Abstract
Cancer burden remain unacceptably high with global incidence of 19.3 Million and 10million cancer mortalities according to the 2020 global cancer estimates. There has been notable improvement in cancer care in Kenya with Chemotherapy being one of the most common and effective treatment modalities available. However, Chemotherapy is associated with Nutrition Impact Symptoms commonly referred to as the chemotherapy side effects, which include nausea, vomiting, sore throat and lack of appetite. However, the link between these side effects and dietary intake is not well studied. This study aimed at assessing the Nutrition Impact Symptoms and their contribution to the dietary intake and the nutrition status of cancer patients above 18 years of age, in Nyeri County Referral Hospital using analytical cross-sectional study design. A researcher administered questionnaire was used to collect data on the Nutrition Impact Symptoms, 24-hour recall and a Food Frequency Questionnaire was used to collect the dietary data and the Malnutrition Universal Screening Tool (MUST) was used to screen for the risk of malnutrition. Dietary data was analyzed using Nutri-Survey and the Statistical Package for the Social Sciences (SPSS). Sixty one percent of the respondents were female while 39% were male. Breast cancer was the most common cancer type in the population (39%), followed by esophageal and throat cancer at 14.5% and gastric cancer at 14%. Prostate cancer was the most prevalent among the male respondents at 11%. Nutrition Impact Symptoms that were reported include loss of appetite (72.1%), vomiting (55.8%), nausea (52.9%), diarrhea (39%), constipation (34.3%) and sore throat (8.1%), swallowing difficulties (0.6%), Pica (5.2%) and general body fatigue (9.3%). Unhealthy dietary patterns associated with the Nutrition Impact Symptoms include skipping meals, (69.2%), taking less than usual quantities of food than normal (71.5%), taking more food than normal quantities when not having side effects (8.7%), avoiding solid foods when symptoms are present (39%) and not eating at all 36.6%. Using the MUST, more than half (51.7%) of the respondents were at a high risk of developing malnutrition, followed by low risk (32.6%) with only 15.7% respondents being at a medium risk of malnutrition. Nutrition Impact Symptoms influence the dietary patterns of the cancer patients, which in turn contributes to the risk of malnourishment. Improving the Nutrition and health outcomes of cancer patients requires behavior change interventions that target the knowledge, attitude and practices of the patients towards the appropriate dietary patterns while on Chemotherapy.
|
Published in
|
Journal of Food and Nutrition Sciences (Volume 13, Issue 3)
|
|
DOI
|
10.11648/j.jfns.20251303.19
|
|
Page(s)
|
189-200 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Cancer, Nutrition Impact Symptoms, Dietary Patterns, Chemotherapy, Malnutrition Universal Screening Tools (MUST)
1. Introduction
Global cancer incidence and mortalities remain unacceptably high
. Malnutrition among the cancer patients is high and approximately 10-20% of the mortalities are associated with cancer- related malnutrition and not as a result of the tumor
| [2] | Muscaritoli M, Lucia S, Farcomeni A, Lorusso V, Saracino V, Barone C, et al. Prevalence of malnutrition in patients at first medical oncology visit: The PreMiO study. Oncotarget 2017; 8: 79884-96. https://doi.org/10.18632/oncotarget.20168 |
[2]
. There is need to reconsider malnutrition in cancer care because evidence shows that it is associated with reduced quality of life and influences the treatment outcomes
| [3] | Opanga Y, Kaduka L, Bukania Z, Mutisya R, Korir A, Thuita V, et al. Nutritional status of cancer outpatients using scored patient generated subjective global assessment in two cancer treatment centers, Nairobi, Kenya. BMC Nutr 2017; 3: 1-7. https://doi.org/10.1186/s40795-017-0181-z |
[3]
.
There has been notable improvement in cancer care in Kenya with Chemotherapy being one of the most common and effective treatment modalities available
. Chemotherapy is associated with Nutrition Impact Symptoms commonly referred to as the chemotherapy side effects, which include nausea, vomiting, sore throat and lack of appetite. De Vries et al., (2017) notes that to optimize dietary intake while on chemotherapy treatment, the patient’s nutrition status and the burden of the nutrition related drug symptoms need to be carefully monitored
| [5] | de Vries YC, van den Berg MMGA, de Vries JHM, Boesveldt S, de Kruif JTCM, Buist N, et al. Differences in dietary intake during chemotherapy in breast cancer patients compared to women without cancer. Support Care Cancer 2017; 25: 2581-91. https://doi.org/10.1007/s00520-017-3668-x |
[5]
.
Nutrition Impact Symptoms associated with Chemotherapy make it difficult to eat and retain nutrients, leading to malnutrition
| [6] | Kumar A. Assessment of Nutritional Status of Locally Advanced Head and Neck Carcinoma Patients Treated With Concomitant Chemo-radiation, by using Scored Patient-Generated Subjective Global Assessment (PG-SGA). J Med Sci Clin Res 2019; 7: 882-9. https://doi.org/10.18535/jmscr/v7i5.97 |
[6]
. The Kenya National treatment protocols emphasizes on cancer symptom management, nutritional support and management of chemotherapy side effects
| [7] | Kalebi. A CF, Mwang’ombe. N, Narayanan. V. Kenya national cancer treatment protocols. Natl Cancer Control Program 2019: 29, 50 |
[7]
, however, notable gaps exist in their management, so as to improve cancer therapy
.
Diet plays a very critical role in improving the nutrition and health outcomes of cancer patients on chemotherapy by preventing micronutrient deficiencies, mortalities reduction and also preventing malnutrition risk
| [2] | Muscaritoli M, Lucia S, Farcomeni A, Lorusso V, Saracino V, Barone C, et al. Prevalence of malnutrition in patients at first medical oncology visit: The PreMiO study. Oncotarget 2017; 8: 79884-96. https://doi.org/10.18632/oncotarget.20168 |
| [9] | Wang Y, Liu K, Long T, Long J, Li Y, Li J, et al. Dietary fish and omega-3 polyunsaturated fatty acids intake and cancer survival: A systematic review and meta-analysis. Crit Rev Food Sci Nutr 2023; 63: 6235-51. https://doi.org/10.1080/10408398.2022.2029826 |
| [10] | Naghshi S, Sadeghi O, Willett WC, Esmaillzadeh A. Dietary intake of total, animal, and plant proteins and risk of all cause, cardiovascular, and cancer mortality: Systematic review and dose-response meta-analysis of prospective cohort studies. The BMJ 2020; 370. https://doi.org/10.1136/bmj.m2412 |
[2, 9, 10]
. Consuming a healthy diet and in adequate amounts helps in prevention of both the tumor itself and also malnutrition among the cancer patients
| [11] | Muscaritoli M, Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin Nutr 2021; 40: 2898-913. https://doi.org/10.1016/j.clnu.2021.02.005 |
| [12] | American Cancer Society. Nutrition for People With Cancer Benefits of good nutrition during cancer treatment 2018: 1-27. |
| [13] | Ministry of Health Kenya. National Guidelines for Healthy Diets. Natl Guidel Healthy Diets Phys Act 2017. |
[11-13]
. Natural polyphenols have been well studied to examine their possible health effects especially defense against oxidative stress because they contain anticancer properties
| [14] | Bhosale PB, Ha SE, Vetrivel P, Kim HH, Kim SM, Kim GS. Functions of polyphenols and its anticancer properties in biomedical research: A narrative review. Transl Cancer Res 2020; 9: 7619-31. https://doi.org/10.21037/tcr-20-2359 |
[14]
. Long chain N-3 fatty acids or fish oils have been used as supplements for cancer patients on chemotherapy in order to stabilize or improve appetite
| [11] | Muscaritoli M, Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin Nutr 2021; 40: 2898-913. https://doi.org/10.1016/j.clnu.2021.02.005 |
[11]
. Dietary fish and marine omega-3 PUFAs have also been associated with survival of cancer patients because of their anti-inflammatory activity
| [9] | Wang Y, Liu K, Long T, Long J, Li Y, Li J, et al. Dietary fish and omega-3 polyunsaturated fatty acids intake and cancer survival: A systematic review and meta-analysis. Crit Rev Food Sci Nutr 2023; 63: 6235-51. https://doi.org/10.1080/10408398.2022.2029826 |
[9]
.
