Diabetic foot disease is one of the most severe complications of diabetes mellitus due to its strong association with ulceration, infection, lower-limb amputation, and increased mortality. In the Dominican Republic and the Caribbean, this burden is further intensified by limited access to early screening technologies and the need for robust, field-deployable solutions adapted to resource-constrained healthcare environments. The objective of this study is to propose a fully analog, discrete-electronics screening device for early neuroischemic diabetic-foot risk assessment. The proposed system integrates two complementary physiological biomarkers: bilateral plantar thermal asymmetry, as an indicator of localized inflammatory stress, and post-occlusive microvascular reactivity, assessed through hyperemic time-to-peak using reflective photoplethysmography. The architecture is based on a hardware-only design that eliminates the need for software, microcontrollers, or digital signal processing, and includes multisite plantar temperature sensing, optical perfusion measurement with synchronous demodulation, a controlled vascular occlusion module, and comparator-based risk classification. This design enables deterministic behavior, direct signal traceability, and local interpretability, which are essential for screening applications in low-infrastructure settings. The main contribution of this work lies in the integration of inflammatory and vascular physiological domains within a single discrete-electronics platform. Unlike existing approaches that rely on digitally mediated systems, the proposed method provides a transparent and resilient alternative for early screening. The study is presented as a design-and-rationale framework with a defined validation pathway, providing a foundation for prototype development, experimental validation, and potential clinical application.
| Published in | Science Discovery Health (Volume 1, Issue 2) |
| DOI | 10.11648/j.sdh.20260102.13 |
| Page(s) | 67-78 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Diabetic Foot, Photoplethysmography, Reactive Hyperemia, Microvascular Dysfunction
Approach / Technology Type | Main Physiological Variable(s) | Typical Technological Dependency | Active Vascular Challenge | Local Standalone Interpretation | Suitability for Low-Infrastructure Settings | Main Limitation |
|---|---|---|---|---|---|---|
Remote plantar temperature monitoring socks | Temperature | Embedded electronics, digital logging, often app/platform support | No | Usually limited | Moderate | Temperature-only approach |
Smart insoles / connected plantar platforms | Pressure, temperature, activity | Microcontroller-based, digital processing, connectivity | No | Variable | Moderate to low | Higher complexity and maintenance burden |
Infrared thermography systems | Surface temperature mapping | Imaging hardware, digital processing, interpretation software | No | Limited without trained analysis | Low to moderate | Higher cost and weaker portability |
Optical perfusion systems | Perfusion / hemodynamics | Often digitally processed optical instrumentation | Sometimes | Rarely | Low to moderate | Complexity and cost |
Multifactorial digital diabetic-foot platforms | Temperature, pressure, adherence, activity | Strong software and platform dependence | Usually no | Rarely | Low in constrained settings | High ecosystem dependence |
Proposed analog discrete multimodal device | Thermal asymmetry + post-occlusive hyperemic time-to-peak | Discrete analog electronics, no software, no microcontroller | Yes | Yes | High | Requires experimental validation and threshold calibration |
Design Domain | Requirement | Engineering Rationale | Expected Target / Working Objective |
|---|---|---|---|
Clinical purpose | Early screening of neuroischemic diabetic-foot risk | The device is intended for screening and triage, not definitive diagnosis | Three-level local risk output: green / yellow / red |
Operating philosophy | Fully analog, software-free, microcontroller-free architecture | To maximize hardware transparency, direct verifiability, and resilience in constrained settings | No firmware, no embedded OS, no cloud dependency |
