Saber-sheath trachea is a deformation of the trachea characterized by a tracheal index of less than 0.67, commonly found in patients with chronic obstructive pulmonary disease (COPD). This condition can lead to symptoms such as shortness of breath, coughing, and recurrent respiratory infections, which may necessitate surgical intervention. We present the case of a 72-year-old male with a left upper pulmonary lobe tumor scheduled for thoracoscopic lobectomy. The patient exhibited severe emphysema and had a tracheal index of 0.28, indicating a significantly narrowed intrathoracic trachea. Preoperative assessments revealed stable vital signs and low risk for perioperative complications, allowing for standard noninvasive monitoring during the procedure. Anesthesia was induced while maintaining spontaneous breathing using inhalation anesthetics. A left-sided double-lumen endotracheal tube was successfully placed for lung isolation. Throughout the surgery, airway pressures remained below 20 cm H2O, and the patient tolerated ventilation well. Following the procedure, fiberoptic bronchoscopy confirmed the absence of airway complications. The patient experienced a smooth recovery, was discharged after 6 days, and reported feeling well at the 3-month follow-up. This case underscores the importance of careful anesthetic management in patients with saber-sheath trachea undergoing thoracic surgery.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Saber-sheath trachea is a deformation of the trachea in the thoracic cavity, and the ratio of the coronal diameter to the sagittal diameter of the trachea in the intrathoracic segment (tracheal index) is <0.67 (2/3)
[1]
Wallace E J, Chung F. General anesthesia in a patient with an enlarged saber sheath trachea [J]. Anesthesiology, 1998, 88(2): 527-9.
. The notable belief is that this change is due to displacement and remodeling of the tracheal cartilage rings caused by prolonged intrathoracic pressure elevation. Most current studies confirm that it is commonly observed in patients with chronic obstructive pulmonary disease (COPD)
[2]
Greene R. "Saber-sheath" trachea: relation to chronic obstructive pulmonary disease [J]. AJR Am J Roentgenol, 1978, 130(3): 441-5.
Greene R, Lechner G L. "Saber-Sheath" Trachea: A Clinical and Functional Study of Marked Coronal Narrowing of the Intrathoracic Trachea [J]. Radiology, 1975, 115(2): 265-8.
Trigaux J P, Hermes G, Dubois P, et al. CT of saber-sheath trachea. Correlation with clinical, chest radiographic and functional findings [J]. Acta Radiol, 1994, 35(3): 247-50.
[5]
Tsao T C, Shieh W B. Intrathoracic tracheal dimensions and shape changes in chronic obstructive pulmonary disease [J]. J Formos Med Assoc, 1994, 93(1): 30-4.
[6]
Wielputz M O, Eberhardt R, Puderbach M, et al. Simultaneous assessment of airway instability and respiratory dynamics with low-dose 4D-CT in chronic obstructive pulmonary disease: a technical note [J]. Respiration, 2014, 87(4): 294-300.
. Patients with saber-sheath trachea may present with symptoms such as shortness of breath, coughing, wheezing, and recurrent respiratory infections. Diagnosis is typically made through imaging studies, such as computed tomography (CT) scans or bronchoscopy
[3]
Greene R, Lechner G L. "Saber-Sheath" Trachea: A Clinical and Functional Study of Marked Coronal Narrowing of the Intrathoracic Trachea [J]. Radiology, 1975, 115(2): 265-8.
Trigaux J P, Hermes G, Dubois P, et al. CT of saber-sheath trachea. Correlation with clinical, chest radiographic and functional findings [J]. Acta Radiol, 1994, 35(3): 247-50.
[8]
Pilate I, Impens N, Joe G T, et al. CT of "saber-sheath" trachea [J]. J Belge Radiol, 1987, 70(3): 183-7.
[3, 4, 8]
. Surgery for the saber-sheath trachea may be considered in the following situations: severe respiratory symptoms that significantly impact the patient's quality of life; persistent or recurrent respiratory infections; failure to respond to conservative treatments such as medications or pulmonary rehabilitation; and progressive narrowing of the trachea. When inducing general anesthesia, a smaller endotracheal tube may be chosen due to the narrowed trachea, and careful attention should be given to tube placement to avoid damage to the tracheal structures. We report the case of a patient with a saber-sheath trachea who underwent thoracic surgery via a lung isolation technique involving the use of a double-lumen endotracheal tube.