Dietary recommendations have been developed to inform cancer patients diet. A Mediterranean diet (MedDiet- a recommended cancer diet) is rich in complex carbohydrates, adequate amounts of fruits, vegetables and nuts. It also entails limited processed foods, red meats, poultry and dairy and it has been used in cancer management widely, although its uptake is still low in most countries
| [15] | Morze J, Danielewicz A, Przybyłowicz K, Zeng H, Hoffmann G, Schwingshackl L. An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer. Eur J Nutr 2021; 60: 1561-86. https://doi.org/10.1007/s00394-020-02346-6 |
[15]
.
Despite this progress in cancer diet, gaps exist on the implementation and especially on the link with the nutrition status of the cancer patients experiencing chemotherapy side effects. Malnutrition among the cancer patients remain high and the association between the dietary practices and the nutrition status of the cancer patients remain unclear. A study conducted in two hospitals in Nairobi County showed that 31% of cancer patients were malnourished, with notable increase among the patients with gastro-intestinal tumors
| [3] | Opanga Y, Kaduka L, Bukania Z, Mutisya R, Korir A, Thuita V, et al. Nutritional status of cancer outpatients using scored patient generated subjective global assessment in two cancer treatment centers, Nairobi, Kenya. BMC Nutr 2017; 3: 1-7. https://doi.org/10.1186/s40795-017-0181-z |
[3]
The European Society for Clinical Nutrition and Metabolism (ESPEN) guidelines outlines the need for proper malnutrition screening by the healthcare provider at the first contact with the cancer patient, to detect any nutritional disturbances that could be controlled if diagnosed earlier
| [11] | Muscaritoli M, Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin Nutr 2021; 40: 2898-913. https://doi.org/10.1016/j.clnu.2021.02.005 |
[11]
. In Kenya however, evidence shows that there still exists gaps in malnutrition recognition among cancer patients. In addition, malnutrition screening tools have been greatly under-utilized
| [10] | Naghshi S, Sadeghi O, Willett WC, Esmaillzadeh A. Dietary intake of total, animal, and plant proteins and risk of all cause, cardiovascular, and cancer mortality: Systematic review and dose-response meta-analysis of prospective cohort studies. The BMJ 2020; 370. https://doi.org/10.1136/bmj.m2412 |
[10]
.
This study therefore sought to bridge this gap, and seek the contribution of chemotherapy induced nutrition impact symptoms to the dietary intake and the nutrition status of adult cancer outpatients attending Nyeri County Referral Hospital, Kenya.
2. Materials and Methods
2.1. Research Design
This study employed analytical cross-sectional study design, appropriate for collecting data at one point in time. A researcher administered questionnaire was used to collect data on sociodemographic and economic characteristics of the cancer patients. A food frequency questionnaire and a 24-hour recall were used to collect dietary data and a MUST was used to screen the patients for malnutrition risk. A study conducted in Netherlands on determining the Malnutrition status of the hospitalized patients similarly employed an observational research design, using the Malnutrition Universal Screening tool
| [16] | Auma CMN, Mweu MM, Opiyo RO. Performance of Malnutrition Universal Screening Tool and Patient-Generated Global Subjective Assessment in screening for cancer-related malnutrition in Nairobi, Kenya. F1000Research 2022; 11: 755. https://doi.org/10.12688/f1000research.123059.1 |
[16]
.
2.2. Study Area
This study was done in Nyeri County Referral Hospital in Nyeri County, Kenya. This is one of the regions with a high burden of Non-Communicable Diseases
| [17] | Wambalaba FW, Son B, Wambalaba AE, Nyong’o D, Nyong’o A. Prevalence and Capacity of Cancer Diagnostics and Treatment: A Demand and Supply Survey of Health-Care Facilities in Kenya. Cancer Control 2019; 26: 1-12. https://doi.org/10.1177/1073274819886930 |
| [18] | NCIDP 2013-2017. Republic of Kenya Nyeri County Intergrated Development Plan 2013-2017 Department of Finance and Economic Planning 2013: 324. |
[17, 18]
. The hospital has a bed capacity of 407 beds, providing both in- and out-patients care, serving a population of over 800,000 residents.
2.3. Sample Size Determination and Sampling Strategy
Fischer’s formula
was used to estimate a sample size of 185 respondents at 95% Confidence Interval, 0.05 margins of error with an assumed malnutrition prevalence in Nyeri at 0.5 and an estimated non-response rate of 10%. The list of participants attending the clinic was used to select the sample using systematic random sampling. The first respondent was randomly selected using the table of random numbers generated from www.stattrek.com to determine the starting point. Every second respondent was systematically drawn until 185 respondents were achieved. The research team interviewed the respondents during the two days of clinic visits for a period of three weeks.
2.4. Validity and Reliability
A study on performance of the MUST in Nairobi Kenya reported a sensitivity of 83.1%, 95% CI and specificity of 85.7%, 95%CI
| [16] | Auma CMN, Mweu MM, Opiyo RO. Performance of Malnutrition Universal Screening Tool and Patient-Generated Global Subjective Assessment in screening for cancer-related malnutrition in Nairobi, Kenya. F1000Research 2022; 11: 755. https://doi.org/10.12688/f1000research.123059.1 |
[16]
. Pre-testing of the research instruments enhanced the validity and reliability of the research instruments and the methodology. 10% of the total sample (18 respondents) was used in pre-testing the data collection tools at Meru level 5 Hospital. Pre-testing aimed at evaluating the efficacy of the research instruments, sampling strategies and the method that the researcher had chosen for data analysis. It also aimed at enhancing the validity and reliability.
Internal consistency method was used (split half method) to indicate the degree of homogeneity of the items in the research instrument. The items on the instrument were divided into two. Reliability analysis was conducted on both sets of data and a reliability coefficient of 0.725 was generated, which is considered adequate for group studies
.
2.5. Data Collection Procedure
Two research assistants with Bachelor of Science in Nutrition and dietetics were trained to assist in data collection. They were trained on how to administer the researcher administered questionnaire, 24-hour recall, FFQ, MUST, how to record the information and on ethical consideration during the process. The oncology nurse in charge assisted in retrieving the information on the previous weight trend from the patients file.
The socio-economic and demographic characteristics of respondents’ data was collected using a researcher administered questionnaire. Sections of the questionnaire included data on the cancer type, chemotherapy drugs, duration on chemotherapy, side effects, dietary patterns, cancer staging and comorbidities. A 24-hour recall was used to collect dietary intake data while an FFQ assessed the frequency foods from various food groups was consumed. A Malnutrition Universal Screening Tool was used to screen the cancer patients for malnutrition. It utilizes three parameters related to each other to determine the nutrition status and thus stands as a good tool of assessing cancer-related malnutrition
| [16] | Auma CMN, Mweu MM, Opiyo RO. Performance of Malnutrition Universal Screening Tool and Patient-Generated Global Subjective Assessment in screening for cancer-related malnutrition in Nairobi, Kenya. F1000Research 2022; 11: 755. https://doi.org/10.12688/f1000research.123059.1 |
[16]
.
