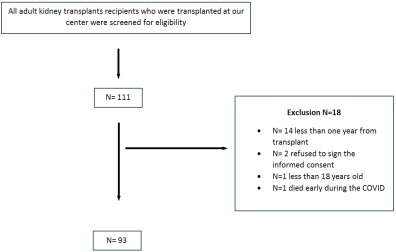
Background: Kidney transplant recipients are immunocompromised and at high risk of developing COVID-19. Tixagevimab/cilgavimab has been shown to reduce the risk of COVID-19 in immunocompromised individuals. However, information regarding the safety and efficacy of tixagevimab/cilgavimab use in kidney transplant recipients remains limited. Therefore, in this study, we aimed to evaluate the efficacy and safety of tixagevimab/cilgavimab in individuals who have undergone kidney transplantation. Methods: A retrospective, single-center study was conducted on all patients who underwent kidney transplantation between June 2022 and January 2023. The recipients were divided into treatment and control groups based on tixagevimab/cilgavimab therapy status. The incidence of COVID-19, acute rejection, hypersensitivity reactions, and cardiac events was compared between the groups. Results: A total of 93 patients were included in the study, of whom 38 received tixagevimab/cilgavimab. Prior to drug administration, 38 patients (40.9%) were infected with COVID-19; of these, 12 (31.6%) required hospitalization and two (5.2%) required admission to the intensive care unit (ICU). During the post-administration period, seven patients (7.5%) developed COVID-19; of these patients, four (57%) received tixagevimab/cilgavimab, and three (43%) did not. None of the patients required hospitalization or ICU admission. Conclusion: The incidence of COVID-19 was similar across study groups. However, the severity of the infection appeared to be milder in patients who received tixagevimab/cilgavimab.
| Published in | International Journal of Infectious Diseases and Therapy (Volume 11, Issue 1) |
| DOI | 10.11648/j.ijidt.20261101.12 |
| Page(s) | 9-16 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
COVID-19, Tixagevimab, Cilgavimab
Characteristic | Total (n =93) | Received 150 mg. (n=15) | Received 300 mg. (n=23) | Didn't receive (n= 55) |
|---|---|---|---|---|
Gender, n (%) | ||||
Female | 33 (35.5%) | 5 (33.3%) | 9 (39.1%) | 19 (34.5%) |
Male | 60 (64.5%) | 10 (66.7%) | 14 (60.9%) | 36 (65.5%) |
Age, mean (SD) | 47.1 (13.70) | 47.5 (14.7) | 46.13 (15.19) | 46.6 (14.8) |
ABO, n (%) | ||||
A | 30 (32.3%) | 7 (46.7%) | 4 (17.4%) | 19 (34.5%) |
AB | 4 (4.3%) | 0 | 2 (8.7%) | 2 (3.6%) |
B | 15 (16.1%) | 1 (6.7%) | 5 (21.7%) | 9 (16.4%) |
O | 44 (47.3%) | 7 (46.7%) | 12 (52.2%) | 25 (45.5%) |
Induction therapy, n (%) | ||||
ATG | 43 (46.2%) | 9 (60%) | 15 (65.2%) | 19 (34.5%) |
Basiliximab | 22 (23.7%) | 4 (26.7%) | 6 (26.1%) | 12 (21.8%) |
Unknown | 28 (30.1%) | 2 (13.3%) | 2 (8.7%) | 24 (43.6%) |
Renal Disease, n (%) | ||||
Alport | 1 (1.1%) | 0 | 0 | 1 (1.8%) |
APCKD | 4 (4.3%) | 3 (20%) | 1 (4.3%) | - |
DM | 22 (23.7%) | 5 (33.3%) | 8 (34.8%) | 9 (16.4%) |
FSGS | 4 (4.3%) | 0 | 1 (4.3%) | 3 (5.5%) |
HTN | 19 (20.4%) | 2 (13.3%) | 4 (17.4%) | 13 (23.6%) |
IgA | 2 (2.2%) | 0 | 0 | 2 (3.6%) |
Lupus nephritis | 1 (1.1%) | 0 | 0 | 1 (1.8%) |
other | 6 (6.5%) | 0 | 1 (4.3%) | 5 (9.1%) |
Reflux | 4 (4.3%) | 0 | 1 (4.3%) | 3 (5.5%) |
Unknown | 30 (32.3%) | 5 (33.3%) | 7 (30.4%) | 18 (32.7%) |
DM, n (%) | ||||
Yes | 42 (45.2%) | 9 (60%) | 10 (43.5%) | 23 (41.8%) |
Smoker, n (%) | ||||
Yes | 11 (11.8%) | 3 (20%) | 3 (13%) | 5 (9.1%) |