2. Case Report
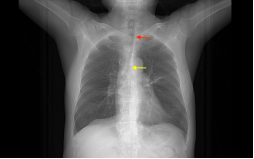
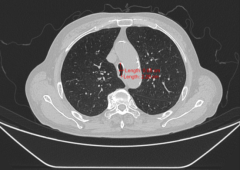
A 72-year-old man with a height of 165 cm, a weight of 61 kg, and a left upper pulmonary lobe tumor was scheduled for thoracoscopic lobectomy. Showing a barrel-shaped chest, he suffered from COPD with chronic productive cough. Pulmonary function tests revealed severe emphysema with a predicted FEV1 value of 49.8%, an FEV1/FVC of 52.84%, and arterial blood gas analysis with a paO2 of 67 mmHg, a paCO2 of 41 mmHg, and a pH of 7,442. Chest CT suggested a narrow scabrid and intrathoracic trachea, with a 0.65 cm coronal and 2.28 cm sagittal diameter, resulting in a tracheal index of 0.28 (Figures 1 and 2).
Figure 2. Coronal and sagittal tracheal diameter at the height of the aortic arch: tracheal index of 0.28.
Based on the results of the preoperative assessment, the patient was at low risk of circulatory fluctuations during the perioperative period, the duration of the procedure was short, and the likelihood of severe changes in homeostasis was low; therefore, we chose to use standard noninvasive monitoring, including electrocardiograms, finger pulse oxygen saturation, end-expiratory carbon dioxide, and noninvasive blood pressure. Upon entering the operating room, the patient had no obvious signs of respiratory obstruction, and the monitor showed stable vital signs. Since the patient had no previous diagnosis of "saber-sheath trachea", the possibility that his tracheal stenosis was caused by external compression could not be completely excluded; therefore, it would be safer to induce anesthesia while maintaining spontaneous breathing. Inhalation anesthetics were used to ensure that the patient's spontaneous breathing was maintained. After confirming that the patient had no airway obstruction during sleep, we administered 12 mg of cisatracurium and 20 µg of sufentanil intravenously. Under satisfactory muscle relaxation, direct laryngoscopy revealed grade 1 Cormack-Lehane visualization. A 32F-left double-lumen was inserted smoothly with no significant resistance and satisfactory isolation of the left and right lung airways. The patient was positioned in the right lateral position, and mechanical ventilation (volume controlled, 450 ml/min, 12 breaths/min, airway pressure 15 cm H2O) was started after verifying the correct tube position.
At the start of the procedure, the catheter on the left side was closed, and ventilation of the right lung alone was initiated. The tidal volume was set at 300 ml/min, and the respiratory rate was 15 breaths/min. The ventilator showed an airway pressure of 17 cmH2O. Throughout the procedure, his airway pressure did not exceed 20 cmH2O, and his end-expiratory CO2 and finger pulse oxygen levels were both within the normal range. After the completion of the procedure, we removed the double-lumen endotracheal tubes and placed a laryngeal mask for flexible fiberoptic bronchoscopy (FOB). FOB confirmed that the patient's airway mucosa was not bleeding and did not rupture. Because neuromuscular monitoring was not performed, to avoid reversal of the residual neuromuscular block, the patient was given intravenous neostigmine after recovery of spontaneous breathing. The patient recovered well 6 days after surgery and was discharged from the hospital. At the 3-month follow-up after surgery, the patient felt well.
3. Discussion
The saber-sheath trachea was first described in cadavers by pathologist Simmonds
. A diagnosis requires the following criteria: (1) an intrathoracic tracheal index (coronal/sagittal diameter) <2/3, (2) no evidence of a mediastinal mass, (3) narrowing of the entire length of the intrathoracic trachea, (4) abrupt coronal tracheal widening at the thoracic outlet, and (5) thickening of the tracheal wall with ring-like ossifications of the cartilage
[2]
Greene R. "Saber-sheath" trachea: relation to chronic obstructive pulmonary disease [J]. AJR Am J Roentgenol, 1978, 130(3): 441-5.
. The most notable belief is that the saber-sheath trachea is mainly found in patients with chronic obstructive pulmonary disease, which may be caused by deformation and remodeling of the tracheal cartilage rings due to prolonged cough and increased intrathoracic pressure from hyperinflation of the lungs
[10]
Callan E, Karandy E J, Hilsinger R L, Jr. "Saber-sheath" trachea [J]. Ann Otol Rhinol Laryngol, 1988, 97(5 Pt 1): 512-5.
. Although this patient did not have significant emphysema on chest CT, he had prolonged cough and sputum production preoperatively, a typical barrel chest on physical examination, pulmonary function test results showing a significant decrease in FEV1/FVC and blood gas analysis confirming type I respiratory failure, and a diagnosis of chronic obstructive pulmonary disease was made.
