The UK remains one of the countries with the lowest breastfeeding rates in the world despite the well-recognised benefits of breastfeeding. The National Health Service (NHS) provides guidance on how breastfeeding mothers should be supported in the workplace. However, the implementation of the guidance is not consistent across the sector, hence impacting on mothers’ ability to initiate or sustain breastfeeding. This study draws on data collected from 983 survey responses targeted at mothers working in the health sector. The study found that health sector employees are not well supported to breastfeed upon return to work. Only 36.3% of the participants (n=983) reported their workplace had a breastfeeding policy. Participants cited breastfeeding as a reason for staying longer on maternity leave because of lack of workplace support. This also affected mothers’ ability to benefit from shared parental leave, as it would require the mother to return to work early. This study highlights the barriers mothers in the health sector face with breastfeeding upon return to work while expected to continue fulfilling their duties, which includes promoting and supporting breastfeeding to other mothers and patients. The findings of this study expose the urgent need for the UK health sector to review its workplace policy to implement the guidance provided by the NHS to support breastfeeding employees returning to work. More broadly, the study exposes the extent of breastfeeding challenges in the UK and the need for a legislative reform to include breastfeeding in the national family friendly rights which will obligate employers to provide resources to support breastfeeding mothers in the workplace.
| Published in | International Journal of Law and Society (Volume 8, Issue 1) |
| DOI | 10.11648/j.ijls.20250801.14 |
| Page(s) | 25-36 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Breastfeeding, Infant Feeding, Breastfeeding Promotion, Equality
Factor | N | Correlation | 95% CI | P-value |
|---|---|---|---|---|
Breastfeeding policy | 793 | 0.088 | (0.018, 0.156) | 0.013 |
Supervisor discussion about breastfeeding upon pregnancy announcement | 793 | 0.105 | (0.036, 0.174) | 0.003 |
Supervisory discussion about breastfeeding upon returning to work after pregnancy leave | 791 | 0.098 | (0.028, 0.166) | 0.006 |
Feeling supported to breastfeed in the workplace | 792 | -0.115 | (-0.184, -0.046) | 0.001 |
Being able to express milk at work | 793 | 0.154 | (0.086, 0.222) | 0.000 |
Return time to work | 786 | 0.085 | (0.015, 0.154) | 0.017 |
Factor | N | Correlation | 95% CI | P-value |
|---|---|---|---|---|
Offering shared parental leave | 888 | 0.530 | (0.481, 0.576) | 0.000 |
Offering enhanced shared parental leave | 891 | 0.541 | (0.493, 0.586) | 0.000 |
Being able to breastfeed for as long as planned | 721 | 0.092 | (0.019, 0.164) | 0.013 |
Having a workplace breastfeeding policy | 888 | 0.376 | (0.318, 0.431) | 0.000 |
Supervisor discussion about breastfeeding upon pregnancy announcement | 886 | 0.393 | (0.336, 0.447) | 0.000 |
Supervisory discussion about breastfeeding upon returning to work after pregnancy leave | 884 | 0.401 | (0.344, 0.455) | 0.000 |
Having breastfeeding signage around workplace | 888 | 0.295 | (0.233, 0.354) | 0.000 |
Feeling supported to breastfeed in the workplace | 886 | -0.341 | (-0.398, -0.282) | 0.000 |
Return time to work | 885 | -0.110 | (-0.174, -0.044) | 0.001 |
