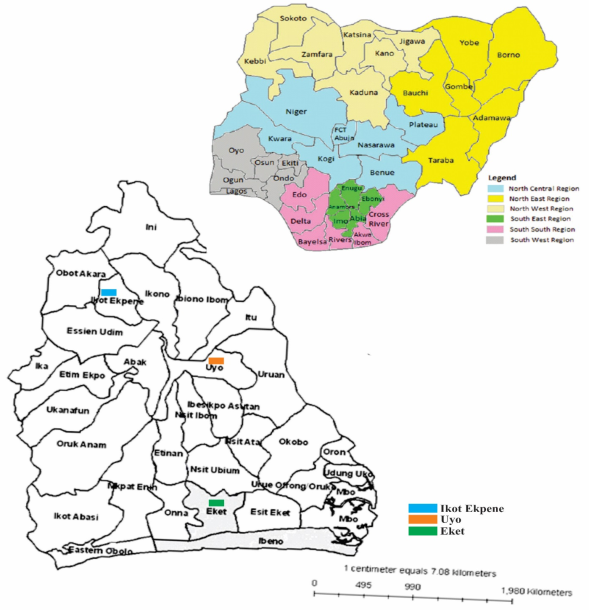
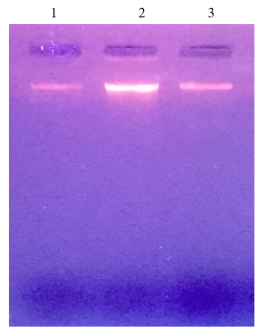
Sepsis is a life threatening medical emergency, Gram negative bacteria the principal causes of sepsis are seen in higher proportions among pediatrics populations and are mostly antibiotic resistance organisms. This study was carried out to determine antibiotic resistance of Gram negative bacteria, antibiotic resistance genes involve in sepsis among under five children in Akwa Ibom State, Nigeria. A hospital-based descriptive observational study of neonates with or without clinical features of sepsis. The subjects were children seen in General Hospital Ikot Ekpene, University Teaching Hospital Uyo and Immanuel Hospital Eket. A total of 180 children were sampled (60 from each hospital). A two milliliters (2 ml) sterile syringe with a 23gauge needle was used to collect blood sample aseptically from the vein of the arm of the child, inoculated on thioglycollate broth and subculture on MaConkey, blood and chocolate agar. Gram staining, biochemical characterization, antimicrobial susceptibility and resistance of Gram negative bacteria, their resistance genes were done. Of the 180 children, 123 tested positive for bacterial infections. Escherichia coli 25(13.9%), Proteus mirabilis 19(10.6%), Pseudomonas aeruginosa 15(8.3%), Klebsiella pneumoniae 12(6.7%), Serratia ficaria 9(5.0%), Rhizobium radiobacter 8(4.4%), Klebsiella oxytoca 7(3.9%), Chromobacterium violaceum 7(3.9%), Serratia marcescens 5(2.8%), Escherichia fergusonii 4(2.2%), Pseudomonas luteola 3(1.7%), Burkholderia cepacia 3(1.7%), Achromobacter xylosoxidans 3(1.7%), Burkholderia vietnamiensis 2(1.1%) and Serratia odorifera 1(0.6%). Pseudomonas aeruginosa was resistance to the 12 antibiotic used 12(100%), Three isolates were finally selected for molecular analysis, E. coli, P. aeruginosa, K. pneumoniae acquire blaSHV, PAGS, PASS, Cnf1 and hlyC genes, blaTEM amplify Pseudomonas and Klebsiella, FimH amplify only Klebsiella. Gram negative bacteria develop antibiotic resistance which poses a significant challenge in treating infections caused by this organism emphasizing the importance of responsible antibiotic use to mitigate further development of resistance.
| Published in | International Journal of Microbiology and Biotechnology (Volume 10, Issue 3) |
| DOI | 10.11648/j.ijmb.20251003.15 |
| Page(s) | 111-130 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Sepsis, Antibiotic, Resistance Genes, Gram Negative Bacteria, Children
Sample ID | DNA Concentration (ug/ul) | DNA Purity (260/280) |
|---|---|---|
A | 311 | 1.82 |
B | 395 | 1.89 |
C | 361 | 1.80 |
Target | Primer | Primer Sequence (5̗’- 3’) | Bases | Product Size (bp) | Ref. |
|---|---|---|---|---|---|
blaTEM | TEM-F | TCCGCTCATGAGACAATAACC | 21 | 890 | (Sturenburg et al., 2004) [23] . |
TEM-R | TTGGTCTGACAGTTACCAATGC | 22 | 890 | (Sturenburg et al., 2004) [23] . | |
bla SHV | SHV-F | TGGTTATGCGTTATATTCGCC | 21 | 868 | (Pai et al., 1999) [24] . |
SHV-R | GGTTAGCGTTGCCAGTGCT | 19 | 868 | (Pai et al., 1999) [24] . | |
blaCTX-M | CTX-F | TCTTCCAGAATAAGGAATCCC | 21 | 909 | (Sturenburg et al., 2004) [23] . |
CTX-R | CCGTTTCCGCTATTACAAAC | 20 | 909 | (Sturenburg et al., 2004) [23] . |
Gene Type | Primer | Primer Sequence | Bases Product Size (bp) | Ref. |
|---|---|---|---|---|
CARB KPC | CARB-F | 5’ATTCGCTAAACTCGAACAG-3’19 | 1069 | (Mlynarcik et al., 2016) [25] . |
CARB-R | 5’AAGAAAGCCCTTGAATGAG-3’19 | 1069 | (Mlynarcik et al., 2016) [25] . | |
VIM-1 | VIM-I-F | 5’GAGCTCTTCTATCCTGGTG-3’19 | 1069 | (Mlynarcik et al., 2016) [25] . |
VIM-1-R | 5’CTTGACAACTCATGAACGG-3’19 | 1069 | (Mlynarciket al., 2016) [25] . |
Primer | Primer Sequence (5̗’- 3’) | Bases | Product Size (bp) | Ref. |
|---|---|---|---|---|
PAGS-F | GGGGGATCTTCGGACCTCA | 19 | 910 | (Spilker et al., 2004) [26] . |
PAGS-R | TCCTTAGAGTGCCCACCCG | 19 | 910 | (Spilker et al., 2004) [26] . |
PASS-F | GGGGGATCTTCGGACCTCA | 19 | 930 | (Spilker et al., 2004) [26] . |
PASS-R | TCCTTAGAGTGCCCACCCG | 19 | 910 | (Spilker et al., 2004) [26] . |
Virulence Gene | Primer Sequence (5’-3’) | Bases Product size (bp) | Ref. |
|---|---|---|---|
fimH | F: TGCAGAACGGATAAGCCGTGG | 21 470 | (Johnson and Stell, 2000) [27] . |
R: GCAGTCACCTGCCCTCCGGTA | 21 460 | (Johnson and Stell, 2000) [27] . | |
cnfI | F: AAGATGGAGTTTCCTATGCAGGAG | 24 498 | (Johnson and Stell, 2000) [27] . |
R: CATTCAGAGTCCTGCCCTCATTATT | 25 498 | (Johnson and Stell, 2000) [27] . | |
hlyC | F: AGGTTCTTGGGCATGTATCCT | 21 556 | (Bingen-Bidois et al., 2002) [28] . |
R: TTGCTTTGCAGACTGCAGTGT | 21 556 | (Bingen-Bidois et al., 2002) [28] . |
Gram negative bacteria | Nos. of tested bacteria (n), (n/N)% in (General Hospital) | Nos. of tested bacteria (n), (n/N)% in (Teaching Hospital) | Nos. of tested bacteria (n), (n/N)% in (Immanuel Hospital) | Total nos. of tested bacteria (n), (n/N)% |
|---|---|---|---|---|
Escherichia coli | 8 (13.3) | 3 (5.0) | 14 (23.3) | 25 (13.9) |
Proteus mirabilis | 5 (8.3) | 8 (13.3) | 6 (10.0) | 19 (10.6) |
Pseudomonas aeruginosa | 6 (10.0) | 9 (15.0) | 0 (0) | 15 (8.3) |
K. pneumoniae | 4 (6.7) | 8 (13.3) | 0 (0) | 12 (6.7) |
S. ficaria | 3 (5.0) | 3 (5.0) | 3 (5.0) | 9 (5.0) |
Rhizobium radiobacter | 4 (6.7) | 1 (1.7) | 3 (5.0) | 8 (4.4) |
Klebsiella oxytoca | 1 (1.7) | 2 (3.3) | 4 (6.7) | 7 (3.9) |
Chromobacterium violaceum | 0 (0) | 5 (8.3) | 2 (3.3) | 7 (3.9) |
Serratia marcescens | 2 (3.3) | 2 (3.3) | 1 (1.7) | 5 (2.8) |
Escherichia fergusonii | 1 (1.7) | 0 (0) | 3 (5.0) | 4 (2.2) |
P. luteola | 1 (1.7) | 0 (0) | 2 (3.3) | 3 (1.7) |