Thermal sensing | Bilateral multisite plantar temperature comparison | Focal asymmetry is more clinically informative than isolated absolute temperature | At least 3 bilateral plantar sites; expandable to 5–6 pairs |
Thermal output variable | Maximum bilateral thermal asymmetry | Screening should emphasize focal inflammatory burden | ST=max(∣ΔT1∣,∣ΔT2∣,…,∣ΔTn∣) |
Thermal stability | Repeatable differential acquisition under stable contact conditions | Reduces false interpretation from sensor drift | Stable bilateral differential output during fixed baseline interval |
Optical sensing | Reflective infrared perfusion acquisition | Provides a noninvasive surrogate of local vascular behavior | Infrared LED + photodiode reflective channel |
Optical robustness | Ambient-light-tolerant acquisition | Field deployment requires resistance to uncontrolled illumination | Synchronous demodulation or equivalent analog rejection strategy |
Post-occlusive challenge | Brief, controlled vascular occlusion with reproducible release | Enables functional assessment beyond static perfusion | Short standardized occlusion interval followed by timed release |
Vascular output variable | Hyperemic time-to-peak | Simple and physiologically interpretable recovery marker | |
Peak detection | Analog identification of post-release perfusion maximum | Must remain consistent with non-digital design philosophy | Derivative-based peak detection with comparator logic |
Basal signal adequacy | Minimum acceptable pulsatile optical amplitude | Reduces false classification from poor optical coupling | Comparator-based minimum pulse-quality check |
Risk integration | Local hardware combination of thermal and vascular markers | Intended to preserve interpretability and immediate usability | Weighted threshold logic implemented with analog comparators |
User interface | Immediate local screening display | Supports point-of-care or outreach use | Green / yellow / red indicator plus optional numeric timing output |
Portability | Operation in low-infrastructure environments | Relevant for the Dominican Republic and Caribbean outreach settings | Battery-compatible, self-contained unit |
Maintainability | Local serviceability with conventional components | Important for long-term deployment outside high-complexity infrastructures | Use of widely available analog and CMOS components |
Calibration | Manual or semi-manual local adjustment | Necessary for discrete-electronics reproducibility | Threshold trimming and baseline calibration at hardware level |
Safety positioning | Noninvasive screening device | Avoids overstating maturity or regulatory class | Pre-diagnostic screening and referral support only |
Validation path | Bench, feasibility, and pilot clinical stages | Manuscript is design-stage, so validation must be staged | Bench characterization → healthy feasibility → pilot diabetic cohort |
Translational goal | Suitability for primary care, community campaigns, and academic prototyping | Aligns the engineering concept with regional health-system realities | Usable in screening, teaching, and prototype-driven translational research |
Technology Category | Main Biomarker(s) | Typical System Architecture | Dependence on Software / Embedded Processing | Active Functional Challenge | Local Interpretability | Suitability for Resource-Constrained Settings | Key Limitation Relative to the Proposed System |
|---|---|---|---|---|---|---|---|
Plantar temperature monitoring socks | Local temperature | Wearable digital textile or sock-based platform | High | No | Moderate | Moderate | Typically limited to thermal monitoring alone |
Smart insoles / connected plantar platforms | Pressure, temperature, activity | Embedded sensor array with digital acquisition | High | No | Moderate | Moderate to low | Greater technological dependency and higher system complexity |
Infrared thermography systems | Surface thermal distribution | Imaging-based digital platform | High | No | Low to moderate without trained interpretation | Low to moderate | High equipment cost and reduced portability |