2.6. Data Analysis
Data was collected and analyzed using the Statistical Package for Social Sciences (SPSS) software version 27. Nutri-survey 2007 was used to analyze the 24-hr recall data that collected individual nutrient intake. Parametric statistical tests were performed on the data, putting into consideration the assumptions of parametric tests. Normality test was determined using the Kolmogorov - Smirnov test, (p>0.05) showing that the test was insignificant and thus the distribution of the sample was not drawn from significantly different population.
Descriptive statistics (Percentages, mean and Standard Deviation) was performed on categorical data (demographic and socio-economic characteristics, chemical treatment, clinical diagnosis, staging and comorbidities of the respondents. Inferential statistics (Chi-square tests) were used to test the association between chemotherapy side effects (categorical) and dietary patterns from the FFQ (categorical), The statistical significance threshold was set at α=0.05 (two tailed). Similarly, Chi-square tests was used to establish the association between chemotherapy side effects (categorical) and the risk of malnutrition (continuous scale, at a statistical significance of α=0.05 (two tailed), 95% CI. Inferential statistics-Pearson’s Moment correlation (statistical significance of α=0.05 (two tailed), 95% CI) was used to determine the association between two continuous variables Dietary data from the 24-hour recall and the malnutrition risk (using MUST). Further, to predict the value of the dependent variable from the independent variable (scale, scale), multiple regression analysis was done. The equation for the linear regression model was:
(Where Y is a continuous dependent (nutrition status) variable B0 is constant B1 is regression coefficient and X1 is a continuous independent variable, (dietary intake)).
The statistical significance threshold was set at α=0.05 (two tailed, 95% CI).
3. Results
3.1. Socio-Economic and Demographic Characteristics of the Study Population
The study had a 93% response rate which is within the acceptable range
. Sixty one percent were female while 39% of them were male. The mean (SD) age of the respondents was 65.9 for male and 55.8 for female. The youngest respondent in the population was 23 years old, with the oldest being 93 years old. Half of the respondents survive on a monthly income of between 0-10,000 Kenyan shillings and only 2.6% of the respondents earning more than Ksh. 50,000.
Table 1. Socio-economic and demographic characteristics of the study population.
Respondent’s Characteristics | Frequency | Percent (%) |
Respondents gender | N=172 | |
Male | 67 | 39.0 |
Female | 105 | 61.0 |
Religion | | |
Christianity | 165 | 95.9 |
Muslim | 7 | 4.1 |
Respondent’s education level | | |
Primary | 105 | 61.0 |
Secondary | 50 | 29.1 |
College | 16 | 9.3 |
University | 1 | .60 |
Marital Status of the respondents | | |
Married | 125 | 72.7 |
Single | 31 | 18.0 |
Widowed/Deceased | 16 | 9.3 |
Monthly Income | | |
0-10,000 | 86 | 50.0 |
10,000-20,000 | 49 | 28.5 |
20,000-50,000 | 32 | 18.6 |
50,000-100,000 | 5 | 2.9 |
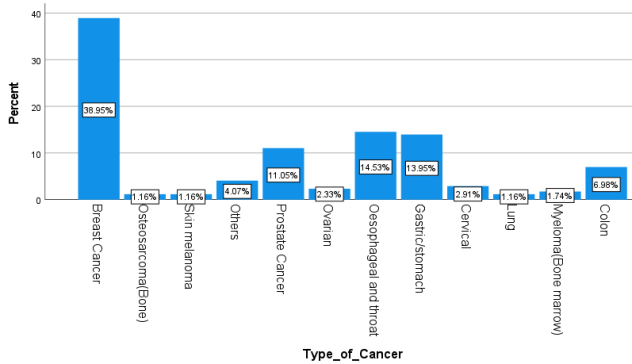
Figure 1. Percentage distribution of cancer types.
Gender was significantly associated with the respondents’ BMI (p=0.01) and the overall risk of malnutrition as estimated using Malnutrition Universal screening tool (MUST) was found to have a significant association with the age of the respondents. The cancer type was significantly associated with BMI and MUST at p<0.05 at all levels. There was a statistically significant association between education level and the monthly income of the respondents at p<0.05 rejecting a null hypothesis that there is no association between education level and the monthly income of the respondents.
3.2. Clinical Diagnosis of Cancer
Various cancer types were reported by the respondents, with the largest percentage of respondents having breast cancer (39%), followed by esophageal and throat cancer at (14.5%) and gastric cancer at 14%. Prostate cancer was the most prevalent among the male respondents at 11%. Other cancer cases reported included colon cancer (7%), ovarian cancer (2.3%), ervical cancer (2.9%) and bone marrow (1.2%).
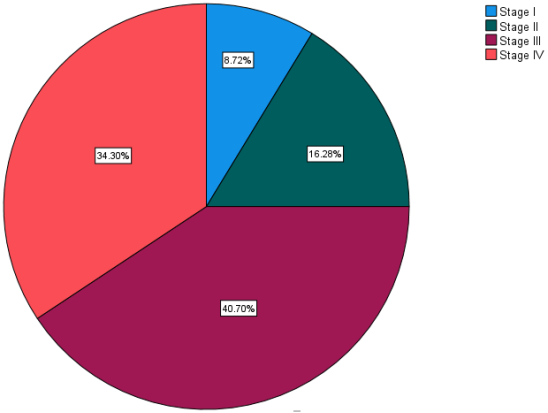
3.3. Stage of Diagnosis
The average year of diagnosis ranged from 2014 to 2023, with the majority of the respondents being diagnosed with cancer in 2022 (28.5%) followed by 2023 (26.7%). At the point of diagnosis, 34.3% subjects had a late diagnosis at stage IV and 40.7% of all cancer cases was diagnosed at stage III (40.7%). Only 25% had been diagnosis at stage I and II as shown in
figure 2 below.
Figure 2. Clinical diagnosis of cancer patients.
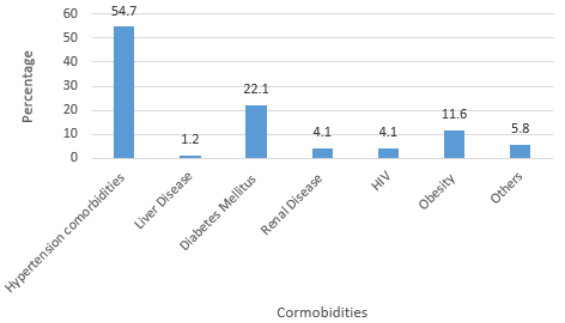
3.4. Comorbidities
Based on the Charlson comorbidity index, most cancer patients at NCRH had hypertension (54.7%), followed by Diabetes Mellitus (22.1%) and obese cases were 11.6%. The
figure 3 below is a representation of the distribution of the respondents by the comorbidities present.
Figure 3. Distribution of respondents by the comorbidities.
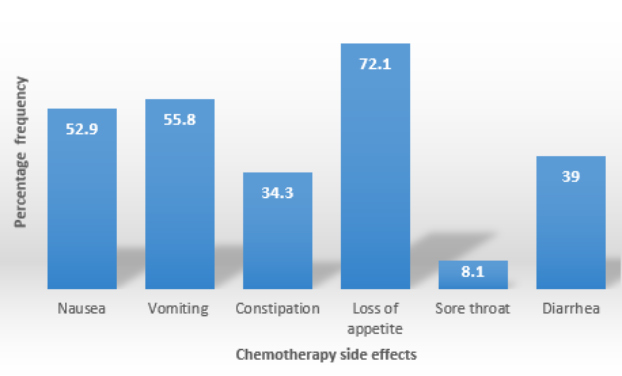
3.5. Nutrition Impact Symptoms
Ninety three percent of the respondents reported to have experienced side effects after using the chemotherapy drugs. The most common symptoms reported included, loss of appetite (72.1%) vomiting (55.8%), nausea (52.9%), diarrhea (39%), constipation (34.3%) sore throat 8.1%, swallowing difficulties (0.6%), Pica (5.2%) and general body fatigue (9.3%) as shown in
figure 4 below. The duration of the side effects varied with individuals, but the most common was between 4-7 days.
