Aims and Objectives: The purpose of this study was to investigate the symptoms and quality of life level in patients after rectal cancer anus-preserving surgery, and to explore the factors affecting the quality of life level. In addition, a correlation analysis was conducted between symptoms and quality of life level. Background: Patients after rectal cancer anus-preserving surgery may have related complications, and the quality of life is also affected by various factors. It is particularly important to pay attention to and improve the quality of life of patients, so it is necessary to clarify the influencing factors and better clinical nursing intervention. Design: A cross-sectional study. Methods: From June 2020 to May 2022, a convenience sample of 165 participants were recruited at two tertiary hospitals in Guangdong, China. Quality of life and postoperative symptoms were assessed using the Cancer Patient Quality of Life Measurement Scale (FACT-G) and the Chinese Cancer Anderson Symptom Assessment Scale (MDASI) face-to-face or by telephone. Results: The overall quality of life score of patients after rectal cancer anus-preserving surgery was 54.07±14.58 points. The top three most severe symptoms were sleep, fatigue, and numbness or tingling in the limbs or face. The most severe gastrointestinal symptom was constipation. The severity of symptoms, gastrointestinal symptoms, and symptom interference were negatively moderately correlated with the total score of quality of life (P<0.01). The severity of symptoms, the severity of gastrointestinal symptoms, and the degree of symptom interference were independent factors affecting the quality of life of patients after RCAPS, with statistical significance (P<0.05). Conclusion: The quality of life of patients after rectal cancer anus-preserving surgery is at a medium level. The higher the severity of symptoms and symptom interference of patients after rectal cancer anus-preserving surgery, the lower the quality of life of patients. Relevance to clinical practice: To provide a theoretical basis for clinical nursing interventions for patients after rectal cancer anus-preserving surgery, so as to improve their quality of life.
| Published in | Journal of Surgery (Volume 13, Issue 1) |
| DOI | 10.11648/j.js.20251301.13 |
| Page(s) | 17-26 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Rectal Cancer Sphincter-Preserving Surgery, Quality of Life, Symptoms, Influencing Factors
Number of people | Percentage | |
|---|---|---|
Gender | ||
Female | 78 | 47.27% |
Male | 87 | 52.73% |
Age | ||
<60 | 90 | 54.55% |
≥60 | 75 | 45.45% |
Educational level | ||
Primary school and below | 60 | 36.36% |
Middle school or technical | 68 | 41.21% |
secondary school College or above | 37 | 22.42% |
Ethnicity | ||
Han ethnicity | 150 | 90.91% |
ethnic minorities | 15 | 9.09% |
Household registration type | ||
town | 136 | 82.42% |
countryside | 29 | 17.58% |
Marital Status | ||
Married | 147 | 89.09% |
Unmarried or divorced or widowed | 18 | 10.91% |
BMI | ||
Normal | 128 | 77.58% |
Overweight or obese | 37 | 22.42% |
Diabetes | ||
None | 138 | 83.64% |
Present | 27 | 16.36% |
Hypertension | ||
None | 133 | 80.61% |
Present | 32 | 19.39% |
Postoperative Stage | ||
3 months postoperative | 58 | 35.15% |
6 months postoperative | 52 | 31.52% |
9 months postoperative | 35 | 21.21% |
12 months postoperative | 20 | 12.12% |
Scale and dimensions | Mean ± Standard Deviation |
|---|---|
Quality of life scale | |
Physiological condition | 17.15±3.85 |
Social and family condition | 14.38±4.12 |
Emotional condition | 11.86±4.12 |
Functional condition | 10.68±4.73 |
Total score of quality of life | 54.07±14.58 |
Anderson Symptom Scale | |
Severity of Symptoms | 24.73±9.57 |
Severity of Gastrointestinal Symptoms | 12.58±4.01 |
Degree of interference | 14.98±5.74 |
Items | Average scores |
|---|---|
Symptom Items | |
Disturbed sleep | 3.99±2.18 |
Fatigue | 3.95±2.09 |
Numbness/tingling | 3.89±2.28 |
Difficulty remembering | 1.70±1.61 |
Sadness | 1.53±1.66 |
Vomiting | 1.37±1.53 |
Dry mouth | 1.29±1.51 |
Drowsiness | 1.27±1.25 |
Lack of appetite | 1.25±1.34 |
Distress/feeling upset | 1.23±1.38 |
Nausea | 1.19±1.57 |
Pain | 1.09±1.29 |
Shortness of breath | 1.04±1.39 |
Gastrointestinal Symptom Items | |
constipation | 4.42±1.62 |