Optical perfusion assessment systems | Perfusion, blood-flow-related optical signals | Optical instrumentation, usually digitally processed | Moderate to high | Sometimes | Moderate | Low to moderate | Often not optimized for simple local screening workflows |
Multifactorial digital diabetic-foot systems | Temperature, pressure, adherence, activity, remote monitoring | Connected digital ecosystem | High | Usually no | Variable | Low in infrastructurally constrained settings | Strong ecosystem dependence and maintenance burden |
Post-occlusive vascular laboratory methods | Reactive hyperemia, vascular recovery | Specialized vascular testing environment | Moderate to high | Yes | Moderate | Low | Limited portability and low field suitability |
Proposed analog discrete multimodal system | Plantar thermal asymmetry + post-occlusive hyperemic time-to-peak + basal pulse adequacy | Fully analog, discrete-electronics local screening platform | None | Yes | High | High | Requires staged validation and threshold calibration |
PPG | Photoplethysmography |
T_peak | Time to Peak Hyperemia |
S_T | Thermal Asymmetry Indicator |
PAD | Peripheral Arterial Disease |
| [1] | Ahmad, M., Patel, K., Davies, A. H., & Shalhoub, J. (2024). Noninvasive optical methods to assess tissue perfusion in patients with peripheral arterial disease and diabetes mellitus: A scoping review and discussion. JVS-Vascular Insights, 2 (Suppl. A), 100034. |
| [2] | Allen, J. (2007). Photoplethysmography and its application in clinical physiological measurement. Physiological Measurement, 28(3), R1–R39. |
| [3] | Armstrong, D. G., Boulton, A. J. M., & Bus, S. A. (2017). Diabetic foot ulcers and their recurrence. The New England Journal of Medicine, 376(24), 2367–2375. |
| [4] | Bagavathiappan, S., Philip, J., Jayakumar, T., Raj, B., Rao, P. N. S., Varalakshmi, M., & Mohan, V. (2010). Infrared thermal imaging for diabetic neuropathy diagnosis. Diabetes Technology & Therapeutics, 12(8), 615–621. |
| [5] | Balasubramanian, G., Chittoria, R. K., Singh, A. K., & Jha, A. K. (2021). Evaluation of cutaneous microcirculation in diabetic foot using post-occlusive reactive hyperemia. Microcirculation, 28(6), e12692. |
| [6] | Beach, C., Krach, M. R., Perinpanayagam, S., & Wafai, L. (2021). Monitoring dynamic plantar temperatures in diabetes. Sensors, 21(5), 1717. |
| [7] | Billings, J., Gee, J., Ghulam, Z., & Abdullah, H. A. (2024). Smart compression sock for diabetic foot ulcer detection. Sensors, 24(21), 6928. |
| [8] | Bus, S. A., et al. (2021). Home monitoring of foot skin temperature to prevent ulcer recurrence. BMJ Open Diabetes Research & Care, 9(1), e002392. |
| [9] | Doulamis, A., et al. (2021). Photonics-based monitoring of diabetic foot ulcers. Bioengineering, 8(2), 27. |
| [10] | Ferguson, T. S., et al. (2013). Diabetic foot complications in Jamaica. West Indian Medical Journal, 62(3), 216–223. |
| [11] | Hambleton, I. R., et al. (2009). Mortality after diabetes-related amputation in the Caribbean. Diabetes Care, 32(2), 306–307. |
| [12] | Hennis, A. J. M., et al. (2004). Risk of amputation in Caribbean populations. Diabetes Care, 27(11), 2636–2641. |
| [13] | International Diabetes Federation. (2025). IDF diabetes atlas (11th ed.). |
| [14] | Islam, S., et al. (2013). Epidemiology of diabetic foot infections in the Caribbean. The Permanente Journal, 17(2), 37–40. |
| [15] | Kabbani, M., et al. (2013). Microcirculation in diabetic foot. Microvascular Research, 87, 1–6. |
| [16] | Lanting, S. M., et al. (2017). Reactive hyperemia in diabetic foot. Microvascular Research, 115, 51–56. |
| [17] | Lavery, L. A., et al. (2004). Home temperature monitoring to prevent ulcers. Diabetes Care, 27(11), 2642–2647. |
| [18] | Lovell, L., Dunkley, A., Gaskin, P., & Reid, M. (2023). Diabetic foot ulceration in Barbados. International Wound Journal, 20(4), 935–941. |
| [19] | Lovell, L., et al. (2025). Diabetic foot in Afro-Caribbean populations. International Journal of Environmental Research and Public Health, 22(2), 304. |
| [20] | Dalporto, B. A. L., Mary, S., & Gallur, S. (2026). The importance of discrete electronics in biomedical applications: reliability, verifiability, and technological resilience in critical healthcare systems. LATAM Revista Latino-americana de Ciencias Sociales y Humanidades, 7(1), 3149–3155. |