Figure 4. Chemotherapy side effects.
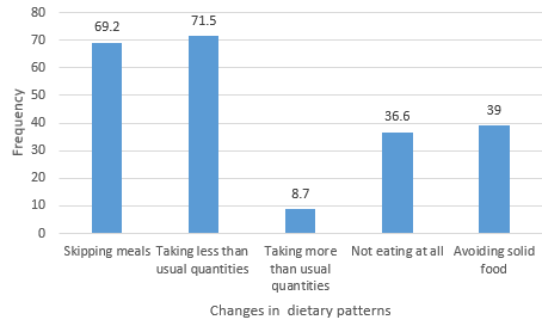
3.6. Dietary Changes Associated with Chemotherapy Side Effects
Thirty four percent of the respondents reported that the avoid the following foods when side effects are present; refined foods (9.3%), oily foods (3.5%), animal protein (1.2%), wheat-based foods (2.3%) and rice (7%). Dietary changes that the respondents associated with the chemotherapy side effects include, skipping meals, (69.2%), taking less than usual quantities of food, (71.5%), taking more food than normal quantities when not having side effects (8.7%), avoiding solid foods when symptoms are present (39%) and not eating at all (36.6%) as shown in
figure 5 below.
Figure 5. Dietary changes associated with chemotherapy side effect.
3.7. Association Between Chemotherapy Side Effects and Dietary Practices of the Respondents
Chi square tests and odds risk ratio was used to show the association between chemotherapy side effects and dietary practices (using FFQ) of the respondents. The association between nausea and skipping meals when symptoms are present was significant (P=0.04), rejecting the null hypothesis that there is no significant association between nausea presence and skipping meals. Loss of appetite led to taking less than usual quantities of the served food, (P<0.05) while nausea was significantly associated with skipping of meals (P=0.04). Presence of sore throat was associated significantly with taking less than usual quantities of food and also avoidance of solid foods, (P<0.05) as shown in the
table 2 below.
Table 2. Association between chemotherapy side effects and the dietary practices (N-172).
Nutrition Impact symptoms | Skipping meals | Taking less than usual quantities | Taking more than usual quantities | Not eating at all | Avoiding solid foods |
Nausea | 0.04* | 0.12 | 0.09 | 0.28 | 0.38 |
Vomiting | 0.43 | 0.14 | 0.16 | 0.17 | 0.54 |
Constipation | 0.37 | 0.47 | 0.85 | 0.28 | 0.69 |
Loss of appetite | 0.62 | 0.01* | 0.20 | 0.37 | 0.24 |
Sore throat | 0.86 | 0.00* | 0.21 | 0.61 | 0.02* |
Diarrhea | 0.35 | 0.97 | 0.64 | 0.61 | 0.54 |
Estimating the relative risk using odds ratio, the patients who had nausea were 4.95 times likely to skip meals when the side effects were present compared to when side effects were not present. Similarly, those who reported loss of appetite as the side effects were 1.39 times likely to take less than usual amounts of food when the side effects were present. Those who had sore throat were 2.75 times likely to take less than usual amounts of food and 3.04 times likely to avoid any solid foods when the symptoms were present compared to when the side effects were absent as shown below.
Table 3. Association between chemotherapy side effects and the dietary practices; odds ratio.
| | | | 95% C. I |
N | P-value | Odds Ratio | Lower | Upper |
Nausea *Skipping meals | 172 | 0.04 | 4.95 | 1.383 | 17.795 |
Loss of appetite * Taking less than usualquantities | 172 | 0.01 | 1.39 | .077 | 2.025 |
Sore throat* Taking less than usual | 172 | .00 | 2.75 | .57 | 13.17 |
Sore throat *Avoiding solid foods | 172 | .00 | 3.04 | .638 | 14.56 |
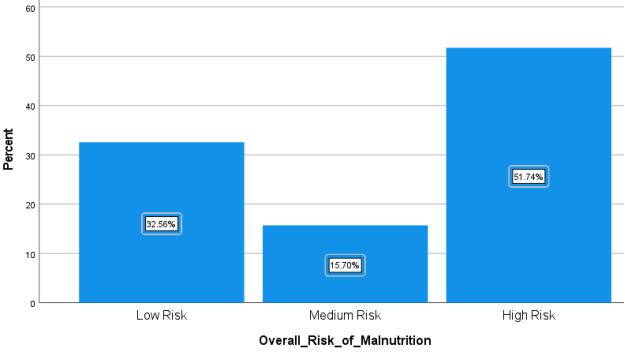
3.8. Malnutrition Screening of Cancer Patients Using MUST
Malnutrition Universal Screening tool (MUST) was used to screen the cancer patients for malnutrition risk. More than half (51.7%) were at a high risk of developing malnutrition, followed by low risk (32.6%) with only 15.7% respondents being at a medium risk of malnutrition as shown below,
figure 6.
Figure 6. Percentage risk of malnutrition for the cancer patients using MUST.
3.9. Body Mass Index (BMI)
The BMI of participants was classified as per the WHO classification
| [22] | Centers of disease control. Body mass index: Considerations for practitioners. Cdc 2011: 4. |
[22]
. Using the BMI, Half of the respondents, (50%) had a normal nutrition status and only 19.8% respondents were underweight as illustrated in
table 4 below.
Table 4. BMI classification of the respondents.
Classification | N | % |
<18.5 (underweight) | 34 | 19.8% |
18.5-24.9 (Normal) | 86 | 50.0% |
25-29.9 (Overweight) | 34 | 19.8% |
>30.0 (Obese) | 18 | 10.5% |
A significant difference between BMI and Malnutrition Universal screening tool in classifying the Nutrition status was found, (Pearson Chi square Value=76.497 a), significance (2 sided) p=<0.01).
3.10. Association Between the variables
Loss of appetite was significantly associated with the MUST with P<0.05, rejecting the hypothesis that there is no significant association between chemotherapy side effects and the risk of malnutrition. Other chemotherapy side effects had a P>0.05 as shown below on
table 5, failing to reject the hypothesis that there is no significant association between nausea, vomiting, constipation, sore throat and the Nutrition status of the cancer patients.
Table 5. Association between chemotherapy side effects and the nutrition status of the respondents.
Chemotherapy Side Effects | BMI | MUST |
Nausea | 0.58 | 0.51 |
Vomiting | 0.34 | 0.16 |
Constipation | 0.95 | 0.85 |
Loss of appetite | 0.12 | 0.04* |
Sore throat | 0.54 | 0.65 |
Diarrhea | 0.45 | 0.24 |
The individual energy intake (from the 24-hour recall data) was cross-tabulated with the malnutrition Universal screening tool and the relationship was statistically significant, (P<0.05) as indicated in
table 6 below, rejecting the null hypothesis that there is no significant association between the energy intake and the risk of being malnourished.
Table 6. Association between individual energy intake and the Nutrition status.
| R | R Square | B | Std. Error | Beta | Significance |
| (Constant) | .408a | .167 | 1.388 | .157 | | .000 |
Energy | | | .000 | .000 | -.106 | .167 |
4. Discussion
4.1. Socio-Economic and Demographic Characteristics of the Respondents
Both men and women are affected by cancer non-selectively. More female (61%) had different types of cancer compared to male (39%), with the leading type of cancer among female being breast cancer (39%) and prostate cancer being the leading cancer type in men (11%). These findings agree with the 2020 global cancer statics, which breast cancer surpassed the lung cancer incidence and was top of the commonly diagnosed cancers at 11.7% globally, and prostate was top leading male cancer at 7.3%
| [23] | Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2021; 71: 209-49. https://doi.org/10.3322/caac.21660 |
[23]
. However, this study reveals higher statistics compared to the global estimates, indicating that there may be gaps in the cancer reporting or that it is because this study focused on the cancer patients on chemotherapy only.