BMI, mean (SD) | 28.44 (5.8) | 29.3 (4.5) | 28.14 (6.1) | 28.6 (5.5) |
Dose of vaccine, n (%) | ||||
1 | 1 (1.1%) | 0 | 0 | 1 (1.8%) |
2 | 11 (11.8%) | 1 (6.7%) | 3 (13%) | 7 (12.7%) |
3 | 74 (79.6%) | 11 (73.3%) | 18 (78.3%) | 45 (81.8%) |
4 | 7 (7.5%) | 3 (20%) | 2 (8.7%) | 2 (3.6%) |
CNI, n (%) | ||||
Cyclo | 4 (4.3%) | 0 | 1 (4.3%) | 3 (5.5%) |
Tac | 89 (95.7%) | 15 (100%) | 22 (95.7%) | 52 (94.5%) |
MMF, n (%) | ||||
Yes | 84 (90.3%) | 15 (100%) | 21 (91.3%) | 48 (87.3%) |
Steroid, n (%) | ||||
Yes | 91 (97.8%) | 15 (100%) | 22 (95.7%) | 54 (98.2%) |
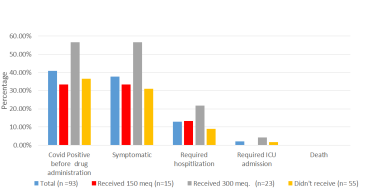
Characteristic | Total (n =93) | Received 150 mg. (n=15) | Received 300 mg. (n=23) | Didn't receive (n= 55) |
|---|---|---|---|---|
Covid Positive before July 2022 | 38 (40.9%) | 5 (13.1%) | 13 (34.2%) | 20 (52.6%) |
Symptomatic | 35 (92.1%) | 5 (13.1%) | 13 (34.2%) | 17 (44.7%) |
Required hospitalization | 12 (31.6%) | 2 (5.2%) | 5 (13.1%) | 5 (13.1%) |
Required ICU admission | 2 (5.2%) | 0 | 1 (2.6%) | 1 (2.6%) |
Death | 0 | 0 | 0 | 0 |
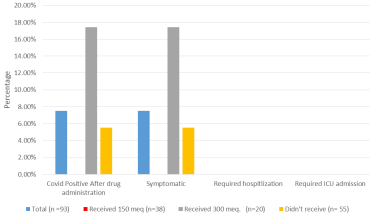
Covid Positive After July 2022 | 7 (7.5%) | 0 | 4 (57%) | 3 (43%) |
Symptomatic | 7 (100%) | 0 | 4 (57%) | 3 (43%) |
Required hospitalization | 0 | 0 | 0 | 0 |
Required ICU admission | 0 | 0 | 0 | 0 |
Death | 0 | 0 | 0 | 0 |
Characteristic | Total (n =93) | Received 150 mg. (n=15) | Received 300 mg. (n=23) | Didn't receive (n= 55) |
|---|---|---|---|---|
Anaphylactic reaction | 3 (3.2%) | 3 (20%) | 0 | 0 |
Bleeding | 0 | 0 | 0 | 0 |
AKI | 5 (5.4%) | 2 (13.3%) | 2 (8.7%) | 1 (1.18%) |
Characteristic | Receiving | P value | |
|---|---|---|---|
No (n= 55, 100%) | Yes (n=38, 100%) | ||
Covid Positive before July 2022 | 20 (52.6%) | 18 (47.4%) | 0.391 |
Symptomatic | 17 (48.6%) | 18 (51.4%) | 0.286 |
Required hospitalization | 5 (41.7%) | 7 (58.3%) | 0.267 |
Required ICU admission | 1 (50%) | 1 (50%) | 0.400 |
Death | 0 | 0 | 0.109 |
Covid Positive After July 2022 | 3 (42.9%) | 4 (57.1%) | 0.438 |
Symptomatic | 3 (42.9%) | 4 (57.1%) | 0.152 |
Required hospitalization | 0 | 0 | 0.082 |
Required ICU admission | 0 | 0 | 0.082 |
Death | 0 | 0 | 0.082 |
BMI | Body Mass Index |
(CNI) | Calcineurin Inhibitor |
ATG | Antithymocyte Globulin |
AKI | Acute Kidney Injury |
ICU | Intensive Care Unit |
| [1] | Han SH, Yoo SG, Han K Do, La Y, Kwon DE, Lee KH. The incidence and effect of cytomegalovirus disease on mortality in transplant recipients and general population: Real-world nationwide cohort data. Int J Med Sci. 2021; 18(14): 3333–41. |
| [2] | Kumar D, Ferreira VH, Blumberg E, Silveira F, Cordero E, Perez-Romero P, et al. A 5-year prospective multicenter evaluation of influenza infection in transplant recipients. Clin Infect Dis. 2018; 67(9): 1322–9. |
| [3] | Johnson LE, D’Agata EMC, Paterson DL, Clarke L, Qureshi ZA, Potoski BA, et al. Pseudomonas aeruginosa bacteremia over a 10-year period: Multidrug resistance and outcomes in transplant recipients. Transpl Infect Dis. 2009; 11(3): 227–34. |
| [4] | Levin MJ, Ustianowski A, De Wit S, Launay O, Avila M, Templeton A, et al. Intramuscular AZD7442 (Tixagevimab–Cilgavimab) for Prevention of Covid-19. N Engl J Med. 2022; 386(23): 2188–200. |
| [5] | AlShaqaq A, AlDemerdash M, AlAbadi A, Elgadaa B, Musaied N, Shaikh I, et al. Safety and Antibody Response to BNT162b2 and ChAdOx1 nCoV-19 Vaccines in Kidney Transplant Recipients. J Environ Sci Public Heal. 2021; 05(04): 407–19. |