| [21] | Martín-Vaquero, J., et al. (2019). Wearable temperature monitoring in diabetic patients. Sensors, 19, 776. |
| [22] | Matijevich, E., et al. (2024). Digital health solutions for diabetic foot syndrome. Sensors, 24(9), 2675. |
| [23] | Mejias, S. G., & Ramphul, K. (2018). Peripheral arterial disease in diabetic patients in Santo Domingo. Archives of Medical Science, 3, e35–e40. |
| [24] | Monteiro-Soares, M., et al. (2023). IWGDF guidelines on prevention of diabetic foot ulcers. Diabetes/Metabolism Research and Reviews. |
| [25] | Pan American Health Organization. (2024). Dominican Republic health profile. |
| [26] | Pan American Health Organization. (2025). Diabetes in the Americas. |
| [27] | Pan American Health Organization. (2025). NCDs at a glance 2025. |
| [28] | Reyzelman, A. M., et al. (2018). Temperature-monitoring socks. Journal of Diabetes Science and Technology, 12(5), 1004–1009. |
| [29] | Reyzelman, A. M., et al. (2022). Real-world smart sock evaluation. Journal of Diabetes Science and Technology, 16(5), 1077–1084. |
| [30] | Rosell-Diago, M. P., et al. (2024). Thermal and pressure analysis in diabetic foot. Applied Sciences, 14(19), 8726. |
| [31] | Schaper, N. C., et al. (2024). IWGDF guidelines update. Diabetes/Metabolism Research and Reviews. |
| [32] | Shih, C. D., et al. (2024). Remote temperature monitoring program. JMIR Diabetes, 9, e46096. |
| [33] | Taylor, C. G., et al. (2014). Diabetic foot burden in Barbados. The Lancet Diabetes & Endocrinology, 2(1), 39–40. |
| [34] | Walrond, E. R. (2001). Caribbean diabetic foot management. West Indian Medical Journal, 50(Suppl. 1), 24–26. |
| [35] | World Health Organization. (2018). Dominican Republic NCD profile. |
| [36] | World Health Organization. (2024). Dominican Republic country profile. |
| [37] | Yamamoto-Suganuma, R., et al. (2009). Hyperemia and vascular disease in diabetes. Diabetic Medicine, 26(11), 1151–1157. |
| [38] | Zequera, M., et al. (2024). Plantar temperature and pressure distribution. Sensors, 24(17), 5579. |
APA Style
Dalporto, B. A. L., Mary, S., Gallur, S. (2026). Analog Multimodal Device for Early Neuroischemic Diabetic Foot Screening. Science Discovery Health, 1(2), 67-78. https://doi.org/10.11648/j.sdh.20260102.13
ACS Style
Dalporto, B. A. L.; Mary, S.; Gallur, S. Analog Multimodal Device for Early Neuroischemic Diabetic Foot Screening. Sci. Discov. Health 2026, 1(2), 67-78. doi: 10.11648/j.sdh.20260102.13
@article{10.11648/j.sdh.20260102.13,
author = {Baldo Alberto Luigi Dalporto and Sabine Mary and Santiago Gallur},
title = {Analog Multimodal Device for Early Neuroischemic Diabetic Foot Screening},
journal = {Science Discovery Health},
volume = {1},
number = {2},
pages = {67-78},
doi = {10.11648/j.sdh.20260102.13},
url = {https://doi.org/10.11648/j.sdh.20260102.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sdh.20260102.13},
abstract = {Diabetic foot disease is one of the most severe complications of diabetes mellitus due to its strong association with ulceration, infection, lower-limb amputation, and increased mortality. In the Dominican Republic and the Caribbean, this burden is further intensified by limited access to early screening technologies and the need for robust, field-deployable solutions adapted to resource-constrained healthcare environments. The objective of this study is to propose a fully analog, discrete-electronics screening device for early neuroischemic diabetic-foot risk assessment. The proposed system integrates two complementary physiological biomarkers: bilateral plantar thermal asymmetry, as an indicator of localized inflammatory stress, and post-occlusive microvascular reactivity, assessed through hyperemic time-to-peak using reflective photoplethysmography. The architecture is based on a hardware-only design that eliminates the need for software, microcontrollers, or digital signal processing, and includes multisite plantar temperature sensing, optical perfusion measurement with synchronous demodulation, a controlled vascular