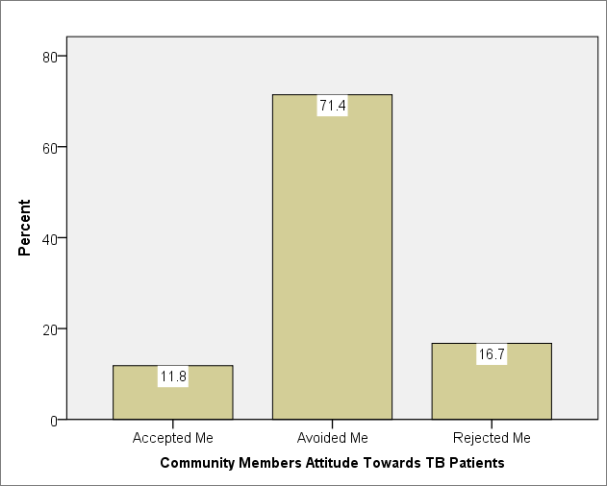
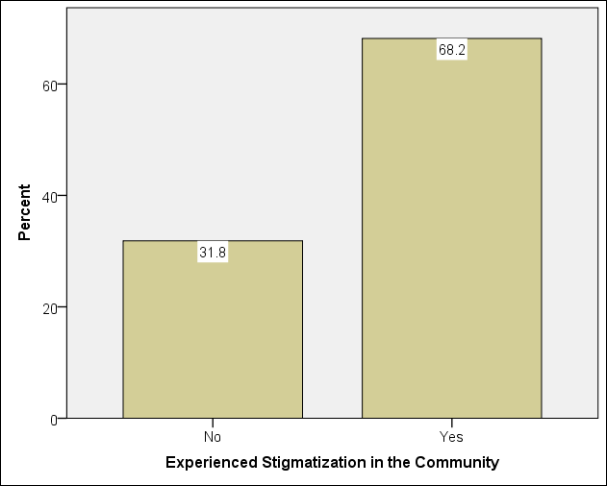
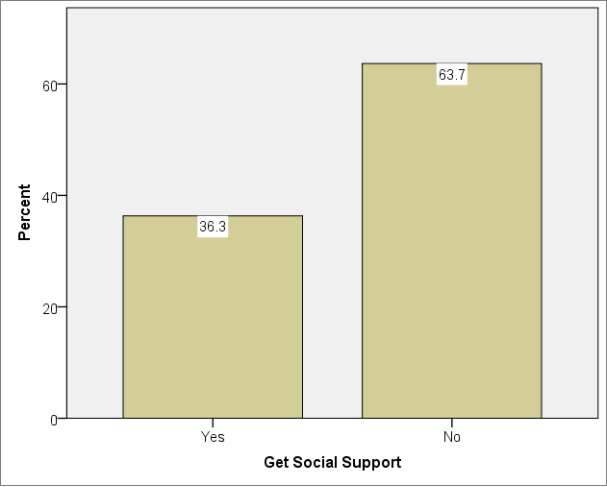
Background: Tuberculosis (TB) continues to be a significant public health issue in Ghana, and stigma and compromised community support are intrinsic barriers to successful treatment, diagnosis, and control. Knowledge of community attitudes and sociodemographic factors that influence stigma is crucial for developing targeted interventions in Nkoranza South Municipality. Methods: This was a cross-sectional study that included 245 randomly selected TB patients aged 18 and older who were currently receiving or had completed treatment between 2016 and 2020 in the Nkoranza South Municipality. Data were collected using a semi-structured questionnaire, administered through the home and healthcare facility by trained enumerators. Using SPSS version 26, Fisher’s Exact Test was used to examine association, and logistic regression was used to assess the impact of socio-demographic factors on stigma and support. Frequencies were used to explore suggestions for reducing stigma and improving TB care, with a statistical significance set at p<0.05. Results: The study revealed that 71.4% of TB patients interviewed reported avoidance by the community. About 17% felt rejected, and only 12% felt accepted by the members of their communities. About 64% reported a lack of support, and 68.2% reported experiencing stigma. TB patients aged 20-39 years had higher odds of experiencing a lack of support (aOR = 3.15, 95% CI: 1.35-7.39, p = 0.008). Respondents practicing other religions, unlike Christianity, had lower odds of stigmatization (aOR = 0.08, 95% CI: 0.01-0.53, p = 0.010) and lack of support (aOR = 0.10, 95% CI: 0.02-0.68, p = 0.019) compared to those practising traditional religion. Ethnic groups such as the Dagaari had lower odds of experiencing stigmatizations (aOR = 0.10, 95% CI: 0.02-0.44, p = 0.002) and lack of support (aOR = 0.19, 95% CI: 0.05-0.74, p = 0.016). Educational level was not significantly associated with stigma or support. TB patients suggested community education, TB awareness creation, and improved staff professionalism as crucial steps to reduce stigma and enhance TB care. Conclusion: TB stigma and support gaps are prevalent in Nkoranza South Municipality, with predominant influences of age, occupation, religion, and ethnicity. The challenges need culturally adapted public health education, improved healthcare professionalism, and sustained community mobilization to optimize the TB outcome and combat stigma. Future studies should investigate whether community-based education and advocacy interventions can reduce stigma associated with TB and increase long-term support for patients.
| Published in | Science Journal of Public Health (Volume 13, Issue 5) |
| DOI | 10.11648/j.sjph.20251305.12 |
| Page(s) | 257-268 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Tuberculosis, Stigma, Community Support, Sociodemographic Factors, Nkoranza South Municipality