Burkholderia cepacia | 1 (1.7) | 0 (0) | 2 (3.3) | 3 (1.7) |
Achromobacter xylosoxidans | 1 (1.7) | 1 (1.7) | 1 (1.7) | 3 (1.7) |
B. vietnamiensis | 1 (1.7) | 1 (1.7) | 0 (0) | 2 (1.1) |
S. odorifera | 1 (1.7) | 0 (0) | 0 (0) | 1 (0.6) |
Total | 39 (65.0) | 43 (71.7) | 41 (68.3) | 123 (68.3) |
Nos. of isolated Gram negative bacteria | AP | TET (%) | COT (%) | GEN (%) | CRX (%) | CHL (%) | CTR (%) | CTX (%) | CIP (%) | AMK (%) | VAN (%) | CPZ (%) | MEM (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
E. coli (25) | S | 13 (52.0) | 10 (40.0) | 22 (88.0) | 2 (8.0) | 21 (84.0) | 2 (8.0) | 0 | 11 (44.0) | 25 (100.0) | 11 (44.0) | 0 | 0 |
R | 10 (40.0) | 13 (52.0) | 3 (12.0) | 19 (76.0) | 0 | 13 (52.0) | 25 (100.0) | 10 (40.0) | 0 | 12 (48.0) | 25 (100.0) | 24 (96.0) | |
P. mirabilis (19) | S | 12 (63.2) | 11 (57.9) | 16 (84.2) | 1 (5.3) | 5 (26.3) | 3 (15.8) | 0 | 7 (36.8) | 19 (100.0) | 14 (73.7) | 0 | 1 (5.3) |
R | 5 (26.3) | 8 (42.1) | 2 (10.5) | 15 (78.9) | 6 (31.6) | 13 (68.4) | 18 (94.7) | 4 (21.1) | 0 | 3 (15.8) | 19 (100.0) | 18 (94.7) | |
P. aeruginosa (15) | S | 1 (6.7) | 0 | 5 (33.3) | 0 | 2 (13.3) | 0 | 0 | 5 (33.3) | 5 (33.3) | 6 (40.0) | 0 | 0 |
R | 13 (86.7) | 13 (86.7) | 10 (66.7) | 15 (100.0) | 13 (86.7) | 15 (100.0) | 15 (100.0) | 10 (66.7) | 10 (66.7) | 9 (60.0) | 15 (100.0) | 15 (100.0) | |
K. pneumonia (12) | S | 2 (16.7) | 4 (33.3) | 10 (83.3) | 0 | 11 (91.7) | 0 | 0 | 1 (8.3) | 12 (100.0) | 8 (66.7) | 0 | 0 |
R | 10 (83.3) | 8 (66.7) | 1 (8.3) | 11 (91.7) | 0 | 11 (91.7) | 12 (100.0) | 11 (91.7) | 0 | 4 (33.3) | 12 (100.0) | 12 (100.0) | |
S. ficaria (9) | S | 9 (100.0) | 8 (88.9) | 8 (88.9) | 4 (44.4) | 6 (66.7) | 0 | 0 | 8 (88.9) | 9 (100.0) | 9 (100.0) | 1 (11.1) | 0 |
R | 0 | 0 | 1 (11.1) | 3 (33.3) | 2 (22.2) | 8 (88.9) | 9 (100.0) | 1 (11.1) | 0 | 0 | 7 (77.8) | 9 (100.0) |
Nos. of isolated Gram negative bacteria | AP | TET (%) | COT (%) | GEN (%) | CRX (%) | CHL (%) | CTR (%) | CTX (%) | CIP (%) | AMK (%) | VAN (%) | CPZ (%) | MEM (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
R. radiobacter (8) | S | 3 (37.5) | 4 (50.0) | 8 (100.0) | 0 | 7 (87.5) | 0 | 0 | 8 (100.0) | 8 (100.0) | 3 (37.5) | 1 (11.1) | 0 |
R | 3 (37.5) | 3 (37.5) | 0 | 5 (62.5) | 1 (12.5) | 8 (100.0) | 8 (100.0) | 0 | 0 | 0 | 7 (77.8) | 9 (100.0) | |
K. oxytoca (7) | S | 0 | 1 (14.3) | 1 (14.3) | 0 | 7 (100.0) | 0 | 0 | 0 | 1 (14.3) | 6 (85.7) | 0 | 0 |
R | 7 (100.0) | 6 (85.7) | 6 (85.7) | 6 (85.7) | 0 | 7 (100.0) | 7 (100.0) | 7 (100.0) | 3 (42.9) | 1 (14.3) | 7 (100.0) | 7 (100.0) | |
C. violaceum (7) | S | 7 (100.0) | 3 (42.9) | 6 (85.7) | 0 | 4 (57.1) | 0 | 0 | 7 (100.0) | 7 (100.0) | 2 (28.6) | 0 | 0 |
R | 0 | 3 (42.9) | 1 (14.3) | 6 (85.7) | 1 (14.3) | 7 (100.0) | 7 (100.0) | 0 | 0 | 1 (14.3) | 7 (100.0) | 7 (100.0) | |
S. marcescens (5) | S | 4 (80.0) | 2 (40.0) | 5 (100.0) | 0 | 5 (100.0) | 0 | 0 | 4 (80.0) | 5 (100.0) | 4 (80.0) | 0 | 0 |
R | 0 | 3 (60.0) | 0 | 4 (80.0) | 0 | 4 (80.0) | 5 (100.0) | 0 | 0 | 1 (20.0) | 4 (80.0) | 5 (100.0) | |
E. fergusonii (4) | S | 4 (100.0) | 1 (25.0) | 4 (100.0) | 0 | 3 (75.0) | 0 | 0 | 3 (75.0) | 4 (100.0) | 3 (75.0) | 0 | 0 |
R | 0 | 1 (25.0) | 0 | 3 (75.0) | 0 | 3 (75.0) | 4 (1000) | 0 | 0 | 1 (25.0) | 4 (100.0) | 3 (75.0) |
Nos. of isolated Gram negative bacteria | AP | TET (%) | COT (%) | GEN (%) | CRX (%) | CHL (%) | CTR (%) | CTX (%) | CIP (%) | AMK (%) | VAN (%) | CPZ (%) | MEM (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
P. luteola (3) | S | 3 (100.0) | 1 (33.3) | 3 (100.0) | 0 | 3 (100.0) | 0 | 0 | 2 (66.7) | 3 (100.0) | 3 (100.0) | 0 | 0 |
R | 0 | 1 (33.3) | 0 | 3 (100.0) | 0 | 3 (100.0) | 3 (100.0) | 1 (33.3) | 0 | 0 | 2 (66.7) | 3 (100.0) | |
B. cepacia (3) | S | 1 (33.3) | 0 | 2 (66.7) | 0 | 3 (100.0) | 1 (33.3) | 0 | 3 (100.0) | 3 (100.0) | 1 (33.3) | 0 | 0 |
R | 2 (66.7) | 2 (66.7) | 0 | 3 (100.0) | 0 | 2 (66.7) | 3 (100.0) | 0 | 0 | 1 (33.3) | 3 (100.0) | 3 (100.0) | |
A. xylosoxidans (3) | S | 0 | 1 (33.3) | 0 | 0 | 3 (100.0) | 0 | 0 | 3 (100.0) | 3 (100.0) | 0 | 0 | 0 |
R | 3 (100.0) | 1 (33.3) | 2 (66.7) | 3 (100.0) | 0 | 3 (100.0) | 3 (100.0) | 0 | 0 | 2 (66.7) | 3 (100.0) | 3 (100.0) | |
B. vietnamiensis (2) | S | 0 | 0 | 1 (50.0) | 0 | 1 (50.0) | 0 | 0 | 1 (50.0) | 2 (100.0) | 0 | 0 | 0 |
R | 2 (100.0) | 2 (100.0) | 0 | 2 (100.0) | 0 | 2 (100.0) | 2 (100.0) | 0 | 0 | 1 (50.0) | 2 (100.0) | 2 (100.0) | |
S. odorifera (1) | S | 1 (100.0) | 0 | 1 (100.0) | 0 | 1 (100.0) | 0 | 0 | 1 (100.0) | 1 (100.0) | 1 (100.0) | 0 | 0 |
R | 0 | 1 (100.0) | 0 | 1 (100.0) | 0 | 1 (100.0) | 1 (100.0) | 0 | 0 | 0 | 1 (100.0) | 1 (100.0) |
Gram negative bacteria | Nos. of isolated Gram negative bacteria | Nos. of resistance antibiotic (X) | MARI = X/Y (%) | Antibiotic resistance pattern (ARP) | Antibiotic resistance class (ARC) |
|---|---|---|---|---|---|
Escherichia coli | 2 | 9 | 9/12 = 0.75 = 75 | CRX, CTR, CTX, TET, CIP, COT, VAN, GEN, MEM | Ceph, tetra, fluoro, sulf, glyco, aminogly, carb |
2 | 8 | 8/12 = 0.7 = 70 | CRX, CTX, CPZ, TET, COT, CIP, AMK, MEM | Ceph, sulf, tetra, fluoro, aminogly, carb | |
6 | 7 | 7/12 = 0.6 = 60 | CRX, CTR, CTX, CPZ, COT, CIP, MEM | Ceph, sulf, fluoro, carb | |
5 | 6 | 6/12 = 0.5 = 50 | CRX, CTX, CPZ, TET, VAN, MEM | Ceph, tetra, glyco, carb | |
8 | 5 | 5/12 = 0.4 = 40 | CRX, CTR, CTX, CPZ, MEM | Ceph, carb | |
2 | 4 | 4/12 = 0.3 = 30 | CTR, CTX, CPZ, MEM | Ceph, carb | |
25 | |||||
Proteus mirabilis | 2 | 8 | 8/12 = 0.7 = 70 | CRX, CTR, CTX, CPZ, CIP, COT, CHL, MEM | Ceph, fluoro, sulf, chlo, carb |
11 | 6 | 6/12 = 0.5 = 50 | CTX, CPZ, TET, COT, VAN, MEM | Ceph, tetra, sulf, glyco, carb | |