| [6] | Focosi D, McConnell S, Casadevall A, Cappello E, Valdiserra G, Tuccori M. Monoclonal antibody therapies against SARS-CoV-2. Lancet Infect Dis [Internet]. 2022; 22(11): e311–26. Available from: |
| [7] | Montgomery H, Hobbs FDR, Padilla F, Arbetter D, Templeton A, Seegobin S, et al. Efficacy and safety of intramuscular administration of tixagevimab–cilgavimab for early outpatient treatment of COVID-19 (TACKLE): a phase 3, randomised, double-blind, placebo-controlled trial. Lancet Respir Med. 2022; 10(10): 985–96. |
| [8] | Keam SJ. Tixagevimab + Cilgavimab: First Approval. Drugs [Internet]. 2022; 82(9): 1001–10. Available from: |
| [9] | FDA. Coronavirus (COVID-19) Update: FDA Authorizes New Long-Acting Monoclonal Antibodies for Pre-exposure Prevention of COVID-19 in Certain Individuals [Internet]. |
| [10] | Nguyen Y, Flahault A, Chavarot N, Melenotte C, Cheminant M, Deschamps P, et al. Pre-exposure prophylaxis with tixagevimab and cilgavimab (Evusheld) for COVID-19 among 1112 severely immunocompromised patients. Clin Microbiol Infect. 2022; 28(12): 1654.e1-1654.e4. |
| [11] | Kaminski, Hannah, MickaelGiga, Agathe Vermorel L. COVID-19 morbidity decreases with tixagevimab–cilgavimab preexposure prophylaxisinkidney transplant recipient nonresponders orlow-vaccine responders. 2020; (January): 2020–3. |
| [12] | McConnell D, Harte M, Walsh C, Murphy D, Nichol A, Barry M, et al. Comparative effectiveness of neutralising monoclonal antibodies in high risk COVID-19 patients: a Bayesian network meta-analysis. Sci Rep. 2022; 12(1): 1–12. |
| [13] | Sarrell BA, Bloch K, El Chediak A, Kumm K, Tracy K, Forbes RC, et al. Monoclonal antibody treatment for COVID-19 in solid organ transplant recipients. Transpl Infect Dis. 2022; 24(1): 1–10. |
| [14] | Loo YM, McTamney PM, Arends RH, Abram ME, Aksyuk AA, Diallo S, et al. The SARS-CoV-2 monoclonal antibody combination, AZD7442, is protective in nonhuman primates and has an extended half-life in humans. Sci Transl Med. 2022; 14(635): 1–21. |
| [15] | Benotmane I, Velay A, Gautier-Vargas G, Olagne J, Obrecht A, Cognard N, et al. Breakthrough COVID-19 cases despite prophylaxis with 150 mg of tixagevimab and 150 mg of cilgavimab in kidney transplant recipients. Am J Transplant. 2022; 22(11): 2675–81. |
| [16] | Al Jurdi A, Morena L, Cote M, Bethea E, Azzi J, Riella L V. Tixagevimab/cilgavimab pre-exposure prophylaxis is associated with lower breakthrough infection risk in vaccinated solid organ transplant recipients during the omicron wave. Am J Transplant. 2022; 22(12): 3130–6. |
| [17] | Benotmane I, Velay A, Gautier-Vargas G, Olagne J, Thaunat O, Fafi-Kremer S, et al. Pre-exposure prophylaxis with 300 mg Evusheld elicits limited neutralizing activity against the Omicron variant. Kidney Int. 2022; 102(2): 442–4. |
| [18] | Harris a D, Goodman KE, Magder LS, Baghdadi JD, Pineles L, Levine AR, et al. Clinical Infectious Diseases Clinical Infectious Diseases ® 2021;73(11): e4113-23. 2022; 75(Xx Xx): 312–3. Available from: |
| [19] | Focosi, Daniele AC. A Critical Analysis of the Use of Cilgavimab plus Tixagevimab Monoclonal Antibody Cocktail (EvusheldTM) for COVID-19 Prophylaxis and Treatmentxis and Treatment. Viruses. 2022; 14(1999). |