Income inequality has been increasing worldwide, education is one of the markers of financial stability and there is clear evidence that the higher the education level, the greater the chances of securing a formal employment and a higher income in response
| [24] | Hinata A, Kabasawa K, Watanabe Y, Kitamura K, Ito Y, Takachi R, et al. Education, household income, and depressive symptoms in middle-aged and older Japanese adults. BMC Public Health 2021; 21: 1-10. https://doi.org/10.1186/s12889-021-12168-8 |
[24]
. Cancer care has been reportedly expensive and a big percent of the population requires to pay for some of the services since the NHIF does not comprehensively cover cancer treatment. In addition, the educated cancer patients have access to private care, improving their treatment outcomes. The significant association between education level and the monthly income of the respondents (P<0.05) was confirmed by this study. This explains why most of the respondents (61%) who had the basic primary education level had limited ability to comprehensive health care, consume the recommended servings of fruits, vegetables, milk and milk products and fish products which have been associated with the important bioactive compounds for fighting against cancer.
Gender had a significant association with the nutrition status. The overall risk of malnutrition as estimated using Malnutrition Universal screening tool (MUST) was found to have a significant association with the age of the respondents. This agrees with literature that one of the factors that influence nutrition status of individuals in gender. Men tend to be more masculine than their female counterparts.
4.2. Clinical Diagnosis of Cancer
The KEMRI regional cancer registry reveals 80% rates of late cancer diagnosis
| [17] | Wambalaba FW, Son B, Wambalaba AE, Nyong’o D, Nyong’o A. Prevalence and Capacity of Cancer Diagnostics and Treatment: A Demand and Supply Survey of Health-Care Facilities in Kenya. Cancer Control 2019; 26: 1-12. https://doi.org/10.1177/1073274819886930 |
[17]
. The treatment goal for cancer stage IV patients is to improve the length and quality of life but not curative. In this study, the average year of diagnosis ranged from 2014 to 2023, with the majority of the respondents being diagnosed with cancer in 2022 followed by 2023. Seventy five percent of the cancer cases were made at stage III and stage IV. There is clear evidence that if cancer is diagnosed early, the treatment outcomes are better than when diagnosed at late stages,
| [25] | MoH-Kenya. Kenya STEPwise Survey for Non Communicable Diseases Risk Factors 2015 Report. Public Health 2015; 5: 8-210. |
[25]
. This raises the need for adequate cancer awareness across populations.
Based on the Charlson comorbidity index, most cancer patients at NCRH had hypertension, followed by Diabetes Mellitus and obesity. The non-communicable diseases such as cancer, hypertension and diabetes share the risk factors and this may explain this observation. Comorbidities affect cancer prognosis and it has been noted that comorbidities are associated with poor survival and poor quality of life leading to high health care cost
| [26] | Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40: 373-83. https://doi.org/10.1016/0021-9681(87)90171-8 |
[26]
. If a reduction in these chronic diseases has to be realized, the entire population requires nutrition education and counselling on how to prevent the non-communicable diseases through healthy lifestyle, (diets and physical activity). This however may need to be relooked at. From this study, less than half of the respondents had received nutrition education and counselling in the course of their treatment.
4.3. Chemotherapy Treatment and the Nutrition Impact Symptoms
Chemotherapy drugs were used in combination and not as a single dose and most of the respondents reported having experienced chemotherapy side effects in the course of their treatment. The most common combination was capecitabine and oxaliplatin and the most common nutrition related side effect was loss of appetite. Different drugs are administered to different individuals depending on a number of factors such as the type of cancer type and stage of cancer. If adverse outcomes occur in the course of the treatment, a change in the drugs combination is made.
Side effects associated with cancer treatment include nausea, vomiting, diarrhea, lack of appetite, sore throat among others. Chemotherapy induced diarrhea (CID) and Chemotherapy induced constipation (CIC) have been reported as the most common gastro-intestinal toxicities with a prevalence of 80% and 16% respectively. however, the mechanisms that lead to CID and CIC are yet not very clear but suggestions have been made that this may be as a result of intersecting mechanisms such as tumor inflammation, secretory dysfunctions among others
| [27] | McQuade RM, Stojanovska V, Abalo R, Bornstein JC, Nurgali K. Chemotherapy-induced constipation and diarrhea: Pathophysiology, current and emerging treatments. Front Pharmacol 2016; 7: 1-14. https://doi.org/10.3389/fphar.2016.00414 |
[27]
.
From this study, the CIC prevalence was 34.3% and the CID prevalence was 39%, which was lower than what McQuade et al., 2016 reported. This may be as a result of the drugs that the chemotherapy patients at NCRH are given to combat the side effects. Nausea and vomiting also is a nutrition related side effects, which is associated with weight loss and loss of nutrients from the body.
Nutritional education programs also need to be incorporated in the cancer care management to advise the patients on the methods of food preparation so as to reduce nausea and vomiting. From these findings on the chemotherapy induced side effects, it can be concluded that nutrition education and counseling is very critical when it comes to cancer care. Less than half of the population who had not received any nutritional counselling throughout their treatment period might have benefited from nutrition education and their nutrition status would have been improved, which in return could have improved the treatment outcomes.
4.4. Dietary Practices
Dietary patterns of the cancer patients are very pertinent and they need to be closely monitored especially because of the chemotherapy induced side effects. Dietary changes that the respondents associated with the chemotherapy side effects that were revealed from this study include, skipping meals, taking less than usual quantities of food than normal and avoiding solid foods when symptoms are present. A recent systematic review on how the modern dietary practices influence the cancer risk and progression recommends incorporating a Mediterranean dietary intervention to reduce the odds of cancer advancement
| [28] | Nagy S, Petrosky SN, Beckler MD, Kesselman MM. The Impact of Modern Dietary Practices on Cancer Risk and Progression: A Systematic Review. Cureus 2023. https://doi.org/10.7759/cureus.46639 |
[28]
.
Similarly, the American Cancer Society guidelines for a healthy diet recommends consumption of nutrient dense foods to maintain a healthy body weight for the cancer patients, consume adequate fruits and vegetables whole grains, limited use of red and processed meats, sugars and processed foods
| [29] | Rock CL, Thomson C, Gansler T, Gapstur SM, Mccullough ML, Patel AV, et al. American Cancer Society Guideline for Diet and Physical Activity for Cancer Prevention 2020; 70: 245-71. https://doi.org/10.3322/caac.21591 |
[29]
The starchy foods and the fatty foods categories were the most consumed with majority of the respondents reporting to be taking them on a daily basis. This may be because the highest percentage of the respondents (40.1%) are farmers and mostly the starchy foods are readily available. However, this poses nutritional risks to them. The non-communicable diseases risk factors are similar, the main one being obesity and diets rich in fats and starches. Obesity pathophysiology is also linked to fat deposition associated with excessive intake of fats and carbohydrates. Whole grains for cancer care increase the bulkiness of stool. Bulky stools have an increased transit time which reduces the interaction between carcinogenic substances with normal cells. It also limits the bacterial endotoxins which damages the cells from being absorbed. The whole grains are rich in fiber. During the digestion process, fiber breaks down into short chain fatty acids which are a source of energy that the cancer cells have the inability to utilize. This lowers the growth and development of the cancer cells
| [28] | Nagy S, Petrosky SN, Beckler MD, Kesselman MM. The Impact of Modern Dietary Practices on Cancer Risk and Progression: A Systematic Review. Cureus 2023. https://doi.org/10.7759/cureus.46639 |
[28]
.
