Abstract
Background: Malnutrition is a significant public health challenge, particularly among children under the age of five, with severe implications for growth, development, and long-term health outcomes. This study assessed the prevalence and determinants of malnutrition in children under five years old in Obuama Community, Degema Local Government Area, Rivers State, Nigeria. Methods: An Analytical cross-sectional study was conducted using a multi-stage sampling technique for four months (19th August - 21st of November 2024). Anthropometric measurements, including mid-upper arm circumference (MUAC), weight, height, and World Health Organization (WHO) growth standards, were used to assess the nutritional status of 165 children. Data analysis was performed using the Statistical Product and Service Solution Package (SPSS) Version 27. Results: The study showed a low prevalence of acute malnutrition (2.4%) based on MUAC measurements. Among the children, 2.4% reported moderate undernutrition, 0.6% were overweight, and 1.2% were obese, using the BMI-for-age assessments. Substantially more malnutrition was also shown in children 36 months and older and in those with malaria (p < 0.05). The caregivers reported limited awareness of their children’s nutritional status, with 46.7% expressing uncertainty about whether their child was malnourished. Children aged above 48 months and malaria diagnosis were independent predictors of malnutrition (p < 0.05). Conclusion: Malnutrition was prevalent among children in Obuama community. The observation of both undernutrition and overnutrition (overweight and obesity) highlights a dual burden of malnutrition. The findings emphasized the need for targeted nutritional interventions, including caregivers’ education on proper infant and young child feeding practices, early detection of malnutrition, and strategies to address both undernutrition and obesity. Public health programs should also integrate malaria prevention and treatment as part of a comprehensive effort to reduce malnutrition.
Keywords
Malnutrition, Prevalence, MUAC, BMI, Under-five Children
1. Introduction
In low- and middle-income countries (LMICs), malnutrition affects more children under five years of age, making it one of the most significant global public health problems
. Malnutrition, as defined by the World Health Organization (WHO), includes both undernutrition (stunting, wasting, and underweight) and overnutrition (overweight, obesity) and is defined as "deficiencies, excesses, or imbalances in a person's intake of energy and/or nutrients"
. In 2022, thirty-six million children were overweight or obese, forty-five million were wasted (too thin for height), and 149 million children under five were stunted (too short for age) globally
| [3] | Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, de Onis M, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013; 382 (9890): 427-51. https://doi.org/10.1016/S0140-6736(13)60937-X |
[3]
. These conditions have significant short- and long-term effects, such as higher death rates, increased susceptibility to infections, and decreased cognitive development
.
Malnutrition in children under five is a persistent problem in Nigeria, where national statistics show that 37% are stunted, 7% wasted, and 23% underweight
| [5] | National Population Commission (NPC) [Nigeria], ICF International. Nigeria Demographic and Health Survey 2018. Abuja, Nigeria: NPC and ICF; 2019. |
[5]
. The situation is dangerous, especially in remote communities such as Obuama in Rivers State, where inadequate access to healthcare, food insecurity, and poverty contribute to dietary deficiencies
| [6] | Smith J, Doe A, Johnson C. Malnutrition in rural Nigerian communities: socio-economic and environmental determinants. J Rural Health. 2017; 33(3): 300-10. |
[6]
. Rivers State is situated in the South-South geopolitical region of Nigeria in the Niger Delta area. It has enormous oil resources, but most communities suffer from underdevelopment, environmental degradation, and poor infrastructure, which contribute to malnutrition
| [7] | Okari TG, Nte AR, Frank BA. Prevalence of malnutrition in under-five children in Okrika Town. Niger J Paediatr. 2018; 45(2): 112-8. |
[7]
. Okari et al. (2018) reported a 10.8% prevalence of malnutrition in Okrika, a neighboring community, with underweight being the most common manifestation
. Given comparable socioeconomic conditions, Obuama is likely to experience similar patterns. Malnutrition in children under the age of five is caused by a combination of factors such as low nutritional intake and sickness, as well as underlying conditions such as poverty, maternal education, and poor sanitation
| [9] | Bhutta ZA, Das JK, Rizvi A, Gaffey MF, Walker N, Horton S, et al. Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost? Lancet. 2013; 382 (9890): 452-77. https://doi.org/10.1016/S0140-6736(13)60996-4 |
[9]
. Protein-energy malnutrition (PEM) is widespread in Nigeria, with kwashiorkor and marasmus being the most severe cases
| [10] | Owino V, Ahmed T, Freemark M, Kelly P, Loy A, Manary M, et al. Environmental enteric dysfunction and growth failure/stunting in global child health. J Pediatr Gastroenterol Nutr. 2020; 70(1): 6-21. https://doi.org/10.1097/MPG.0000000000002498 |
[10]
. Furthermore, cultural practices like a lack of exclusive breastfeeding and early introduction of complementary foods contribute to poor nutritional outcomes
| [11] | Senbanjo IO, Oshikoya KA, Odusanya OO, Njokanma OF. Maternal and child under-nutrition in rural and urban communities of Lagos State, Nigeria: the relationship and risk factors. Matern Child Nutr. 2013; 9(4): 365-79. https://doi.org/10.1111/j.1740-8709.2011.00396.x |
[11]
. The interplay of malnutrition and infectious diseases such as malaria and diarrhea generates a vicious cycle that worsens child health
| [12] | Guerrant RL, DeBoer MD, Moore SR, Scharf RJ, Lima AA. The impoverished gut—a triple burden of diarrhoea, stunting and chronic disease. Nat Rev Gastroenterol Hepatol. 2013; 10(4): 220-9. https://doi.org/10.1038/nrgastro.2012.239 |
[12]
.