Variables | Frequency (n=245) | Percent |
|---|---|---|
Age Level | ||
<20 yrs | 10 | 4.1 |
20 – 39 yrs | 137 | 55.9 |
40 – 59 yrs | 59 | 24.1 |
60 yrs and above | 39 | 15.9 |
Sex | ||
male | 174 | 71.0 |
female | 71 | 29.0 |
Educational level | ||
Middle / JHS | 52 | 21.2 |
No formal education | 52 | 21.2 |
Primary | 33 | 13.5 |
SHS/Vocational | 71 | 29.0 |
Tertiary | 37 | 15.1 |
Occupation | ||
Civil servant | 33 | 13.5 |
Farmer | 85 | 34.7 |
Other | 56 | 22.9 |
Trader | 71 | 29.0 |
Religion | ||
Christianity | 201 | 82.0 |
Others | 35 | 14.3 |
Traditional | 9 | 3.7 |
Ethnicity | ||
Bono | 165 | 67.3 |
Dagaari | 33 | 13.5 |
Dagomba | 20 | 8.2 |
Mamprusi | 8 | 3.3 |
Others | 19 | 7.8 |
Marital status | ||
Cohabitation | 17 | 6.9 |
Divorced | 7 | 2.9 |
Married | 155 | 63.3 |
Single | 55 | 22.4 |
Widowed | 11 | 4.5 |
Variables/Categories | Experience Stigmatization n=245(%) | Fisher's Exact Test p-value | Lack of support n=245(%) | Fisher's Exact Test p-value | ||
|---|---|---|---|---|---|---|
No | Yes | No | Yes | |||
Age Group | P<.001 | no | yes | P<.001 | ||
<20 yrs | 3(30.0) | 7(70.0) | 4(40.0) | 6(60.0) | ||
20 – 39 yrs | 29(21.2) | 108(78.8) | 35(25.5) | 102(74.5) | ||
40 – 59 yrs | 24(40.7) | 35(59.3) | 28(47.5) | 31(52.5) | ||
60 yrs and above | 22(56.4) | 17(43.6) | 22(56.4) | 17(43.6) | ||
Sex | 0.546 | 1.000 | ||||
male | 53(30.5) | 121(69.5) | 63(36.2) | 111(63.8) | ||
female | 25(35.2) | 46(64.8) | 26(36.6) | 45(63.4) | ||
Educational level | 0.009 | 0.244 | ||||
Middle / JHS | 18(34.6) | 34(65.4) | 18(34.6) | 34(65.4) | ||
No formal education | 24(46.2) | 28(53.8) | 24(46.2) | 28(53.8) | ||
Primary | 14(42.4) | 19(57.6) | 15(45.5) | 18(54.5) | ||
SHS/Vocational | 15(21.1) | 56(79.9) | 21(29.6) | 50(70.4) | ||
Tertiary | 7(18.9) | 30(81.1) | 11(29.7) | 26(70.3) | ||
Occupation | 0.003 | 0.008 | ||||
Civil servant | 6(18.2) | 27(81.8) | 9(27.3) | 24(72.7) | ||
Farmer | 30(35.3) | 55(64.7) | 32(37.6) | 53(62.4) | ||
Other | 27(48.2) | 29(51.8) | 30(53.6) | 26(46.4) | ||
Trader | 15(21.1) | 56(78.9) | 18(25.4) | 53(74.6) | ||
Religion | P<.001 | P<.001 | ||||
Christianity | 51(25.4) | 150(74.6) | 63(31.3) | 138(68.7) | ||
Others | 25(71.4) | 10(28.6) | 24(68.6) | 11(31.4) | ||
Traditional | 2(22.2) | 7(77.8) | 2(22.2) | 7(77.8) | ||
Ethnicity | 0.003 | P<.001 | ||||
Bono | 44(26.7) | 121(73.3) | 46(27.9) | 119(72.1) | ||
Dagaari | 20(60.6) | 13(39.4) | 22(66.7) | 11(33.3) | ||
Dagomba | 8(40.0) | 12(60.0) | 11(55.0) | 9(45.0) | ||
Mamprusi | 1(12.5) | 7(87.5) | 3(37.5) | 5(62.5) | ||
Others | 5(26.3) | 14(73.7) | 7(36.8) | 12(63.2) | ||
Marital status | 0.311 | 0.520 | ||||
Cohabitation | 3(17.6) | 14(82.4) | 6(35.3) | 11(64.7) | ||
Divorced | 3(42.9) | 4(57.1) | 4(57.1) | 3(42.9) | ||
Married | 50(32.3) | 105(67.7) | 54(34.8) | 101(65.2) | ||
Single | 16(29.1) | 39(70.9) | 19(34.5) | 36(65.5) | ||
Widowed | 6(54.5) | 5(45.5) | 6(54.5) | 5(45.5) | ||
Variables/ Categories | Stigmatization | Lack of support | ||||||
|---|---|---|---|---|---|---|---|---|
cOR (95%CI) | P-value | aOR (95%CI) | P-value | cOR (95%CI) | P-value | aOR (95%CI) | P-value | |