Being able to express milk at work | 884 | 0.233 | (0.170, 0.294) | 0.000 |
GP | General Practitioner |
NHS | National Health Service |
SPL | Shared Parental Leave |
UK | United Kingdom |
UNICEF | United Nations International Children’s Fund |
WHO | World Health Organisation |
| [1] | Akre, J. (2989) “Infant feeding: the physiological basis.” Bull. World Health Orga. 67 (Suppl.), 1–107. |
| [2] | Schanler, R. (Guest ed). Preface. The Pediatric Clinics of North America. 2001, 48(1), xix–xx. |
| [3] | Riordan, J. Breastfeeding and human lactation. Jones and Bartlett Publishers Sudbury, 2005. |
| [4] | Lawrence, R. A.; Lawrence, R. M. Breastfeeding: a guide for the medical profession. 6th Edition. London, Mosby, 2005. |
| [5] | World Health Organisation (WHO). Infant and Young Child Feeding: Model Chapter for Textbooks for Medical Students and Allied Health Professionals. Geneva: World Health Organization. SESSION 2, The physiological basis of breastfeeding, 2009. |
| [6] | Di Filippo, P.; Lizzi, M.; Raso, M.; Di Pillo, S.; Chiarelli, F.; Attanasi, M. (2022) “The Role of Breastfeeding on Respiratory Outcomes Later in Childhood.” Front. Pediatr., 10, 829414. |
| [7] | Lamberti, L. M.; Zakarija-Grković, I.; Fischer Walker, C. L.; Theodoratou, E.; Nair, H.; Campbell, H.; Black, R. E. (2013) “Breastfeeding for reducing the risk of pneumonia morbidity and mortality in children under two: A systematic literature review and meta-analysis.” BMC Pub. Health, 13 (Suppl. S3), S18. |
| [8] | Isaacs, E. B.; Fischl, B. R.; Quinn, B. T.; Chong, W. K.; Gadian, D. G.; Lucas, A. (2010) “Impact of breast milk on intelligence quotient, brain size, and white matter development.” Pediatr. Res., 67(4), 357-362. |
| [9] | Eidelman, A. I.; Schanler, R. J.; Johnston, M.; Landers, S.; Noble, L.; Szucs, K.; Viehmann, L. (2012) “Breast-feeding and the use of human milk.” Pediatrics, 129(3), e827-e841. |
| [10] | Horta, B. L.; Loret de Mola, C.; Victora, C. G. (2015) “Breastfeeding and intelligence: a systematic review and meta‐analysis.” Acta Paediatr., 104,14-19. |
| [11] | Victora, C. G.; Horta, B. L.; de Mola, C. L.; Quevedo, L.; Pinheiro, R. T.; Gigante, D. P.; Gonçalves, H.; Barros, F. C. (2015) “Association between Breastfeeding and Intelligence, Educational Attainment, and Income at 30 Years of Age: A Prospective Birth Cohort Study from Brazil.” Lancet Glob. Health, 3, e199–e205. |
| [12] | Khan, J.; Vesel, L.; Bahl, R.; Martines, J. C. (2015) “Timing of breastfeeding initiation and exclusivity of breastfeeding during the first month of life: Effects on neonatal mortality and morbidity—A systematic review and meta-analysis.” Matern. Child Health J., 19, 468–479. |
| [13] | Moore, R. E.; Xu, L. L.; Townsend, S. D. (2021) “Prospecting Human Milk Oligosaccharides as a Defense Against Viral Infections.” ACS Infect. Dis., 7, 254–263. |
| [14] | Xiao, L.; van’t Land, B.; Engen, P. A.; Naqib, A.; Green, S. J.; Nato, A.; Leusink-Muis, T.; Garssen, J.; Keshavarzian, A.; Stahl, B.; et al. (2018) “Human Milk Oligosaccharides Protect against the Development of Autoimmune Diabetes in NOD-Mice.” Sci. Rep., 8, 3829. |
| [15] | Gopalakrishna, K. P.; Hand, T. W. (2020) “Influence of Maternal Milk on the Neonatal Intestinal Microbiome.” Nutrients, 12, 823. |