Despite government interventions such as Community-Based Management of Acute Malnutrition (CMAM) and vitamin A supplementation programs, rural malnutrition rates remain high
. This is attributed in part to inadequate healthcare systems, poor policy implementation, and a lack of community awareness
.
Furthermore, new concerns such as childhood obesity are becoming more prevalent in Nigeria, showing a nutritional shift towards energy-dense but nutrient-poor diets
. This double burden of malnutrition, which includes both undernutrition and overnutrition, presents a significant challenge for public health interventions
| [16] | Wells JC, Sawaya AL, Wibaek R, Mwangome M, Poullas MS, Yajnik CS, et al. The double burden of malnutrition: aetiological pathways and consequences. Lancet. 2020; 395 (10217): 75-88. https://doi.org/10.1016/S0140-6736(19)32472-9 |
[16]
.
The literature search found no studies assessing malnutrition in Obuama, thereby creating a gap in localized data needed for focused interventions. This study aimed to assess the prevalence and determinants of malnutrition among children under five years of age in Obuama, determine caregivers’ awareness, and associated health conditions. The findings will help policymakers and healthcare providers to develop effective nutrition initiatives for similar rural areas.
2. Materials and Methods
2.1. Study Design
An analytical cross-sectional study design, conducted for four months from 19th August to 21st of November 2024, was used for the study.
2.2. Study Area
The study was conducted in Obuama, a rural, riverine community in the Degema Local Government Area of Rivers State, Nigeria. Its geographic coordinates are longitude 7° 47’ and 10° 0’ East and latitude 6° 25’ and 8° 8’ North. Rivers State is one of the thirty-six states located in the South-South geopolitical region of Nigeria in the oil-rich Niger Delta area. The state capital is Port Harcourt. The state has twenty-three Local Government Areas (LGAs). The Degema Local Government Area has 17 political wards. Obuama has an estimated population of 39, 337 as of 2024, and it is in ward 14. The major occupation of the people is fishing, although small-scale farming and trading are also common. Other people also work in government establishments such as the Local Government Council, health care facilities, and schools.
2.3. Study Population
The study population was children aged 0-59 months.
Inclusion Criteria
1) Children aged 0-59 months who lived in the community for at least a year.
2) Mothers/Caregivers who provided consent for their children to take part in the study.
Exclusion Criteria
1) Children reported to have other significant co-morbidities such as sickle cell anaemia, among others.
2) Children with severe illnesses such as pneumonia, measles, cellulitis, otitis media, among others.
2.4. Sample Size Determination
The sample size for this study was calculated using Cochran’s formula for cross-sectional studies:
n = Z^2 * p * (1 - p) / d^2. Where: n=minimum sample size, Z=Standard normal deviate (1. 96 for a 95% confidence level),
p = Estimated proportion of the population with the attribute (10.8%, derived from an earlier study in Okrika in Rivers State)
| [7] | Okari TG, Nte AR, Frank BA. Prevalence of malnutrition in under-five children in Okrika Town. Niger J Paediatr. 2018; 45(2): 112-8. |
[7]
, d = Margin of error (0. 05).
n=1. 962 x 0. 108 x (1 - 0. 108) / 0. 052 =148. 034. Assuming a non-response rate of 10%, the adjusted sample size (N) was calculated as follows: N = n / (1-non-response) = 148. 034/ (1-0. 01) =148. 034/0. 09=164. 4, but 165 was used.
2.5. Sampling Technique
A multi-stage sampling method involving four stages was used. The first stage was the selection of Degema LGA from the 23 LGAs of Rivers State using simple random sampling by balloting. The second stage was the selection of ward 14 (Obuama) from the 17 wards of Degema Local Government Area, also by simple random sampling through balloting. The third stage was the selection of households by systematic random sampling. The first household was selected by simple random sampling, after which the next households with eligible children were selected using the sampling interval of 3 until the required sample size of 165 households was selected. The fourth stage was the selection of one participant from each household using simple random sampling by balloting. Only one mother/caregiver with an eligible child per household was selected.
2.6. Tools for Measurement
The Shakir’s tape was used to measure the mid-upper arm circumference (MUAC), the weighing scale to measure the weight in kilograms, and the height/length board to measure the height/length in centimeters. The WHO growth chart for children under five years, males and females, was also used to assess the nutritional status of the children.
2.7. Data Analysis
BMI-for-age was calculated using the WHO child growth standards. The data obtained was entered into a Microsoft Excel 365 spreadsheet, cleaned, checked for missing values, validated, and exported to the Statistical Product and Service Solution Package (SPSS) Version 27 (Armonk, NY: IBM Corporation). The data was further validated with the validation function of SPSS. The data was analyzed using SPSS Version 27. The chi-square test was used to assess the significance of associations between nutritional status categories (normal, underweight, overweight, obesity) and child characteristics such as gender, age group, and health conditions (e. g., malaria, pneumonia, gastritis). A significant level of p < 0.05 was considered statistically significant. In the multivariate logistic regression analysis, the dependent and independent variables were expressed as binary data. The dependent variable was malnutrition status and expressed as 1=malnourished (moderately underweight, overweight, or obese by BMI-for-age; n=7) and 0=not malnourished (normal BMI-for-age; n=158). The independent variables were sex (male = 1, female = 0), age group (months) (1 = 0-11, 0 = 12-23, 24-35, 36-47, 48-59), malaria diagnosis (yes = 1, no = 0), pneumonia diagnosis (yes = 1, no = 0), and gastritis diagnosis (yes = 1, no = 0). Only the significant variables in the bivariate analysis were included.