diarrhea | 2.69±1.37 |
feeling bloated | 2.49±1.69 |
change in taste | 1.55±1.21 |
difficulty swallowing | 1.43±1.34 |
Interference Items | |
Enjoyment of life | 4.19±2.14 |
Working (including housework) | 3.54±1.74 |
Mood | 2.38±1.86 |
Activity | 2.22±1.80 |
Relations with other people | 1.38±1.19 |
Walking | 1.27±1.15 |
Variable | Assignment | |
|---|---|---|
Y | Quality of Life Total Score | Continuous Variable |
X1 | Gender | 1=Female, 2=Male |
X2 | Age | 1=<60 years old, 2=>60 years old |
X3 | Educational Level | 1=Elementary school or below, 2=Middle school/Technical school, 3=College/University or above |
X4 | BMI | 1=Normal, 2=Overweight or obese |
X5 | Diabetes | 1=No, 2=Yes |
X6 | Marital Status | 1=Married, 2=Unmarried/Divorced/Widowed |
X6 | Postoperative Stage | 1=3 months, 2=6 months, 3=9 months, 4=12 months |
X7 | Severity of Symptoms | Continuous Variable |
X8 | Severity of Gastrointestinal Symptoms | Continuous Variable |
X9 | Interference of Symptoms | Continuous Variable |
Variables | β | Standard Error | t | P | 95%CI |
|---|---|---|---|---|---|
Gender | |||||
Female | 0.00 | reference | |||
Male | 4.09 | 1.48 | 2.767 | 0.006 | 1.19,6.99 |
Age Group | |||||
<60 | 0.00 | reference | |||
≥60 | -5.81 | 1.64 | -3.544 | 0.001 | -9.03,-2.60 |
Education Level | |||||
Elementary school or below | 0.00 | reference | |||
Middle school or technical secondary school | 3.00 | 1.69 | 1.777 | 0.078 | -0.31,6.30 |
College or above | 6.79 | 2.08 | 3.267 | 0.001 | 2.72,10.87 |
Marital Status | |||||
Married | 0.00 | reference | |||
Unmarried or divorced or widowed | -8.28 | 2.41 | -3.431 | 0.001 | -13.01,-3.55 |
BMI | |||||
Normal | 0.00 | reference | |||
Overweight or obese | -5.41 | 1.80 | -3.001 | 0.003 | -8.95,-1.88 |
Diabetes | |||||
None | 0.00 | reference | |||
Present | -8.30 | 2.08 | -3.996 | 0.000 | -12.37,-4.23 |
Postoperative Stage | |||||
3 months postoperative | 0.00 | reference | |||
6 months postoperative | 1.05 | 1.76 | 0.594 | 0.554 | -2.41,4.51 |
9 months postoperative | 2.41 | 2.01 | 1.196 | 0.234 | -1.54,6.35 |
12 months postoperative | 6.31 | 2.47 | 2.552 | 0.012 | 1.46,11.15 |
Severity of Symptoms | -0.29 | 0.09 | -3.123 | 0.002 | -0.47,-0.11 |
Severity of gastrointestinal symptoms | -0.52 | 0.22 | -2.391 | 0.018 | -0.95,-0.09 |
Degree of interference caused by symptoms | -0.39 | 0.15 | -2.644 | 0.009 | -0.68,-0.10 |
BMI | Body Mass Index |
FACT-G | Functional Assessment of Cancer Therapy-Generic Scale |
LARS | Low Anterior Resection Syndrome |
MDASI-GI | M.D. Anderson Symptom Inventory-Gastrointestinal Cancer Module |
QOL | Quality of Life |
RC | Rectal Cancer |
TME | Totalmesorectalexcision |
| [1] | CA: 2015 China Cancer Statistics Released [J]. Chinese Medical Innovation, 2016, 13(05): 6. |
| [2] | Sakr A, Sauri F, Alessa M, et al. Assessment and management of low anterior resection syndrome after sphincter preserving surgery for rectal cancer. Chinese medical journal. 2020; 133(15): 1824-1833. |
| [3] | Seow W, Dudi-Venkata NN, Bedrikovetski S, Kroon HM, Sammour T. Outcomes of open vs laparoscopic vs robotic vs transanal total mesorectal excision (TME) for rectal cancer: a network meta-analysis. Techniques in coloproctology. 2023; 27(5): 345-360. |
| [4] | Peng Lijie, Li Guosheng. Research progress on low anterior resection syndrome after sphincter-preserving surgery for rectal cancer [J]. Journal of Medical Research, 2021, 50(04): 13-16. |
| [5] | Liu Hanmei. Factors influencing self-management of intestinal symptoms in patients after sphincter-preserving surgery for rectal cancer and countermeasures [D]. Zunyi Medical University, 2018. |
| [6] | Mahalingam S, Seshadri RA, Veeraiah S. Long-Term Functional and Oncological Outcomes Following Intersphincteric Resection for Low Rectal Cancers. Indian journal of surgical oncology. 2017; 8(4): 457-461. |
| [7] | King, Madeleine T et al. “The Functional Assessment of Cancer Therapy Eight Dimension (FACT-8D), a Multi-Attribute Utility Instrument Derived From the Cancer-Specific FACT-General (FACT-G) Quality of Life Questionnaire: Development and Australian Value Set.” Value in health: the journal of the International Society for Pharmacoeconomics and Outcomes Research vol. 24, 6 (2021): 862-873. |