| [16] | Dai, D. L. Y.; Petersen, C.; Hoskinson, C.; Del Bel, K. L.; Becker, A. B.; Moraes, T. J.; … Turvey, S. E. (2023) “Breastfeeding Enrichment of B. longum subsp. infantis mitigates the effect of antibiotics on the microbiota and childhood asthma risk.” Med., 4, 92–112. e5. |
| [17] | Berger, P. K.; Plows, J. F.; Jones, R. B.; Alderete, T. L.; Yonemitsu, C.; Poulsen, M.; Ryoo, J. H.; Peterson, B. S.; Bode, L.; Goran, M. I. (2020) “Human Milk Oligosaccharide 2′-Fucosyllactose Links Feedings at 1 Month to Cognitive Development at 24 Months in Infants of Normal and Overweight Mothers.” PLoS ONE, 15, e0228323. |
| [18] | Boutrid, N.; Rahmoune, H.; Bioud, B.; Abdelmalek, D.; Amrane, M. (2022) “Breastfeeding Impact on Kidney Functions: A Systematic Review.” Am. Heart J., 254, 258. |
| [19] | Tsanidou, E.; Gougoula, V.; Tselebonis, A.; Kontogiorgis, C.; Constantinidis, T. C.; Nena, E. (2019) “Socio-Demographic Factors Affecting Initiation and Duration of Breastfeeding in a Culturally Diverse Area of North Eastern Greece.” Folia Med., 61, 566–571. |
| [20] | Al Sabati, S. Y.; Mousa, O. (2019) “Effect of early initiation of breastfeeding on the uterine consistency and the amount of vaginal blood loss during early postpartum period.” Nurs. Prim. Care, 3(3), 2-7. |
| [21] | Stordal, B. (2023) “Breastfeeding reduces the risk of breast cancer: A call for action in high-income countries with low rates of breastfeeding.” Cancer Med., 12(4), 4616-4625. |
| [22] | Muro-Valdez, J. C.; Meza-Rios, A.; Aguilar-Uscanga, B. R.; Lopez-Roa, R. I.; Medina-Díaz, E.; Franco-Torres, E. M.; Zepeda-Morales, A. S. M. (2023) “Breastfeeding-Related Health Benefits in Children and Mothers: Vital Organs Perspective.” Medicina, 59, 1535. |
| [23] | Maswime, S.; Buchmann, E. (2017) “A systematic review of maternal near miss and mortality due to postpartum hemorrhage.” Int J Gynaecol Obstet, 137(1), 1-7. |
| [24] | Sobhy, S. I.; Mohame, N. A. (2004) “The effect of early initiation of breast feeding on the amount of vaginal blood loss during the fourth stage of labor.” J. Egypt. Public Health Assoc., 79(1-2), 1-12. |
| [25] |
World Health Organization (WHO), 2023. Infant and young child feeding. [online] Available at:
https://www.who.int/news-room/fact-sheets/detail/infant-and-young-child-feeding [Accessed 22 November 2024]. |
| [26] | Munday, D. (2008) “Back to work: breastfeeding: it is imperative that mothers returning to work after childbirth are able to continue to breastfeed their infant if they choose to do so. In recognition of this, the NHS and all other employers throughout the UK have a legal obligation to support employees who want to continue to breastfeed.” Community Practitioner., 81(5), 40-42. |
| [27] | Simmons V. (2002) “Exploring inconsistent breastfeeding advice”. British Journal of Midwifery, 10(5), 297-301. |
| [28] | Wallenborn, J. T.; Perera, R. A.; Wheeler, D. C.; Lu, J.; Masho, S. W. (2019) “Workplace support and breastfeeding duration: The mediating effect of breastfeeding intention and self-efficacy.” Birth, 46(1), 121-128. |
| [29] | Gheyoh Ndzi, E. (2023) “Shared Parental Leave: A Key Barrier to Breastfeeding in the UK.” Int. J. Law Soc., 6(1), 62-69. |
| [30] | Glass, J. L.; Noonan, M. C. (2016) “Telecommuting and earnings trajectories among American women and men 1989–2008.” Soc. Forces, 95(1), 217-250. |
| [31] | Keevash, J.; Norman, A.; Forrest, H.; Mortimer, S. (2018) “What influences women to stop or continue breastfeeding? A thematic analysis.” Br. J. Midwifery, 26(10), 651-658. |