2.8. Ethical Approval
Ethical approval was obtained from the Rivers State University Teaching Hospital Research Ethics Committee. Informed consent was obtained from heads of households and caregivers. Participation was voluntary, and participants can leave the study at any time without penalty. Data were kept confidential and stored in a password-protected computer accessible only to the research team.
3. Results
The study included a total of 165 children under five years of age from Obuama Community. The gender distribution showed a slight predominance of male children, who accounted for 52.1% of the participants, while female children made up 47.9%.
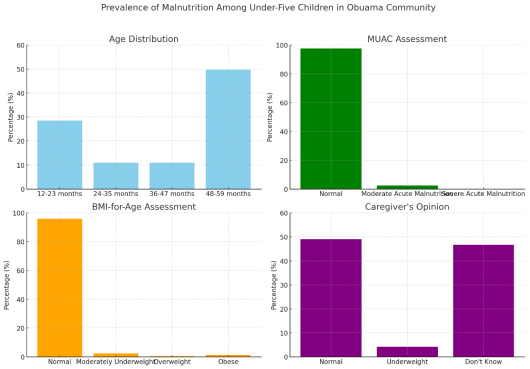
The prevalence of acute malnutrition based on MUAC measurements was 2.4% (4 out of 165 children, including 1.2% moderate acute malnutrition and 1.2% severe acute malnutrition). Based on BMI-for-age (WHO growth charts), 95.8% of children were within a normal nutritional status (-2 to +2 Z-score), 2.4% were moderately underweight (<- 2 to ≥ -3 Z-score), 0.6% were overweight (> +2 to ≤ +3 Z-score), and 1.2% were obese (> +3 Z-score) (
Table 1). Notably, all cases of overweight and obesity occurred in female children, and all underweight cases were in children aged 36-59 months.
“Malnourished” includes all children classified as moderately underweight, overweight, or obese by BMI-for-age (n=7), and “Not malnourished” refers to children with normal nutritional status by BMI-for-age (n=158). Caregivers’ perceptions of their children’s nutrition revealed that 46.7% of caregivers were unaware of their children’s nutritional status (“No idea”). About 49.7% of caregivers believed their children were of normal weight, while 4.2% perceived their children to be underweight. No one perceived that their children were overweight or obese.
Figure 1 shows the prevalence of malnutrition among children less than five years of age in Obuama community.
Table 1. Prevalence of Malnutrition Based on BMI-for-age.
BMI-for-age category | Frequency (n=165) | Percentage (%) |
Normal weight (-2 to +2 Z-score) | 158 | 95.8% |
Moderately underweight (< -2 to ≥ -3 Z-score) | 4 | 2.4% |
Severe acute malnutrition (< -3 Z-score) | 0 | 0.0% |
Overweight (> +2 to ≤ +3 Z-score) | 1 | 0.6% |
Obesity (> +3 Z-score) | 2 | 1.2% |
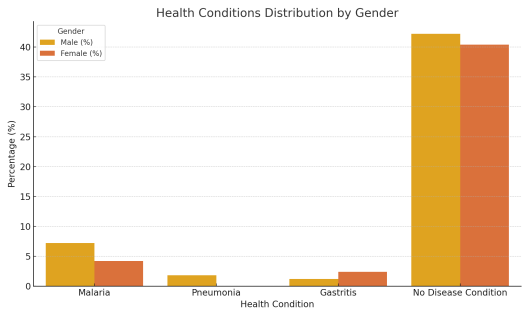
Common illnesses reported among the children included malaria (11.4% of children), pneumonia (1.8%), and gastritis (3.6%) (
Table 2). Most children (82.6%) had no reported disease condition in the two weeks prior to the survey.
Figure 2 shows the distribution of these health conditions by gender.
Table 2. Health Conditions Distribution by Gender.
Health Condition | Male (%) | Female (%) | Total (%) |
Malaria | 7.2% | 4.2% | 11.4% |
Pneumonia | 1.8% | 0.0% | 1.8% |
Gastritis | 1.2% | 2.4% | 3.6% |
No disease condition | 42.2% | 40.4% | 82.6% |
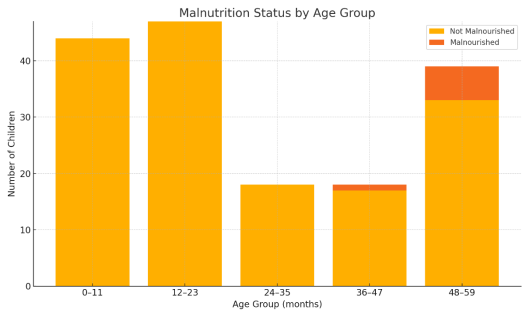
Bivariate analysis was conducted to explore associations between malnutrition status and selected variables. There was no statistically significant difference in malnutrition prevalence between male and female children (p=0.09). In contrast, malnutrition status was significantly associated with the age group (p=0.002), with all malnourished cases occurring in children 36 months or older. Children aged 48-59 months had the highest rate of malnutrition (15.4%), compared to no cases in children under 35 months. Age distribution analysis revealed that children between 12 and 23 months were the largest proportion of the study population at 28.5%. This age group is particularly significant, as it is a critical window in child development when nutritional deficiencies often become clear. However, malnutrition in this study was seen only among older children.