| [20] | Benotmane I, Olagne J, Gautier-Vargas G, Cognard N, Heibel F, Braun-Parvez L, et al. Tixagevimab-cilgavimab as an Early Treatment for COVID-19 in Kidney Transplant Recipients. Transplantation. 2023; Publish Ah. |
| [21] | Gottlieb J, Simon S, Barton J, Barnikel M, Bachmann M, Klingenberg MS, et al. Efficacy of pre-exposure prophylaxis to prevent SARS-CoV-2 infection after lung transplantation: a two center cohort study during the omicron era. Infection [Internet]. 2023; (0123456789). Available from: |
| [22] | Cochran W, Salto-Alejandre S, Barker L, Langlee J, Freed K, Carter D, et al. COVID-19 Outcomes in Solid Organ Transplant Recipients Who Received Tixagevimab-cilgavimab Prophylaxis and/or Bebtelovimab Treatment in a Nurse-driven Monoclonal Antibody Program during the Omicron Surge. Transplantation. 2023; 107(2): E60–1. |
| [23] | Alejo JL, Kim JD, Chiang TPY, Avery RK, Karaba AH, Jefferis A, et al. Patient-reported outcomes after Tixagevimab and Cilgavimab pre-exposure prophylaxis among solid organ transplant recipients: Safety, effectiveness, and perceptions of risk. Clin Transplant. 2023; 37(4): 1–8. |
APA Style
Habibullah, Z., Bukhari, M., Al-Otaibi, N., Albadawi, N., Khalil, M., et al. (2026). Efficacy and Outcome of Tixagevimab-Cilgavimab Prophylaxis Administration in Kidney Transplant Patients. International Journal of Infectious Diseases and Therapy, 11(1), 9-16. https://doi.org/10.11648/j.ijidt.20261101.12
ACS Style
Habibullah, Z.; Bukhari, M.; Al-Otaibi, N.; Albadawi, N.; Khalil, M., et al. Efficacy and Outcome of Tixagevimab-Cilgavimab Prophylaxis Administration in Kidney Transplant Patients. Int. J. Infect. Dis. Ther. 2026, 11(1), 9-16. doi: 10.11648/j.ijidt.20261101.12
@article{10.11648/j.ijidt.20261101.12,
author = {Zainab Habibullah and Muhammed Bukhari and Nouf Al-Otaibi and Nashat Albadawi and Mohammed Khalil and Abdulhakeem Al-Marwani},
title = {Efficacy and Outcome of Tixagevimab-Cilgavimab Prophylaxis Administration in Kidney Transplant Patients},
journal = {International Journal of Infectious Diseases and Therapy},
volume = {11},
number = {1},
pages = {9-16},
doi = {10.11648/j.ijidt.20261101.12},
url = {https://doi.org/10.11648/j.ijidt.20261101.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijidt.20261101.12},
abstract = {Background: Kidney transplant recipients are immunocompromised and at high risk of developing COVID-19. Tixagevimab/cilgavimab has been shown to reduce the risk of COVID-19 in immunocompromised individuals. However, information regarding the safety and efficacy of tixagevimab/cilgavimab use in kidney transplant recipients remains limited. Therefore, in this study, we aimed to evaluate the efficacy and safety of tixagevimab/cilgavimab in individuals who have undergone kidney transplantation. Methods: A retrospective, single-center study was conducted on all patients who underwent kidney transplantation between June 2022 and January 2023. The recipients were divided into treatment and control groups based on tixagevimab/cilgavimab therapy status. The incidence of COVID-19, acute rejection, hypersensitivity reactions, and cardiac events was compared between the groups. Results: A total of 93 patients were included in the study, of whom 38 received tixagevimab/cilgavimab. Prior to drug administration, 