5 | 5 | 5/12 = 0.4 = 40 | CRX, CTX, CPZ, CHL, MEM | Ceph, chlo, carb | |
1 | 4 | 4/12 = 0.3 = 30 | CRX, CTX, CPZ, MEM | Ceph, carb | |
19 | |||||
Pseudomonas aeruginosa | 9 | 12 | 12/12 = 1 = 100 | CRX, CTR, CTX, CPZ, CIP, TET, COT, CHL, VAN, GEN, AMK, MEM | Ceph, fluoro, tetra, sulf, chlo, glyco, aminogly, carb |
1 | 11 | 11/12 = 0.9 = 90 | CRX, CTR, CTX, CPZ, CIP, TET, COT, CHL, GEN, AMK, MEM | Ceph, fluoro, tetra, sulf, chlo, aminogly, carb | |
2 | 8 | 8/12 = 0.7 = 70 | CRX, CTR, CTX, CPZ, TET, COT, CHL, MEM | Ceph, tetra, sulf, chlo, carb | |
1 | 7 | 7/12 = 0.6 = 60 | CRX, CTR, CTX, CPZ, TET, COT, MEM | Ceph, tetra, sulf, carb | |
1 | 6 | 6/12 = 0.5 = 50 | CRX, CTR, CTX, CPZ, CHL, MEM | Ceph, chlo, carb | |
1 | 5 | 5/12 = 0.4 = 40 | CRX, CTR, CTX, CPZ, MEM | Ceph, carb | |
15 |
Gram negative bacteria | Nos. of isolated Gram negative bacteria | Nos. of resistance antibiotic (X) | MARI = X/Y (%) | Antibiotic resistance pattern (ARP) | Antibiotic resistance class (ARC) |
|---|---|---|---|---|---|
Klebsiella pneumoniae | 1 | 10 | 10/12 = 0.8 = 80 | CRX, CTR, CTX, CPZ, CIP, COT, TET, VAN, AMK, MEM | Ceph, fluoro, sulf, tetra, glyco, aminogly, carb |
4 | 9 | 9/12 = 0.75 = 75 | CRX, CTR, CTX, CPZ, TET, COT, CIP, VAN, MEM | Ceph, tetra, sulf, fluoro, glyco, carb | |
1 | 8 | 8/12 = 0.7 = 70 | CRX, CTR, CTX, CPZ, TET, COT, CIP, MEM | Ceph, tetra, sulf, fluoro, carb | |
4 | 7 | 7/12 = 0.6 = 60 | CTR, CTX, CPZ, TET, COT, CIP, MEM | Ceph, tetra, sulf, fluoro, carb | |
1 | 6 | 6/12 = 0.5 = 50 | CRX, CTR, CTX, CPZ, CIP, MEM | Ceph, fluoro, carb | |
1 | 5 | 5/12 = 0.4 = 40 | CRX, CTR, CTX, CPZ, MEM | Ceph, carb | |
12 | |||||
Serratia ficaria | 2 | 6 | 6/12 = 0.5 = 50 | CTR, CTX, CPZ, CIP, GEN, MEM | Ceph, fluoro, aminogly, carb |
2 | 5 | 5/12 = 0.4 = 40 | CTR, CTX, CPZ, CHL, MEM | Ceph, chloro, carb | |
4 | 4 | 4/12 = 0.3 = 30 | CTR, CTX, CPZ, MEM | Ceph, carb | |
1 | 2 | 2/12 = 0.2 = 20 | CTX, MEM | Ceph, carb | |
9 | |||||
Rhizobium radiobacter | 2 | 7 | 7/12 = 0.6 = 60 | CRX, CTR, CTX, CPZ, TET, COT, MEM | Ceph, tetra, sulf, carb |
3 | 6 | 6/12 = 0.5 = 50 | CRX, CTR, CTX, CPZ, COT, MEM | Ceph, sulf, carb | |
1 | 5 | 5/12 = 0.4 = 40 | CRX, CTR, CTX, CPZ, MEM | Ceph, carb | |
2 | 3 | 3/12 = 0.3 = 30 | CTR, CTX, CHL | Ceph, chloro | |
8 |
Gram negative bacteria | Nos. of isolated Gram negative bacteria | Nos. of resistance antibiotic (X) | MARI = X/Y (%) | Antibiotic resistance pattern (ARP) | Antibiotic resistance class (ARC) |
|---|---|---|---|---|---|
Klebsiella oxytoca | 2 | 10 | 10/12 = 0.8 = 80 | CRX, CTR, CTX, CPZ, TET, CIP, COT, VAN, AMK, MEM | Ceph, tetra, fluoro, sulf, glyco, aminogly, carb |
4 | 9 | 9/12 = 0.75 = 75 | CRX, CTR, CTX, CPZ, TET, COT, CIP, GEN, MEM | Ceph, tetra, sulf, fluoro, aminogly, carb | |
1 | 8 | 8/12 = 0.7 = 70 | CTR, CTX, CPZ, TET, COT, CIP, GEN, MEM | Ceph, tetra, sulf, fluoro, aminogly, carb | |
7 | |||||
Chromo bacterium violaceum | 2 | 7 | 7/12 = 0.6 = 60 | CRX, CTR, CTX, CPZ, VAN, GEN, MEM | Ceph, glyco, aminogly, carb |
2 | 6 | 6/12 = 0.5 = 50 | CRX, CTR, CTX, CPZ, COT, MEM | Ceph, sulf, carb | |
2 | 5 | 5/12 = 0.4 = 40 | CRX, CTR, CTX, CPZ, MEM | Ceph, carb | |
1 | 4 | 4/12 = 0.3 = 30 | CTR, CTX, CPZ, MEM | Ceph, carb | |
7 | |||||
Serratia marcescens | 1 | 6 | 6/12 = 0.5 = 50 | CRX, CTR, CTX, CPZ, COT, MEM | Ceph, sulf, carb |
3 | 5 | 5/12 = 0.4 = 40 | CTR, CTX, CPZ, COT, MEM | Ceph, sulf, carb | |
1 | 4 | 4/12 = 0.3 = 30 | CRX, CTR, CTX, MEM | Ceph, carb | |
5 | |||||
Escherichia fergusonii | 1 | 6 | 6/12 = 0.5 = 50 | CRX, CTR, CTX, CPZ, VAN, MEM | Ceph, glyco, carb |
1 | 5 | 5/12 = 0.4 = 40 | CRX, CTR, CTX, CPZ, MEM | Ceph, carb | |
2 | 4 | 4/12 = 0.3 = 30 | CTR, CTX, CPZ, MEM | Ceph, carb | |
4 | |||||
Pseudomonas luteola | 1 | 6 | 6/12 = 0.5 = 50 | CRX, CTR, CTX, CPZ, CIP, MEM | Ceph, fluoro, carb |
2 | 5 | 5/12 = 0.4 = 40 | CRX, CTR, CTX, CPZ, MEM | Ceph, carb | |
3 |
Gram negative bacteria | Nos. of isolated Gram negative bacteria | Nos. of resistance antibiotic (X) | MARI = X/Y (%) | Antibiotic resistance pattern (ARP) | Antibiotic resistance class (ARC) |
|---|---|---|---|---|---|
Burkholderia cepacia | 2 | 7 | 7/12 = 0.6 = 60 | CRX, CTX, CPZ, TET, COT, VAN, MEM | Ceph, tetra, sulf, glyco, carb |
1 | 5 | 5/12 = 0.4 = 40 | CRX, CTR, CTX, CPZ, MEM | Ceph, carb | |
3 | |||||
Achromobacter xylosoxidans | 1 | 9 | 9/12 = 0.75 = 75 | CRX, CTR, CTX, CPZ, TET, COT, VAN, GEN, MEM | Ceph, tetra, sulf, glyco, aminogly, carb |
1 | 8 | 8/12 = 0.7 = 70 | CRX, CTR, CTX, CPZ, TET, GEN, VAN, MEM | Ceph, tetra, aminogly, glyco, carb | |
1 | 6 | 6/12 = 0.5 = 50 | CRX, CTR, CTX, CPZ, TET, MEM | Ceph, tetra, carb | |
3 | |||||
Burkholderia vietnamiensis | 1 | 8 | 8/12 = 0.7 = 70 | CRX, CTR, CTX, CPZ, TET, COT, VAN, MEM | Ceph, tetra, sulf, glycol, carb |
1 | 7 | 7/12 = 0.6 = 60 | CRX, CTR, CTX, CPZ, TET, COT, MEM | Ceph, tetra, sulf, carb | |
2 | |||||
Serratia odorifera | 1 | 6 | 6/12 = 0.5 = 50 | CTR, CTX, CRX, CPZ, COT, MEM | Ceph, sulf, carb |
1 | |||||
Total isolated bacteria | 123 |
Resistant gene | Present of resistant gene in Gram negative bacteria | Absent of resistant gene in Gram negative bacteria |
|---|---|---|
Bla TEM | Pseudomonas and Klebsiella | Escherichia coli |
Bla SHV | E. coli, Pseudomonas and Klebsiella | - |
Bla CTX-M | - | E. coli, Pseudomonas and Klebsiella |
CARB KPC | - | E. coli, Pseudomonas and Klebsiella |
VIM-1 | - | E. coli, Pseudomonas and Klebsiella |
PASS | E. coli, Pseudomonas and Klebsiella | - |
PAGS | E. coli, Pseudomonas and Klebsiella | - |