Age Group | ||||||||
<20 yrs | 3.02(0.68-13.44) | 0.147 | 3.82(0.92-6.52) | 0.145 | 1.94(0.47-7.99) | 0.358 | 3.29(0.66-16.37) | 0.146 |
20 – 39 yrs | 4.82(2.27-10.24) | P<.001 | 2.4(0.92-6.52) | 0.072 | 3.77(1.80-7.91) | P<.001 | 3.15(1.35-7.39) | 0.008 |
40 – 59 yrs | 1.89(0.83-4.28) | 0.128 | 1.64(0.62-4.31) | 0.318 | 1.43(0.64-3.23) | 0.386 | 1.60(0.64-4.00) | 0.314 |
60 yrs and above | Ref | Ref | Ref | Ref | ||||
Educational level | ||||||||
Middle / JHS | 0.44(0.16-1.20) | 0.109 | 0.46(0.10-2.13) | 0.323 | - | - | - | - |
No formal education | 0.27(0.10-0.73) | 0.010 | 0.38(0.7-2.02) | 0.259 | ||||
Primary | 0.32(0.11-0.93) | 0.036 | 0.39(0.07-2.04) | 0.263 | ||||
SHS/Vocational | 0.87(0.32-2.37) | 0.787 | 1.07(0.26-4.45) | 0.923 | ||||
Tertiary | Ref | Ref | ||||||
Occupation | ||||||||
Civil servant | 1.21(0.42-3.45) | 0.728 | 0.56(0.11-2.86) | 0.482 | 0.91(0.36-2.31) | 0.835 | 0.66(0.23-1.87) | 0.432 |
Farmer | 0.49(0.23-1.01) | 0.054 | 0.69(0.27-1.79) | 0.443 | 0.56(0.28-1.12) | 0.103 | 0.67(0.30-1.47) | 0.316 |
Other | 0.29(0.13-0.62) | 0.002 | 0.15(0.05-0.42) | P<.001 | 0.29(0.14-0.62) | 0.001 | 0.22(0.10-0.55) | 0.001 |
Trader | Ref | Ref | Ref | Ref | ||||
Religion | ||||||||
Christianity | 0.84(0.17-4.18) | 0.832 | 0.42(0.07-2.58) | 0.351 | 0.63(0.13-3.10) | 0.566 | 0.25(0.41-1.56) | 0.139 |
Others | 0.11(020-0.65) | 0.014 | 0.08(0.01-0.53) | 0.010 | 0.13(0.02-0.74) | 0.021 | 0.10(0.02-0.68) | 0.019 |
Traditional | Ref | Ref | Ref | ` | ||||
Ethnicity | ||||||||
Bono | 0.98(0.33-2.89) | 0.974 | 0.25(0.07-0.98) | 0.046 | 1.51(0.56-4.07) | 0.416 | 0.67(0.21-2.14) | 0.503 |
Dagaari | 0.23(0.67-0.80) | 0.021 | 0.10(0.02-0.44) | 0.002 | 0.29(0.90-0.95) | 0.041 | 0.19(0.05-0.74) | 0.016 |
Dagomba | 0.54(0.14-2.08) | 0.368 | 0.22(0.04-1.12) | 0.068 | 0.48(0.13-1.72) | 0.258 | 0.20(0.05-0.92) | 0.039 |
Mamprusi | 2.50(0.24-25.72) | 0.441 | 2.09(0.10-45.28) | 0.639 | 0.97(0.18-5.37) | 0.974 | 0.66(0.10-4.54) | 0.676 |
Others | Ref | Ref | Ref | Ref | ||||
TB patients' suggestions for reducing stigma and improving TB case detection | Frequency | Percent |
|---|---|---|
Community education and advocacy | 242 | 98.8 |
Creation of awareness | 244 | 99.6 |
Support for TB patients | 243 | 99.2 |
Good staff professionalism | 245 | 100 |
cOR | Crude Odds Ratio |
aOR | Adjusted Odds Ratio |
Ref | Reference Category |
CI | Confidence Interval |
TB | Tuberculosis |
| [1] | Rebeiro PF, Cohen MJ, Ewing HM, Figueiredo MC, Peetluk LS, Andrade KB, et al. Knowledge and stigma of latent tuberculosis infection in Brazil : implications for tuberculosis prevention strategies. BMC Public Health. 2020; 1-10. Available from: |
| [2] | Desanto D, Velen K, Lessells R, Makgopa S, Gumede D, Fielding K, et al. A qualitative exploration into the presence of TB stigmatization across three districts in South Africa. BMC Public Health. 2023; 1-10. Available from: |
| [3] | Anto BP, Boakye-yiadom J. Factors influencing treatment success in drug-susceptible tuberculosis patients in Ghana : A prospective cohort study. 2025; 1-12. Available from: |