The dietary patterns of the respondents also showed that the WHO recommendations of 3-5 servings of fruits and vegetables per week was not met by all. Less than half (41.9%) were not attaining the minimum daily requirements of the fruit’s servings, with 2.3% rarely consuming fruits at all. Fruits and vegetables are associated with antioxidants that are so important in management of cancer. The anti-oxidant properties of flavonoids, Vitamin C and E and carotenoids are mostly found in fruits and the dark green vegetables. A very small percent of people (8.7%) incorporated nuts and seeds in their diets with the largest percentage consuming the minimum serving. Nuts and seeds are important sources of poly-unsaturated fatty acids, and specifically omega 3 and omega 6 fatty acids. Omega 3 fatty acids have been associated with reduction in inflammation, reduced angiogenesis, metastasis and reduced proliferation of cells
| [30] | Gomes-Neto AW, Vliet IMY van, Osté MCJ, Jong MFC de, Bakker SJL, Jager-Wittenaar H, et al. Malnutrition Universal Screening Tool and Patient-Generated Subjective Global Assessment Short Form and their predictive validity in hospitalized patients. Clin Nutr ESPEN 2021; 45: 252-61. https://doi.org/10.1016/j.clnesp.2021.08.015 |
[30]
.
A small percentage (37.8%) of respondents consumed milk and milk products, which are very high sources of calcium, key in bone strengthening. One of the common problems associated with chemotherapy treatment in cancer care is bone loss. Chemotherapy drugs such as doxorubicin and cisplatin reduce calcium levels in the body, leading to body loss
| [30] | Gomes-Neto AW, Vliet IMY van, Osté MCJ, Jong MFC de, Bakker SJL, Jager-Wittenaar H, et al. Malnutrition Universal Screening Tool and Patient-Generated Subjective Global Assessment Short Form and their predictive validity in hospitalized patients. Clin Nutr ESPEN 2021; 45: 252-61. https://doi.org/10.1016/j.clnesp.2021.08.015 |
[30]
. This must be supplied in adequate amounts together with Vitamin D rich foods because optimal levels of Vitamin D are necessary to enhance calcium absorption. This study reveals that a small percentage of the respondents consumed foods from the fish and meats categories, which is the main dietary source of Vitamin D.
4.5. Nutrition Status of Cancer Patients
More than half of the respondents were at a high risk of developing malnutrition, followed by low risk (32.6%) with only 15.7% respondents being at a medium risk of malnutrition. Using the BMI, Half of the respondents, (50%) had a normal nutrition status and only 19.8% respondents were underweight. Body Mass Index has been greatly used as an indicator for the nutrition status in a healthy population, but it tends to under-estimate weight loss in patients with chronic illnesses
| [16] | Auma CMN, Mweu MM, Opiyo RO. Performance of Malnutrition Universal Screening Tool and Patient-Generated Global Subjective Assessment in screening for cancer-related malnutrition in Nairobi, Kenya. F1000Research 2022; 11: 755. https://doi.org/10.12688/f1000research.123059.1 |
[16]
.
The utilization of Malnutrition Universal Screening tool (MUST) is becoming popular because of its good validity and reliability. MUST utilizes three components, the BMI-Score, unplanned weight loss for the last 6 months and the acute disease score. High risks of malnutrition have been significantly associated with mortality, (HR=3.9; 95%CI, P=0.02)
| [30] | Gomes-Neto AW, Vliet IMY van, Osté MCJ, Jong MFC de, Bakker SJL, Jager-Wittenaar H, et al. Malnutrition Universal Screening Tool and Patient-Generated Subjective Global Assessment Short Form and their predictive validity in hospitalized patients. Clin Nutr ESPEN 2021; 45: 252-61. https://doi.org/10.1016/j.clnesp.2021.08.015 |
[30]
. The malnutrition screening tools have been greatly under-utilized despite the fact that they can predict malnutrition early, and improve the treatment outcome
| [3] | Opanga Y, Kaduka L, Bukania Z, Mutisya R, Korir A, Thuita V, et al. Nutritional status of cancer outpatients using scored patient generated subjective global assessment in two cancer treatment centers, Nairobi, Kenya. BMC Nutr 2017; 3: 1-7. https://doi.org/10.1186/s40795-017-0181-z |
[3]
. A significant difference was found between classifying the nutrition status using BMI and Malnutrition Universal screening tool and this justifies the reason why adoption of more than one tool in determining malnutrition in cancer patients is recommended.
4.6. Association Between Variables
Nausea, vomiting, constipation, loss of appetite, sore throat and diarrhea did not have a significant association with the daily energy intake. On the dietary changes of the respondents, presence of sore throat caused the respondents to avoid solid foods when the sore throat is present. It is common for an individual to avoid certain foods, when they are in pain or as a result of any form of discomfort. However, this has other adverse side effects such as reduced intake of the required calories which affects the nutrition status.
The drugs combination that the respondents were using did not have a significant association with the onset of the side effects. There has been an advancement in cancer care, where chemotherapy patients are given medication to manage the side effects. This may explain this reality that the combinations may not necessarily influence the onset of these side effects
| [31] | Macdonald V. Oncology Corner Le coin de l’oncologie Chemotherapy: Managing side effects and safe handling. vol. 50. 2009. |
[31]
. The side effects arise as a result of a result of intersecting mechanisms such as tumor inflammation, secretory dysfunctions among others
| [27] | McQuade RM, Stojanovska V, Abalo R, Bornstein JC, Nurgali K. Chemotherapy-induced constipation and diarrhea: Pathophysiology, current and emerging treatments. Front Pharmacol 2016; 7: 1-14. https://doi.org/10.3389/fphar.2016.00414 |
[27]
.
A significant positive association was found between chemotherapy side effects and the changes in the dietary patterns. The patients who had nausea were 4.95 times likely to skip meals when the side effects were present compared to when side effects were not present. Similarly, those who reported loss of appetite were 1.39 times likely to take less than usual amounts of food when the side effects were present. Those who had sore throat were 2.75 times likely to take less than usual amounts of food and 3.04 times likely to avoid any solid foods when the symptoms were present compared to when the side effects were absent.
Despite the significant role played by nutrition education in improved nutrition outcomes, 44.19% of the respondents had not received any nutritional education in the course of their treatment. Almost thirty five percent of the respondents who had not received nutritional education reported that there are certain foods that they do not consume at all when the side effects are present for some reasons. Nutrition education is important in improving the nutrition and health outcomes of the cancer outpatients.
5. Conclusions
Chemotherapy side effects influences the dietary practices and the nutrition status of cancer patients. The Nutrition Impact Symptoms makes the respondents lose appetite, vomit and experience difficulty in swallowing, forming unhealthy dietary patterns such as avoidance of certain food groups, taking less than usual quantities of food, skipping meals, excessive consumption of starchy and oily foods reducing the amount of nutrients consumed. This leads to increased risk of malnutrition. There is a weak positive significant relationship between individual’s dietary intake (24hr-recall) and the risk of malnutrition (using MUST), evidenced by a Linear regression, r (0.41), showing that only 16.7% of the overall risk of malnutrition can be explained by the dietary intake. To improve the nutrition and health outcomes of the cancer patients, this study recommends further study on assessment of the food systems dominant in the study area, assess the food security status and establish its association with these dietary practices. In addition, interventions targeting the social and behavior approach need to be implemented to improve the knowledge, attitude and practices of the respondents towards the appropriate dietary practices, when on chemotherapy.