| [8] | Xu, Rui et al. “Patient-reported gastrointestinal symptoms following surgery for gastric cancer and the relative risk factors.” Frontiers in oncology vol. 12 951485. 14 Sep. 2022, |
| [9] | de Vet HCW, Mokkink LB, Mosmuller DG, Terwee CB. Spearman-Brown prophecy formula and Cronbach's alpha: different faces of reliability and opportunities for new applications. J Clin Epidemiol. 2017; 85: 45-49. |
| [10] | Wang Ping, Xia Ping, Wang Yingchun. Correlation analysis of postoperative intestinal symptoms, self-management behaviors, and quality of life in patients with low rectal cancer [J]. Nursing Practice and Research, 2020, 17(06): 14-16. |
| [11] | Zhang Jiahui, Yu Mingwei, Wang Xiaomin, et al. Clinical observation of traditional Chinese medicine improving the quality of life in patients with triple-negative breast cancer after surgery [J]. Journal of Beijing University of Traditional Chinese Medicine, 2022, 45(11): 1095-1102. |
| [12] | Bi Cen, Jing Liwei, Zou Shengqiang, et al. Correlation study between early postoperative symptom cluster and quality of life in patients with esophageal cancer [J]. Nursing Research, 2022, 36(20): 3614-3618. |
| [13] | Zhang Hua, Gu Fan, Dong Yinfeng, et al. Correlation study on symptom cluster and quality of life in patients with gastric cancer [J]. Chongqing Medicine, 2016, 45(32): 4593-4596. |
| [14] | Mu Qianqian, Yu Chunhua, Li Junying. Survey on the current status of psychological distress in newly diagnosed lung cancer patients and analysis of related factors [J]. Journal of Peking University (Medical Edition), 2016, 48(03): 507-514. |
| [15] | Qi, Wenqian et al. “Spiritual Coping in Family Caregivers of Patients With Advanced Cancer: A Cross-Sectional Study.” Journal of pain and symptom management vol. 67, 3 (2024): e177-e184. |
| [16] | Benitez Majano, Sara et al. “Mental Health Morbidities and Time to Cancer Diagnosis Among Adults With Colon Cancer in England.” JAMA network open vol. 5, 10 e2238569. 3 Oct. 2022, |
| [17] | Hofmeister, Dirk et al. “Sleep problems in cancer patients: a comparison between the Jenkins Sleep Scale and the single-item sleep scale of the EORTC QLQ-C30.” Sleep medicine vol. 71 (2020): 59-65. |
| [18] | Balachandran, Diwakar D et al. “Evaluation and Management of Sleep and Circadian Rhythm Disturbance in Cancer.” Current treatment options in oncology vol. 22, 9 81. 2 Jul. 2021, |
| [19] | Battersby, Nick J et al. “Predicting the Risk of Bowel-Related Quality-of-Life Impairment After Restorative Resection for Rectal Cancer: A Multicenter Cross-Sectional Study.” Diseases of the colon and rectum vol. 59, 4 (2016): 270-80. |
| [20] | Yennurajalingam, Sriram et al. “Association between Daytime Activity, Fatigue, Sleep, Anxiety, Depression, and Symptom Burden in Advanced Cancer Patients: A Preliminary Report.” Journal of palliative medicine vol. 19, 8 (2016): 849-56. |
| [21] | Xu Guoxi, Liu Weibo, Wang Canyang, et al. The impact of aerobic exercise on cancer-related fatigue and quality of life in patients receiving adjuvant chemotherapy for colorectal cancer [J]. Modern Oncology Medicine, 2016, 24(14): 2259-2261. |
| [22] | Zhang Xiaoyun, Sun Jing, Liu Jinying. Adequate nutritional support improves cancer-related fatigue and nutritional status in patients undergoing tumor chemotherapy [J]. Modern Oncology Medicine, 2021, 29(16): 2887-2890. |
| [23] | Su Xiaofeng, Wang Jin, Wang Yun, et al. Systematic review of the application of positive psychological intervention in fatigue symptoms of cancer patients [J]. Journal of Yan'an University (Medical Sciences), 2021, 19(03): 100-104. |
| [24] | Bonhof, C S et al. “Painful and non-painful chemotherapy-induced peripheral neuropathy and quality of life in colorectal cancer survivors: results from the population-based PROFILES registry.” Supportive care in cancer: official journal of the Multinational Association of Supportive Care in Cancer vol. 28, 12 (2020): 5933-5941. |
| [25] | Bray, Victoria J et al. “Systematic review of self-reported cognitive function in cancer patients following chemotherapy treatment.” Journal of cancer survivorship: research and practice vol. 12, 4 (2018): 537-559. |
| [26] | El-Fatatry, Basma Mahrous et al. “Role of metformin in oxaliplatin-induced peripheral neuropathy in patients with stage III colorectal cancer: randomized, controlled study.” International journal of colorectal disease vol. 33, 12 (2018): 1675-1683. |