FimH | Klebsiella | E. coli, Pseudomonas |
Cnf1 | E. coli, Pseudomonas and Klebsiella | - |
HlyC | E. coli, Pseudomonas and Klebsiella | - |
TEM | Temoniera |
SHV | Sulf-hydryl |
PAGs | Pseudomonas Aeruginosa Genes |
PASS | Pseudomonas Aeruginosa Subspecie |
Cnf1 | Citotoxic Necrotizing Factor 1 |
hlyc | haemolysin |
Fim H | Type1 Fimbrae |
CDC | Center for Disease and Control |
MDR | Multidrug Resistance |
MAR | Multiple Antibiotics Resistance |
CTX-M | Cifotàximase Munich |
SSI | Surgical Site Infection |
VAP | Ventilator Associated Pneumonia |
CLABSI | Central Line Associated Blood Stream Infection |
MRSA | Methicillin Resistant Staphylococcus aureus |
WHO | World Health Organization |
LMICs | Low and Middle Income Countries |
NPC | National Population Commission |
CLSI | Clinical Laboratory Standards Institute |
ARC | Antibiotic Resistant Class |
ARP | Antibiotic Resistant Pattern |
TET | Tetracycline |
CoT | Cotrimoxazole |
GEN | Gentamicin |
CRX | Cefuroxime |
CHL | Chloramphenicol |
CTR | Ceftriaxone |
CTX | Cefotaxime |
CIP | Ciprofloxacin |
AMK | Amikacin |
VAN | Vancomycin |
CPZ | Ceftazidime |
MEM | Meropenem |
DNA | Deoxyribonucleic Acid |
OD | Optical Density |
EDTA | Ethylinediamine-Tetraacetic Acid |
PCR | Polymerase Chain Reaction |
S | Susceptibility |
AP | Antibiotic Pattern |
R | Resistance |
ESBLS | Extended Spectrum Beta Lactamases |
| [1] | Basco, W. T. Jr. (2021). The febrile infant: new AAP guidance for the first 2 months of life. Medscape News and Perspective. July 19. Available at |
| [2] |
Centers for Disease Control and Prevention (2023). What is sepsis. CDC; Available at
https://www.cdc.gov/sepsis/index.html Accessed 19 January, 2023. |
| [3] | Rudd, K. E., Johnson, S. C., Agesa, K. M., Shackelford, K. A., Tsoi, D., Kievlan, D. R., Colombara, D. V., Ikuta, K. S., Kissoon, N., Finfer, S., Fleischmann-Struzer, C., Machado, F. R., Reinhart, K. K., Rowan, K., Seymour, C. W., Watson, R. S., West, T. E., Marinho, F., Hay, S. I., Lozano, R., Lopez, A. D., Augus, D. C., Murray, C. J. L. and Naghavi, M. (2020). Global, regional and national sepsis incidence and mortality: analysis for the global burden of disease study. Lancet 395(10219): 200-211. |
| [4] | Bonet, M., Souza, J. P., Abalos, E., Bukola, F. and Marian, K. (2018). The global maternal sepsis study and awareness campaign (GLOSS): study protocol. Reproductive Health 15: 1-16. |
| [5] | Olowo-Okere, A., Ibrahim Y. K. E., Nabti, L. Z. and Olayinka, B. O. (2020). High prevalence of multi-drug resistant Gram-negative bacterial infections in Northwest Nigeria. Germs 10(4): 310-321. |
| [6] | Tessema, B., Lippman, N., Knupfer, M., Sack, U. and Konig, B. (2021). Antibiotic resistance pattern of bacterial isolates from neonatal sepsis patients at university hospital of Leipzig, Germany. Multi-disciplinary Digital Publishing Institute 10(3): 323. |
| [7] | Breijyeh, Z., Jubeh, B. and Karaman, R. (2020). Resistance of Gram-negative bacteria to current antibacterial agents and approaches to resolve it. Molecules 25(1340): 1-23. |
| [8] | Carroll, M., Rangaihagari, A., Musabeyezu, E., Singer, D. and Ogbuagu, D. (2016). Five year antimicrobial susceptibility trends among bacterial isolates from a tertiary health-care facility in Kigali, Rwanda. American Journal of Tropical medicine Hygiene 95(6): 1277-1283. |
| [9] | Sisay, M., Worku, T. and Edessa, D. (2019). Microbial epidemiology and antimicrobial resistance patterns of wound infection in Ethiopia: a meta-analysis of laboratory based cross-sectional studies. Biomedicine Central Pharmacology Toxicology 20(35): 1-19. |
| [10] | Olorukooba, A. A., Ifusemu, W. R., Ibrahim, M. S., Jibril, M. B., Amadu, L. and Lawal, B. B. (2020). Prevalence and Factors Associated with Neonatal Sepsis in a Tertiary Hospital, North West Nigeria. Nigerian Medical Journal 61(2): 60-66. |
| [11] | Medugu, N., Iregbu, K. C. and Iron, T. P. (2018). Aetiology of neonatal sepsis in Nigeria and relevance groups B Streptococcus: a systematic review. Plos One 13(7): e0200350. |
| [12] | Onubogu, U. C. and West, B. M. (2022). Pattern and outcome of diseases among children presenting in the emergency room of a tertiary hospitals in Port Harcourt, Nigeria. Open Journal of Pediatrics 12(3): 538-553. |
| [13] |
World Health Organization (2022). Antimicrobial resistance: global report on surveillance. WHO; Available at
http://www.who.int/drugresistance/documents/surveillancereport/en/ |
| [14] | Ogbolu, D. O., Piddock L. J. V. and Webber, M. A. (2019). Opening pandora's box: high level resistance to antibiotics of last resort in Gram-negative bacteria from Nigeria. Journal of Global Antimicrobial Resistance 21: 211-217. |
| [15] | Owowo, E. E., Christopher, M. A., Okon, I. E., Antia, U. E. and Umoh, V. (2019). Prevalence of Helicobacter pylori infection among internally displaced persons from Bakassi peninsular and Etim Ekpo in South Southern, Nigeria. Journal of Biosciences and Medicines 7: 28-37. |
| [16] | Lawn, J. E., Bianchi-Jassir, F., Russell, N. J., Kohli-Lynch, M., Tann, C. J. and Hall, J. (2017). Group B streptococcal disease worldwide for pregnant women, stillbirths and children: why, what, and how to undertake estimates. Clinical Infectious Disease 65(2): S89-S99. |
| [17] | Folgori, L., Bielicki, J., Heath, P. and Sharland, M. (2017). Antimicrobial resistant Gram negative infections in neonates: burden of disease and challenges in treatment. Current Opinion on Infectious Disease 30: 281-288. |