| [32] | Ogbuanu, C.; Glover, S.; Probst, J.; Liu, J.; Hussey, J. (2011) “The effect of maternity leave length and time of return to work on breastfeeding.” Pediatrics, 127(6), e1414-e1427. |
| [33] | Pounds, L.; Fisher, C. M.; Barnes-Josiah, D.; Coleman, J. D.; Lefebvre, R. C. (2017) “The role of early maternal support in balancing full-time work and infant exclusive breastfeeding: A qualitative study.” Breastfeed. Med., 12(1), 33-38. |
| [34] | Gheyoh Ndzi, E.; Raj Westwood, A. (2021) “The un-acknowledged relationship between shared parental leave, breastfeeding and workplace support in UK Universities.” Int. J. Bus. Soc. Sci. Res., 1-7. |
| [35] | Snyder, K.; Hansen, K.; Brown, S.; Portratz, A.; White, K.; Dinkel, D. (2018) “Workplace breastfeeding support varies by employment type: the service workplace disadvantage.” Breastfeed. Med., 13(1), 23-27. |
| [36] | Sayres, S.; Visentin, L. (2018) “Breastfeeding: uncovering barriers and offering solutions.” Current Opinion in Pediatrics, 30(4), 591-596. |
| [37] | Vilar-Compte, M.; Hernández-Cordero, S.; Ancira-Moreno, M.; Burrola-Méndez, S.; Ferre-Eguiluz, I.; Omaña, I.; Pérez Navarro, C. (2021) “Breastfeeding at the workplace: a systematic review of interventions to improve workplace environments to facilitate breastfeeding among working women.” Int. J. Equity Health, 20(1), 110. |
| [38] | Schmied, V.; Lupton, D. (2011) “Blurring the boundaries: breastfeeding and maternal subjectivity.” Sociol. Health Illn., 23, 234–250. |
| [39] | Dodgson, J. E.; Chee, Y. O.; Yap, T. S. (2004) “Workplace breastfeeding support for hospital employees.” J. Adv. Nurs., 47(1), 91-100. |
| [40] | Rollins, N. C.; Bhandari, N.; Hajeebhoy, N.; Horton, S.; Lutter, C. K.; Martines, J. C.;... Group, T. L. B. S. (2016) “Why invest, and what it will take to improve breastfeeding practices?” Lancet, 387(10017), 491-504. |
| [41] | Scott, V. C.; Taylor, Y. J.; Basquin, C.; Venkitsubramanian, K. (2019) “Impact of key workplace breastfeeding support characteristics on job satisfaction, breastfeeding duration, and exclusive breastfeeding among health care employees.” Breastfeed. Med., 14(6), 416-423. |
| [42] | Anderson, J.; Kuehl, R. A.; Drury, S. A. M.; Tschetter, L.; Schwaegerl, M.; Hildreth, M.; ... Lamp, J. (2015) “Policies aren’t enough: The importance of interpersonal communication about workplace breastfeeding support.” J. Hum. Lact., 31(2), 260-266. |
| [43] | Burks, K. M. R. (2015) “Mothers' perceptions of workplace breastfeeding support.” The University of Vermont and State Agricultural College. |
| [44] | Chang, Y.-S.; Harger, L.; Beake, S.; Bick, D. (2021) “Women's and Employers’ Experiences and Views of Combining Breastfeeding with a Return to Paid Employment: A Systematic Review of Qualitative Studies.” J. Midwifery Womens Health, 66, 641-655. |
| [45] | Hauck, Y. L.; Bradfield, Z.; Kuliukas, L. (2021) “Women’s experiences with breastfeeding in public: An integrative review.” Women Birth, 34(3), e217-e227. |
| [46] | Kendall, S.; Merritt, R.; Eida, T.; Pérez-Escamilla, R. (2021) “Becoming breastfeeding friendly in Great Britain- Does implementation science work?” Maternal Child Nutr., 19, e13393. |
| [47] | Marks, D.; O'Connor, R. (2015) “Health professionals’ attitudes towards the promotion of breastfeeding.” Br. J. Midwifery, 23(1), 50-58. |