| [27] | Liu Xueying, Liang Bing. Analysis of factors related to postoperative bowel dysfunction in patients with laparoscopic rectal cancer-preserving surgery. Henan Journal of Surgery, 2023, 29(01): 105-107. |
| [28] | Li Ji, Zhou Shiyun. Observation of postoperative bowel function and analysis of related influencing factors in patients with low rectal cancer undergoing laparoscopic-assisted transanal total mesorectal excision. Practical Cancer Journal, 2022, 37(03): 471-473. |
| [29] | Li Hui, Yao Cui, Feng Yifei, et al. Influence of individualized biofeedback training combined with early defecation function training on intestinal function, anorectal dynamics, and quality of life in patients with low rectal cancer after sphincter-preserving surgery. Modern Advances in Biomedicine, 2022, 22(19): 3660-3664. |
| [30] | Huang Shaoqing. Clinical study on the treatment of postoperative diarrhea in rectal cancer with Yiqi Qingre Jiedu Decoction combined with montmorillonite powder. New Chinese Medicine, 2023, 55(04): 130-134. |
| [31] | Liu Weixia. Retrospective study on acute diarrhea after colorectal cancer surgery. China Medical University, 2018. |
| [32] | De Felice, Francesca et al. “Locally Advanced Rectal Cancer: Treatment Approach in Elderly Patients.” Current treatment options in oncology vol. 21, 1 1. 11 Jan. 2020, |
APA Style
Wei, X., Zeng, Y., Zhang, Z., Deng, M. (2025). Factors Influencing Quality of Life in Patients After Rectal Cancer Anus-Preserving Surgery: A Cross-Sectional Study. Journal of Surgery, 13(1), 17-26. https://doi.org/10.11648/j.js.20251301.13
ACS Style
Wei, X.; Zeng, Y.; Zhang, Z.; Deng, M. Factors Influencing Quality of Life in Patients After Rectal Cancer Anus-Preserving Surgery: A Cross-Sectional Study. J. Surg. 2025, 13(1), 17-26. doi: 10.11648/j.js.20251301.13
@article{10.11648/j.js.20251301.13,
author = {Xiuli Wei and Yue Zeng and Zitao Zhang and Minping Deng},
title = {Factors Influencing Quality of Life in Patients After Rectal Cancer Anus-Preserving Surgery: A Cross-Sectional Study
},
journal = {Journal of Surgery},
volume = {13},
number = {1},
pages = {17-26},
doi = {10.11648/j.js.20251301.13},
url = {https://doi.org/10.11648/j.js.20251301.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.js.20251301.13},
abstract = {Aims and Objectives: The purpose of this study was to investigate the symptoms and quality of life level in patients after rectal cancer anus-preserving surgery, and to explore the factors affecting the quality of life level. In addition, a correlation analysis was conducted between symptoms and quality of life level. Background: Patients after rectal cancer anus-preserving surgery may have related complications, and the quality of life is also affected by various factors. It is particularly important to pay attention to and improve the quality of life of patients, so it is necessary to clarify the influencing factors and better clinical nursing intervention. Design: A cross-sectional study. Methods: From June 2020 to May 2022, a convenience sample of 165 participants were recruited at two tertiary hospitals in Guangdong, China. Quality of life and postoperative symptoms were assessed using the Cancer Patient Quality of Life Measurement Scale (FACT-G) and the Chinese Cancer Anderson Symptom Assessment Scale (MDASI) face-to-face or by telephone. Results: The overall quality of life score of patients after rectal cancer anus-preserving surgery was 54.07±14.58 points. The top three most severe symptoms were sleep, fatigue, and numbness or tingling in the limbs or face. The most severe gastrointestinal symptom was constipation. The severity of symptoms, gastrointestinal symptoms, and symptom interference were negatively moderately correlated with the total score of quality of life (P. Conclusion: The quality of life of patients after rectal cancer anus-preserving surgery is at a medium level. The higher the severity of symptoms and symptom interference of patients after rectal cancer anus-preserving surgery, the lower the quality of life of patients. Relevance to clinical practice: To provide a theoretical basis for clinical nursing interventions for patients after rectal cancer anus-preserving surgery, so as to improve their quality of life.