| [18] | Lister, P. D., Wolter, D. J. and Hanson, N. D. (2009). Antibacterial resistant Pseudomonas aeruginosa: clinical impact and complex regulation of chromosomally encoded resistance mechanisms. Clinical Microbiology Reviews 22(4): 582-610. |
| [19] | Devi, U., Bora, R., Das, J. K. and Mahanta, J. (2018). Extended-spectrum β-lactamase and carbapenemase-producing Gram-negative bacilli in neonates from a tertiary care centre in Dibrugarh, Assam, India. Indian Journal of Medical Research 147(1): 110-114. |
| [20] |
Centre for Disease Control and Prevention (2019). Antibiotics resistance threats in the United States, Atlanta GA; United States department of health and human services. Available at
www.cdc.gov/DrugdResistance/Biggestthreats.Html * accessed 31 October 2022. |
| [21] | National Population Commission of Nigeria (NPC) (2011). The population projection: map showing the three senatorial districts in Akwa Ibom State. |
| [22] | Clinical and Laboratory Standard Institude (CLSI). (2020). Performance standards for antimicrobial susceptiblity testing, 28th edition. CLSI supplement M100. Wayne: Clinical and Laboratory Standard Institude 38: 102-122. |
| [23] | Sturenburg, E., Kuhn, A., Mack, D. and Laufs, R. (2004). A novel extended-spectrum beta- lactamase CTX-M-23 with a P167T substitution in the active-site omega loop associated with ceftazidime resistance. Journal of Antimicrobial Chemotherapy 54: 406-409. |
| [24] | Pai, H., Lysu, S., Lee, J., Kim, J., Kwon, Y., Kim, J. and Choe, K. (1999). Survey of extended- spectrum beta-lactamases in clinical isolates of Escherichia coli and Klebsiella pneumoniae: prevalence of TEM-52 in Korea. Journal of Clinical Microbiology 37: 1758-1763. |
| [25] | Mlynarcik, P., Roderova, M. and Kolar, M. (2016). Primer evaluation for PCR and its application for detection of carbapenemases in enterobacteriaceae. Jundishapur Journal of Microbiology 9(1): 29314. |
| [26] | Spilker, T., Coenye, T., Vandamme, P. and Lipuma, J. (2004). PCR-based assay for differentiation of Pseudomonas aeruginosa from other Pseudomonas species recovered from cystic fibrosis patients. Journal of Clinical Microbiology 42: 2074-2079. |
| [27] | Johnson, J. R. and Stell, A. L. (2000). Extended virulence genotype of Escherichia coli strains from patients with urosepsis in relation to phylogeny and host compromise. Journal of Infectious Disease 181(1): 261-272. |
| [28] | Bingen-Bidois, M., Clermont, O., Bonacorsi, S., Terki, M., Brahimi, N. and Loukil, C. (2002). Phylogenetic analysis and prevalence of urosepsis strains of Esherichia coli bearing pathogenicity island-like domains. Infectious Immunology 70(6): 3216-3226. |
| [29] | Klick, B. and Guins, T. (2021). Sepsis in the urgent care setting. Current Problems in Pediatric and Adolescent Health Care 51(2): 1-9. |
| [30] | Rasool, M. S., Siddiqui, F., Ajaz, M. and Rasool, S. A. (2019). Prevalence and antibiotic resistance profiles of Gram negative bacilli associated with urinary tract infections (UTIs) in Karachi, Pakistan. Pakistan Journal of Pharmaceutical Sciences 32(6): 2617-2623. |
| [31] | Miranda, S., Harahap, A., Husada, D. and Faramarisa, F. N. (2024). Microbial pattern of neonatal sepsis in the neonatal intensive care unit of Dr. Ramelan navy central hospital. International Journal of Pediatrics 2024: 1-8. |
| [32] | Getabelew, A., Aman, M., Fantaye, E. and Yeheyis, T. (2018). Prevalence of neonatal sepsis and associated factors among neonates in neonatal intensive care unit at selected governmental hospitals in Shashemene town, Oromia regional state, Ethiopia. International Journal of Pediatrics 2018: 1-7. |
| [33] | Godfrey, E., Majaliwa, E., Assenga, E. N. (2022). Aetiology, antimicrobial susceptibility and outcome of children with sepsis, admitted at Muhimbili national hospital, Dar es Salaam. Pan African Medical Journal 42(167): 1937-8688. |
| [34] | Habyarimana, T., Murenzi, D., Musoni, E., Yadufashije, C. and Niyonzima, F. N. (2021). Bacteriological profile and antimicrobial susceptibility patterns of bloodstream infection at Kigali university teaching hospital. Infection and Drug Resistance 14: 699- 707. |
| [35] | Almohammady, M. N., Eltahlawy, E. M. and Reda, N. M. (2020). Pattern of bacterial profle and antibiotic susceptibility among neonatal sepsis cases at Cairo university children hospital. Journal of Taibah University Medical Sciences 15(1): 39-47. |
| [36] | Adedokun, A. A., Onosakponome, E. O. and Nyenke, C. U. (2020). Early onset and late onset of neonatal sepsis in a tertiary hospital, South-South, Nigeria. Journal of Advances in Microbiology 20: 19-29. |
| [37] | Droz, N., Hsia, Y., Ellis, S., Dramowski, A., Sharland, M. and Basmaci, R. (2019). Bacterial pathogens and resistance causing community acquired paediatric bloodstream infections in low and middle-income countries: a systematic review and meta- analysis. Antimicrobial Resistance and Infection Control 8(1): 207. |
| [38] | Peterside, O., Pondei, K. and Akinbami, F. O. (2015). Bacteriological profile and antibiotic susceptibility pattern of neonatal sepsis at a teaching hospital in Bayelsa state. Nigeria Tropical Medicine Health 43(3): 183-190. |
| [39] | Shehab El-Din, E. M. R., El-Sokkary, M. M. A., Bassiouny, M. R. and Hassan, R. (2015). Epidemiology of neonatal sepsis and implicated pathogens: a study from Egypt. Biomedical Resource International 2015: 509484. |
| [40] | Joshi, S. J., Ghole, V. S. and Niphadkar, K. B. (2000). Neonatal Gram negative bacteraemia. India Journal of Pediatric 67(1): 27-32. |