Figure 3 shows the malnutrition status by age group. On health conditions, children who had been diagnosed with malaria were significantly more likely to be malnourished than those who had not (15.8% vs 2.7%, p=0.03). There was no significant association between reported pneumonia or gastritis and malnutrition status in this study (p>0.05).
Table 3 summarizes the association between nutritional status and gender, age group, and diseases.
Table 3. Association of Malnutrition Status with Child Characteristics.
Factor | Category | Malnourished n (%) | Not Malnourished n (%) | p-value |
Sex | Male | 1 (1.2%) | 85 (98.8%) | 0.09α |
| Female | 6 (7.6%) | 73 (92.4%) | - |
Age group (months) | 0-11 | 0 (0.0%) | 44 (100%) | 0.002α* |
| | | | |
| 12-23 | 0 (0.0%) | 47 (100%) | - |
| 24-35 | 0 (0.0%) | 18 (100%) | - |
| 36-47 | 1 (5.6%) | 17 (94.4%) | - |
| 48-59 | 6 (15.4%) | 33 (84.6%) | - |
Malaria diagnosis | Yes | 3 (15.8%) | 16 (84.2%) | 0.03α* |
| No | 4 (2.7%) | 142 (97.3%) | - |
Pneumonia diagnosis | Yes | 0 (0.0%) | 3 (100%) | 1.00 |
| No | 7 (4.3%) | 155 (95.7%) | - |
Gastritis diagnosis | Yes | 0 (0.0%) | 6 (100%) | 1.00 |
| No | 7 (4.4%) | 152 (95.6%) | - |
The multivariate regression reported that children aged 48-59 months had approximately 10 times the odds of malnutrition compared to younger children (p=0.008). Also, recent malaria diseases increased the odds of malnutrition by nearly 7-fold (p=0.03), as shown in
Table 4.
Table 4. Multivariate Logistic Regression Analysis of Factors Associated with Malnutrition Among Children Under Five in Obuama Community.
Variable | Adjusted Odds Ratio (aOR) | 95% Confidence Interval | p-value |
Age group (months) | | | |
0-35 (Reference) | 1.00 | - | - |
36-47 | 2.8 | 0.22 - 35.4 | 0.42 |
48-59 | 9.7 | 1.82 - 51.5 | 0.008* |
Malaria diagnosis | | | |
No (Reference) | 1.00 | - | - |
Yes | 6.8 | 1.21 - 38.4 | 0.03* |
Model summary: Logistic regression model including age group and malaria diagnosis as covariates.
*Statistically significant at p < 0.05.
Figure 1. Prevalence of Malnutrition Among Under-Five Children in Obuama Community.
Figure 2. Health Conditions Distribution by Gender.
Figure 3. Malnutrition status by age group.
4. Discussion
This study reported a 2.4% prevalence of moderate acute malnutrition (MAM) based on MUAC measures and BMI-for-age classifications, which is lower than Nigeria's national acute malnutrition rate of 6.8%
| [5] | National Population Commission (NPC) [Nigeria], ICF International. Nigeria Demographic and Health Survey 2018. Abuja, Nigeria: NPC and ICF; 2019. |
[5]
. The low prevalence in Obuama may be attributed to local health efforts or seasonal food availability throughout the study period. However, the presence of severe acute malnutrition (SAM) in our sample (2.4% of children, all female) highlights potential gender disparities in nutritional status, which is consistent with the findings of Fentahun et al. (2018), who reported that cultural biases frequently lead to preferential feeding of male children
| [17] | Fentahun W, Alemseged F, Wakayo T. Gender disparities in nutritional status of under-five children in Ethiopia: evidence from the 2011 Ethiopia Demographic and Health Survey. Afr Health Sci. 2018; 18(1): 131-9. https://doi.org/10.4314/ahs.v18i1.18 |
[17]
. Although the difference was not statistically significant (p>0.05), six of the seven malnourished children were female. This trend suggests that female children might be at higher risk of malnutrition in this community, echoing the observed cultural patterns.
Notably, the study found occurrences of overweight (0.6%) and obesity (1.2%) among female children. This is consistent with global trends that show an increase in childhood obesity in low- and middle-income countries because of dietary shifts towards processed foods and sugary beverages. This occurrence is referred to as the "double burden of malnutrition," in which undernutrition and overnutrition coexist in the same population
| [18] | Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries. Nutr Rev. 2012; 70(1): 3-21. https://doi.org/10.1111/j.1753-4887.2011.00456.x |
| [19] | UNICEF. Improving Child Nutrition: The Achievable Imperative for Global Progress. New York: United Nations Children’s Fund (UNICEF); 2013. |
[18, 19]
. The prevalence of overweight and obesity in Obuama, especially in rural areas, may be attributed to increased urbanization and the adoption of Westernized diets
| [20] | Black RE, Allen LH, Bhutta ZA, Caulfield LE, de Onis M, Ezzati M, et al. Maternal and child undernutrition: global and regional exposures and health consequences. Lancet. 2008; 371 (9608): 243-60. https://doi.org/10.1016/S0140-6736(07)61690-0 |
[20]
. The finding that all overweight/obese children were females needs more research into gender-specific lifestyle and nutritional determinants.
Age was a key factor in this study. Malnutrition was reported only among children aged 3 years and above, with none of the infants under 12 months being malnourished. This may suggest that younger infants—potentially protected by breastfeeding and close maternal care—had better nutritional status, while nutritional deficits became prominent in older preschool children after weaning. Children aged 48-59 months had the highest prevalence of malnutrition (15.4%). This pattern may indicate cumulative effects of prolonged inadequate nutrition or repeated episodes of disease that retards growth in the later toddler years. This is not consistent with other studies that highlighted infancy (especially 6-23 months) as a critical period for undernutrition; however, in this community, older children might experience more diverse diet exposure (increasing risk of overnutrition) or prolonged suboptimal feeding, leading to undernutrition manifesting later.