},
year = {2025}
}
TY - JOUR T1 - Factors Influencing Quality of Life in Patients After Rectal Cancer Anus-Preserving Surgery: A Cross-Sectional Study AU - Xiuli Wei AU - Yue Zeng AU - Zitao Zhang AU - Minping Deng Y1 - 2025/01/23 PY - 2025 N1 - https://doi.org/10.11648/j.js.20251301.13 DO - 10.11648/j.js.20251301.13 T2 - Journal of Surgery JF - Journal of Surgery JO - Journal of Surgery SP - 17 EP - 26 PB - Science Publishing Group SN - 2330-0930 UR - https://doi.org/10.11648/j.js.20251301.13 AB - Aims and Objectives: The purpose of this study was to investigate the symptoms and quality of life level in patients after rectal cancer anus-preserving surgery, and to explore the factors affecting the quality of life level. In addition, a correlation analysis was conducted between symptoms and quality of life level. Background: Patients after rectal cancer anus-preserving surgery may have related complications, and the quality of life is also affected by various factors. It is particularly important to pay attention to and improve the quality of life of patients, so it is necessary to clarify the influencing factors and better clinical nursing intervention. Design: A cross-sectional study. Methods: From June 2020 to May 2022, a convenience sample of 165 participants were recruited at two tertiary hospitals in Guangdong, China. Quality of life and postoperative symptoms were assessed using the Cancer Patient Quality of Life Measurement Scale (FACT-G) and the Chinese Cancer Anderson Symptom Assessment Scale (MDASI) face-to-face or by telephone. Results: The overall quality of life score of patients after rectal cancer anus-preserving surgery was 54.07±14.58 points. The top three most severe symptoms were sleep, fatigue, and numbness or tingling in the limbs or face. The most severe gastrointestinal symptom was constipation. The severity of symptoms, gastrointestinal symptoms, and symptom interference were negatively moderately correlated with the total score of quality of life (P. Conclusion: The quality of life of patients after rectal cancer anus-preserving surgery is at a medium level. The higher the severity of symptoms and symptom interference of patients after rectal cancer anus-preserving surgery, the lower the quality of life of patients. Relevance to clinical practice: To provide a theoretical basis for clinical nursing interventions for patients after rectal cancer anus-preserving surgery, so as to improve their quality of life. VL - 13 IS - 1 ER -
Department of Gastrointestinal Surgery, First Affiliated Hospital of Jinan University, Guangzhou, China
Luohu Hospital Group Yijing Community Health Service Center, Shenzhen, China
Department of Gastrointestinal Surgery, First Affiliated Hospital of Jinan University, Guangzhou, China
Department of Nursing Department, Fifth Affiliated Hospital of Jinan University, Heyuan, China
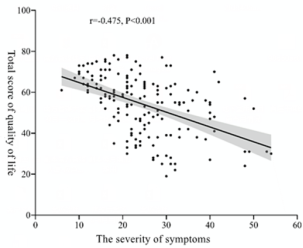
Figure 1. Scatter plot of the correlation analysis between the severity of symptoms and quality of life.
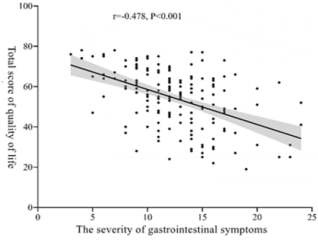
Figure 2. Scatter plot of the correlation analysis between the severity of gastrointestinal symptoms and quality of life.
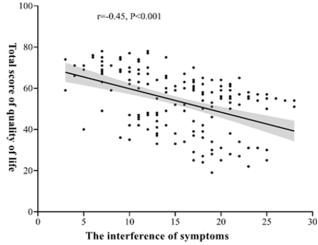
Figure 3. Scatter plot of the correlation analysis between the interference of symptoms and quality of life.
Information