| [41] | Aletayeb, S. M. H., Khosravi, A. D., Dehdashtian, M., Kompani, F., Mortazavi, S. M. and Aramesh, M. R. (2011). Identification of bacterial agents and antimicrobial susceptibility of neonatal sepsis: a 54-month study in a tertiary hospital. African Journal of Microbiology Research 5(5): 528-531. |
| [42] | Bansal, S., Jain, A., Agarwal, J. and Malik, G. K. (2004). Significance of coagulase negative staphylococci in neonates with late onset septicaemia. Indian Journal of Pathology and Microbiology 47(4): 586-568. |
| [43] | Agnihotri, N., Kaistha, N. and Gupta, V. (2004). Antimicrobial susceptibility of isolates from neonatal septicaemia. Japanese Journal of Infectious Disease 57(6): 273-275. |
| [44] | Raha, B. K., Baki, M. A., Begum, T., Nahar, N., Jahan, N. and Begum, M. (2014). Clinical, bacteriological profile and outcome of neonatal sepsis in a tertiary care hospital. Medicine Today 26(1): 18-21. |
| [45] | Lund, A. M., Christensen, E. and Skovby, F. (2002). Diagnosis and acute treatment of inborn metabolic diseases in infants. Ugeskrift for Laeger 164(48): 5613-5619. |
| [46] | Vinodkumar, C. S., Neelagund, Y. F., Suneeta, K., Sudha, B., Kalapannavar, N. K. and Basavarajapa, K. G. (2008). Perinatal risk factors and microbial profile of neonatal septicaemia: a multi-centred study. Journal of Obstetrics Gynecology of India 58(1): 32-40. |
| [47] | Giannoni, E., Agyeman, P. K. A., Stocker, M., Posfay-Barbe, K. M., Heininger, U., Spycher, B. D. and Schlapbach, L. J. (2018). Neonatal sepsis of early onset and hospital-acquired and community-acquired late onset: a prospective population-based cohort study. The Journal of Pediatrics 201: 106-114. |
| [48] | Laxman, B. and Roja, A. (2022). Achromobacter xylosoxidans causing late-onset sepsis with pneumonia in a term neonate. Indian Journal of Neonatal Medicine and Research 10(3): PC01-PC03. |
| [49] | Oyekale, O. T., Ojo, B. O., Olajide, A. T. and Oyekale, O. I. (2022). Bacteriological profile and antibiogram of blood culture isolates from bloodstream infections in a rural tertiary hospital in Nigeria. Africa Journal of Laboratory Medicine 11(1): 2225-2010. |
| [50] | Kebede, B., Yihunie, W., Abebe, D., Tegegne, B. A. and Belayneh, A. (2022). Gram negative bacteria isolates and their antibiotic resistance patterns among pediatrics patients in Ethiopia: a systematic review. Epidemiology of Infectious Diseases Systematic Review 10: 1-9. |
| [51] | Arowosegbe, A. O., Ojo, D. A., Dedeke, I. O., Shittu, O. B. and Akingbade, O. A. (2017). Neonatal sepsis in a Nigerian tertiary hospital: clinical features, clinical outcome, aetiology and antibiotic susceptibility pattern. Southern African Journal of infectious Diseases 32(4): 127-131. |
| [52] | Shobowale, E. O., Solarin, A. U. and Faniran, A. A. (2017). Neonatal sepsis in a Nigerian private tertiary hospital: bacterial isolates risk factors and antibiotic susceptibility pattern. Annals African Medicine 16(2): 52-58. |
| [53] | Yusef, D., Shalakhti, T., Awad, S., Algharaibeh, H. A. and Khasawneh, W. (2018). Clinical characteristics and epidemiology of sepsis in the neonatal intensive care unit in the era of multi-drug resistant organisms: a retrospective review. Pediatrics and Neonatology 59(1): 35-41. |
| [54] | Popescu, C. R., Cavanagh, M. M., Tembo, B., Chiume, M., Lufesi, N., Goldfarb, D. M., Kissoon, N. and Lavoie, P. M. (2020). Neonatal sepsis in low-income countries: epidemiology, diagnosis and prevention. Expert Review of Anti-Infective Therapy 18(5): 443-452. |
| [55] |
Tesini, B. L. (2022). Overview of neonatal infections-pediatrics. MSD manuals; Available at
https://www.msdmanuels.com/en-sg/professional/pediatrics/infections-in-neonates/overview-of-neonatal-infections accessed 1 May 2023. |
| [56] | Jiang, Z., Ren, Y. and Ye, S. (2024). Chromobacterium violaceum infections in children: two case reports and literature review. European Journal of Clinical Microbiology and Infectious Diseases 43(2024): 2477-2483. |
| [57] | Nwadioha, S. I., Kashibu, E., Alao, O. O. and Aliyu, I. (2011). Bacterial isolates in blood cultures of children with suspected septicaemia in Kano: a two year study. Niger Postgard Medicinal Journal 18: 130-133. |
| [58] | Onipede, A. O., Onuayade, A. A., Elusiyan, J. B., Obiajunwa, P. O., Ogundare, E. O., Olaniran, O. O., Adeyemi, L. A. and Oyelami, O. O. (2009). Invasive bacteria isolates from children with severe infections in a Nigerian hospital. Journal of Infection in Developing Countries 3(6): 429-436. |
| [59] | Mukherjee, S., Mitra, S., Dutta, S. and Basu, S. (2021). Neonatal sepsis: the impact of carbapenem-resistant and hypervirulent Klebsiella pneumoniae. Frontiers in Medicine 8: 634349. |
| [60] | Bai, X., Wei, Q., Duan, T., Yi, Y., Peng, H. and Hu, L. (2021). Predominance of Gram negative infections a cause of neonatal sepsis among low birth weight preterm infants. Journal of Laboratory Medicine 45(1): 7-12. |
| [61] | Ahmad, A., Sarwar, N., Aslam, R., Ali, S., Aslam, B., Arshad, M. A., Hameed, H. and Arshad, M. I. (2021). Pattern of clinical drug resistance and occurrence of Gram negative bacterial neonatal sepsis at a tertiary care hospital. Pakistan Journal of Pharmaceutical Sciences 34(5): 1873-1878. |
| [62] | Obadare, T., Adejuyigbe, E., Adeyemo, A. and Aboderin, O. (2021). Characterization of neonatal sepsis in a tertiary hospital in Nigeria. International Journal of Infectious Diseases 116: 1-130. |
| [63] | Obaro, H. K., Abdulkadir, B. and Abdullahi, S. (2022). In vitro antibiotic susceptibility of bacterial pathogens and risk factors associated with culture positive neonatal sepsis in two hospitals, Katsina metropolis Nigeria. African Journal of Clinical Experimental Microbiology 23(4): 378-388. |