Caregivers’ awareness was crucial, with 46.7% of them unable to assess their child's nutritional state. Senbanjo et al. (2013) reported a knowledge gap in Lagos, where maternal education had a substantial influence on child feeding behaviors
| [21] | Manyike PC, Chinawa JM, Ubesie AC, Obu HA, Nwokocha AR, Odetunde OI. Prevalence of malnutrition among pre-school children in South-east Nigeria. Ital J Pediatr. 2014; 40(1): 75. https://doi.org/10.1186/s13052-014-0075-5 |
[21]
. The disparity between nutritional status and caregivers’ perceptions (
Figure 1) emphasizes the need for improved community education. Most caregivers of malnourished children did not recognize the condition, which may delay intervention. Community-based nutrition education programs, as suggested by the United Nations Children Fund (UNICEF), have the potential to improve caregivers’ knowledge and encourage better feeding habits
| [22] | Chukwu KJ, Ubesie AC, Egbuna O. Under-five malnutrition in a south-eastern Nigeria metropolitan city: the challenges and implications. Afr Health Sci. 2019; 19(4): 3078-84. https://doi.org/10.4314/ahs.v19i4.42 |
[22]
.
Malaria (11.4%) and gastritis (3.6%) were frequent among the children assessed. There was a statistically significant link between malaria infection and malnutrition in children with a recent malaria episode: children with a recent malaria episode had a markedly higher malnutrition rate. This finding supports the link between malnutrition and infectious diseases, and malnutrition increases susceptibility to infections while infections are worsened by nutrient depletion
| [23] | Hamel MJ, Slutsker L, O’Meara WP, Otieno K, Bayoh N, Kamau A, et al. Malnutrition prevalence and program coverage in orphanages in Bauchi and Cross River States, Nigeria. BMC Public Health. 2015; 15: 942. https://doi.org/10.1186/s12889-015-2262-3 |
[23]
. According to Black et al. (2013), undernutrition accounts for 45% of all deaths in children under five years in Sub-Saharan Africa, emphasizing the importance of combined health and nutrition interventions
| [24] | Idowu OA, Akinyele IO, Oguntona EB, Oniang’o R, Oniang’o D. Nutritional status of children in displaced communities: a study in Abuja, Nigeria. Afr J Food Agric Nutr Dev. 2020; 20(3): 14175-91. https://doi.org/10.18697/ajfand.91.18664 |
[24]
. While malaria was associated with undernutrition, the number of reported cases of pneumonia and gastroenteritis was insignificant to conclude, and there was no significant association between malnutrition and these diseases. The low prevalence of pneumonia (1.8%) and gastritis (3.6%) may be due to the small sample size, which reduced the statistical power to show any effect of these diseases on nutritional status. The multivariate regression analysis reported that age above 48 months and malaria diagnosis were independent predictors of malnutrition after adjusting for confounders.
Comparative Analysis with Other Studies
The malnutrition prevalence in Obuama (2-3% acute malnutrition) was lower than the 10.8% prevalence reported in Okrika town, Rivers State, which has similar characteristics
| [7] | Okari TG, Nte AR, Frank BA. Prevalence of malnutrition in under-five children in Okrika Town. Niger J Paediatr. 2018; 45(2): 112-8. |
[7]
, and those reported in other regions of Nigeria. Studies in Ebonyi State and Enugu documented higher undernutrition rates of 9.7% and 5.9%, respectively, due to differences in agricultural productivity and healthcare access
| [25] | Federal Ministry of Health (Nigeria). National Strategic Plan of Action for Nutrition 2014-2019. Abuja, Nigeria: FMOH; 2014. |
| [26] | World Health Organization. Integrated Management of Childhood Illness: Chart Booklet. Geneva: WHO; 2014. |
[25, 26]
. The findings also showed that overweight rates in this rural community, though low, were consistent with reports from more urban parts of Nigeria, suggesting that rural areas are not immune to the global childhood obesity epidemic
| [27] | Nigeria Federal Ministry of Health. National Policy on Food and Nutrition. Abuja: FMOH; 2016. |
[27]
. The coexistence of undernutrition and overnutrition in Obuama reflects the national trend of a double burden of malnutrition.
The level of awareness in Obuama agrees with those reported in a 2020 study of internally displaced persons (IDP) camps in Abuja, where a considerable proportion of mothers could not correctly assess their child’s nutritional status
| [28] | United Nations Children’s Fund (UNICEF). Nigeria: Situation Analysis of Children and Women. Abuja: UNICEF; 2017. |
[28]
. This suggests the need for nationwide nutritional education and better growth monitoring practices.
Strengths and Limitations
Strengths: This study used WHO-standardized anthropometric measures (MUAC and BMI-for-age) to assess nutritional status, enhancing the validity and comparability of the findings. The use of both MUAC and BMI-for-age provided a comprehensive assessment of acute malnutrition and chronic nutritional status.
Limitations: The cross-sectional design limits causal inference while showing associations (e.g., between malaria and malnutrition), but the direction of these relationships is unconfirmed. The sample size was small for detecting associations with low-prevalence conditions like pneumonia, which may explain the no significant findings for such health conditions. Additionally, seasonal factors (such as post-harvest food availability or seasonal disease outbreaks) at the time of data collection could have influenced the results. This study was in a single rural community. So, the findings may not apply to other settings. Also, there is the issue of measurement errors (e.g., weight, height), which may lead to misclassification.