| [4] | Huq KATME, Moriyama M, Krause D, Shirin H, Awoonor-willaims JK, Rahman M, et al. Perceptions, Attitudes, Experiences and Opinions of Tuberculosis Associated Stigma : A Qualitative Study of the Perspectives among the Bolgatanga Municipality People of Ghana. International Journal of Environmental Research and Public Health. 2022; 19(22): 1-19. Available from: |
| [5] | Gyimah FT, Dako-gyeke P. Perspectives on TB patients ’ care and support : a qualitative study conducted in Accra Metropolis, Ghana. Globalization and Health. 2019; 9: 1-9. Available from: |
| [6] | Polat H, Bahcecioglu G, Tan M. Determining the relationship between stigmatization and social support in tuberculosis patients. Journal of Clinical Tuberculosis and Other Mycobacterial Diseases [Internet]. 2024; 37(November): 100502. Available from: |
| [7] | Bodur MS, Çil B. A Research on Healthcare Professionals ’ Stigma Towards Tuberculosis Patients. Thoracic Research and Practice. 2025; 26(3): 88-96. Available from: |
| [8] | Kamble BD, Singh SK, Jethani S, D VGC, Acharya BP. Social stigma among tuberculosis patients attending DOTS centers in Delhi. Journal of Family Medicine and Primary Care. 2020; 4-9. Available from: |
| [9] | Craciun OM, Torres R, Llanes B, Romay-Barja M. Tuberculosis Knowledge, Attitudes, and Practice in Middle- and Low-Income Countries : A Systematic Review. Journal of Tropical Medicine. 2023; 2023: 1-15. Available from: |
| [10] | Alfaiate A, Rodrigues R, Aguiar A, Sc M, Duarte R. Tuberculosis and COVID-19 Related Stigma : Portuguese Patients Experiences. Tuberculosis and Respiratory Diseases. 2023; 216-25. Available from: |
| [11] | Sazali MF, Sharizman S, Abdul S, Ch MBBBAO. Improving Tuberculosis Medication Adherence : The Potential of Integrating Digital Technology and Health Belief Model. Tuberculosis and Respiratory Diseases. 2022; 82-93. Available from: |
| [12] | Bajema KL, Kubiak RW, Guthrie BL, Graham SM, Govere S, Thulare H, et al. Tuberculosis-related stigma among adults presenting for HIV testing in KwaZulu- Natal, South Africa. BMC Public Health. 2020; 1-8. Available from: |
| [13] | Wambura G, Id M, Nyamogoba HDN, Chiang SS, Mcgarvey T. PLOS ONE Burden of stigma among tuberculosis patients in a pastoralist community in Kenya : A mixed methods study. PLOS ONE [Internet]. 2020; 15(10): 1-14. Available from: |
| [14] | Salisu HM, Ojule IN, Adeniji FO, Kwakye GK. Prevalence and trend of TB/HIV co-infection in Suhum Municipality, Ghana. Global Public Health Research [Internet]. 2022; 2(7): 1-12. Available from: |
| [15] | Brüggemann R, Schlumberger F, Chinshailo F, Willis M, Kadyrov A. Stigmatization and discrimination of female tuberculosis patients in Kyrgyzstan - a phenomenological study. International Journal for Equity in Health. 2025; 1-14. Available from: |
| [16] | Nabei JN, Bonful HA, Afari EA, Mohammed AG. Predictors of quality of life of TB / HIV co-infected patients in the Northern region of Ghana. BMC Infectious Diseases [Internet]. 2024; 1-10. Available from: |