38 patients (40.9%) were infected with COVID-19; of these, 12 (31.6%) required hospitalization and two (5.2%) required admission to the intensive care unit (ICU). During the post-administration period, seven patients (7.5%) developed COVID-19; of these patients, four (57%) received tixagevimab/cilgavimab, and three (43%) did not. None of the patients required hospitalization or ICU admission. Conclusion: The incidence of COVID-19 was similar across study groups. However, the severity of the infection appeared to be milder in patients who received tixagevimab/cilgavimab.},
year = {2026}
}
TY - JOUR T1 - Efficacy and Outcome of Tixagevimab-Cilgavimab Prophylaxis Administration in Kidney Transplant Patients AU - Zainab Habibullah AU - Muhammed Bukhari AU - Nouf Al-Otaibi AU - Nashat Albadawi AU - Mohammed Khalil AU - Abdulhakeem Al-Marwani Y1 - 2026/03/10 PY - 2026 N1 - https://doi.org/10.11648/j.ijidt.20261101.12 DO - 10.11648/j.ijidt.20261101.12 T2 - International Journal of Infectious Diseases and Therapy JF - International Journal of Infectious Diseases and Therapy JO - International Journal of Infectious Diseases and Therapy SP - 9 EP - 16 PB - Science Publishing Group SN - 2578-966X UR - https://doi.org/10.11648/j.ijidt.20261101.12 AB - Background: Kidney transplant recipients are immunocompromised and at high risk of developing COVID-19. Tixagevimab/cilgavimab has been shown to reduce the risk of COVID-19 in immunocompromised individuals. However, information regarding the safety and efficacy of tixagevimab/cilgavimab use in kidney transplant recipients remains limited. Therefore, in this study, we aimed to evaluate the efficacy and safety of tixagevimab/cilgavimab in individuals who have undergone kidney transplantation. Methods: A retrospective, single-center study was conducted on all patients who underwent kidney transplantation between June 2022 and January 2023. The recipients were divided into treatment and control groups based on tixagevimab/cilgavimab therapy status. The incidence of COVID-19, acute rejection, hypersensitivity reactions, and cardiac events was compared between the groups. Results: A total of 93 patients were included in the study, of whom 38 received tixagevimab/cilgavimab. Prior to drug administration, 38 patients (40.9%) were infected with COVID-19; of these, 12 (31.6%) required hospitalization and two (5.2%) required admission to the intensive care unit (ICU). During the post-administration period, seven patients (7.5%) developed COVID-19; of these patients, four (57%) received tixagevimab/cilgavimab, and three (43%) did not. None of the patients required hospitalization or ICU admission. Conclusion: The incidence of COVID-19 was similar across study groups. However, the severity of the infection appeared to be milder in patients who received tixagevimab/cilgavimab. VL - 11 IS - 1 ER -
Multiorgan Transplant Center, King Abdullah Medical City, Makkah, Saudi Arabia
Multiorgan Transplant Center, King Abdullah Medical City, Makkah, Saudi Arabia
Pharmacy, Umm Alquraa University, Makkah, KSA
Multiorgan Transplant Center, King Abdullah Medical City, Makkah, Saudi Arabia
Multiorgan Transplant Center, King Abdullah Medical City, Makkah, Saudi Arabia
Multiorgan Transplant Center, King Abdullah Medical City, Makkah, Saudi Arabia
Information