5. Conclusion
The study showed that malnutrition was prevalent among children in Obuama community, and cases of overweight and obesity were reported, highlighting the need for caregiver education and targeted nutritional interventions. After adjusting for confounders in the multivariate regression analysis, age above 48 months and malaria were independent predictors of malnutrition. These findings emphasized the importance of targeting older preschool-aged children for nutritional interventions and preventing malaria to reduce malnutrition in riverine communities.
6. Recommendations for Policy and Practice
1) Community Nutrition Programs: The Rivers State Primary Health Care Management Board (RSPHCMB) should implement community-based caregiver education on balanced child diets, exclusive breastfeeding, proper weaning practices, and regular growth monitoring
| [29] | Federal Ministry of Health (Nigeria), UNICEF. National Guidelines for Community Management of Acute Malnutrition. Abuja: FMOH; 2011. |
[29]
. This will enhance caregivers’ knowledge in early identification and prevention of malnutrition.
2) Healthcare Integration: The RSPHCMB should integrate malnutrition screening and management into routine pediatrics care, especially in malaria control programs
| [30] | Nigeria Centre for Disease Control. National Guidelines for Integrated Disease Surveillance and Response. Abuja: NCDC; 2019. |
[30]
. For example, during childhood malaria treatment visits, children should be screened for malnutrition, and on the other hand, malnourished children should be assessed and treated for common infections like malaria.
3) Further Research: Longitudinal studies are recommended to assess nutritional status through different seasons and in children above five years. Such studies would clarify the timing of the onset of malnutrition and the long-term impacts of early childhood nutrition in this community. Also, qualitative research into cultural feeding practices in Obuama may shed more light on the gender differences seen in nutritional outcomes.
Abbreviations
MUAC | Mid-Upper Arm Circumference |
BMI | Body Mass Index |
WHO | World Health Organization |
PEM | Protein-energy Malnutrition |
CMAM | Community-Based Management of Acute Malnutrition |
SPSS | Statistical Product and Service Solution Package |
LMICs | Low- and Middle-income Countries |
RSPHCMB | Rivers State Primary Health Care Management Board |
Acknowledgments
The authors do acknowledge the Chiefs, opinion leaders, heads of households, local guides, and the mothers of Obuama community for their cooperation during the research.
Author Contributions
Ifeoma Nwaduito: Conceptualization, Data curation, Formal Analysis, Methodology, Supervision, Validation, Visualization, Writing - original draft.
Nduye Christie Tobin Briggs: Conceptualization, Data curation, Formal Analysis, Methodology, Supervision, Validation, Writing - review & editing.
Pauline Aruoture Green: Data curation, Methodology, Validation, Writing - review & editing.
Nnanna Victor Onyekwere: Data curation, Methodology, Supervision, Validation, Writing - review & editing.
Ositadinma Mberekpe Pius: Data curation, Methodology, Supervision, Validation, Writing - review & editing.
Uwowa Gogo Obediah: Data curation, Methodology, Writing - review & editing.
Ekeneotumu Thompson Geoffrey: Data curation, Methodology, Writing - review & editing.
Funding
The research received no external financial support.
Data Availability Statement
The database used and analyzed for the study is available from the corresponding author and will be available on request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
World Health Organization. Malnutrition. 2024 [cited 2025 Mar 26]. Available from:
https://www.who.int/health-topics/malnutrition.
|
| [2] |
UNICEF. Levels and Trends in Child Malnutrition. 2023 [cited 2025 Mar 26]. Available from:
https://data.unicef.org/topic/nutrition/malnutrition/
|
| [3] |
Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, de Onis M, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013; 382 (9890): 427-51.
https://doi.org/10.1016/S0140-6736(13)60937-X
|
| [4] |
de Onis M, Branca F. Childhood stunting: a global perspective. Matern Child Nutr. 2016; 12 (Suppl 1): 12-26.
https://doi.org/10.1111/mcn.12231
|
| [5] |
National Population Commission (NPC) [Nigeria], ICF International. Nigeria Demographic and Health Survey 2018. Abuja, Nigeria: NPC and ICF; 2019.
|
| [6] |
Smith J, Doe A, Johnson C. Malnutrition in rural Nigerian communities: socio-economic and environmental determinants. J Rural Health. 2017; 33(3): 300-10.
|
| [7] |
Okari TG, Nte AR, Frank BA. Prevalence of malnutrition in under-five children in Okrika Town. Niger J Paediatr. 2018; 45(2): 112-8.
|
| [8] |
Adebayo O. Prevalence of malnutrition in rural communities of Nigeria. J Public Health Res. 2022; 11(1): e2022001.
https://doi.org/10.4081/jphr.2022.2022001
|
| [9] |
Bhutta ZA, Das JK, Rizvi A, Gaffey MF, Walker N, Horton S, et al. Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost? Lancet. 2013; 382 (9890): 452-77.
https://doi.org/10.1016/S0140-6736(13)60996-4
|
| [10] |
Owino V, Ahmed T, Freemark M, Kelly P, Loy A, Manary M, et al. Environmental enteric dysfunction and growth failure/stunting in global child health. J Pediatr Gastroenterol Nutr. 2020; 70(1): 6-21.
https://doi.org/10.1097/MPG.0000000000002498
|
| [11] |
Senbanjo IO, Oshikoya KA, Odusanya OO, Njokanma OF. Maternal and child under-nutrition in rural and urban communities of Lagos State, Nigeria: the relationship and risk factors. Matern Child Nutr. 2013; 9(4): 365-79.