| [17] | Kasozi W, Muyanja SZ, Musaazi J, Etwom A, Lemukol J, Sagaki P, et al. A qualitative exploration of community knowledge, attitudes, and practices towards tuberculosis in the Karamoja subregion, northeastern Uganda. BMC Health Services Research [Internet]. 2024; 1-8. Available from: |
| [18] | Oladele DA, Balogun MR, Odeyemi K, Salako BL. Research Article A Comparative Study of Knowledge, Attitude, and Determinants of Tuberculosis-Associated Stigma in Rural and Urban Communities of Lagos State, Nigeria. Tuberculosis and Respiratory Diseases. 2020; 2020. Available from: |
| [19] | Tb WHO, Sharing K, Handbooks O. World Health Organisation. Geneva, Switzerland: World Health Organization; 2025. p. 1-3 Social support in TB management. Available from: |
| [20] | Carvalho M, Viktoria I, Id K, Pereira L, Benites A, Id S, et al. The contribution of stigma to the transmission and treatment of tuberculosis in a hyperendemic indigenous population in Brazil. PLOS ONE. 2020; 15(12): 1-13. Available from: |
| [21] | Laycock KM, Enane LA, Steenhoff AP. Tuberculosis in Adolescents and Young Adults : Emerging Data on TB Transmission and Prevention among Vulnerable Young People. Tropical Medicine and Infectious Disease. 2021; 6(148): 1-17. Available from: |
| [22] | Waterous P, Chingono R, Mackworth-young C, Nyamayaro C, Kandiye FR, Marambire E, et al. PLOS GLOBAL PUBLIC HEALTH interventions to improve TB Care for adolescents and young adults. PLOS Global Public Health [Internet]. 2024; 4(11): 1-17. Available from: |
| [23] |
World Health Organization. The End TB Strategy [Internet]. Geneva, Switzerland: World Health Organization; 2015. p. 1-20. Available from:
https://iris.who.int/bitstream/handle/10665/331326/WHO-HTM-TB-2015.19-eng.pdf?sequence=1 |
| [24] | Ereso BM, Sagbakken M, Gradmann C, Yimer SA. Determinants of an unfavorable treatment outcome among tuberculosis patients in the Jimma Zone, Southwest Ethiopia. Scientific Reports. 2024; 1-11. Available from: |
APA Style
Leta, P. K., Aboagye, D. A., Gmanyami, J. M., Nsiah, R. B., Boasiako, R. G. A., et al. (2025). Exploring Community Attitudes and Sociodemographic Determinants of Stigma and Support Towards Tuberculosis Patients: A Cross-Sectional Study in Nkoranza South Municipality, Ghana. Science Journal of Public Health, 13(5), 257-268. https://doi.org/10.11648/j.sjph.20251305.12
ACS Style
Leta, P. K.; Aboagye, D. A.; Gmanyami, J. M.; Nsiah, R. B.; Boasiako, R. G. A., et al. Exploring Community Attitudes and Sociodemographic Determinants of Stigma and Support Towards Tuberculosis Patients: A Cross-Sectional Study in Nkoranza South Municipality, Ghana. Sci. J. Public Health 2025, 13(5), 257-268. doi: 10.11648/j.sjph.20251305.12
AMA Style
Leta PK, Aboagye DA, Gmanyami JM, Nsiah RB, Boasiako RGA, et al. Exploring Community Attitudes and Sociodemographic Determinants of Stigma and Support Towards Tuberculosis Patients: A Cross-Sectional Study in Nkoranza South Municipality, Ghana. Sci J Public Health. 2025;13(5):257-268. doi: 10.11648/j.sjph.20251305.12