Abbreviations
MUST | Malnutrition Universal Screening Tool |
BMI | Body Mass Index |
NCRH | Nyeri County Referral Hospital |
CIN | Chemotherapy Induced Nausea |
CIV | Chemotherapy Induced Vomiting |
Acknowledgments
I would like to appreciate the support from the Department of Health at Nyeri County during this research. In addition, special appreciation goes to the staff at the oncology department in Nyeri County Referral Hospital for the support in data collection.
Author Contributions
Dorothy Kareainto Bundi: Conceptualization, methodology, data analysis, and writing
Paul Sang: Methodology, review and editing
Amos Ronoh: Methodology, data analysis, review and editing
Funding
This work is not supported by any external funding.
Data Availability Statement
The data supporting the outcome of this research work has been reported in this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Deo SVS, Sharma J, Kumar S. GLOBOCAN 2020 Report on Global Cancer Burden: Challenges and Opportunities for Surgical Oncologists. Ann Surg Oncol 2022; 29: 6497-500.
https://doi.org/10.1245/s10434-022-12151-6
|
| [2] |
Muscaritoli M, Lucia S, Farcomeni A, Lorusso V, Saracino V, Barone C, et al. Prevalence of malnutrition in patients at first medical oncology visit: The PreMiO study. Oncotarget 2017; 8: 79884-96.
https://doi.org/10.18632/oncotarget.20168
|
| [3] |
Opanga Y, Kaduka L, Bukania Z, Mutisya R, Korir A, Thuita V, et al. Nutritional status of cancer outpatients using scored patient generated subjective global assessment in two cancer treatment centers, Nairobi, Kenya. BMC Nutr 2017; 3: 1-7.
https://doi.org/10.1186/s40795-017-0181-z
|
| [4] |
Hosseinzadeh E, Banaee N, Nedaie HA. Cancer and Treatment Modalities. Curr Cancer Ther Rev 2017; 13.
https://doi.org/10.2174/1573394713666170531081818
|
| [5] |
de Vries YC, van den Berg MMGA, de Vries JHM, Boesveldt S, de Kruif JTCM, Buist N, et al. Differences in dietary intake during chemotherapy in breast cancer patients compared to women without cancer. Support Care Cancer 2017; 25: 2581-91.
https://doi.org/10.1007/s00520-017-3668-x
|
| [6] |
Kumar A. Assessment of Nutritional Status of Locally Advanced Head and Neck Carcinoma Patients Treated With Concomitant Chemo-radiation, by using Scored Patient-Generated Subjective Global Assessment (PG-SGA). J Med Sci Clin Res 2019; 7: 882-9.
https://doi.org/10.18535/jmscr/v7i5.97
|
| [7] |
Kalebi. A CF, Mwang’ombe. N, Narayanan. V. Kenya national cancer treatment protocols. Natl Cancer Control Program 2019: 29, 50
|
| [8] |
Pucci C, Martinelli C, Ciofani G. Innovative approaches for cancer treatment: Current perspectives and new challenges. Ecancermedicalscience2019; 13: 1-26.
https://doi.org/10.3332/ecancer.2019.961
|
| [9] |
Wang Y, Liu K, Long T, Long J, Li Y, Li J, et al. Dietary fish and omega-3 polyunsaturated fatty acids intake and cancer survival: A systematic review and meta-analysis. Crit Rev Food Sci Nutr 2023; 63: 6235-51.
https://doi.org/10.1080/10408398.2022.2029826
|
| [10] |
Naghshi S, Sadeghi O, Willett WC, Esmaillzadeh A. Dietary intake of total, animal, and plant proteins and risk of all cause, cardiovascular, and cancer mortality: Systematic review and dose-response meta-analysis of prospective cohort studies. The BMJ 2020; 370.
https://doi.org/10.1136/bmj.m2412
|
| [11] |
Muscaritoli M, Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin Nutr 2021; 40: 2898-913.
https://doi.org/10.1016/j.clnu.2021.02.005
|
| [12] |
American Cancer Society. Nutrition for People With Cancer Benefits of good nutrition during cancer treatment 2018: 1-27.
|
| [13] |
Ministry of Health Kenya. National Guidelines for Healthy Diets. Natl Guidel Healthy Diets Phys Act 2017.
|
| [14] |
Bhosale PB, Ha SE, Vetrivel P, Kim HH, Kim SM, Kim GS. Functions of polyphenols and its anticancer properties in biomedical research: A narrative review. Transl Cancer Res 2020; 9: 7619-31.
https://doi.org/10.21037/tcr-20-2359
|
| [15] |
Morze J, Danielewicz A, Przybyłowicz K, Zeng H, Hoffmann G, Schwingshackl L. An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer. Eur J Nutr 2021; 60: 1561-86.
https://doi.org/10.1007/s00394-020-02346-6
|
| [16] |
Auma CMN, Mweu MM, Opiyo RO. Performance of Malnutrition Universal Screening Tool and Patient-Generated Global Subjective Assessment in screening for cancer-related malnutrition in Nairobi, Kenya. F1000Research 2022; 11: 755.
https://doi.org/10.12688/f1000research.123059.1
|
| [17] |
Wambalaba FW, Son B, Wambalaba AE, Nyong’o D, Nyong’o A. Prevalence and Capacity of Cancer Diagnostics and Treatment: A Demand and Supply Survey of Health-Care Facilities in Kenya. Cancer Control 2019; 26: 1-12.
https://doi.org/10.1177/1073274819886930
|
| [18] |
NCIDP 2013-2017. Republic of Kenya Nyeri County Intergrated Development Plan 2013-2017 Department of Finance and Economic Planning 2013: 324.
|
| [19] |
Sun Y, Phillips PCB. Understanding the Fisher equation. J Appl Econom 2004; 19: 869-86.
https://doi.org/10.1002/jae.760
|
| [20] |
Danner D. Reliability - The Precision of a Measurement. GESIS Surv Guidel 2016.
https://doi.org/10.15465/gesis-sg
|
| [21] |
Fincham JE. Response rates and responsiveness for surveys, standards, and the Journal. Am J Pharm Educ 2008; 72: 43.
https://doi.org/10.5688/aj720243
|
| [22] |
Centers of disease control. Body mass index: Considerations for practitioners. Cdc 2011: 4.
|
| [23] |
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2021; 71: 209-49.
https://doi.org/10.3322/caac.21660
|
| [24] |
Hinata A, Kabasawa K, Watanabe Y, Kitamura K, Ito Y, Takachi R, et al. Education, household income, and depressive symptoms in middle-aged and older Japanese adults. BMC Public Health 2021; 21: 1-10.
https://doi.org/10.1186/s12889-021-12168-8
|
| [25] |
MoH-Kenya. Kenya STEPwise Survey for Non Communicable Diseases Risk Factors 2015 Report. Public Health 2015; 5: 8-210.
|
| [26] |
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40: 373-83.
https://doi.org/10.1016/0021-9681(87)90171-8
|
| [27] |
McQuade RM, Stojanovska V, Abalo R, Bornstein JC, Nurgali K. Chemotherapy-induced constipation and diarrhea: Pathophysiology, current and emerging treatments. Front Pharmacol 2016; 7: 1-14.
https://doi.org/10.3389/fphar.2016.00414
|
| [28] |
Nagy S, Petrosky SN, Beckler MD, Kesselman MM. The Impact of Modern Dietary Practices on Cancer Risk and Progression: A Systematic Review. Cureus 2023.
https://doi.org/10.7759/cureus.46639
|
| [29] |
Rock CL, Thomson C, Gansler T, Gapstur SM, Mccullough ML, Patel AV, et al. American Cancer Society Guideline for Diet and Physical Activity for Cancer Prevention 2020; 70: 245-71.