https://doi.org/10.1111/j.1740-8709.2011.00396.x
|
| [12] |
Guerrant RL, DeBoer MD, Moore SR, Scharf RJ, Lima AA. The impoverished gut—a triple burden of diarrhoea, stunting and chronic disease. Nat Rev Gastroenterol Hepatol. 2013; 10(4): 220-9.
https://doi.org/10.1038/nrgastro.2012.239
|
| [13] |
Save the Children (Nigeria). Community-Based Management of Acute Malnutrition (CMAM). 2022 [cited 2025 Mar 26]. Available from:
https://nigeria.savethechildren.net/
|
| [14] |
Ogunniyi K, Oyebade A, Atolagbe J. Prevalence and determinants of malnutrition among under-five children in Southwest Nigeria. Int J Community Med Public Health. 2023; 10(4): 1308-15.
https://doi.org/10.18203/2394-6040.ijcmph20230905
|
| [15] |
Popkin BM, Corvalan C, Grummer-Strawn LM. Dynamics of the double burden of malnutrition: the changing nutrition reality. Lancet. 2020; 395(10217): 65-74.
https://doi.org/10.1016/S0140-6736(19)32497-3
|
| [16] |
Wells JC, Sawaya AL, Wibaek R, Mwangome M, Poullas MS, Yajnik CS, et al. The double burden of malnutrition: aetiological pathways and consequences. Lancet. 2020; 395 (10217): 75-88.
https://doi.org/10.1016/S0140-6736(19)32472-9
|
| [17] |
Fentahun W, Alemseged F, Wakayo T. Gender disparities in nutritional status of under-five children in Ethiopia: evidence from the 2011 Ethiopia Demographic and Health Survey. Afr Health Sci. 2018; 18(1): 131-9.
https://doi.org/10.4314/ahs.v18i1.18
|
| [18] |
Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries. Nutr Rev. 2012; 70(1): 3-21.
https://doi.org/10.1111/j.1753-4887.2011.00456.x
|
| [19] |
UNICEF. Improving Child Nutrition: The Achievable Imperative for Global Progress. New York: United Nations Children’s Fund (UNICEF); 2013.
|
| [20] |
Black RE, Allen LH, Bhutta ZA, Caulfield LE, de Onis M, Ezzati M, et al. Maternal and child undernutrition: global and regional exposures and health consequences. Lancet. 2008; 371 (9608): 243-60.
https://doi.org/10.1016/S0140-6736(07)61690-0
|
| [21] |
Manyike PC, Chinawa JM, Ubesie AC, Obu HA, Nwokocha AR, Odetunde OI. Prevalence of malnutrition among pre-school children in South-east Nigeria. Ital J Pediatr. 2014; 40(1): 75.
https://doi.org/10.1186/s13052-014-0075-5
|
| [22] |
Chukwu KJ, Ubesie AC, Egbuna O. Under-five malnutrition in a south-eastern Nigeria metropolitan city: the challenges and implications. Afr Health Sci. 2019; 19(4): 3078-84.
https://doi.org/10.4314/ahs.v19i4.42
|
| [23] |
Hamel MJ, Slutsker L, O’Meara WP, Otieno K, Bayoh N, Kamau A, et al. Malnutrition prevalence and program coverage in orphanages in Bauchi and Cross River States, Nigeria. BMC Public Health. 2015; 15: 942.
https://doi.org/10.1186/s12889-015-2262-3
|
| [24] |
Idowu OA, Akinyele IO, Oguntona EB, Oniang’o R, Oniang’o D. Nutritional status of children in displaced communities: a study in Abuja, Nigeria. Afr J Food Agric Nutr Dev. 2020; 20(3): 14175-91.
https://doi.org/10.18697/ajfand.91.18664
|
| [25] |
Federal Ministry of Health (Nigeria). National Strategic Plan of Action for Nutrition 2014-2019. Abuja, Nigeria: FMOH; 2014.
|
| [26] |
World Health Organization. Integrated Management of Childhood Illness: Chart Booklet. Geneva: WHO; 2014.
|
| [27] |
Nigeria Federal Ministry of Health. National Policy on Food and Nutrition. Abuja: FMOH; 2016.
|
| [28] |
United Nations Children’s Fund (UNICEF). Nigeria: Situation Analysis of Children and Women. Abuja: UNICEF; 2017.
|
| [29] |
Federal Ministry of Health (Nigeria), UNICEF. National Guidelines for Community Management of Acute Malnutrition. Abuja: FMOH; 2011.
|
| [30] |
Nigeria Centre for Disease Control. National Guidelines for Integrated Disease Surveillance and Response. Abuja: NCDC; 2019.