@article{10.11648/j.sjph.20251305.12,
author = {Peter Kipo Leta and Dacosta Awuah Aboagye and Jonathan Mawutor Gmanyami and Richmond Bediako Nsiah and Rachael Georgina Antwi Boasiako and Khadijatu Adiss Yusif and Oscar Lambert and Mercy Negble and Obed Atsu-Ofori and Foster Bediako Gbafu and Mavis Vikpedomo Baalasuuri and John Humphrey Amuasi and Paulina Clara Appiah and Dominic Nyarko and Frank Prempeh and Margaret Morrison and Theodora Konadu Owusu Amponsah and Amponsah Kinsley Osei and Victor Jamoni},
title = {Exploring Community Attitudes and Sociodemographic Determinants of Stigma and Support Towards Tuberculosis Patients: A Cross-Sectional Study in Nkoranza South Municipality, Ghana
},
journal = {Science Journal of Public Health},
volume = {13},
number = {5},
pages = {257-268},
doi = {10.11648/j.sjph.20251305.12},
url = {https://doi.org/10.11648/j.sjph.20251305.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjph.20251305.12},
abstract = {Background: Tuberculosis (TB) continues to be a significant public health issue in Ghana, and stigma and compromised community support are intrinsic barriers to successful treatment, diagnosis, and control. Knowledge of community attitudes and sociodemographic factors that influence stigma is crucial for developing targeted interventions in Nkoranza South Municipality. Methods: This was a cross-sectional study that included 245 randomly selected TB patients aged 18 and older who were currently receiving or had completed treatment between 2016 and 2020 in the Nkoranza South Municipality. Data were collected using a semi-structured questionnaire, administered through the home and healthcare facility by trained enumerators. Using SPSS version 26, Fisher’s Exact Test was used to examine association, and logistic regression was used to assess the impact of socio-demographic factors on stigma and support. Frequencies were used to explore suggestions for reducing stigma and improving TB care, with a statistical significance set at pResults: The study revealed that 71.4% of TB patients interviewed reported avoidance by the community. About 17% felt rejected, and only 12% felt accepted by the members of their communities. About 64% reported a lack of support, and 68.2% reported experiencing stigma. TB patients aged 20-39 years had higher odds of experiencing a lack of support (aOR = 3.15, 95% CI: 1.35-7.39, p = 0.008). Respondents practicing other religions, unlike Christianity, had lower odds of stigmatization (aOR = 0.08, 95% CI: 0.01-0.53, p = 0.010) and lack of support (aOR = 0.10, 95% CI: 0.02-0.68, p = 0.019) compared to those practising traditional religion. Ethnic groups such as the Dagaari had lower odds of experiencing stigmatizations (aOR = 0.10, 95% CI: 0.02-0.44, p = 0.002) and lack of support (aOR = 0.19, 95% CI: 0.05-0.74, p = 0.016). Educational level was not significantly associated with stigma or support. TB patients suggested community education, TB awareness creation, and improved staff