Although the incidence of “saber-sheath trachea” is low in COPD patients, the degree of airway stenosis in such patients correlates with FEV1/FVC values
[11]
Ciccarese F, Poerio A, Stagni S, et al. Saber-sheath trachea as a marker of severe airflow obstruction in chronic obstructive pulmonary disease [J]. Radiol Med, 2014, 119(2): 90-6.
, suggesting that anesthesiologists should consider chest imaging for patients with low FEV1/FVC values when performing preoperative evaluation. In addition to routine airway assessment, the anesthesiologist should know where the tracheal stenosis begins and ends, measure the length of the stenosis, measure the diameter of the trachea at the narrowest point and confirm whether the patient has a preferred body position, difficulty breathing while lying down, and difficulty sleeping due to difficulty breathing. If there are no contraindications, the induction of anesthesia without mechanical ventilation, such as intrathecal anesthesia or regional block, is the best option for the procedure. If the patient must be intubated, the anesthesiologist should choose a smaller tracheal tube based on the severity of the tracheal stenosis. At the end of the procedure, the endotracheal tube should be removed after ensuring that the patient's muscle strength and consciousness have fully recovered to avoid hypoxia or even asphyxiation due to the residual effects of drugs, and muscle relaxation should be monitored throughout the procedure.
Based on the height, weight, and normal tracheal dimensions of the patient, a 37F double-lumen tracheal tube. However, the patient's chest CT suggested a “saber-sheath trachea” with a tracheal index of 0.28 at the narrowest point and a tracheal index of 0.49 at 1 cm above the aortic arch. At the same time, CT images suggest calcification around the narrowed trachea, which may limit tracheal flexibility. The use of an excessively thick endotracheal tube might cause the trachea to rupture
[12]
Marty-Ane C H, Picard E, Jonquet O, et al. Membranous tracheal rupture after endotracheal intubation [J]. Ann Thorac Surg, 1995, 60(5): 1367-71.
. However, there are no clear criteria or formulas for the selection of catheter type when inserting a double-lumen endotracheal tube in patients with “saber-sheath trachea”. The choice of the tube should be based on a combination of the normal tracheal ring diameter and the tracheal index. The size of the double-lumen endotracheal tube is first determined by the patient's normal tracheal diameter. If the tracheal index is between 0.5 and 0.7, a catheter one size smaller than normal is used; if the tracheal index is less than 0.5, a catheter two or even three sizes smaller than normal is used. In the absence of conclusive evidence, such a recommendation is risky. It is hoped that more clinical studies will focus on patients with this type of disease and that recommendations for catheter selection in such patients can be developed in the future. If the anesthesiologist is strongly concerned about the airway, a bronchial blocking tube may also be considered. However, the advantages and disadvantages of bronchial blocking tubes should be fully understood before they are used. The diameter of the blocking tube is very small and causes very little damage to the airway mucosa, but it is very easy to displace
[14]
Weigeldt M, Paul M, Schulz-Drost S, et al. [Anesthesia, ventilation and pain treatment in thoracic trauma] [J]. Unfallchirurg, 2018, 121(8): 634-641.
. When performing tracheal intubation in patients with “saber-sheath trachea”, FOB should be used for guidance to better visualize the narrowed trachea and to avoid injuries caused by blind insertion. Due to a lack of experience, FOB was not performed on the patient. Before extubation, an examination of the airway was conducted by inserting a flexible fiberoptic bronchoscope through a laryngeal mask, and fortunately, there was no significant airway damage. Previous researchers have experimented with a method of intubation in which a laryngeal mask is placed to ensure patient ventilation. Then, a tracheal tube is inserted through the laryngeal mask, and the tip of the tube is positioned proximal to the stenotic segment. An exchange catheter is placed 2 cm above the tracheal carina, which ensures that the tracheal tube can be reinserted smoothly through the exchange catheter and that jet ventilation can be allowed in cases of accidental intubation
[15]
Asai T, Shingu K. Airway management of a patient with tracheal stenosis for surgery in the prone position [J]. Can J Anaesth, 2004, 51(7): 733-6.
In summary, airway protection is the most important step in the perioperative period for patients with a saber-sheath trachea. It is recommended that the anesthesiologist first choose an anesthetic that does not require tracheal intubation. If the patient must be extubated, the smallest possible endotracheal tube should be chosen to ensure that carbon dioxide retention or hypoxemia does not occur. After the procedure, FOB should be performed to confirm that there is no rupture or bleeding in the airway.