| [48] | Hussainy, S. Y.; Dermele, N. (2011) “Knowledge, attitudes and practices of health professionals and women towards medication use in breastfeeding: A review.” Int. Breastfeed. J., 6(1), 1-16. |
| [49] | Dodgson, J. E.; Bloomfield, M.; Choi, M. (2014) “Are health science students' beliefs about infant nutrition evidence-based?” Nurs. Educ. Today, 34(1), 92-99. |
| [50] | Smith, J.; Javanparast, S.; Craig, L. (2017) “Bringing babies and breasts into workplaces: Support for breastfeeding mothers in workplaces and childcare services at the Australian National University.” Breastfeed. Rev., 25(1), 45-57. |
| [51] | Hearfield, H.; Collier, J.; Paize, F. (2022) “Breast Feeding Experiences of NHS Staff Returning to Work From Maternity Leave: A National Study.” BJPsych Open, 8(Suppl 1), S53–4. |
| [52] | Dagher, R. K.; McGovern, P. M.; Schold, J. D.; Randall, X. J. (2016) “Determinants of breastfeeding initiation and cessation among employed mothers: a prospective cohort study.” BMC Pregn. Childbirth, 16(1), 194. |
| [53] | Kosmala-Anderson, J.; Wallace, L. M. (2006) “Breastfeeding works: the role of employers in supporting women who wish to breastfeed and work in four organizations in England.” J. Pub. Health, 3, 183–191. |
| [54] | Peer, E., Brandimarte, L., Samat, S., Acquisti, A. (2017) “Beyond the turk: alternative platforms for crowdsourcing behavioral research.” J. Exp. Soc. Psychol., 153-163. |
| [55] | R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. |
| [56] | Morrison AH, Gentry R, Anderson J. (2019) “Mothers' reasons for early breastfeeding cessation.” The American Journal of Maternal/Child Nursing, 44(6), 325-30. |
| [57] | Brahm, P.; Valdes, V. (2017) “Benefits of breastfeeding and risks associated with not breastfeeding.” Rev. Chil. Pediatr., 88(1), 15-21. |
| [58] | Brugaillères, P.; Deguen, S.; Lioret, S.; Haidar, S.; Delamaire, C.; Counil, E.; Vandentorren, S. (2024) “Maternal employment characteristics as a structural social determinant of breastfeeding after return to work in the European Region: a scoping review.” Int. Breastfeed J., 19(1), 38. |
| [59] | Thomas, C. L.; Murphy, L. D.; Mills, M. J.; Zhang, J.; Fisher, G. G.; Clancy, R. L. (2022) “Employee lactation: A review and recommendations for research, practice, and policy.” Human Resour. Manag. Rev., 32(3), 100848. |
| [60] | Islam, M. J.; Broidy, L.; Baird, K.; Rahman, M.; Zobair, K. M. (2021) “Early exclusive breastfeeding cessation and postpartum depression: Assessing the mediating and moderating role of maternal stress and social support.” PLoS One, 16(5), e0251419. |
| [61] | Yuen, M.; Hall, O. J.; Masters, G. A.; Nephew, B. C.; Carr, C.; Leung, K.; Griffen, A.; McIntyre, L.; Byatt, N.; Moore Simas, T. A. (2022) “The Effects of Breastfeeding on Maternal Mental Health: A Systematic Review.” J. Womens Health, 31(6), 787–807. |
| [62] | Spitzmueller, C.; Wang, Z.; Zhang, J.; Thomas, C. L.; Fisher, G. G.; Matthews, R. A.; Strathearn, L. (2016) “Got milk? Workplace factors related to breastfeeding among working mothers.” J. Organ. Behav, 37(5), 692-718. |
| [63] | Burns, E.; Triandafilidis, Z. (2019) “Taking the path of least resistance: a qualitative analysis of return to work or study while breastfeeding.” Int. Breastfeeding J., 14, 1-13. |
| [64] | Cipollone, A.; Patacchini, E.; Vallanti, G. (2014) “Female labour market participation in Europe: novel evidence on trends and shaping factors”. IZA J. Eur. Labor Stud., 3, 1-40. |
