify at-risk populations. Integrate SAFE Strategy: Adopt the WHO's SAFE strategy, which includes surgery for advanced cases, mass antibiotic distribution, facial cleanliness promotion, and environmental improvements.},
year = {2025}
}
TY - JOUR T1 - Prevalence and Risk Factors of Active Trachoma Among 1–9-Year-Old Children in Gulele Sub City, Addis Ababa, Ethiopia, 2023 AU - Abdurehman Seid Mohammed AU - Emebet Tesfaye AU - Mustofa Hassen Yesuf AU - Zewdu Minda AU - Ali Hassen Yesuf AU - Getachew Mekete Diress Y1 - 2025/01/07 PY - 2025 N1 - https://doi.org/10.11648/j.ijidt.20251001.11 DO - 10.11648/j.ijidt.20251001.11 T2 - International Journal of Infectious Diseases and Therapy JF - International Journal of Infectious Diseases and Therapy JO - International Journal of Infectious Diseases and Therapy SP - 1 EP - 10 PB - Science Publishing Group SN - 2578-966X UR - https://doi.org/10.11648/j.ijidt.20251001.11 AB - Background: The most common cause of blindness and one of the most neglected tropical diseases is trachoma. It is a significant public health issue in underdeveloped nations. Hands, fomites, and eye-seeking flies can spread it through direct contact with contaminated nasal and ocular secretions. The main objective of this study is to assess the prevalence and risk factors of active trachoma among 1–9-year-old children in Gulele Sub City in Addis Ababa, Ethiopia. Methods: A community-based cross-sectional study was conducted in the Gulele sub-city from May 1 to July 30. A systematic random sampling technique was implemented to select study participants. To assure and control the quality of the data, a validated tool, and a cross-checked system were implemented. Bivariable and multi-variable binary logistic regression were used to identify factors associated with active trachoma. 95% confidence intervals and P-values were used to measure the strength of the association, and a P-value Result: The result shows that the overall prevalence of active trachoma among preschool-aged children was 23.3% [95% CI: (19–25.1)]. Age of a child (AOR=1.63, 95% CI: 1.33, 2.03), frequently washing faces (AOR=1.46, 95% CI: 1.26, 2.42), a child with Unclean faces (AOR=2.83, 95% CI: 1.43, 3.64), improper solid waste disposal (AOR=4.24, 95% CI: 3.25, 5.25), were factors associated with active trachoma. Conclusion: The prevalence of active trachoma among preschool-aged children was high. The age of a child, frequently washing faces, the unclean face of the child, and proper solid waste disposal are important factors associated with active trachoma. This study indicated that trachoma is a public health problem Recommendation: to address the high prevalence of active trachoma among preschool-aged children, the following recommendations are essential: Enhance Hygiene Practices: Implement community education programs promoting regular face washing to reduce infection rates. Improve Sanitation: Ensure proper solid waste disposal and enhance access to clean water and sanitation facilities in endemic areas. Regular Health Surveillance: Conduct periodic trachoma prevalence surveys to monitor infection rates and identify at-risk populations. Integrate SAFE Strategy: Adopt the WHO's SAFE strategy, which includes surgery for advanced cases, mass antibiotic distribution, facial cleanliness promotion, and environmental improvements. VL - 10 IS - 1 ER -
Department of Public Health, Saint Peter Specialized Hospital, Addis Ababa, Ethiopia
Department of Public Health, Saint Peter Specialized Hospital, Addis Ababa, Ethiopia
Department of Internal Medicine, Saint Peter Specialized Hospital, Addis Ababa, Ethiopia
Department of Anaesthesia Saint Peter Specialized Hospital, Addis Ababa, Ethiopia
Department of Urologic-Surgery, School of Medicine, Wollo University, Dessie, Ethiopia
Department of Anesthesia, College of Health Sciences, School of Medicine, Debre Tabor University, Debre Tabor, Ethiopia
Information