occlusion module, and comparator-based risk classification. This design enables deterministic behavior, direct signal traceability, and local interpretability, which are essential for screening applications in low-infrastructure settings. The main contribution of this work lies in the integration of inflammatory and vascular physiological domains within a single discrete-electronics platform. Unlike existing approaches that rely on digitally mediated systems, the proposed method provides a transparent and resilient alternative for early screening. The study is presented as a design-and-rationale framework with a defined validation pathway, providing a foundation for prototype development, experimental validation, and potential clinical application.},
year = {2026}
}
TY - JOUR T1 - Analog Multimodal Device for Early Neuroischemic Diabetic Foot Screening AU - Baldo Alberto Luigi Dalporto AU - Sabine Mary AU - Santiago Gallur Y1 - 2026/05/19 PY - 2026 N1 - https://doi.org/10.11648/j.sdh.20260102.13 DO - 10.11648/j.sdh.20260102.13 T2 - Science Discovery Health JF - Science Discovery Health JO - Science Discovery Health SP - 67 EP - 78 PB - Science Publishing Group SN - 3142-9041 UR - https://doi.org/10.11648/j.sdh.20260102.13 AB - Diabetic foot disease is one of the most severe complications of diabetes mellitus due to its strong association with ulceration, infection, lower-limb amputation, and increased mortality. In the Dominican Republic and the Caribbean, this burden is further intensified by limited access to early screening technologies and the need for robust, field-deployable solutions adapted to resource-constrained healthcare environments. The objective of this study is to propose a fully analog, discrete-electronics screening device for early neuroischemic diabetic-foot risk assessment. The proposed system integrates two complementary physiological biomarkers: bilateral plantar thermal asymmetry, as an indicator of localized inflammatory stress, and post-occlusive microvascular reactivity, assessed through hyperemic time-to-peak using reflective photoplethysmography. The architecture is based on a hardware-only design that eliminates the need for software, microcontrollers, or digital signal processing, and includes multisite plantar temperature sensing, optical perfusion measurement with synchronous demodulation, a controlled vascular occlusion module, and comparator-based risk classification. This design enables deterministic behavior, direct signal traceability, and local interpretability, which are essential for screening applications in low-infrastructure settings. The main contribution of this work lies in the integration of inflammatory and vascular physiological domains within a single discrete-electronics platform. Unlike existing approaches that rely on digitally mediated systems, the proposed method provides a transparent and resilient alternative for early screening. The study is presented as a design-and-rationale framework with a defined validation pathway, providing a foundation for prototype development, experimental validation, and potential clinical application. VL - 1 IS - 2 ER -
Department of Electrical Engineering, Instituto Tecnológico de Santo Domingo (INTEC), Santo Domingo, Dominican Republic
Department of Humanidades, Instituto Tecnológico de Santo Domingo (INTEC), Santo Domingo, Dominican Republic
Department of Humanidades, Instituto Tecnológico de Santo Domingo (INTEC), Santo Domingo, Dominican Republic
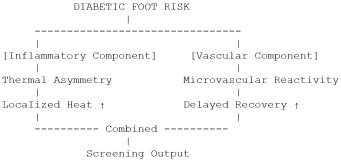
Figure 1. Physiological rationale of the proposed multimodal screening approach.
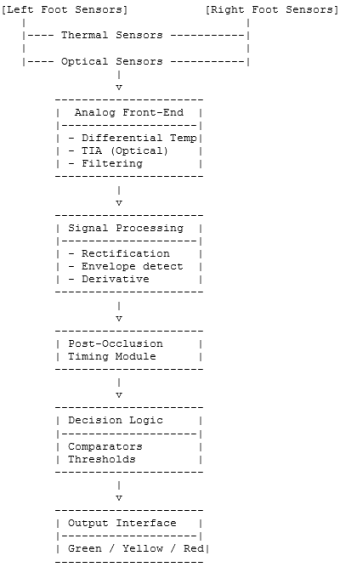
Figure 2. Global architecture of the proposed analog discrete screening system.
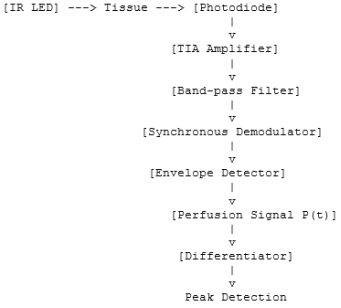
Figure 3. Analog signal-processing chain of the reflective optical subsystem.
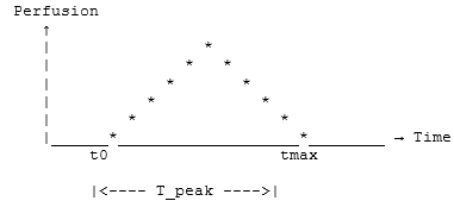
Figure 4. Idealized temporal profile of post-occlusive reactive hyperemia. After cuff release at time t₀, perfusion increases to a peak at tmax.
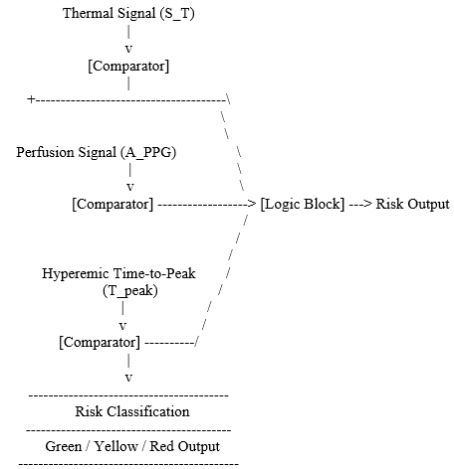
Figure 5. Hardware-based decision logic of the proposed screening system.
Information