| [65] | Cislaghi, B.; Heise, L. (2020) “Gender norms and social norms: differences, similarities and why they matter in prevention science.” Sociol. Health Illn, 42(2), 407-422. |
| [66] | Cavapozzi, D.; Francesconi, M.; Nicoletti, C. (2021) “The impact of gender role norms on mothers’ labor supply.” J. Econ. Behav. Organ, 186, 113-134. |
| [67] | Trice, H. M.; Beyer, J. M. The cultures of work organizations. Prentice-Hall, Inc., 1993. |
| [68] | Acker, J. (2012) “Gendered organizations and intersectionality: Problems and possibilities.” Equality, Divers. Inclusion, 31(3), 214-224. |
APA Style
Ndzi, E. G., Hinchcliffe, D., Neilson, D. (2025). The Impact of Legal Policies and Workplace Culture on Breastfeeding in the UK Health Sector. International Journal of Law and Society, 8(1), 25-36. https://doi.org/10.11648/j.ijls.20250801.14
ACS Style
Ndzi, E. G.; Hinchcliffe, D.; Neilson, D. The Impact of Legal Policies and Workplace Culture on Breastfeeding in the UK Health Sector. Int. J. Law Soc. 2025, 8(1), 25-36. doi: 10.11648/j.ijls.20250801.14
AMA Style
Ndzi EG, Hinchcliffe D, Neilson D. The Impact of Legal Policies and Workplace Culture on Breastfeeding in the UK Health Sector. Int J Law Soc. 2025;8(1):25-36. doi: 10.11648/j.ijls.20250801.14
@article{10.11648/j.ijls.20250801.14,
author = {Ernestine Gheyoh Ndzi and Danielle Hinchcliffe and Darcy Neilson},
title = {The Impact of Legal Policies and Workplace Culture on Breastfeeding in the UK Health Sector
},
journal = {International Journal of Law and Society},
volume = {8},
number = {1},
pages = {25-36},
doi = {10.11648/j.ijls.20250801.14},
url = {https://doi.org/10.11648/j.ijls.20250801.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijls.20250801.14},
abstract = {The UK remains one of the countries with the lowest breastfeeding rates in the world despite the well-recognised benefits of breastfeeding. The National Health Service (NHS) provides guidance on how breastfeeding mothers should be supported in the workplace. However, the implementation of the guidance is not consistent across the sector, hence impacting on mothers’ ability to initiate or sustain breastfeeding. This study draws on data collected from 983 survey responses targeted at mothers working in the health sector. The study found that health sector employees are not well supported to breastfeed upon return to work. Only 36.3% of the participants (n=983) reported their workplace had a breastfeeding policy. Participants cited breastfeeding as a reason for staying longer on maternity leave because of lack of workplace support. This also affected mothers’ ability to benefit from shared parental leave, as it would require the mother to return to work early. This study highlights the barriers mothers in the health sector face with breastfeeding upon return to work while expected to continue fulfilling their duties, which includes promoting and supporting breastfeeding to other mothers and patients. The findings of this study expose the urgent need for the UK health sector to review its workplace policy to implement the guidance provided by the NHS to support breastfeeding employees returning to work. More broadly, the study exposes the extent of breastfeeding challenges in the UK and the need for a legislative reform to include breastfeeding in the national family friendly rights which will obligate employers to provide resources to support breastfeeding mothers in the workplace.