| [64] | Obe, O. A., Mutiu, W. B., Ubuane, P. O. and Odulate, I. O. (2023). Bacteriological profile and antibiotic susceptibility pattern of common isolates of neonatal sepsis in a tertiary hospital from Lagos, Nigeria. Open Access Library Journal 10(8): 2333-9721. |
| [65] | Roy, S., Gaind, R., Chellani, H., Mohanty, S., Datta, S., Singh, A. K. and Basu, S. (2013). Neonatal septicaemia caused by diverse clones of Klebsiella pneumoniae and Escherichia coli harbouring blaCTX-M-15. Indian Journal of Medical Research 137: 791-799. |
| [66] | Vijayakanthi, N., Bahl, D., Kaur, N., Maria, A., and Dubey, N. K. (2013). Frequency and characteristics of infections caused by extended-spectrum beta-lactamase-producing organisms in neonates: a prospective cohort study. Bio-Medical Research International 2013: 1-8. |
| [67] | Datta, S., Roy, S., Chatterjee, S., Saha, A., Sen, B., Pal, T. and Basu, S. (2015). Correction: a five-year experience of carbapenem resistance in enterobacteriaceae causing neonatal septicaemia. Predominance of NDM-1: Plos One 10(9). |
| [68] | Ravikant, K. P., Ranotkar, S., Zutshi, S., Lahkar, M., Phukan, C. and Kandarpa, S. K. (2016). Prevalence and identification of extended spectrum β-lactamases (ESBL) in Escherichia coli isolated from a tertiary care hospital in North-East India. Indian Journal of Experimental Biology 54: 108-114. |
| [69] | Bora, A. and Ahmed, G. (2012). Detection of NDM-1 in Clinical Isolates of Klebsiella pneumoniae from North East India. Journal of Clinical and Diagnostic Research 6: 794-800. |
| [70] | Azab, K. S. M., Abdel-Rahman, M. A., El-Sheikh, H. H., Azab, E., Gobouri, A. A. and Farag, M. M. S. (2021). Distribution of extended- spectrum β-lactamase (ESBL) encoding genes among multidrug-resistant Gram negative pathogens collected from three different countries. Antibiotics 10(3): 247. |
| [71] | Ahmad-Hamad, P. and Khadija, K. M. (2019). Prevalence of blaTEM, blaSHV, and blaCTX-M genes among ESBL-producing Klebsiella pneumoniae and Escherichia coli isolated from Thalassemia in Erbil, Iraq. Mediterranean Journal of Hematology and Infectious Diseases 11(1). |
| [72] | Jorgensen, J. H., McElmeel, M. L., Fulcher, L. C. and Zimmer, B. L. (2010). Detection of CTX- M-type extended-spectrum beta-lactamase (ESBLs) by testing with microscan overnight and ESBL confirmation panels. Journal of Clinical Microbiology 48(1): 120-123. |
| [73] | Doi, Y., Park, Y. S., Rivera, J. I., Adams-Haduch, J. M., Hingwe, A., Sordillo, E. M. and Paterson, D. L. (2013). Community-associated extended-spectrum β-lactamase- producing Escherichia coli infection in the United States. Clinical Infectious Diseases 56(5): 641-648. |
| [74] | Ouedraogo, A. S., Sanou, M., Kissou, A., Sanou, S., Solare, H., Kabore, F. and Godreuil, S. (2016). High prevalence of extended-spectrum ß-lactamase producing enterobacteriaceae among clinical isolates in Burkina Faso. BioMedical Central Infectious Diseases 16(1). |
| [75] | Devrim, F., Serdaroglu, E., Caglar, I., Oruc, Y., Demiray, N., Bayram, N. and Devrim, I. (2018). The emerging resistance in nosocomial urinary tract infections: from the pediatrics perspective. Mediterranean Journal of Hematology and Infectious Diseases 10(1). |
| [76] | Uyanga, F. Z., Ekundayo, E. O., Nwankwo, E. O. and Ibanga, I. A. (2020). Molecular characterization of extended spectrum beta-lactamase from Enterobacter cloacae, E. coli and Klebsiella pneumoniae from pregnant women in South-south Nigeria. International Journal of Microbiology and Biotechnology 5(2): 48-54. |
| [77] | Al-Tahish, G. A. A., Al-Yosaffi, E. A., Othman, A. M., Al-Shamahy, H. A., Al-Haddad, A. M., Al-Moyed, K. A. and Al-Shawkany, A. M. (2024). Prevalence of blaTEM, blaSHV and blaCTM-M genes among ESBL-producing Escherichia coli isolated from the blood samples of intensive care units patients of university hospitals in Sana'a City, Yemen. Universal Journal of Pharmaceutical Research 8(6): 1-7. |
| [78] | Ojdana, D., Sacha, P., Wieczorek, P., Czaban, S., Michalska, A., Jaworowska, J. and Tryniszewska, E. (2014). The occurrence of blaCTX-M, blaSHV and blaTEM genes in extended-spectrum β-lactamase positive strains of Klebsiella pneumoniae, Escherichia coli and Proteus mirabilis in Poland. International Journal of Antibiotics 2014: (7). |
APA Style
Mary, C., Jarlath, U., Etanguno, O., Maria, B., Veronica, N. (2025). Molecular Characterization of Gram Negative Bacteria Involved in Sepsis Among Under Five Children in Akwa Ibom State Nigeria. International Journal of Microbiology and Biotechnology, 10(3), 111-130. https://doi.org/10.11648/j.ijmb.20251003.15
ACS Style
Mary, C.; Jarlath, U.; Etanguno, O.; Maria, B.; Veronica, N. Molecular Characterization of Gram Negative Bacteria Involved in Sepsis Among Under Five Children in Akwa Ibom State Nigeria. Int. J. Microbiol. Biotechnol. 2025, 10(3), 111-130. doi: 10.11648/j.ijmb.20251003.15
@article{10.11648/j.ijmb.20251003.15,
author = {Christopher Mary and Umoh Jarlath and Owowo Etanguno and Bassey Maria and Nyoyoko Veronica},
title = {Molecular Characterization of Gram Negative Bacteria Involved in Sepsis Among Under Five Children in Akwa Ibom State Nigeria
},
journal = {International Journal of Microbiology and Biotechnology},
volume = {10},
number = {3},
pages = {111-130},
doi = {10.11648/j.ijmb.20251003.15},
url = {https://doi.org/10.11648/j.ijmb.20251003.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmb.20251003.15},