Acknowledgments
Not applicable.
Author Contributions
XW collected case information, reviewed the literature, and drafted the manuscript. YW have revised the language corrections and structure of sentences in the manuscript.
Consent for Publication
Not applicable.
Funding
This work is not supported by any external funding.
Data Availability Statement
The data supporting the outcome of this research work has been reported in this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Wallace E J, Chung F. General anesthesia in a patient with an enlarged saber sheath trachea [J]. Anesthesiology, 1998, 88(2): 527-9.
Greene R, Lechner G L. "Saber-Sheath" Trachea: A Clinical and Functional Study of Marked Coronal Narrowing of the Intrathoracic Trachea [J]. Radiology, 1975, 115(2): 265-8.
Trigaux J P, Hermes G, Dubois P, et al. CT of saber-sheath trachea. Correlation with clinical, chest radiographic and functional findings [J]. Acta Radiol, 1994, 35(3): 247-50.
[5]
Tsao T C, Shieh W B. Intrathoracic tracheal dimensions and shape changes in chronic obstructive pulmonary disease [J]. J Formos Med Assoc, 1994, 93(1): 30-4.
[6]
Wielputz M O, Eberhardt R, Puderbach M, et al. Simultaneous assessment of airway instability and respiratory dynamics with low-dose 4D-CT in chronic obstructive pulmonary disease: a technical note [J]. Respiration, 2014, 87(4): 294-300.
Ciccarese F, Poerio A, Stagni S, et al. Saber-sheath trachea as a marker of severe airflow obstruction in chronic obstructive pulmonary disease [J]. Radiol Med, 2014, 119(2): 90-6.
Wan, Y., Wang, X. (2024). Anesthetic Management of a Patient with Saber-Sheath Trachea. Cardiology and Cardiovascular Research, 8(3), 83-86. https://doi.org/10.11648/j.ccr.20240803.11
@article{10.11648/j.ccr.20240803.11,
author = {Ying Wan and Xin Wang},
title = {Anesthetic Management of a Patient with Saber-Sheath Trachea
},
journal = {Cardiology and Cardiovascular Research},
volume = {8},
number = {3},
pages = {83-86},
doi = {10.11648/j.ccr.20240803.11},
url = {https://doi.org/10.11648/j.ccr.20240803.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20240803.11},
abstract = {Saber-sheath trachea is a deformation of the trachea characterized by a tracheal index of less than 0.67, commonly found in patients with chronic obstructive pulmonary disease (COPD). This condition can lead to symptoms such as shortness of breath, coughing, and recurrent respiratory infections, which may necessitate surgical intervention. We present the case of a 72-year-old male with a left upper pulmonary lobe tumor scheduled for thoracoscopic lobectomy. The patient exhibited severe emphysema and had a tracheal index of 0.28, indicating a significantly narrowed intrathoracic trachea. Preoperative assessments revealed stable vital signs and low risk for perioperative complications, allowing for standard noninvasive monitoring during the procedure. Anesthesia was induced while maintaining spontaneous breathing using inhalation anesthetics. A left-sided double-lumen endotracheal tube was successfully placed for lung isolation. Throughout the surgery, airway pressures remained below 20 cm H2O, and the patient tolerated ventilation well. Following the procedure, fiberoptic bronchoscopy confirmed the absence of airway complications. The patient experienced a smooth recovery, was discharged after 6 days, and reported feeling well at the 3-month follow-up. This case underscores the importance of careful anesthetic management in patients with saber-sheath trachea undergoing thoracic surgery.
},
year = {2024}
}
TY - JOUR
T1 - Anesthetic Management of a Patient with Saber-Sheath Trachea
AU - Ying Wan
AU - Xin Wang
Y1 - 2024/08/20
PY - 2024
N1 - https://doi.org/10.11648/j.ccr.20240803.11
DO - 10.11648/j.ccr.20240803.11
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 83
EP - 86
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20240803.11
AB - Saber-sheath trachea is a deformation of the trachea characterized by a tracheal index of less than 0.67, commonly found in patients with chronic obstructive pulmonary disease (COPD). This condition can lead to symptoms such as shortness of breath, coughing, and recurrent respiratory infections, which may necessitate surgical intervention. We present the case of a 72-year-old male with a left upper pulmonary lobe tumor scheduled for thoracoscopic lobectomy. The patient exhibited severe emphysema and had a tracheal index of 0.28, indicating a significantly narrowed intrathoracic trachea. Preoperative assessments revealed stable vital signs and low risk for perioperative complications, allowing for standard noninvasive monitoring during the procedure. Anesthesia was induced while maintaining spontaneous breathing using inhalation anesthetics. A left-sided double-lumen endotracheal tube was successfully placed for lung isolation. Throughout the surgery, airway pressures remained below 20 cm H2O, and the patient tolerated ventilation well. Following the procedure, fiberoptic bronchoscopy confirmed the absence of airway complications. The patient experienced a smooth recovery, was discharged after 6 days, and reported feeling well at the 3-month follow-up. This case underscores the importance of careful anesthetic management in patients with saber-sheath trachea undergoing thoracic surgery.