professionalism as crucial steps to reduce stigma and enhance TB care. Conclusion: TB stigma and support gaps are prevalent in Nkoranza South Municipality, with predominant influences of age, occupation, religion, and ethnicity. The challenges need culturally adapted public health education, improved healthcare professionalism, and sustained community mobilization to optimize the TB outcome and combat stigma. Future studies should investigate whether community-based education and advocacy interventions can reduce stigma associated with TB and increase long-term support for patients.
},
year = {2025}
}
TY - JOUR T1 - Exploring Community Attitudes and Sociodemographic Determinants of Stigma and Support Towards Tuberculosis Patients: A Cross-Sectional Study in Nkoranza South Municipality, Ghana AU - Peter Kipo Leta AU - Dacosta Awuah Aboagye AU - Jonathan Mawutor Gmanyami AU - Richmond Bediako Nsiah AU - Rachael Georgina Antwi Boasiako AU - Khadijatu Adiss Yusif AU - Oscar Lambert AU - Mercy Negble AU - Obed Atsu-Ofori AU - Foster Bediako Gbafu AU - Mavis Vikpedomo Baalasuuri AU - John Humphrey Amuasi AU - Paulina Clara Appiah AU - Dominic Nyarko AU - Frank Prempeh AU - Margaret Morrison AU - Theodora Konadu Owusu Amponsah AU - Amponsah Kinsley Osei AU - Victor Jamoni Y1 - 2025/09/19 PY - 2025 N1 - https://doi.org/10.11648/j.sjph.20251305.12 DO - 10.11648/j.sjph.20251305.12 T2 - Science Journal of Public Health JF - Science Journal of Public Health JO - Science Journal of Public Health SP - 257 EP - 268 PB - Science Publishing Group SN - 2328-7950 UR - https://doi.org/10.11648/j.sjph.20251305.12 AB - Background: Tuberculosis (TB) continues to be a significant public health issue in Ghana, and stigma and compromised community support are intrinsic barriers to successful treatment, diagnosis, and control. Knowledge of community attitudes and sociodemographic factors that influence stigma is crucial for developing targeted interventions in Nkoranza South Municipality. Methods: This was a cross-sectional study that included 245 randomly selected TB patients aged 18 and older who were currently receiving or had completed treatment between 2016 and 2020 in the Nkoranza South Municipality. Data were collected using a semi-structured questionnaire, administered through the home and healthcare facility by trained enumerators. Using SPSS version 26, Fisher’s Exact Test was used to examine association, and logistic regression was used to assess the impact of socio-demographic factors on stigma and support. Frequencies were used to explore suggestions for reducing stigma and improving TB care, with a statistical significance set at pResults: The study revealed that 71.4% of TB patients interviewed reported avoidance by the community. About 17% felt rejected, and only 12% felt accepted by the members of their communities. About 64% reported a lack of support, and 68.2% reported experiencing stigma. TB patients aged 20-39 years had higher odds of experiencing a lack of support (aOR = 3.15, 95% CI: 1.35-7.39, p = 