},
year = {2025}
}
TY - JOUR T1 - The Impact of Legal Policies and Workplace Culture on Breastfeeding in the UK Health Sector AU - Ernestine Gheyoh Ndzi AU - Danielle Hinchcliffe AU - Darcy Neilson Y1 - 2025/01/24 PY - 2025 N1 - https://doi.org/10.11648/j.ijls.20250801.14 DO - 10.11648/j.ijls.20250801.14 T2 - International Journal of Law and Society JF - International Journal of Law and Society JO - International Journal of Law and Society SP - 25 EP - 36 PB - Science Publishing Group SN - 2640-1908 UR - https://doi.org/10.11648/j.ijls.20250801.14 AB - The UK remains one of the countries with the lowest breastfeeding rates in the world despite the well-recognised benefits of breastfeeding. The National Health Service (NHS) provides guidance on how breastfeeding mothers should be supported in the workplace. However, the implementation of the guidance is not consistent across the sector, hence impacting on mothers’ ability to initiate or sustain breastfeeding. This study draws on data collected from 983 survey responses targeted at mothers working in the health sector. The study found that health sector employees are not well supported to breastfeed upon return to work. Only 36.3% of the participants (n=983) reported their workplace had a breastfeeding policy. Participants cited breastfeeding as a reason for staying longer on maternity leave because of lack of workplace support. This also affected mothers’ ability to benefit from shared parental leave, as it would require the mother to return to work early. This study highlights the barriers mothers in the health sector face with breastfeeding upon return to work while expected to continue fulfilling their duties, which includes promoting and supporting breastfeeding to other mothers and patients. The findings of this study expose the urgent need for the UK health sector to review its workplace policy to implement the guidance provided by the NHS to support breastfeeding employees returning to work. More broadly, the study exposes the extent of breastfeeding challenges in the UK and the need for a legislative reform to include breastfeeding in the national family friendly rights which will obligate employers to provide resources to support breastfeeding mothers in the workplace. VL - 8 IS - 1 ER -
York Business School, York St John University, York, UK
School of Biological and Environmental Sciences, Liverpool John Moores University, Liverpool, UK
School of Education, Languages and Psychology, York St John University, York, UK
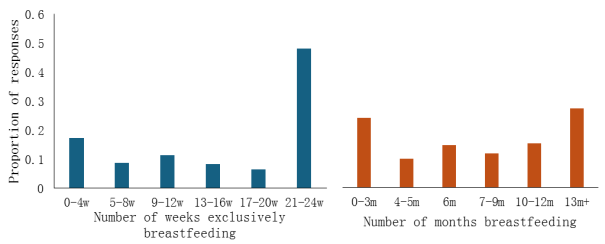
Figure 1. Proportion of survey responses showing number of weeks exclusively breastfeeding during leave and number of months breastfeeding (either exclusively or combined with other feeding methods) during leave.
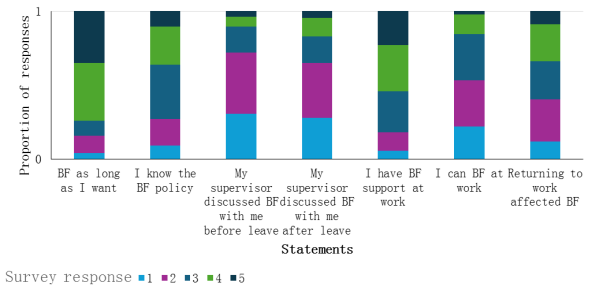
Figure 2. Proportion of survey responses scoring levels of agreement with several statements concerning breastfeeding, where 1 = strongly disagree and 5 = strongly agree.
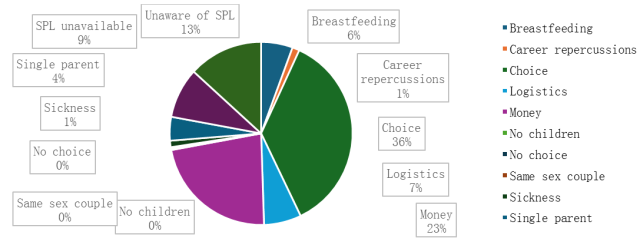
Figure 3. Reasons provided for decision-making with regards to parental leave.
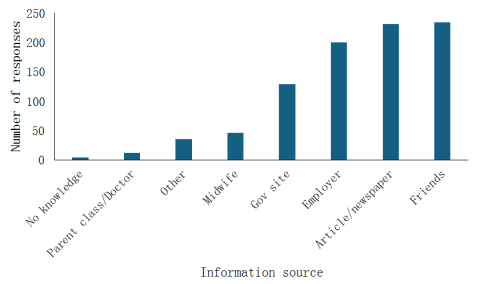
Figure 4. Information sources on shared parental leave, based on survey responses.
Information