https://doi.org/10.3322/caac.21591
|
| [30] |
Gomes-Neto AW, Vliet IMY van, Osté MCJ, Jong MFC de, Bakker SJL, Jager-Wittenaar H, et al. Malnutrition Universal Screening Tool and Patient-Generated Subjective Global Assessment Short Form and their predictive validity in hospitalized patients. Clin Nutr ESPEN 2021; 45: 252-61.
https://doi.org/10.1016/j.clnesp.2021.08.015
|
| [31] |
Macdonald V. Oncology Corner Le coin de l’oncologie Chemotherapy: Managing side effects and safe handling. vol. 50. 2009.
|
Cite This Article
-
APA Style
Bundi, D., Ronoh, A., Sang, P. (2025). Nutrition Impact Symptoms, Dietary Patterns and Malnutrition Risk Among Adult Cancer Outpatients on Chemotherapy in Nyeri County Referral Hospital, Kenya. Journal of Food and Nutrition Sciences, 13(3), 189-200. https://doi.org/10.11648/j.jfns.20251303.19
 Copy
|
Copy
|
 Download
Download
ACS Style
Bundi, D.; Ronoh, A.; Sang, P. Nutrition Impact Symptoms, Dietary Patterns and Malnutrition Risk Among Adult Cancer Outpatients on Chemotherapy in Nyeri County Referral Hospital, Kenya. J. Food Nutr. Sci. 2025, 13(3), 189-200. doi: 10.11648/j.jfns.20251303.19
Copy
|
Download
AMA Style
Bundi D, Ronoh A, Sang P. Nutrition Impact Symptoms, Dietary Patterns and Malnutrition Risk Among Adult Cancer Outpatients on Chemotherapy in Nyeri County Referral Hospital, Kenya. J Food Nutr Sci. 2025;13(3):189-200. doi: 10.11648/j.jfns.20251303.19
Copy
|
Download
-
@article{10.11648/j.jfns.20251303.19,
author = {Dorothy Bundi and Amos Ronoh and Paul Sang},
title = {Nutrition Impact Symptoms, Dietary Patterns and Malnutrition Risk Among Adult Cancer Outpatients on Chemotherapy in Nyeri County Referral Hospital, Kenya
},
journal = {Journal of Food and Nutrition Sciences},
volume = {13},
number = {3},
pages = {189-200},
doi = {10.11648/j.jfns.20251303.19},
url = {https://doi.org/10.11648/j.jfns.20251303.19},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jfns.20251303.19},
abstract = {Cancer burden remain unacceptably high with global incidence of 19.3 Million and 10million cancer mortalities according to the 2020 global cancer estimates. There has been notable improvement in cancer care in Kenya with Chemotherapy being one of the most common and effective treatment modalities available. However, Chemotherapy is associated with Nutrition Impact Symptoms commonly referred to as the chemotherapy side effects, which include nausea, vomiting, sore throat and lack of appetite. However, the link between these side effects and dietary intake is not well studied. This study aimed at assessing the Nutrition Impact Symptoms and their contribution to the dietary intake and the nutrition status of cancer patients above 18 years of age, in Nyeri County Referral Hospital using analytical cross-sectional study design. A researcher administered questionnaire was used to collect data on the Nutrition Impact Symptoms, 24-hour recall and a Food Frequency Questionnaire was used to collect the dietary data and the Malnutrition Universal Screening Tool (MUST) was used to screen for the risk of malnutrition. Dietary data was analyzed using Nutri-Survey and the Statistical Package for the Social Sciences (SPSS). Sixty one percent of the respondents were female while 39% were male. Breast cancer was the most common cancer type in the population (39%), followed by esophageal and throat cancer at 14.5% and gastric cancer at 14%. Prostate cancer was the most prevalent among the male respondents at 11%. Nutrition Impact Symptoms that were reported include loss of appetite (72.1%), vomiting (55.8%), nausea (52.9%), diarrhea (39%), constipation (34.3%) and sore throat (8.1%), swallowing difficulties (0.6%), Pica (5.2%) and general body fatigue (9.3%). Unhealthy dietary patterns associated with the Nutrition Impact Symptoms include skipping meals, (69.2%), taking less than usual quantities of food than normal (71.5%), taking more food than normal quantities when not having side effects (8.7%), avoiding solid foods when symptoms are present (39%) and not eating at all 36.6%. Using the MUST, more than half (51.7%) of the respondents were at a high risk of developing malnutrition, followed by low risk (32.6%) with only 15.7% respondents being at a medium risk of malnutrition. Nutrition Impact Symptoms influence the dietary patterns of the cancer patients, which in turn contributes to the risk of malnourishment. Improving the Nutrition and health outcomes of cancer patients requires behavior change interventions that target the knowledge, attitude and practices of the patients towards the appropriate dietary patterns while on Chemotherapy.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Nutrition Impact Symptoms, Dietary Patterns and Malnutrition Risk Among Adult Cancer Outpatients on Chemotherapy in Nyeri County Referral Hospital, Kenya
AU - Dorothy Bundi
AU - Amos Ronoh
AU - Paul Sang
Y1 - 2025/06/23
PY - 2025
N1 - https://doi.org/10.11648/j.jfns.20251303.19
DO - 10.11648/j.jfns.20251303.19
T2 - Journal of Food and Nutrition Sciences
JF - Journal of Food and Nutrition Sciences
JO - Journal of Food and Nutrition Sciences
SP - 189
EP - 200
PB - Science Publishing Group
SN - 2330-7293
UR - https://doi.org/10.11648/j.jfns.20251303.19
AB - Cancer burden remain unacceptably high with global incidence of 19.3 Million and 10million cancer mortalities according to the 2020 global cancer estimates. There has been notable improvement in cancer care in Kenya with Chemotherapy being one of the most common and effective treatment modalities available. However, Chemotherapy is associated with Nutrition Impact Symptoms commonly referred to as the chemotherapy side effects, which include nausea, vomiting, sore throat and lack of appetite. However, the link between these side effects and dietary intake is not well studied. This study aimed at assessing the Nutrition Impact Symptoms and their contribution to the dietary intake and the nutrition status of cancer patients above 18 years of age, in Nyeri County Referral Hospital using analytical cross-sectional study design. A researcher administered questionnaire was used to collect data on the Nutrition Impact Symptoms, 24-hour recall and a Food Frequency Questionnaire was used to collect the dietary data and the Malnutrition Universal Screening Tool (MUST) was used to screen for the risk of malnutrition. Dietary data was analyzed using Nutri-Survey and the Statistical Package for the Social Sciences (SPSS). Sixty one percent of the respondents were female while 39% were male. Breast cancer was the most common cancer type in the population (39%), followed by esophageal and throat cancer at 14.5% and gastric cancer at 14%. Prostate cancer was the most prevalent among the male respondents at 11%. Nutrition Impact Symptoms that were reported include loss of appetite (72.1%), vomiting (55.8%), nausea (52.9%), diarrhea (39%), constipation (34.3%) and sore throat (8.1%), swallowing difficulties (0.6%), Pica (5.2%) and general body fatigue (9.3%). Unhealthy dietary patterns associated with the Nutrition Impact Symptoms include skipping meals, (69.2%), taking less than usual quantities of food than normal (71.5%), taking more food than normal quantities when not having side effects (8.7%), avoiding solid foods when symptoms are present (39%) and not eating at all 36.6%. Using the MUST, more than half (51.7%) of the respondents were at a high risk of developing malnutrition, followed by low risk (32.6%) with only 15.7% respondents being at a medium risk of malnutrition. Nutrition Impact Symptoms influence the dietary patterns of the cancer patients, which in turn contributes to the risk of malnourishment. Improving the Nutrition and health outcomes of cancer patients requires behavior change interventions that target the knowledge, attitude and practices of the patients towards the appropriate dietary patterns while on Chemotherapy.
VL - 13
IS - 3
ER -
Copy
|
Download