0.008). Respondents practicing other religions, unlike Christianity, had lower odds of stigmatization (aOR = 0.08, 95% CI: 0.01-0.53, p = 0.010) and lack of support (aOR = 0.10, 95% CI: 0.02-0.68, p = 0.019) compared to those practising traditional religion. Ethnic groups such as the Dagaari had lower odds of experiencing stigmatizations (aOR = 0.10, 95% CI: 0.02-0.44, p = 0.002) and lack of support (aOR = 0.19, 95% CI: 0.05-0.74, p = 0.016). Educational level was not significantly associated with stigma or support. TB patients suggested community education, TB awareness creation, and improved staff professionalism as crucial steps to reduce stigma and enhance TB care. Conclusion: TB stigma and support gaps are prevalent in Nkoranza South Municipality, with predominant influences of age, occupation, religion, and ethnicity. The challenges need culturally adapted public health education, improved healthcare professionalism, and sustained community mobilization to optimize the TB outcome and combat stigma. Future studies should investigate whether community-based education and advocacy interventions can reduce stigma associated with TB and increase long-term support for patients. VL - 13 IS - 5 ER -
Public Health Department, Ghana Health Service, Accra, Ghana
Administrative Department, A1 Hospital, Kumasi, Ghana
School of Public Health, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana; Department of Implementation Research, Bernhard Nocht Institute of Tropical Medicine, Hamburg, Germany
Public Health Department, Ghana Health Service, Accra, Ghana
Public Health Department, Ghana Health Service, Accra, Ghana
Public Health Department, Ghana Health Service, Accra, Ghana
School of Public Health, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana; Governance Department, Ubora Foundation Africa, Accra, Ghana; Department of Health Education, Global Health Insight and Education, Accra, Ghana
Nursing and Midwifery Department, Garden City University, Kumasi, Ghana
School of Public Health, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana
School of Public Health, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana
Department of Vocational Training, University of Cape Coast, Cape Coast, Ghana
Global Health and Infectious Diseases Research Group, Kumasi Centre for Collaborative Research in Tropical Medicine, Kumasi, Ghana; School of Public Health, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana; Department of Implementation Research, Bernhard Nocht Institute of Tropical Medicine, Hamburg, Germany
Public Health Department, Ghana Health Service, Accra, Ghana
Public Health Department, Ghana Health Service, Accra, Ghana
Public Health Department, Ghana Health Service, Accra, Ghana
Membership and Regional Operations Directorate, National Health Insurance Authority, Accra, Ghana
School of Public Health, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana
Public Health Department, Ghana Health Service, Accra, Ghana
Public Health Department, Ghana Health Service, Accra, Ghana
Information