abstract = {Sepsis is a life threatening medical emergency, Gram negative bacteria the principal causes of sepsis are seen in higher proportions among pediatrics populations and are mostly antibiotic resistance organisms. This study was carried out to determine antibiotic resistance of Gram negative bacteria, antibiotic resistance genes involve in sepsis among under five children in Akwa Ibom State, Nigeria. A hospital-based descriptive observational study of neonates with or without clinical features of sepsis. The subjects were children seen in General Hospital Ikot Ekpene, University Teaching Hospital Uyo and Immanuel Hospital Eket. A total of 180 children were sampled (60 from each hospital). A two milliliters (2 ml) sterile syringe with a 23gauge needle was used to collect blood sample aseptically from the vein of the arm of the child, inoculated on thioglycollate broth and subculture on MaConkey, blood and chocolate agar. Gram staining, biochemical characterization, antimicrobial susceptibility and resistance of Gram negative bacteria, their resistance genes were done. Of the 180 children, 123 tested positive for bacterial infections. Escherichia coli 25(13.9%), Proteus mirabilis 19(10.6%), Pseudomonas aeruginosa 15(8.3%), Klebsiella pneumoniae 12(6.7%), Serratia ficaria 9(5.0%), Rhizobium radiobacter 8(4.4%), Klebsiella oxytoca 7(3.9%), Chromobacterium violaceum 7(3.9%), Serratia marcescens 5(2.8%), Escherichia fergusonii 4(2.2%), Pseudomonas luteola 3(1.7%), Burkholderia cepacia 3(1.7%), Achromobacter xylosoxidans 3(1.7%), Burkholderia vietnamiensis 2(1.1%) and Serratia odorifera 1(0.6%). Pseudomonas aeruginosa was resistance to the 12 antibiotic used 12(100%), Three isolates were finally selected for molecular analysis, E. coli, P. aeruginosa, K. pneumoniae acquire blaSHV, PAGS, PASS, Cnf1 and hlyC genes, blaTEM amplify Pseudomonas and Klebsiella, FimH amplify only Klebsiella. Gram negative bacteria develop antibiotic resistance which poses a significant challenge in treating infections caused by this organism emphasizing the importance of responsible antibiotic use to mitigate further development of resistance.
},
year = {2025}
}
TY - JOUR T1 - Molecular Characterization of Gram Negative Bacteria Involved in Sepsis Among Under Five Children in Akwa Ibom State Nigeria AU - Christopher Mary AU - Umoh Jarlath AU - Owowo Etanguno AU - Bassey Maria AU - Nyoyoko Veronica Y1 - 2025/09/11 PY - 2025 N1 - https://doi.org/10.11648/j.ijmb.20251003.15 DO - 10.11648/j.ijmb.20251003.15 T2 - International Journal of Microbiology and Biotechnology JF - International Journal of Microbiology and Biotechnology JO - International Journal of Microbiology and Biotechnology SP - 111 EP - 130 PB - Science Publishing Group SN - 2578-9686 UR - https://doi.org/10.11648/j.ijmb.20251003.15 AB - Sepsis is a life threatening medical emergency, Gram negative bacteria the principal causes of sepsis are seen in higher proportions among pediatrics populations and are mostly antibiotic resistance organisms. This study was carried out to determine antibiotic resistance of Gram negative bacteria, antibiotic resistance genes involve in sepsis among under five children in Akwa Ibom State, Nigeria. A hospital-based descriptive observational study of neonates with or without clinical features of sepsis. The subjects were children seen in General Hospital Ikot Ekpene, University Teaching Hospital Uyo and Immanuel Hospital Eket. A total of 180 children were sampled (60 from each hospital). A two milliliters (2 ml) sterile syringe with a 23gauge needle was used to collect blood sample aseptically from the vein of the arm of the child, inoculated on thioglycollate broth and subculture on MaConkey, blood and chocolate agar. Gram staining, biochemical characterization, antimicrobial susceptibility and resistance of Gram negative bacteria, their resistance genes were done. Of the 180 children, 123 tested positive for bacterial infections. Escherichia coli 25(13.9%), Proteus mirabilis 19(10.6%), Pseudomonas aeruginosa 15(8.3%), Klebsiella pneumoniae 12(6.7%), Serratia ficaria 9(5.0%), Rhizobium radiobacter 8(4.4%), Klebsiella oxytoca 7(3.9%), Chromobacterium violaceum 7(3.9%), Serratia marcescens 5(2.8%), Escherichia fergusonii 4(2.2%), Pseudomonas luteola 3(1.7%), Burkholderia cepacia 3(1.7%), Achromobacter xylosoxidans 3(1.7%), Burkholderia vietnamiensis 2(1.1%) and Serratia odorifera 1(0.6%). Pseudomonas aeruginosa was resistance to the 12 antibiotic used 12(100%), Three isolates were finally selected for molecular analysis, E. coli, P. aeruginosa, K. pneumoniae acquire blaSHV, PAGS, PASS, Cnf1 and hlyC genes, blaTEM amplify Pseudomonas and Klebsiella, FimH amplify only Klebsiella. Gram negative bacteria develop antibiotic resistance which poses a significant challenge in treating infections caused by this organism emphasizing the importance of responsible antibiotic use to mitigate further development of resistance. VL - 10 IS - 3 ER -
Department of Microbiology, Faculty of Biological Sciences, Akwa Ibom State University, Ikot Akpaden, Nigeria
Department of Microbiology, Faculty of Biological Sciences, Akwa Ibom State University, Ikot Akpaden, Nigeria
Department of Microbiology, Faculty of Biological Sciences, Akwa Ibom State University, Ikot Akpaden, Nigeria
Department of Microbiology, Faculty of Biological Sciences, Akwa Ibom State University, Ikot Akpaden, Nigeria
Department of Biological Sciences, Topfaith University, Mkpatak, Nigeria
Information