|
Cite This Article
-
APA Style
Nwadiuto, I., Briggs, N. C. T., Green, P. A., Onyekwere, N. V., Pius, O. M., et al. (2025). Prevalence and Determinants of Malnutrition Among Under-Five Children in Obuama Community, Rivers State, Nigeria: A Community-Based Analytical Cross-Sectional Study. World Journal of Public Health, 10(3), 316-324. https://doi.org/10.11648/j.wjph.20251003.22
 Copy
|
Copy
|
 Download
Download
ACS Style
Nwadiuto, I.; Briggs, N. C. T.; Green, P. A.; Onyekwere, N. V.; Pius, O. M., et al. Prevalence and Determinants of Malnutrition Among Under-Five Children in Obuama Community, Rivers State, Nigeria: A Community-Based Analytical Cross-Sectional Study. World J. Public Health 2025, 10(3), 316-324. doi: 10.11648/j.wjph.20251003.22
Copy
|
Download
AMA Style
Nwadiuto I, Briggs NCT, Green PA, Onyekwere NV, Pius OM, et al. Prevalence and Determinants of Malnutrition Among Under-Five Children in Obuama Community, Rivers State, Nigeria: A Community-Based Analytical Cross-Sectional Study. World J Public Health. 2025;10(3):316-324. doi: 10.11648/j.wjph.20251003.22
Copy
|
Download
-
@article{10.11648/j.wjph.20251003.22,
author = {Ifeoma Nwadiuto and Nduye Christie Tobin Briggs and Pauline Aruoture Green and Nnanna Victor Onyekwere and Ositadinma Mberekpe Pius and Uwowa Gogo Obediah and Ekeneotumu Thompson Geoffrey},
title = {Prevalence and Determinants of Malnutrition Among Under-Five Children in Obuama Community, Rivers State, Nigeria: A Community-Based Analytical Cross-Sectional Study
},
journal = {World Journal of Public Health},
volume = {10},
number = {3},
pages = {316-324},
doi = {10.11648/j.wjph.20251003.22},
url = {https://doi.org/10.11648/j.wjph.20251003.22},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20251003.22},
abstract = {Background: Malnutrition is a significant public health challenge, particularly among children under the age of five, with severe implications for growth, development, and long-term health outcomes. This study assessed the prevalence and determinants of malnutrition in children under five years old in Obuama Community, Degema Local Government Area, Rivers State, Nigeria. Methods: An Analytical cross-sectional study was conducted using a multi-stage sampling technique for four months (19th August - 21st of November 2024). Anthropometric measurements, including mid-upper arm circumference (MUAC), weight, height, and World Health Organization (WHO) growth standards, were used to assess the nutritional status of 165 children. Data analysis was performed using the Statistical Product and Service Solution Package (SPSS) Version 27. Results: The study showed a low prevalence of acute malnutrition (2.4%) based on MUAC measurements. Among the children, 2.4% reported moderate undernutrition, 0.6% were overweight, and 1.2% were obese, using the BMI-for-age assessments. Substantially more malnutrition was also shown in children 36 months and older and in those with malaria (p < 0.05). The caregivers reported limited awareness of their children’s nutritional status, with 46.7% expressing uncertainty about whether their child was malnourished. Children aged above 48 months and malaria diagnosis were independent predictors of malnutrition (p < 0.05). Conclusion: Malnutrition was prevalent among children in Obuama community. The observation of both undernutrition and overnutrition (overweight and obesity) highlights a dual burden of malnutrition. The findings emphasized the need for targeted nutritional interventions, including caregivers’ education on proper infant and young child feeding practices, early detection of malnutrition, and strategies to address both undernutrition and obesity. Public health programs should also integrate malaria prevention and treatment as part of a comprehensive effort to reduce malnutrition.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Prevalence and Determinants of Malnutrition Among Under-Five Children in Obuama Community, Rivers State, Nigeria: A Community-Based Analytical Cross-Sectional Study
AU - Ifeoma Nwadiuto
AU - Nduye Christie Tobin Briggs
AU - Pauline Aruoture Green
AU - Nnanna Victor Onyekwere
AU - Ositadinma Mberekpe Pius
AU - Uwowa Gogo Obediah
AU - Ekeneotumu Thompson Geoffrey
Y1 - 2025/08/05
PY - 2025
N1 - https://doi.org/10.11648/j.wjph.20251003.22
DO - 10.11648/j.wjph.20251003.22
T2 - World Journal of Public Health
JF - World Journal of Public Health
JO - World Journal of Public Health
SP - 316
EP - 324
PB - Science Publishing Group
SN - 2637-6059
UR - https://doi.org/10.11648/j.wjph.20251003.22
AB - Background: Malnutrition is a significant public health challenge, particularly among children under the age of five, with severe implications for growth, development, and long-term health outcomes. This study assessed the prevalence and determinants of malnutrition in children under five years old in Obuama Community, Degema Local Government Area, Rivers State, Nigeria. Methods: An Analytical cross-sectional study was conducted using a multi-stage sampling technique for four months (19th August - 21st of November 2024). Anthropometric measurements, including mid-upper arm circumference (MUAC), weight, height, and World Health Organization (WHO) growth standards, were used to assess the nutritional status of 165 children. Data analysis was performed using the Statistical Product and Service Solution Package (SPSS) Version 27. Results: The study showed a low prevalence of acute malnutrition (2.4%) based on MUAC measurements. Among the children, 2.4% reported moderate undernutrition, 0.6% were overweight, and 1.2% were obese, using the BMI-for-age assessments. Substantially more malnutrition was also shown in children 36 months and older and in those with malaria (p < 0.05). The caregivers reported limited awareness of their children’s nutritional status, with 46.7% expressing uncertainty about whether their child was malnourished. Children aged above 48 months and malaria diagnosis were independent predictors of malnutrition (p < 0.05). Conclusion: Malnutrition was prevalent among children in Obuama community. The observation of both undernutrition and overnutrition (overweight and obesity) highlights a dual burden of malnutrition. The findings emphasized the need for targeted nutritional interventions, including caregivers’ education on proper infant and young child feeding practices, early detection of malnutrition, and strategies to address both undernutrition and obesity. Public health programs should also integrate malaria prevention and treatment as part of a comprehensive effort to reduce malnutrition.
VL - 10
IS - 3
ER -
Copy
|
Download