VL - 8
IS - 3
ER -
Wan, Y., Wang, X. (2024). Anesthetic Management of a Patient with Saber-Sheath Trachea. Cardiology and Cardiovascular Research, 8(3), 83-86. https://doi.org/10.11648/j.ccr.20240803.11
@article{10.11648/j.ccr.20240803.11,
author = {Ying Wan and Xin Wang},
title = {Anesthetic Management of a Patient with Saber-Sheath Trachea
},
journal = {Cardiology and Cardiovascular Research},
volume = {8},
number = {3},
pages = {83-86},
doi = {10.11648/j.ccr.20240803.11},
url = {https://doi.org/10.11648/j.ccr.20240803.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20240803.11},
abstract = {Saber-sheath trachea is a deformation of the trachea characterized by a tracheal index of less than 0.67, commonly found in patients with chronic obstructive pulmonary disease (COPD). This condition can lead to symptoms such as shortness of breath, coughing, and recurrent respiratory infections, which may necessitate surgical intervention. We present the case of a 72-year-old male with a left upper pulmonary lobe tumor scheduled for thoracoscopic lobectomy. The patient exhibited severe emphysema and had a tracheal index of 0.28, indicating a significantly narrowed intrathoracic trachea. Preoperative assessments revealed stable vital signs and low risk for perioperative complications, allowing for standard noninvasive monitoring during the procedure. Anesthesia was induced while maintaining spontaneous breathing using inhalation anesthetics. A left-sided double-lumen endotracheal tube was successfully placed for lung isolation. Throughout the surgery, airway pressures remained below 20 cm H2O, and the patient tolerated ventilation well. Following the procedure, fiberoptic bronchoscopy confirmed the absence of airway complications. The patient experienced a smooth recovery, was discharged after 6 days, and reported feeling well at the 3-month follow-up. This case underscores the importance of careful anesthetic management in patients with saber-sheath trachea undergoing thoracic surgery.
},
year = {2024}
}
TY - JOUR
T1 - Anesthetic Management of a Patient with Saber-Sheath Trachea
AU - Ying Wan
AU - Xin Wang
Y1 - 2024/08/20
PY - 2024
N1 - https://doi.org/10.11648/j.ccr.20240803.11
DO - 10.11648/j.ccr.20240803.11
T2 - Cardiology and Cardiovascular Research
JF - Cardiology and Cardiovascular Research
JO - Cardiology and Cardiovascular Research
SP - 83
EP - 86
PB - Science Publishing Group
SN - 2578-8914
UR - https://doi.org/10.11648/j.ccr.20240803.11
AB - Saber-sheath trachea is a deformation of the trachea characterized by a tracheal index of less than 0.67, commonly found in patients with chronic obstructive pulmonary disease (COPD). This condition can lead to symptoms such as shortness of breath, coughing, and recurrent respiratory infections, which may necessitate surgical intervention. We present the case of a 72-year-old male with a left upper pulmonary lobe tumor scheduled for thoracoscopic lobectomy. The patient exhibited severe emphysema and had a tracheal index of 0.28, indicating a significantly narrowed intrathoracic trachea. Preoperative assessments revealed stable vital signs and low risk for perioperative complications, allowing for standard noninvasive monitoring during the procedure. Anesthesia was induced while maintaining spontaneous breathing using inhalation anesthetics. A left-sided double-lumen endotracheal tube was successfully placed for lung isolation. Throughout the surgery, airway pressures remained below 20 cm H2O, and the patient tolerated ventilation well. Following the procedure, fiberoptic bronchoscopy confirmed the absence of airway complications. The patient experienced a smooth recovery, was discharged after 6 days, and reported feeling well at the 3-month follow-up. This case underscores the importance of careful anesthetic management in patients with saber-sheath trachea undergoing thoracic surgery.
VL - 8
IS - 3
ER -